

Predictability of Dental Distalization with Clear Aligners: A Systematic Review

 ,
,  ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
:
1. Introduction
- The material used for the production of the masks is highly innovative; polyurethane is generally used, and even more recently, a multilayer aromatic thermoplastic polyurethane/copolyester, which despite being very thin, guarantees greater resistance and flexibility, and is also hypoallergenic, inert and biologically stable [32].
- Increasing efforts are being made in digitalization using the latest technology to diagnose each case precisely and professionally. During the first visit, a complete 3D scan is performed to see the general state of the oral cavity. Furthermore, it is possible to carry out a video simulation so you can see what the final result will be like before starting orthodontic treatment [33,34].
- Another innovation consists in the use of a 3D printer to produce the aligners [35].
2. Materials and Methods
2.1. Protocol and Registration
2.2. Search Processing
2.3. Eligibility Criteria
2.4. Data Processing
2.5. PICOS Criteria
Quality Assessment
3. Results
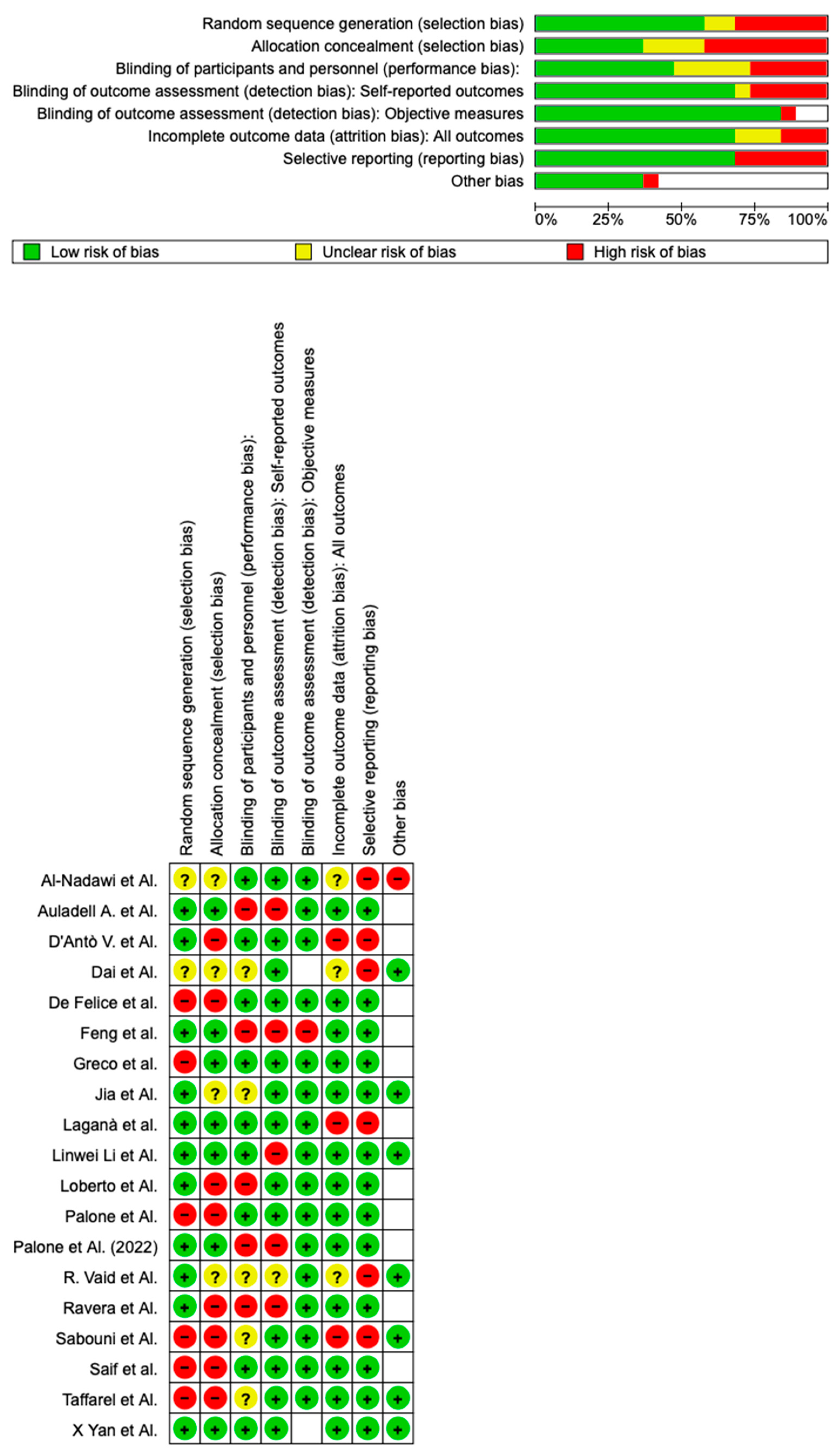
Quality Assessment and Risk of Bias
4. Discussion
4.1. Time of Use
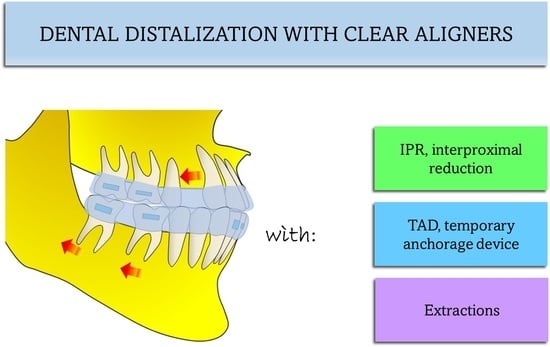
4.2. TADs
4.3. IPR
4.4. Extraction
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BPA | bisphenol A |
| CA | clear aligners |
| CAD/CAM | computer-aided design and computer-aided manufacturing |
| CAT | clear aligner therapy |
| CBCT | cone beam computed tomography |
| EOF | extra-oral force |
| IPR | interproximal reduction |
| TAD | temporary anchorage device |
| DPA | difference between predicted and actual |
References
- Auladell, A.; De La Iglesia, F.; Quevedo, O.; Walter, A.; Puigdollers, A. The Efficiency of Molar Distalization Using Clear Aligners and Mini-Implants: Two Clinical Cases. Int. Orthod. 2022, 20, 100604. [Google Scholar] [CrossRef]
- Yan, X.; Zhang, X.; Ren, L.; Yang, Y.; Wang, Q.; Gao, Y.; Jiang, Q.; Jian, F.; Long, H.; Lai, W. Effectiveness of Clear Aligners in Achieving Proclination and Intrusion of Incisors among Class II Division 2 Patients: A Multivariate Analysis. Prog. Orthod. 2023, 24, 12. [Google Scholar] [CrossRef] [PubMed]
- Zanon, G.; Contardo, L.; Reda, B. The Impact of Orthodontic Treatment on Masticatory Performance: A Literature Review. Cureus 2022, 14, e30453. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Inchingolo, A.M.; Dipalma, G. Non-Hodgkin Lymphoma Affecting the Tongue: Unusual Intra-Oral Location. Head Neck Oncol. 2011, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Huh, H.H.; Chaudhry, K.; Stevens, R.; Subramani, K. Practice of Lingual Orthodontics and Practitioners’ Opinion and Experience with Lingual Braces in the United States. J. Clin. Exp. Dent. 2021, 13, e789–e794. [Google Scholar] [CrossRef]
- Dang, Q.T.; Huynh, T.D.; Inchingolo, F.; Dipalma, G.; Inchingolo, A.D.; Cantore, S.; Paduanelli, G.; Nguyen, K.C.D.; Ballini, A.; Isacco, C.G.; et al. Human Chondrocytes from Human Adipose Tissue-Derived Mesenchymal Stem Cells Seeded on a Dermal-Derived Collagen Matrix Sheet: Our Preliminary Results for a Ready to Go Biotechnological Cartilage Graft in Clinical Practice. Stem Cells Int 2021, 2021, 6664697. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Pacifici, A.; Gargari, M.; Inchingolo, A.D.; Inchingolo, A.M.; Dipalma, G.; Marrelli, M.; Abenavoli, F.M.; Pacifici, L. Use of Dermal-Fat Grafts in the Post-Oncological Reconstructive Surgery of Atrophies in the Zygomatic Region: Clinical Evaluations in the Patients Undergone to Previous Radiation Therapy. Head Face Med. 2012, 8, 33. [Google Scholar] [CrossRef]
- Bowman, S.J. Upper-Molar Distalization and the Distal Jet. J. Clin. Orthod. 2016, 50, 159–169. [Google Scholar]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Di Pede, C.; Garibaldi, M.; Ciocia, A.M.; et al. Treatment of Class III Malocclusion and Anterior Crossbite with Aligners: A Case Report. Medicina 2022, 58, 603. [Google Scholar] [CrossRef]
- Vermesan, D.; Inchingolo, F.; Patrascu, J.M.; Trocan, I.; Prejbeanu, R.; Florescu, S.; Damian, G.; Benagiano, V.; Abbinante, A.; Caprio, M.; et al. Anterior Cruciate Ligament Reconstruction and Determination of Tunnel Size and Graft Obliquity. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 357–364. [Google Scholar]
- Miranda, F.; Barone, S.; Gillot, M.; Baquero, B.; Anchling, L.; Hutin, N.; Gurgel, M.; Al Turkestani, N.; Huang, Y.; Massaro, C.; et al. Artificial Intelligence Applications in Orthodontics. J. Calif. Dent. Assoc. 2023, 51, 2195585. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef]
- Inchingolo, F.; Hazballa, D.; Inchingolo, A.D.; Malcangi, G.; Marinelli, G.; Mancini, A.; Maggiore, M.E.; Bordea, I.R.; Scarano, A.; Farronato, M.; et al. Innovative Concepts and Recent Breakthrough for Engineered Graft and Constructs for Bone Regeneration: A Literature Systematic Review. Materials 2022, 15, 1120. [Google Scholar] [CrossRef]
- Ke, Y.; Zhu, Y.; Zhu, M. A Comparison of Treatment Effectiveness between Clear Aligner and Fixed Appliance Therapies. BMC Oral Health 2019, 19, 24. [Google Scholar] [CrossRef]
- The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/35055811/ (accessed on 5 October 2023).
- Fanali, S.; Tumedei, M.; Pignatelli, P.; Inchingolo, F.; Pennacchietti, P.; Pace, G.; Piattelli, A. Implant Primary Stability with an Osteocondensation Drilling Protocol in Different Density Polyurethane Blocks. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 14–20. [Google Scholar] [CrossRef]
- Gianelly, A.A.; Bednar, J.; Dietz, V.S. Japanese NiTi Coils Used to Move Molars Distally. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 564–566. [Google Scholar] [CrossRef]
- Alogaibi, Y.A.; Al-Fraidi, A.A.; Alhajrasi, M.K.; Alkhathami, S.S.; Hatrom, A.; Afify, A.R. Distalization in Orthodontics: A Review and Case Series. Case Rep. Dent. 2021, 2021, 8843959. [Google Scholar] [CrossRef]
- Jambi, S.; Thiruvenkatachari, B.; O’Brien, K.D.; Walsh, T. Orthodontic Treatment for Distalising Upper First Molars in Children and Adolescents. Cochrane Database Syst. Rev. 2013, 2013, CD008375. [Google Scholar] [CrossRef] [PubMed]
- Hilgers, J.J. The Pendulum Appliance for Class II Non-Compliance Therapy. J. Clin. Orthod. 1992, 26, 706–714. [Google Scholar] [PubMed]
- Al-Ani, M.H.; Mageet, A.O. Extraction Planning in Orthodontics. J. Contemp. Dent. Pract. 2018, 19, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Naragond, A.; Kenganal, S.; Sagarkar, R. Sugaradday Orthodontic Camouflage Treatment in an Adult Patient with a Class II, Division 1 Malocclusion—A Case Report. J. Clin. Diagn. Res. 2013, 7, 395–400. [Google Scholar] [CrossRef]
- Feu, D. Orthodontic Treatment of Periodontal Patients: Challenges and Solutions, from Planning to Retention. Dent. Press. J. Orthod. 2020, 25, 79–116. [Google Scholar] [CrossRef]
- Byloff, F.K.; Darendeliler, M.A.; Clar, E.; Darendeliler, A. Distal Molar Movement Using the Pendulum Appliance. Part 2: The Effects of Maxillary Molar Root Uprighting Bends. Angle Orthod. 1997, 67, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Cantore, S.; Mirgaldi, R.; Ballini, A.; Coscia, M.F.; Scacco, S.; Papa, F.; Inchingolo, F.; Dipalma, G.; De Vito, D. Cytokine Gene Polymorphisms Associate with Microbiogical Agents in Periodontal Disease: Our Experience. Int. J. Med. Sci. 2014, 11, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Sırman, S.S.H.; Özcan, M.; Tozlu, M. Treatment of a Class II Case with Palatally Inserted Distalization Mechanics in an Epilepsy Patient. Turk. J. Orthod. 2017, 30, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Tamer, İ.; Öztaş, E.; Marşan, G. Orthodontic Treatment with Clear Aligners and The Scientific Reality Behind Their Marketing: A Literature Review. Turk. J. Orthod. 2019, 32, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Carpentiere, V.; Piras, F.; Netti, A.; Ferrara, I.; Campanelli, M.; Latini, G.; Viapiano, F.; Costa, S.; Malcangi, G.; et al. Orthodontic Surgical Treatment of Impacted Mandibular Canines: Systematic Review and Case Report. Appl. Sci. 2022, 12, 8008. [Google Scholar] [CrossRef]
- Adina, S.; Dipalma, G.; Bordea, I.R.; Lucaciu, O.; Feurdean, C.; Inchingolo, A.D.; Septimiu, R.; Malcangi, G.; Cantore, S.; Martin, D.; et al. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, G. Statistical Methods for Medical and Biological Students. Stat. Methods Med. Biol. Stud. 1940, 2, 358–359. [Google Scholar]
- AlMogbel, A. Clear Aligner Therapy: Up to Date Review Article. J. Orthod. Sci. 2023, 12, 37. [Google Scholar] [CrossRef]
- Jones, D. Pharmaceutical Applications of Polymers for Drug Delivery; Rapra Review Reports; Rapra Technology: Shrewsbury, MA, USA, 2004; ISBN 978-1-85957-479-9. [Google Scholar]
- Sehrawat, S.; Kumar, A.; Grover, S.; Dogra, N.; Nindra, J.; Rathee, S.; Dahiya, M.; Kumar, D. Study of 3D Scanning Technologies and Scanners in Orthodontics. Mater. Today Proc. 2022, 56, 186–193. [Google Scholar] [CrossRef]
- Jedliński, M.; Mazur, M.; Grocholewicz, K.; Janiszewska-Olszowska, J. 3D Scanners in Orthodontics—Current Knowledge and Future Perspectives—A Systematic Review. Int. J. Environ. Res. Public. Health 2021, 18, 1121. [Google Scholar] [CrossRef]
- Ergül, T.; Güleç, A.; Göymen, M. The Use of 3D Printers in Orthodontics—A Narrative Review. Turk. J. Orthod. 2023, 36, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Hao, J.; Lin, H.; Pan, W.; Yang, J.; Feng, Y.; Wang, G.; Li, J.; Jin, Z.; Zhao, Z.; et al. Deep Learning-Enabled 3D Multimodal Fusion of Cone-Beam CT and Intraoral Mesh Scans for Clinically Applicable Tooth-Bone Reconstruction. Patterns 2023, 4, 100825. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Lee, G.-H.; Moon, D.-N.; Yun, K.-D.; Kim, J.-C.; Lee, K.C. Creation of Digital Virtual Patient by Integrating CBCT, Intraoral Scan, 3D Facial Scan: An Approach to Methodology for Integration Accuracy. J. Craniofacial Surg. 2022, 33, e396–e398. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Liu, L.; Wu, Z.; Shan, D.; Pu, L.; Gao, Y.; Tang, Z.; Li, X.; Jian, F.; Wang, Y.; et al. The Predictability of Orthodontic Tooth Movements through Clear Aligner among First-Premolar Extraction Patients: A Multivariate Analysis. Prog. Orthod. 2022, 23, 52. [Google Scholar] [CrossRef] [PubMed]
- Mavropoulos, A.; Kiliaridis, S. Orthodontic Literature: An Overview of the Last 2 Decades. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 30–40. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Topi, S.; Gnoni, A.; Dipalma, G.; Mancini, A.; Di Domenico, M.; Tartaglia, G.M.; Scarano, A.; et al. The Gaseous Ozone Therapy as a Promising Antiseptic Adjuvant of Periodontal Treatment: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2022, 19, 985. [Google Scholar] [CrossRef]
- D’Antò, V.; Valletta, R.; Ferretti, R.; Bucci, R.; Kirlis, R.; Rongo, R. Predictability of Maxillary Molar Distalization and Derotation with Clear Aligners: A Prospective Study. Int. J. Environ. Res. Public Health 2023, 20, 2941. [Google Scholar] [CrossRef]
- Castroflorio, T.; Sedran, A.; Parrini, S.; Garino, F.; Reverdito, M.; Capuozzo, R.; Mutinelli, S.; Grybauskas, S.; Vaitiekūnas, M.; Deregibus, A. Predictability of Orthodontic Tooth Movement with Aligners: Effect of Treatment Design. Prog. Orthod. 2023, 24, 2. [Google Scholar] [CrossRef]
- Rapone, B.; Lorusso, F.; Dipalma, G.; Ceci, S.; Scarano, A.; Corsalini, M.; Di Venere, D.; Inchingolo, F.; Corriero, A.; Bordea, I. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Meta-Analysis in Evidence-Based Orthodontics—Papadopoulos—2003—Orthodontics & Craniofacial Research—Wiley Online Library. Available online: https://onlinelibrary.wiley.com/doi/full/10.1034/j.1600-0854.2003.3r275.x (accessed on 5 October 2023).
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina (B Aires) 2023, 59, 410. [Google Scholar] [CrossRef]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef] [PubMed]
- Bondemark, L. A Comparative Analysis of Distal Maxillary Molar Movement Produced by a New Lingual Intra-Arch Ni-Ti Coil Appliance and a Magnetic Appliance. Eur. J. Orthod. 2000, 22, 683–695. [Google Scholar] [CrossRef] [PubMed]
- Erverdi, N.; Koyutürk, O.; Küçükkeles, N. Nickel-Titanium Coil Springs and Repelling Magnets: A Comparison of Two Different Intra-Oral Molar Distalization Techniques. Br. J. Orthod. 1997, 24, 47–53. [Google Scholar] [CrossRef]
- Kazancı, F.; Aydoğan, C.; Alkan, Ö. Patients’ and Parents’ Concerns and Decisions about Orthodontic Treatment. Korean J. Orthod. 2016, 46, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Patano, A.; Malcangi, G.; Azzollini, D.; Laudadio, C.; Ciocia, A.M.; Sardano, R.; Ferrante, L.; Campanelli, M.; Dipalma, G.; et al. Mandibular Molar Distalization in Class III Malocclusion: A Systematic Review. Appl. Sci. 2023, 13, 9337. [Google Scholar] [CrossRef]
- Ferguson, D.J.; Carano, A.; Bowman, S.J.; Davis, E.C.; Gutierrez Vega, M.E.; Lee, S.H. A Comparison of Two Maxillary Molar Distalizing Appliances with the Distal Jet. World J. Orthod. 2005, 6, 382–390. [Google Scholar]
- Torsello, F.; D’Amico, G.; Staderini, E.; Marigo, L.; Cordaro, M.; Castagnola, R. Factors Influencing Appliance Wearing Time during Orthodontic Treatments: A Literature Review. Appl. Sci. 2022, 12, 7807. [Google Scholar] [CrossRef]
- Bondemark, L.; Kurol, J. Class II Correction with Magnets and Superelastic Coils Followed by Straight-Wire Mechanotherapy. Occlusal Changes during and after Dental Therapy. J. Orofac. Orthop. 1998, 59, 127–138. [Google Scholar] [CrossRef]
- Chaqués-Asensi, J.; Kalra, V. Effects of the Pendulum Appliance on the Dentofacial Complex. J. Clin. Orthod. 2001, 35, 254–257. [Google Scholar]
- Ackerman, J.L.; Proffit, W.R. Communication in Orthodontic Treatment Planning: Bioethical and Informed Consent Issues. Angle Orthod. 1995, 65, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Gvozdeva, L.M.; Danilova, M.A.; Alexandrova, L.I.; Dmitrienko, I.V. The results of orthodontic treatment using aligners from the perspective of quality of life of patients with dentoalveolar anomalies. Stomatologiya 2021, 100, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Ceci, S.; Coloccia, G.; Azzollini, D.; Malcangi, G.; Mancini, A.; Inchingolo, F.; Trerotoli, P.; Dipalma, G.; Patano, A. Predictability and Effectiveness of Nuvola® Aligners in Dentoalveolar Transverse Changes: A Retrospective Study. Biomedicines 2023, 11, 1366. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, M.; Daryanavard, H.; Ashtiani, A.H.; Moradinejad, M.; Rakhshan, V. A Systematic Review of Biocompatibility and Safety of Orthodontic Clear Aligners and Transparent Vacuum-Formed Thermoplastic Retainers: Bisphenol-A Release, Adverse Effects, Cytotoxicity, and Estrogenic Effects. Dent. Res. J. 2023, 20, 41. [Google Scholar]
- Cen, X.; Pan, X.; Wang, R.; Huang, X.; Zhao, Z. The Complex of Tannic Acid and Cetylpyridinium Chloride: An Antibacterial and Staining-Removal Cleaner for the Aligners. Am. J. Orthod. Dentofac. Orthop. 2023, in press. [CrossRef]
- Patil, G.V.; Lakhe, P.; Niranjane, P. Maxillary Expansion and Its Effects on Circummaxillary Structures: A Review. Cureus 2023, 15, e33755. [Google Scholar] [CrossRef] [PubMed]
- Bruni, A.; Gallo, V.; Parrini, S.; Ferrillo, M.; Garino, F.; Deregibus, A.; Castroflorio, T. Effectiveness of Aligners Versus Rapid Palatal Expander on Palatal Volume in Mixed Dentition Patients: A Randomized Controlled Trial. Research Square 2022. [Google Scholar] [CrossRef]
- Atcherson, S.R.; Mendel, L.L.; Baltimore, W.J.; Patro, C.; Lee, S.; Pousson, M.; Spann, M.J. The Effect of Conventional and Transparent Surgical Masks on Speech Understanding in Individuals with and without Hearing Loss. J. Am. Acad. Audiol. 2017, 28, 58–67. [Google Scholar] [CrossRef]
- Dai, F.; Xu, T.; Shu, G. Comparison of Achieved and Predicted Crown Movement in Adults after 4 First Premolar Extraction Treatment with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 805–813. [Google Scholar] [CrossRef]
- Vaid, N.R.; Sabouni, W.; Wilmes, B.; Bichu, Y.M.; Thakkar, D.P.; Adel, S.M. Customized Adjuncts with Clear Aligner Therapy: “The Golden Circle Model” Explained! J. World Fed. Orthod. 2022, 11, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Taffarel, I.A.; Gasparello, G.G.; Mota-Júnior, S.L.; Pithon, M.M.; Taffarel, I.P.; Meira, T.M.; Tanaka, O.M. Distalization of Maxillary Molars with Invisalign Aligners in Nonextraction Patients with Class II Malocclusion. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e176–e182. [Google Scholar] [CrossRef]
- Sabouni, W.; Muthuswamy Pandian, S.; Vaid, N.R.; Adel, S.M. Distalization Using Efficient Attachment Protocol in Clear Aligner Therapy—A Case Report. Clin. Case Rep. 2023, 11, e6854. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.; Wang, C.; He, Y.; Wang, C.; Apicella, A.; Song, J.; Fan, Y. Effect of 3D Anchorage Attachment on the Alleviating Tipping/Extrusion of Premolars for En-Mass Distalization of Maxillary Molars with Clear Aligners: A Finite Element Study. Med. Nov. Technol. Devices 2023, 18, 100231. [Google Scholar] [CrossRef]
- Al-Nadawi, M.; Kravitz, N.D.; Hansa, I.; Makki, L.; Ferguson, D.J.; Vaid, N.R. Effect of Clear Aligner Wear Protocol on the Efficacy of Tooth Movement: A Randomized Clinical Trial. Angle Orthod. 2021, 91, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Guo, R.; Zhang, L.; Huang, Y.; Jia, Y.; Li, W. Maxillary Molar Distalization with a 2-Week Clear Aligner Protocol in Patients with Class II Malocclusion: A Retrospective Study. Am. J. Orthod. Dentofac. Orthop. 2023, 164, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Ravera, S.; Castroflorio, T.; Garino, F.; Daher, S.; Cugliari, G.; Deregibus, A. Maxillary Molar Distalization with Aligners in Adult Patients: A Multicenter Retrospective Study. Prog. Orthod. 2016, 17, 12. [Google Scholar] [CrossRef]
- Palone, M.; Pignotti, A.; Morin, E.; Pancari, C.; Spedicato, G.A.; Cremonini, F.; Lombardo, L. Analysis of Overcorrection to Be Included for Planning Clear Aligner Therapy: A Retrospective Study. Angle Orthod. 2023, 93, 11–18. [Google Scholar] [CrossRef]
- Loberto, S.; Paoloni, V.; Pavoni, C.; Cozza, P.; Lione, R. Anchorage Loss Evaluation during Maxillary Molars Distalization Performed by Clear Aligners: A Retrospective Study on 3D Digital Casts. Appl. Sci. 2023, 13, 3646. [Google Scholar] [CrossRef]
- Palone, M.; Baciliero, M.; Cervinara, F.; Maino, G.B.; Paoletto, E.; Cremonini, F.; Lombardo, L. Class II Treatment of Transverse Maxillary Deficiency with a Single Bone-Borne Appliance and Hybrid Clear Aligner Approach in an Adult Patient: A Case Report. J. World Fed. Orthod. 2022, 11, 80–94. [Google Scholar] [CrossRef]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of Interproximal Enamel Reduction during Clear Aligner Treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef]
- Feng, X.; Jiang, Y.; Zhu, Y.; Hu, L.; Wang, J.; Qi, Y.; Ma, S. Comparison between the Designed and Achieved Mesiodistal Angulation of Maxillary Canines and Posterior Teeth and Influencing Factors: First Premolar Extraction Treatment with Clear Aligners. Am. J. Orthod. Dentofac. Orthop. 2022, 162, e63–e70. [Google Scholar] [CrossRef]
- Saif, B.S.; Pan, F.; Mou, Q.; Han, M.; Bu, W.; Zhao, J.; Guan, L.; Wang, F.; Zou, R.; Zhou, H.; et al. Efficiency Evaluation of Maxillary Molar Distalization Using Invisalign Based on Palatal Rugae Registration. Am. J. Orthod. Dentofac. Orthop. 2022, 161, e372–e379. [Google Scholar] [CrossRef]
- Laganà, G.; Malara, A.; Lione, R.; Danesi, C.; Meuli, S.; Cozza, P. Enamel Interproximal Reduction during Treatment with Clear Aligners: Digital Planning versus OrthoCAD Analysis. BMC Oral Health 2021, 21, 199. [Google Scholar] [CrossRef]
- Greco, M.; Rossini, G.; Rombolà, A. G-Block: Posterior Anchorage Device Tads-Supported after Molar Distalization with Aligners: An Adult Case Report. Int. Orthod. 2022, 20, 100687. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 110, 418–421. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of Children with Removable Functional Appliance with Microchip Integrated during COVID-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Grec, R.; Janson, G.; Castello Branco, N.; Moura-Grec, P.G.; Patel, M.; Henriques, J. Intraoral Distalizer Effects with Conventional and Skeletal Anchorage: A Meta-Analysis. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 602–615. [Google Scholar] [CrossRef]
- Bondemark, L.; Karlsson, I. Extraoral vs Intraoral Appliance for Distal Movement of Maxillary First Molars: A Randomized Controlled Trial. Angle Orthod. 2005, 75, 699–706. [Google Scholar] [CrossRef]
- Liu, X.; Cheng, Y.; Qin, W.; Fang, S.; Wang, W.; Ma, Y.; Jin, Z. Effects of Upper-Molar Distalization Using Clear Aligners in Combination with Class II Elastics: A Three-Dimensional Finite Element Analysis. BMC Oral Health 2022, 22, 546. [Google Scholar] [CrossRef] [PubMed]
- Kinzinger, G.S.M.; Gross, U.; Fritz, U.B.; Diedrich, P.R. Anchorage Quality of Deciduous Molars versus Premolars for Molar Distalization with a Pendulum Appliance. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Ceratti, C.; Maspero, C.; Consonni, D.; Caprioglio, A.; Connelly, S.; Inchingolo, F.; Tartaglia, G. Cone-Beam Computed Tomographic Assessment of the Mandibular Condylar Volume in Different Skeletal Patterns: A Retrospective Study in Adult Patients. Bioengineering 2022, 9, 102. [Google Scholar] [CrossRef] [PubMed]
- Haouili, N.; Kravitz, N.D.; Vaid, N.R.; Ferguson, D.J.; Makki, L. Has Invisalign Improved? A Prospective Follow-up Study on the Efficacy of Tooth Movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Solano-Mendoza, B.; Sonnemberg, B.; Solano Reina, E.; Iglesias-Linares, A. How Effective Is the Invisalign® System in Expansion Movement with Ex30′ Aligners? Clin. Oral Investig. 2017, 21, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Mavropoulos, A.; Karamouzos, A.; Kiliaridis, S.; Papadopoulos, M. Efficiency of Noncompliance Simultaneous First and Second Upper Molar Distalization: A Three-Dimensional Tooth Movement Analysis. Angle Orthod. 2009, 75, 532–539. [Google Scholar]
- Cui, J.-Y.; Ting, L.; Cao, Y.-X.; Sun, D.-X.; Bing, L.; Wu, X.-P. Morphology Changes of Maxillary Molar Distalization by Clear Aligner Therapy. Int. J. Morphol. 2022, 40, 920–926. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Economic Inequalities and Temporomandibular Disorders: A Systematic Review with Meta-analysis. J. Oral Rehabil. 2023, 50, 715–723. [Google Scholar] [CrossRef]
- Di Stasio, D.; Lauritano, D.; Minervini, G.; Paparella, R.S.; Petruzzi, M.; Romano, A.; Candotto, V.; Lucchese, A. Management of Denture Stomatitis: A Narrative Review. J Biol Regul Homeost Agents 2018, 32, 113–116. [Google Scholar]
- Qazi, N.; Pawar, M.; Padhly, P.P.; Pawar, V.; D’Amico, C.; Nicita, F.; Fiorillo, L.; Alushi, A.; Minervini, G.; Meto, A. Teledentistry: Evaluation of Instagram Posts Related to Bruxism. Technology and Health Care 2023, 31, 1923–1934. [Google Scholar] [CrossRef]
- Papadopoulos, M.A. Efficient Distalization of Maxillary Molars with Temporary Anchorage Devices for the Treatment of Class II Malocclusion. Turk. J. Orthod. 2020, 33, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, D.P.; Sant’Anna, E.F.; Machado, A.W.; Moon, W. Non-Surgical Treatment of Transverse Deficiency in Adults Using Microimplant-Assisted Rapid Palatal Expansion (MARPE). Dent. Press. J. Orthod. 2017, 22, 110–125. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Patano, A.; De Santis, M.; Del Vecchio, G.; Ferrante, L.; Morolla, R.; Pezzolla, C.; Sardano, R.; Dongiovanni, L.; Inchingolo, F.; et al. Comparison of Different Types of Palatal Expanders: Scoping Review. Children 2023, 10, 1258. [Google Scholar] [CrossRef] [PubMed]
- Skeletal Anchorage—An Overview|ScienceDirect Topics. Available online: https://www.sciencedirect.com/topics/medicine-and-dentistry/skeletal-anchorage (accessed on 1 October 2023).
- Inchingolo, A.M.; Malcangi, G.; Costa, S.; Fatone, M.C.; Avantario, P.; Campanelli, M.; Piras, F.; Patano, A.; Ferrara, I.; Di Pede, C.; et al. Tooth Complications after Orthodontic Miniscrews Insertion. Int. J. Environ. Res. Public Health 2023, 20, 1562. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.E.; Chang, C.H.; Chen, J.; Brezniak, N.; Yadav, S. Integrating Skeletal Anchorage into Fixed and Aligner Biomechanics. J. World Fed. Orthod. 2022, 11, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Alle, U.K. Interproximal Reduction Facilitating Orthodontic Teeth Extraction. Cureus 2023, 15, e41403. [Google Scholar] [CrossRef]
- Cirulli, N.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Marinelli, G.; Malcangi, G.; Coloccia, G.; Montenegro, V.; Di Pede, C.; Ciocia, A.M.; et al. Innovative Application of Diathermy in Orthodontics: A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 7448. [Google Scholar] [CrossRef]
- Hariharan, A.; Abu Arqub, S.; Gandhi, V.; Godoy, L.; Kuo, C.-L.; Uribe, F. Evaluation of Interproximal Reduction in Individual Teeth, and Full Arch Assessment in Clear Aligner Therapy: Digital Planning versus 3D Model Analysis after Reduction. Prog. Orthod. 2022, 23, 9. [Google Scholar] [CrossRef]
- Wang, S.; Huang, Y.; Fan, D.; Liu, H.; Yuan, C.; Yang, L.; Wang, P. Effects of Overtreatment with Different Attachment Positions on Maxillary Anchorage Enhancement with Clear Aligners: A Finite Element Analysis Study. BMC Oral Health 2023, 23, 693. [Google Scholar] [CrossRef]
- Lyros, I.; Tsolakis, I.A.; Maroulakos, M.P.; Fora, E.; Lykogeorgos, T.; Dalampira, M.; Tsolakis, A.I. Orthodontic Retainers—A Critical Review. Children 2023, 10, 230. [Google Scholar] [CrossRef]
- Lyu, X.; Cao, X.; Chen, L.; Liu, Y.; Li, H.; Hu, C.; Tan, J. Accumulated Biomechanical Effects of Mandibular Molar Mesialization Using Clear Aligners with Auxiliary Devices: An Iterative Finite Element Analysis. Prog. Orthod. 2023, 24, 13. [Google Scholar] [CrossRef] [PubMed]
- Putrino, A.; Marinelli, E.; Zaami, S. The Power of Customized Clear Aligners in Closing Molar Edentulous Spaces: Clinical and Medico-Legal Considerations in a Scoping Review and Case Report. J. Pers. Med. 2023, 13, 1389. [Google Scholar] [CrossRef] [PubMed]
- Mheidly, N.; Fares, M.Y.; Zalzale, H.; Fares, J. Effect of Face Masks on Interpersonal Communication During the COVID-19 Pandemic. Front. Public Health 2020, 8, 582191. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, I.; Bondemark, L. Intraoral Maxillary Molar Distalization. Angle Orthod. 2006, 76, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.T.; Hajeer, M.Y.; Sultan, K. Treatment Effectiveness of Clear Aligners in Correcting Complicated and Severe Malocclusion Cases Compared to Fixed Orthodontic Appliances: A Systematic Review. Cureus 2023, 15, e38311. [Google Scholar] [CrossRef]
- Karvelas, N.; Dragomir, B.R.; Chehab, A.; Panaite, T.; Papadopoulos, M.A.; Zetu, I. Non-Compliance Distalization Appliances Supported by Mini-Implants: A Systematic Review. Appl. Sci. 2023, 13, 5176. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Articles screening strategy | Keywords: orthodontics AND aligners AND distalization |
| Boolean Indicators: (“A” AND “B”) | |
| Timespan: 10 years (2013-2023) | |
| Electronic Database: Pubmed, Web of Science, Scopus |
| Criteria | Application in the Present Study |
|---|---|
| Population | Both children and adults |
| Intervention | Orthodontic treatment with CAs |
| Comparisons | Comparing movements obtained with aligners |
| Outcomes | Efficacy using CAs to obtain Orthodontic movements |
| Study design | Clinical Trials |
| Authors and Years | Study Design | Number of Patient | Average Age (Years) | Aligners Type | Outcomes |
|---|---|---|---|---|---|
| Dai et al. (2021) [63] | Randomized clinical trial | 17 | 25 ± 5 | Invisalign aligners | Coronal movements of the maxillary and mandibular first molars, canines and central incisors were not fully achieved as expected. |
| R. Vaid et al. (2022) [64] | Observational study | - | - | Invisalign aligners | CAT has been shown to be biomechanically inadequate for achieving complex orthodontic movements based on aligner use alone, and it is the orthodontist’s knowledge of biomechanics that can make any aligner system succeed or fail. |
| Taffarel et al. (2022) [65] | Retrospective study | 32 | 35 ± 9 | Invisalign aligners | The null hypothesis that distalization of posterior teeth occurs in adult patients using Invisalign aligners was rejected. Treatment of Class II malocclusion with Invisalign aligners did not occur as expected in the virtual planning prepared by ClinCheck according to the occlusal outcome evaluation standards established by the ABO upon completion of use of a set of sequentially distalized aligners. |
| Sabouni et al. (2023) [66] | Case report | 1 | 25 | Invisalign aligners | The combined use of aligners with appropriate position and attachment geometry is an effective means of solving more complex orthodontic problems such as Class II malocclusions in a time frame comparable to, if not shorter than, conventional fixed orthodontics but with excellent aesthetics, oral hygiene and quality of life. |
| Jia et al. (2023) [67] | Observational study | - | - | CAT | Transparent aligners can effectively control the rotation and tipping of anchor units caused by 3D anchor attachment. |
| Al-Nadawi et al. (2021) [68] | Prospective study | 80 | 35 | Invisalign aligners | Achieving clinically similar accuracy between the 7-day and 14-day protocols in half the treatment time suggests that a 7-day protocol is an acceptable treatment protocol. |
| X Yan et al. (2023) [2] | Retrospective study | 51 | 25 | Invisalign aligners | For Class II division 2 patients, expected incisor proclination (69.8%) and intrusion (53.3%) are partially achieved with CAT. Excessive labial movement (0.7 mm) of the incisors may occur. Incisor movement is influenced by the amount of expected movement, premolar extraction, canine proclination, molar distalization, mini-implants, and age. |
| Linwei Li et al. (2023) [69] | Retrospective study | 43 | adults | Invisalign aligners | The efficacy of molar distalization with CAs was significantly affected by anterior teeth retraction, and the arch width significantly increased at premolar and molar levels. |
| Ravera et al. (2016) [70] | Retrospective study | 20 (9 males and 11 females) | 29.73 | Invisalign aligners | Aligner therapy in association with composite attachments and Class II elastics can distalize maxillary first molar by 2.25 mm without significant tipping and vertical movements of the crown. |
| Auladell A. et al. (2022) [1] | Case reports | First Case (male) and second case (female) | 40 and 28 | Mini implants in the first case, CA in the second case | The mini-implant and the CA can be used when a correction of 2 mm or more in the sagittal plane treatment is required. |
| D’Antò V. et al. (2023) [41] | Prospective study | 16 (4 males, 12 females) | 25.7 ± 8.8 | Ordoline Aligners (UABOrdoline, Vilnius, Lithuania) | The maxillary molar distalization measured at the buccal cusp tips with CAs is effective, although the clinician’s prescription, which is the ideal end-treatment goal, is no likely to be fulfilled. Therefore, refinements are necessary. |
| Palone et al. (2023) [71] | Retrospective study | 150 (80 females, 70 males) | 33.7 ± 12.7 | CAT | When designing difficult movements like tilt and rotation, around 20% overcorrection should be included in the original planning phase, whereas angulation, intrusion, and extrusion needed little to no correction. |
| Loberto et al. (2023) [72] | Retrospective study | 49 (27 females, 22 males) | 14.9 ± 6 | CAT | The study found significant distalization of maxillary first permanent molars, slight anchorage loss in premolars, and mesial displacement in upper canines. Transparent aligners successfully caused molar shift, but upper canine anchorage loss occurred. |
| Palone et al. (2022) [73] | Case report | 1 female | 22 | Hybrid-CAT | A bone appliance was used to achieve rapid skeletal maxillary expansion and bilateral molar distalization in a patient with Class II malocclusion, maxillary skeletal transverse deficiency, and ectopic maxillary left lateral incisor. |
| De Felice et al. (2020) [74] | Clinical study | 40 | - | CAT | The study found that the actual interproximal enamel reduction (IPR) space did not match the intended amount, and less IPR was performed than anticipated, which may not be clinically significant. |
| Feng et al. (2022) [75] | Clinical study | 21 | adults | CAT | It is possible to avoid unintentional crown tilting into the extraction space during space closure by designing the distal crown tipping of the posterior teeth and the mesial crown tipping of the canines. The preliminary formula that has been provided could serve as a reference for anti-tip designs when using CAs. |
| Saif et al. (2021) [76] | Clinical study | 38 | 25.4 | Invisalign aligners | Invisalign is effective for adult patients requiring 2.6 mm distalization of maxillary molars, but clinicians should be aware of adverse effects, especially if the patient initially had a large overjet. |
| Laganà et al. (2021) [77] | Clinical study | 30 (14 males, 16 females) | 24.53 ± 13.41 | CAT | During treatment with CAs, there is a discrepancy in the amount of interproximal enamel reduction (IPR) reported by the ClinCheck program and the amount of IPR carried out by the orthodontist. |
| Greco et al. (2022) [78] | Case report | 1 female | 25 | G-Block: Posterior anchorage device TADs-supported aligners | After distalization of the maxillary molars with aligners, the use of TADs for posterior anchorage may be an efficient way to manage posterior anchorage, requiring less patient cooperation when using elastics and making movements of the posterior teeth simpler by combining the force expressed by the aligners with the force expressed by the auxiliary system. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, A.M.; Inchingolo, A.D.; Carpentiere, V.; Del Vecchio, G.; Ferrante, L.; Di Noia, A.; Palermo, A.; Di Venere, D.; Dipalma, G.; Inchingolo, F. Predictability of Dental Distalization with Clear Aligners: A Systematic Review. Bioengineering 2023, 10, 1390. https://doi.org/10.3390/bioengineering10121390
Inchingolo AM, Inchingolo AD, Carpentiere V, Del Vecchio G, Ferrante L, Di Noia A, Palermo A, Di Venere D, Dipalma G, Inchingolo F. Predictability of Dental Distalization with Clear Aligners: A Systematic Review. Bioengineering. 2023; 10(12):1390. https://doi.org/10.3390/bioengineering10121390
Chicago/Turabian StyleInchingolo, Angelo Michele, Alessio Danilo Inchingolo, Vincenzo Carpentiere, Gaetano Del Vecchio, Laura Ferrante, Angela Di Noia, Andrea Palermo, Daniela Di Venere, Gianna Dipalma, and Francesco Inchingolo. 2023. "Predictability of Dental Distalization with Clear Aligners: A Systematic Review" Bioengineering 10, no. 12: 1390. https://doi.org/10.3390/bioengineering10121390
APA StyleInchingolo, A. M., Inchingolo, A. D., Carpentiere, V., Del Vecchio, G., Ferrante, L., Di Noia, A., Palermo, A., Di Venere, D., Dipalma, G., & Inchingolo, F. (2023). Predictability of Dental Distalization with Clear Aligners: A Systematic Review. Bioengineering, 10(12), 1390. https://doi.org/10.3390/bioengineering10121390