

Effects of Acute Mental Stress on Choroidal Thickness



Abstract

1. Introduction
2. Methods
2.1. Subjects
2.2. OCT Imaging and Heart Rate Measurements
2.3. OCT Image Processing and Segmentation
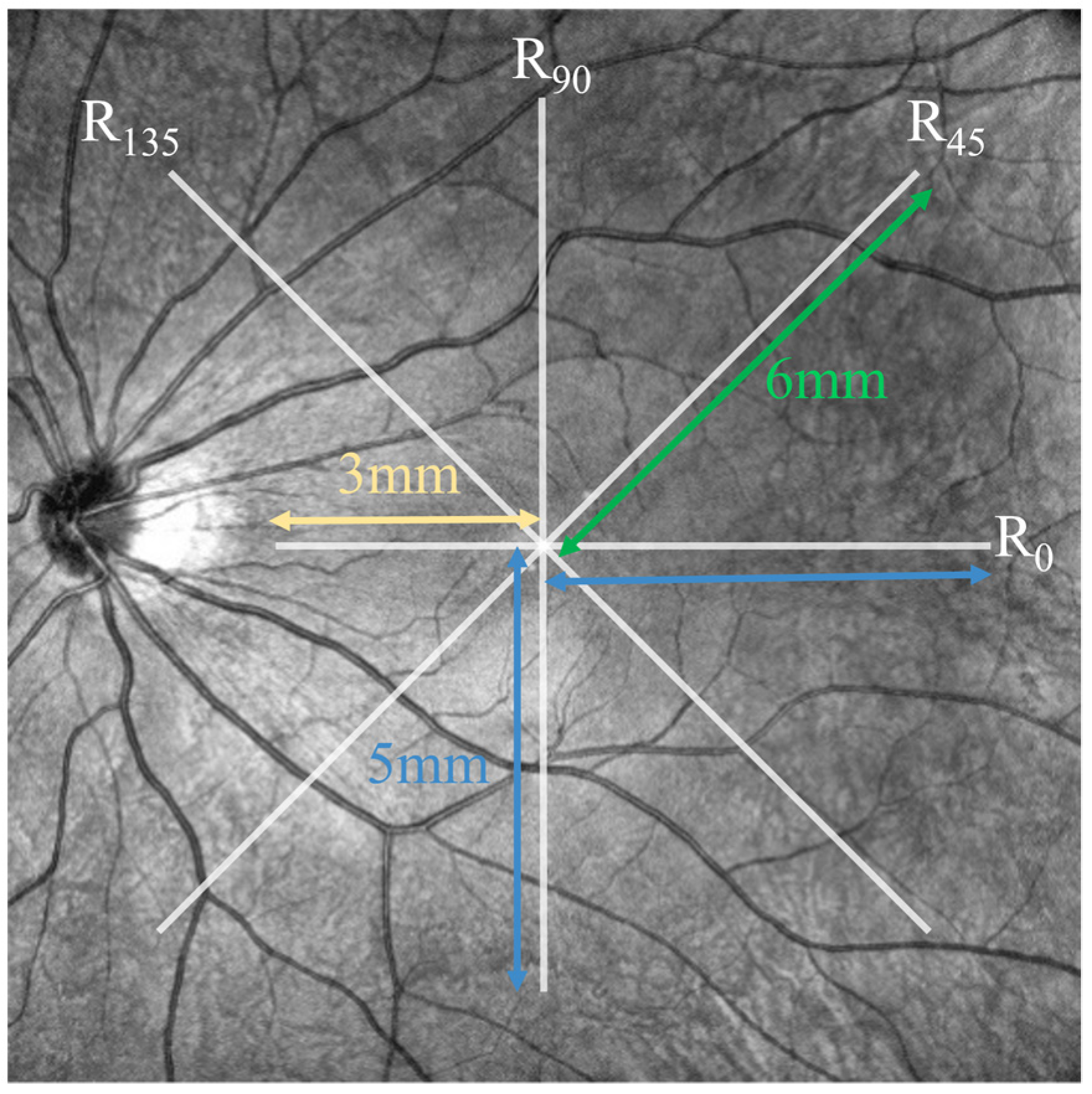
2.4. Measurement of Choroidal, Retinal Thickness, and Posterior Eye Curvature
2.5. Heart Rate Data Analysis
2.6. Statistical Analysis
3. Results
3.1. Subjects and OCT Images
3.2. Automated Segmentation Model
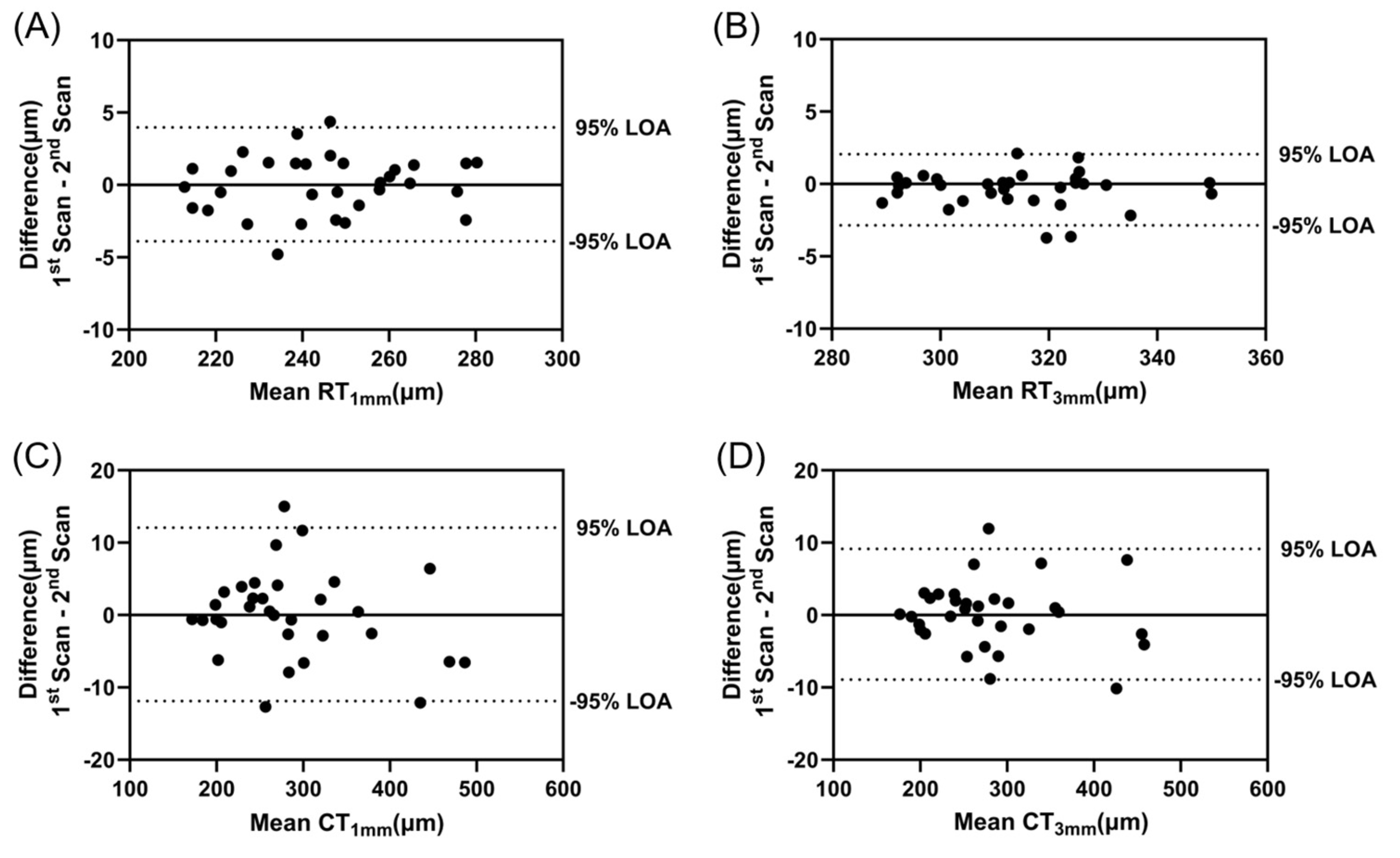
3.3. Within-Session Repeatability
3.4. Changes in Retinal and Choroidal Thickness
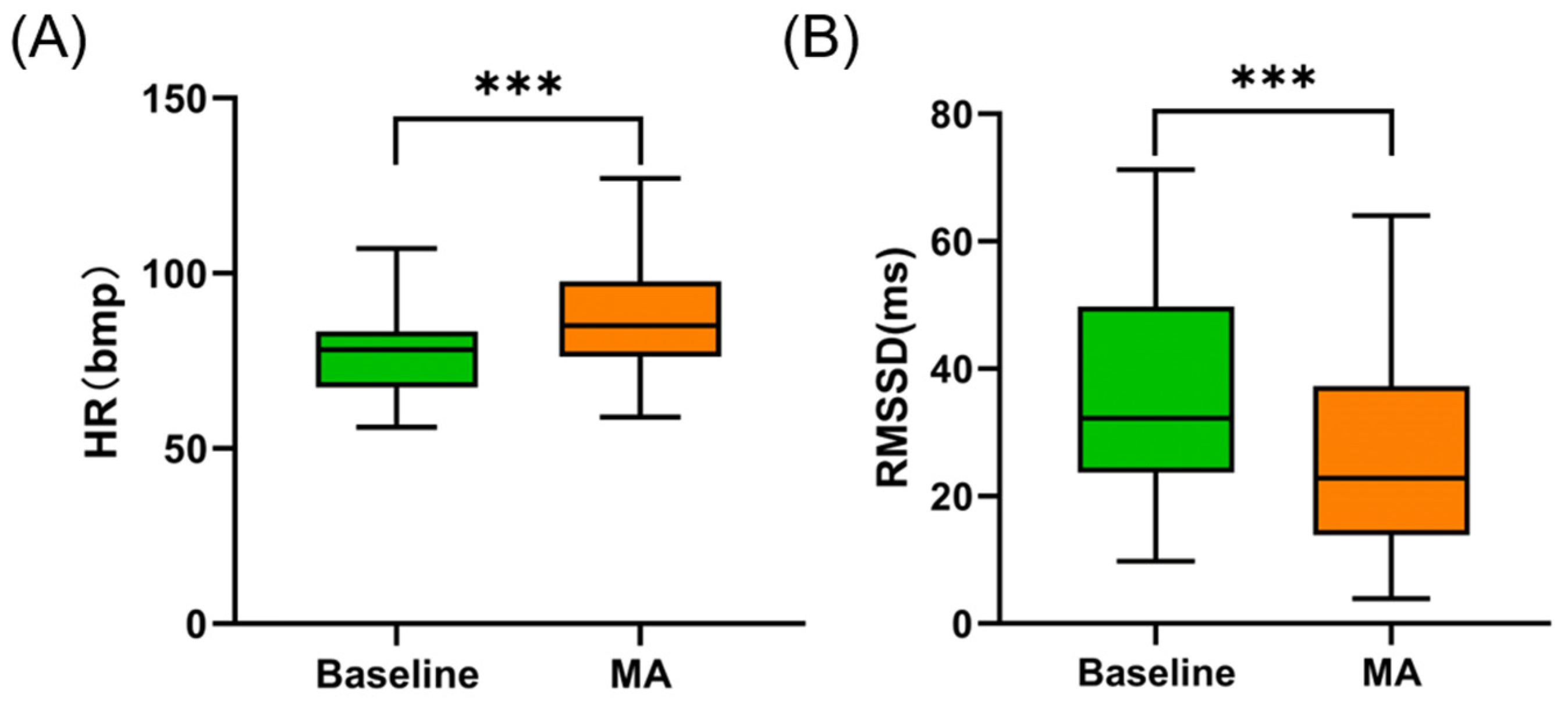
3.5. Heart Rate Parameters Changes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sankaridurg, P.; Tahhan, N.; Kandel, H.; Naduvilath, T.; Zou, H.; Frick, K.D.; Marmamula, S.; Friedman, D.S.; Lamoureux, E.; Keeffe, J.; et al. IMI impact of myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 2. [Google Scholar] [CrossRef]
- Shan, M.; Dong, Y.; Chen, J.; Su, Q.; Wan, Y. Global tendency and frontiers of research on myopia from 1900 to 2020: A bibliometrics analysis. Front. Public Health 2022, 10, 846601. [Google Scholar] [CrossRef]
- Haarman, A.E.G.; Enthoven, C.A.; Tideman, J.W.L.; Tedja, M.S.; Verhoeven, V.J.M.; Klaver, C.C.W. The complications of myopia: A review and meta-analysis. Investig. Ophthalmol. Vis. Sci. 2020, 61, 49. [Google Scholar] [CrossRef]
- Singh, H.; Singh, H.; Latief, U.; Tung, G.K.; Shahtaghi, N.R.; Sahajpal, N.S.; Kaur, I.; Jain, S.K. Myopia, its prevalence, current therapeutic strategy and recent developments: A Review. Indian J. Ophthalmol. 2022, 70, 2788–2799. [Google Scholar] [CrossRef]
- Wildsoet, C.F.; Chia, A.; Cho, P.; Guggenheim, J.A.; Polling, J.R.; Read, S.; Sankaridurg, P.; Saw, S.M.; Trier, K.; Walline, J.J.; et al. IMI—Interventions myopia institute: Interventions for controlling myopia onset and progression report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M106–M131. [Google Scholar] [CrossRef] [PubMed]
- Morgan, I.G.; Wu, P.C.; Ostrin, L.A.; Tideman, J.W.L.; Yam, J.C.; Lan, W.; Baraas, R.C.; He, X.; Sankaridurg, P.; Saw, S.M.; et al. IMI risk factors for myopia. Investig. Ophthalmol. Vis. Sci. 2021, 62, 3. [Google Scholar] [CrossRef] [PubMed]
- Wolffsohn, J.S.; Jong, M.; Smith, E.L., 3rd; Resnikoff, S.R.; Jonas, J.B.; Logan, N.S.; Morgan, I.; Sankaridurg, P.; Ohno-Matsui, K. IMI 2021 reports and digest—Reflections on the implications for clinical practice. Investig. Ophthalmol. Vis. Sci. 2021, 62, 1. [Google Scholar] [CrossRef]
- Bourke, C.M.; Loughman, J.; Flitcroft, D.I.; Loskutova, E.; O’Brien, C. We can’t afford to turn a blind eye to myopia. QJM 2023, 116, 635–639. [Google Scholar] [CrossRef]
- Vogel, S.; Schwabe, L. Learning and memory under stress: Implications for the classroom. NPJ Sci. Learn. 2016, 1, 16011. [Google Scholar] [CrossRef] [PubMed]
- Godoy, L.D.; Rossignoli, M.T.; Delfino-Pereira, P.; Garcia-Cairasco, N.; de Lima Umeoka, E.H. A comprehensive overview on stress neurobiology: Basic concepts and clinical implications. Front. Behav. Neurosci. 2018, 12, 127. [Google Scholar] [CrossRef]
- Joels, M.; Baram, T.Z. The neuro-symphony of stress. Nat. Rev. Neurosci. 2009, 10, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, M.G. Psychological stress and the autonomic nervous system. In Primer on the Autonomic Nervous System, 3rd ed.; Robertson, D., Biaggioni, I., Burnstock, G., Low, P.A., Paton, J.F.R., Eds.; Academic Press: San Diego, CA, USA, 2012; pp. 291–293. [Google Scholar]
- Taelman, J.; Vandeput, S.; Spaepen, A.; Van Huffel, S.; VanderSloten, J.; Verdonck, P.; Nyssen, M.; Haueisen, J. Influence of mental stress on heart rate and heart rate variability. In Proceedings of the 4th European Conference of the International Federation for Medical and Biological Engineering, Antwerp, Belgium, 23–27 November 2008; Springer: Berlin/Heidelberg, Germany, 2009; pp. 1366–1369. [Google Scholar]
- Schneiderman, N.; McCabe, P.M. Psychophysiologic strategies in laboratory research. In Handbook of Research Methods in Cardiovascular Behavioral Medicine; Schneiderman, N., Weiss, S.M., Kaufmann, P.G., Eds.; Springer: Boston, MA, USA, 1989; pp. 349–364. [Google Scholar]
- Bosch, J.A.; de Geus, E.J.; Veerman, E.C.; Hoogstraten, J.; Nieuw Amerongen, A.V. Innate secretory immunity in response to laboratory stressors that evoke distinct patterns of cardiac autonomic activity. Psychosom. Med. 2003, 65, 245–258. [Google Scholar] [CrossRef]
- McDougal, D.H.; Gamlin, P.D. Autonomic control of the eye. Compr. Physiol. 2015, 5, 439–473. [Google Scholar] [CrossRef] [PubMed]
- Delshad, S. Temporal Dynamics of the Eye’s Response to Blur. Ph.D. Thesis, Queensland University of Technology, Brisbane City, Australia, 2018. [Google Scholar]
- Ostrin, L.A.; Harb, E.; Nickla, D.L.; Read, S.A.; Alonso-Caneiro, D.; Schroedl, F.; Kaser-Eichberger, A.; Zhou, X.; Wildsoet, C.F. IMI-the dynamic choroid: New insights, challenges, and potential significance for human myopia. Investig. Ophthalmol. Vis. Sci. 2023, 64, 4. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.R.; Goldstein, D.S. Sympathoneural and adrenomedullary responses to mental stress. Compr. Physiol. 2015, 5, 119–146. [Google Scholar] [CrossRef] [PubMed]
- Ritz, T.; Schulz, S.M.; Rosenfield, D.; Wright, R.J.; Bosquet Enlow, M. Cardiac sympathetic activation and parasympathetic withdrawal during psychosocial stress exposure in 6-month-old infants. Psychophysiology 2020, 57, e13673. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, R.; Montesinos, L.; Melillo, P.; James, C.; Pecchia, L. Ultra-short term HRV features as surrogates of short term HRV: A case study on mental stress detection in real life. BMC Med. Inform. Decis. Mak. 2019, 19, 12. [Google Scholar] [CrossRef] [PubMed]
- Dalmeida, K.M.; Masala, G.L. HRV features as viable physiological markers for stress detection using wearable devices. Sensors 2021, 21, 2873. [Google Scholar] [CrossRef] [PubMed]
- Vasudevan, B.; Ciuffreda, K.J. Additivity of near work-induced transient myopia and its decay characteristics in different refractive groups. Investig. Ophthalmol. Vis. Sci. 2008, 49, 836–841. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, S.; Lin, J.; Chen, W.; Huang, H.; Fan, X.; Cao, X.; Shen, M.; Ye, J.; Zhu, S.; et al. Vascular changes of the choroid and their correlations with visual acuity in pathological myopia. Investig. Ophthalmol. Vis. Sci. 2022, 63, 20. [Google Scholar] [CrossRef]
- Bennett, A.G.; Rudnicka, A.R.; Edgar, D.F. Improvements on littmann’s method of determining the size of retinal features by fundus photography. Graefes Arch. Clin. Exp. Ophthalmol. 1994, 232, 361–367. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3d slicer as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Perona, P.; Malik, J. Scale-space and edge detection using anisotropic diffusion. IEEE Trans. Pattern Anal. Mach. Intell. 1990, 12, 629–639. [Google Scholar] [CrossRef]
- Mari, J.M.; Strouthidis, N.G.; Park, S.C.; Girard, M.J. Enhancement of lamina cribrosa visibility in optical coherence tomography images using adaptive compensation. Investig. Ophthalmol. Vis. Sci. 2013, 54, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Jin, P.; Zhu, J.; Zou, H.; Xu, X.; Tang, M.; Zhou, M.; Gan, Y.; He, J.; Ling, Y.; et al. Multi-scale gcn-assisted two-stage network for joint segmentation of retinal layers and discs in peripapillary oct images. Biomed. Opt. Express 2021, 12, 2204–2220. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental algorithms for scientific computing in python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Umemoto, R.; Hashimoto, Y.; Imabayashi, S.; Yoshitomi, T. Changes in choroidal thickness in healthy participants after induction of sympathetic hyperactivity using the cold pressor test. Graefes Arch. Clin. Exp. Ophthalmol. 2023, 261, 585–587. [Google Scholar] [CrossRef] [PubMed]
- Gregg, M.E.; James, J.E.; Matyas, T.A.; Thorsteinsson, E.B. Hemodynamic profile of stress-induced anticipation and recovery. Int. J. Psychophysiol. 1999, 34, 147–162. [Google Scholar] [CrossRef]
- Thayer, J.F.; Friedman, B.H. Neurovisceral integration model of health disparities in aging. In Critical Perspectives on Racial and Ethnic Differences in Health in Late Life; National Academies Press: Washington, DC, USA, 2004; pp. 567–603. [Google Scholar]
- Usui, S.; Ikuno, Y.; Akiba, M.; Maruko, I.; Sekiryu, T.; Nishida, K.; Iida, T. Circadian changes in subfoveal choroidal thickness and the relationship with circulatory factors in healthy subjects. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2300–2307. [Google Scholar] [CrossRef]
- Burfield, H.J.; Patel, N.B.; Ostrin, L.A. Ocular biometric diurnal rhythms in emmetropic and myopic adults. Investig. Ophthalmol. Vis. Sci. 2018, 59, 5176–5187. [Google Scholar] [CrossRef]
- Chakraborty, R.; Read, S.A.; Collins, M.J. Diurnal variations in axial length, choroidal thickness, intraocular pressure, and ocular biometrics. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5121–5129. [Google Scholar] [CrossRef] [PubMed]
- Ostrin, L.A.; Jnawali, A.; Carkeet, A.; Patel, N.B. Twenty-four hour ocular and systemic diurnal rhythms in children. Ophthalmic Physiol. Opt. 2019, 39, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Delaey, C.; Van De Voorde, J. Regulatory mechanisms in the retinal and choroidal circulation. Ophthalmic Res. 2000, 32, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Alonso-Caneiro, D.; Lingham, G.; Chen, F.K.; Sanfilippo, P.G.; Yazar, S.; Mackey, D.A. Choroidal thickening during young adulthood and baseline choroidal thickness predicts refractive error change. Investig. Ophthalmol. Vis. Sci. 2022, 63, 34. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, L.; Xu, Y.; Pang, Z.; Mu, G. The influence of the choroid on the onset and development of myopia: From perspectives of choroidal thickness and blood flow. Acta Ophthalmol. 2021, 99, 730–738. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Stress, adaptation, and disease. Allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Rohleder, N. Stress-Modulated Pathways; Oxford University Press: Oxford, UK, 2021. [Google Scholar]
- Pereira, V.H.; Campos, I.; Sousa, N. The role of autonomic nervous system in susceptibility and resilience to stress. Curr. Opin. Behav. Sci. 2017, 14, 102–107. [Google Scholar] [CrossRef]
- Chen, J.C.; Schmid, K.L.; Brown, B. The autonomic control of accommodation and implications for human myopia development: A review. Ophthalmic Physiol. Opt. 2003, 23, 401–422. [Google Scholar] [CrossRef]
- Hoseini-Yazdi, H.; Vincent, S.J.; Collins, M.J.; Read, S.A.; Alonso-Caneiro, D. Wide-field choroidal thickness in myopes and emmetropes. Sci. Rep. 2019, 9, 3474. [Google Scholar] [CrossRef]
- Grudzinska, E.; Modrzejewska, M. Modern diagnostic techniques for the assessment of ocular blood flow in myopia: Current state of knowledge. J. Ophthalmol. 2018, 2018, 4694789. [Google Scholar] [CrossRef]
- Jia, Y.; Xue, W.; Wang, Y.; Zhao, L.; Zou, H. Quantitative changes in iris vasculature and blood flow in patients with different refractive errors. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3123–3129. [Google Scholar] [CrossRef] [PubMed]
- Yanov, A.Y.; Prokhorov, A.V. Functional state of the autonomic nervous system in children with varying degrees of myopia. World Appl. Sci. J. 2014, 29, 671–674. [Google Scholar]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart rate variability and cardiac vagal tone in psychophysiological research—Recommendations for experiment planning, data analysis, and data reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zhu, B.; Wang, T.; Wang, H.; Xu, X.; Wang, S.; Yin, Y.; Xiang, Z.; Qian, Y.; Zhang, Z.; et al. Sympathetic nervous system activity is associated with choroidal thickness and axial length in school-aged children. Br. J. Ophthalmol. 2024, 108, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Saxbe, D.E.; Beckes, L.; Stoycos, S.A.; Coan, J.A. Social allostasis and social allostatic load: A new model for research in social dynamics, stress, and health. Perspect. Psychol. Sci. 2020, 15, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.; Vasudevan, B.; Liang, Y.B.; Zhou, H.J.; Ciuffreda, K.J. The association between nearwork-induced transient myopia and progression of refractive error: A 3-year cohort report from Beijing Myopia Progression Study. J. Optom. 2021, 14, 44–49. [Google Scholar] [CrossRef]
- Ciuffreda, K.J.; Lee, M. Differential refractive susceptibility to sustained nearwork. Ophthalmic Physiol. Opt. 2002, 22, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Prousali, E.; Haidich, A.B.; Tzamalis, A.; Ziakas, N.; Mataftsi, A. The role of accommodative function in myopic development: A review. Semin. Ophthalmol. 2022, 37, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Reiner, A.; Fitzgerald, M.E.C.; Del Mar, N.; Li, C. Neural control of choroidal blood flow. Prog. Retin. Eye Res. 2018, 64, 96–130. [Google Scholar] [CrossRef]
- Spaide, R.F. Choroidal blood flow: Review and potential explanation for the choroidal venous anatomy including the vortex vein system. Retina 2020, 40, 1851–1864. [Google Scholar] [CrossRef]
- Zhou, X.; Ye, C.; Wang, X.; Zhou, W.; Reinach, P.; Qu, J. Choroidal blood perfusion as a potential “rapid predictive index” for myopia development and progression. Eye Vis. 2021, 8, 1. [Google Scholar] [CrossRef]
- Angi, M.; Rupolo, G.; de Bertolini, C.; Bisantis, C. Personality, psychophysical stress and myopia progression. A prospective study on 57 university students. Graefes Arch. Clin. Exp. Ophthalmol. 1993, 231, 136–140. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Seeman, T. Protective and damaging effects of mediators of stress. Elaborating and testing the concepts of allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1999, 896, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.N.; Wolffsohn, J.S.; Gilmartin, B. Autonomic correlates of ocular accommodation and cardiovascular function. Ophthalmic Physiol. Opt. 2009, 29, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef]
- Bustamante-Sanchez, A.; Tornero-Aguilera, J.F.; Fernandez-Elias, V.E.; Hormeno-Holgado, A.J.; Dalamitros, A.A.; Clemente-Suarez, V.J. Effect of stress on autonomic and cardiovascular systems in military population: A systematic review. Cardiol. Res. Pract. 2020, 2020, 7986249. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Baseline | MA | Difference | p |
|---|---|---|---|---|
| RT1mm (μm) | 245.717 ± 19.420 | 245.949 ± 19.613 | 0.232 ± 2.352 | 0.575 a |
| RT3mm (μm) | 314.906 ± 15.821 | 314.894 ± 16.007 | −0.012 ± 1.510 | 0.963 a |
| CT1mm (μm) | 288.091 ± 82.384 | 290.833 ± 81.024 | 2.742 ± 7.098 | 0.034 a* |
| CT3mm (μm) | 282.954 ± 76.694 | 286.280 ± 75.912 | 3.326 ± 6.143 | <0.001 b* |
| R0 (mm) | 17.746 ± 4.988 | 17.625 ± 4.958 | −0.122 ± 0.791 | 0.537 b |
| R45 (mm) | 22.074 ± 6.855 | 21.976 ± 7.390 | −0.098 ± 1.573 | 0.221 b |
| R90 (mm) | 22.739 ± 9.699 | 22.698 ± 10.008 | −0.040 ± 1.145 | 0.822 b |
| R135 (mm) | 19.398 ± 5.539 | 19.253 ± 5.113 | −0.145 ± 0.849 | 0.888 b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.; Han, Y.; Liu, M.; Wang, X. Effects of Acute Mental Stress on Choroidal Thickness. Bioengineering 2024, 11, 684. https://doi.org/10.3390/bioengineering11070684
Lin J, Han Y, Liu M, Wang X. Effects of Acute Mental Stress on Choroidal Thickness. Bioengineering. 2024; 11(7):684. https://doi.org/10.3390/bioengineering11070684
Chicago/Turabian StyleLin, Jiechun, Yingxiang Han, Meng Liu, and Xiaofei Wang. 2024. "Effects of Acute Mental Stress on Choroidal Thickness" Bioengineering 11, no. 7: 684. https://doi.org/10.3390/bioengineering11070684
APA StyleLin, J., Han, Y., Liu, M., & Wang, X. (2024). Effects of Acute Mental Stress on Choroidal Thickness. Bioengineering, 11(7), 684. https://doi.org/10.3390/bioengineering11070684