
Beliefs, Practices, and Knowledge of Household Food Handlers Regarding the Impact of Electricity Outages on Food Safety: Findings from a National Cross-Sectional Study in Lebanon


 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
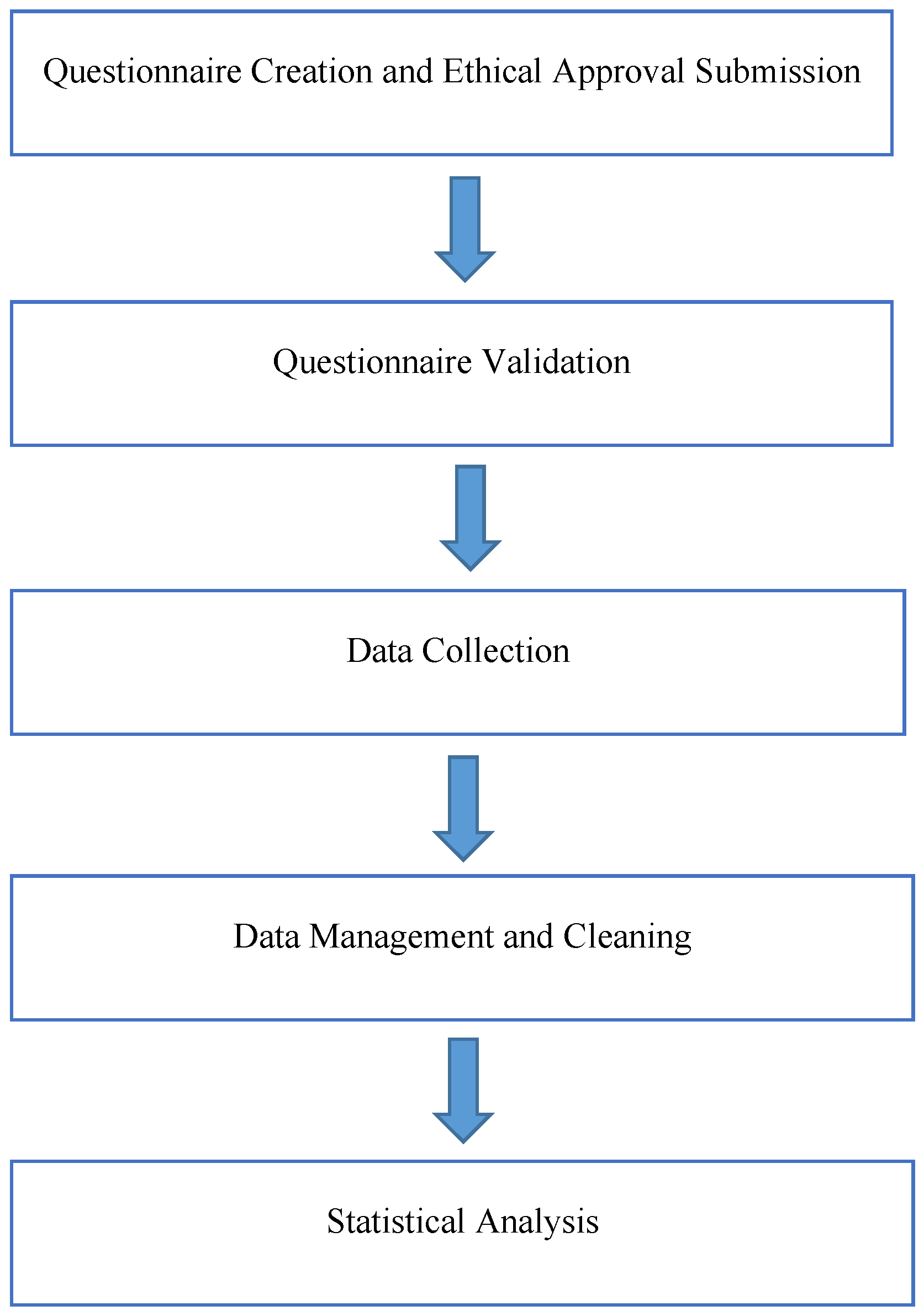
2.2. Schematic Overview of the Survey Program
2.3. Survey Process
2.4. Survey Validation
2.5. Ethical Considerations
2.6. Data Collection
2.7. Statistical Analysis
3. Results
3.1. Participants Socio-Demographic Characteristics
3.2. Basic Questions Related to Food Safety in Households
3.3. Food Safety Knowledge Among Participants
3.4. Beliefs Towards the Risks Associated with Food Safety
3.5. Participant Practices Associated with Food Safety
3.6. Simple and Multiple Logistic Regression Analysis
3.7. Association Between the Different KAP Scores
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Todd, E. Food-Borne Disease Prevention and Risk Assessment. International journal of environmental research and public health. Int. J. Environ. Res. Public Health 2020, 17, 5129. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7399861/ (accessed on 16 October 2021). [CrossRef] [PubMed]
- Havelaar, A.H.; Brul, S.; de Jong, A.; de Jonge, R.; Zwietering, M.H.; Ter Kuile, B.H. Future challenges to microbial food safety. Int. J. Food Microbiol. 2010, 139 (Suppl. S1), S79–S94. Available online: https://pubmed.ncbi.nlm.nih.gov/19913933/ (accessed on 16 October 2021). [CrossRef]
- Centers for Disease Control and Prevention. Challenges in Food Safety. 2020. Available online: https://www.cdc.gov/food-safety/about/what-cdc-is-doing.html (accessed on 27 February 2025).
- Scott, E. Food Safety and Foodborne Disease in 21st Century homes. Can. J. Infect. Dis.=J. Can. Des Mal. Infect. 2003, 14, 277–280. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2094945/ (accessed on 16 October 2021). [CrossRef]
- Byrd-Bredbenner, C.; Berning, J.; Martin-Biggers, J.; Quick, V. Food safety in home kitchens: A synthesis of the literature. Int. J. Environ. Res. Public Health 2013, 10, 4060–4085. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3799528/ (accessed on 16 October 2021). [CrossRef] [PubMed]
- Nasser, H. How to Keep Food Safe During Power Cuts. LAU. 2021. Available online: https://news.lau.edu.lb/2021/how-to-keep-food-safe-during-power-cuts.php (accessed on 27 February 2025).
- Langiano, E.; Ferrara, M.; Lanni, L.; Viscardi, V.; Abbatecola, A.M.; De Vito, E. Food Safety at Home: Knowledge and practices of consumers. Z. Fur Gesundheitswissenschaften=J. Public Health 2012, 20, 47–57. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3268974/ (accessed on 17 October 2021). [CrossRef] [PubMed]
- Manafe, M.; Gordon, R.; Ncube, L. Food Hygiene and food safety practices of households in a township north of Tshwane, Gauteng. Health SA=SA Gesondheid U.S. Natl. Libr. Med. 2023, 28, 2346. Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC10623475/ (accessed on 20 February 2025). [CrossRef]
- World Report 2021: RIGHTS Trends in Lebanon. 2021. Available online: https://www.hrw.org/world-report/2021/country-chapters/lebanon (accessed on 16 April 2021).
- Water Supply Systems on the Verge of Collapse in LEBANON: Over 71 Per Cent of People Risk Losing Access to Water. UNICEF. 2021. Available online: https://www.unicef.org/press-releases/water-supply-systems-verge-collapse-lebanon-over-71-cent-people-risk-losing-access (accessed on 27 February 2025).
- Fadlallah, S.M.; Shehab, M.; Cheaito, K.; Haidar-Ahmad, N.; El Hafi, B.; Saleh, M.; Matar, G.M. PulseNet Lebanon: An overview of its ACTIVITIES, Outbreak investigations, and challenges. Foodborne Pathog. Dis. 2019, 16, 503. Available online: https://www.liebertpub.com/doi/10.1089/fpd.2018.2581 (accessed on 27 February 2025). [CrossRef]
- Finger, J.; Baroni, W.; Maffei, D.; Bastos, D.; Pinto, U. Overview of foodborne disease outbreaks in Brazil from 2000 to 2018. Foods 2019, 8, 434. Available online: https://www.mdpi.com/2304-8158/8/10/434/htm (accessed on 16 October 2021). [CrossRef]
- European Food Safety Authority (EFSA). The European Union Summary report on trends and sources of zoonoses, zoonotic agents and foodborne outbreaks in 2009. Sci. Rep. EFSA ECDC Eur. Food Saf. Auth. J. 2011, 9, 287. [Google Scholar]
- Hassan, H.F.; Dimassi, H. Food Safety and handling knowledge and practices of Lebanese University students. Food Control. Elsevier 2013, 40, 127–133. Available online: https://www.sciencedirect.com/science/article/pii/S0956713513006221 (accessed on 16 October 2021). [CrossRef]
- Hassan, H.F.; Dimassi, H.; Karam, Z.N. Self-reported food safety knowledge and practices of Lebanese food handlers in Lebanese households. Br. Food J. 2018, 120, 518–530. [Google Scholar] [CrossRef]
- Caswell, J.A. Individual, household, and environmental factors affecting food choices and access. In Supplemental Nutrition Assistance Program: Examining the Evidence to Define Benefit Adequacy; The National Academy of Sciences: Washington, DC, USA, 2013. Available online: https://www.ncbi.nlm.nih.gov/books/NBK206912/ (accessed on 17 October 2021).
- Faour-Klingbeil, D. The Microbiological Safety of Fresh Produce in Lebanon—A HOLISTIC “FARM-TO-FORK Chain” Approach to Evaluate Food Safety, Compliance Levels and Underlying Risk Factors. Ph.D. Thesis, University of Plymouth, Plymouth, UK, 2017. Available online: https://pearl.plymouth.ac.uk/bms-theses/156/ (accessed on 27 February 2025).
- Ministry of Environment Lebanon State of the Environment Report. 2001. Available online: http://www.studies.gov.lb/getattachment/Sectors/Environment/2002/ENV-02-7/ENV-02-7.pdf (accessed on 27 February 2025).
- Faour-Klingbeil, D.; Murtada, M.; Kuri, V.; Todd, E.C.D. Understanding the routes of contamination of ready-to-eat vegetables in the Middle East. Food Control 2015, 62, 125–133. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0956713515302462?via=ihub (accessed on 16 October 2021). [CrossRef]
- El-Jardali, F.; Hammoud, R.; Kamleh, R.; Jurdi, M. K2P Briefing Note: Protecting Consumers in Lebanon: The Need for Effective Food Safety System; Knowledge to Policy (K2P) Center: Beirut, Lebanon, 2014. [Google Scholar]
- Ghaida, T.A.; Spinnler, H.E.; Soyeux, Y.; Hamieh, T.; Medawar, S. Risk-based food safety and quality governance at the international law, EU, USA, Canada, and France: Effective system for Lebanon as for the WTO accession. Food Control 2014, 44, 267–282. Available online: https://www.sciencedirect.com/science/article/pii/S0956713514001480 (accessed on 16 October 2021). [CrossRef]
- Kosa, K.M.; Cates, S.C.; Godwin, S.L.; Coppings, R.J.; Speller-Henderson, L. Most Americans are not prepared to ensure food safety during power outagesand other emergencies. Int. Assoc. Food Prot. 2011, 31, 428–436. Available online: http://www.foodprotection.org/files/food-protection-trends/Jul-11-Kosa.pdf (accessed on 15 April 2022).
- MoPH. Ministry of Public Health. Home Page. 2021. Available online: https://www.moph.gov.lb/en/Pages/127/54446/hasan-chairs-a-meeting-of-thehigher-health-council-to-ensure-food-safety-amid-power-cuts (accessed on 17 October 2021).
- Sample Size Calculator. Available online: https://cdn.who.int/media/docs/default-source/ncds/ncd-surveillance/steps/sample-size-calculator.xls?sfvrsn=ee1f4ae8_2 (accessed on 16 October 2021).
- El Haddad, R.; Yahfoufi, N.; Abou Haidar, M.; Hoteit, M. View of knowledge, attitude and practices of Lebanese married women towards food safety. Atena J. Public Health 2020, 2, 1. [Google Scholar]
- USDA. United States Department of Agriculture. Are You and Your Food Prepared for a Power Outage? 2017. Available online: https://www.usda.gov/about-usda/news/blog/are-you-and-your-food-prepared-power-outage (accessed on 27 February 2025).
- Centers for Disease Control and Prevention. Food Safety for Power Outages. 2020. Available online: https://www.cdc.gov/food-safety/foods/keep-food-safe-after-emergency.html (accessed on 1 March 2023).
- FoodSafety.gov. Food Safety During Power Outage. 2021. Available online: https://www.foodsafety.gov/food-safety-charts/food-safety-during-power-outage#:~:text=Discard%20refrigerated%20perishable%20food%20such,after%204%20hours%20without%20power. (accessed on 27 February 2025).
- Soares, L.; Almeida, R.; Cerqueira, E.; Carvalho, J.; Nunes, I. Knowledge, attitudes, and practices in food safety and the presence of coagulasepositive staphylococci on hands of food handlers in the schools of Camacari, Brazil. Food Control 2012, 27, 206–213. Available online: https://www.sciencedirect.com/science/article/pii/S0956713512001442?via%3Dihub (accessed on 11 April 2022). [CrossRef]
- Gong, S.; Wang, X.; Yang, Y.; Bai, L. Knowledge of food safety and handling in households: A survey of food handlers in Mainland Chinaa. Food Control 2015, 64, 45–53. Available online: https://www.sciencedirect.com/science/article/pii/S0956713515303194 (accessed on 11 April 2022). [CrossRef]
- Mkhungo, M.C.; Oyedeji, A.B.; Ijabadeniyi, O.A. Food safety knowledge and microbiological hygiene of households in selected areas of KwaZulu Natal, South Africa. Ital. J. Food Saf. 2018, 7, 6887. Available online: https://pubmed.ncbi.nlm.nih.gov/30046551/ (accessed on 17 April 2022).
- Jevsnik, M.; Hlebec, V.; Raspor, P. Consumer’s awareness of food safety from shopping to eating. Food Control 2007, 19, 737–745. Available online: https://www.sciencedirect.com/science/article/pii/S0956713507001569 (accessed on 11 April 2022). [CrossRef]
- Faour-Klingbeil, D.; Faour-Klingbeil, D. Microbiological quality of ready-toeat fresh vegetables and their link to food safety environment and handling practices in restaurants in Lebanon. LWT 2016, 74, 224–233. [Google Scholar] [CrossRef]
- Zeratsky, K. How long can you keep leftovers? Mayo Found. Med. Educ. Res. 2020. Available online: https://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/expert-answers/food-safety/faq-20058500 (accessed on 27 February 2025).
- Centers for Disease Control and Prevention. Food Poisoning Symptoms. 2021. Available online: https://www.cdc.gov/food-safety/signs-symptoms/index.html (accessed on 27 February 2025).
- Centers for Disease Control and Prevention. Four Steps to Food Safety. 2022. Available online: https://www.cdc.gov/foodsafety/challenges/ (accessed on 16 October 2021).
- Alsayeqh, A.F. Foodborne disease risk factors among women in Riyadh, Saudi Arabia. Food Control 2014, 50, 85–91. Available online: https://www.sciencedirect.com/science/article/abs/pii/S095671351400485X (accessed on 11 April 2022). [CrossRef]
- Australian Institute of Food Safety. Can Vegans Get Food Poisoning? 2019. Available online: https://www.foodsafety.com.au/blog/can-vegans-get-food-poisoning (accessed on 16 October 2021).
- Food and Drug Administration. Cooking from Food Safety for Moms to be. Center for Food Safety and Applied Nutrition. 2018. Available online: https://www.fda.gov/food/people-risk-foodborne-illness/food-safety-moms-be-glance (accessed on 27 February 2025).
- Bahn, R.; Yehya, A.A.; Zurayk, R. Lebanon Food Security Portal—Food Security Brief#25; American University of Beirut: Beirut, Lebanon, 2022; Available online: https://aub.edu.lb/fafs/foodsecurity/Documents/2022-04-19(Lebanon-Food-Security-Portal-Food-Security-Brief-25).pdf (accessed on 27 February 2025).
- Lee, H.K.; Abdul Halim, H.; Thong, K.L.; Chai, L.C.; Tchounwou, P.B. Assessment of food safety knowledge, attitude, self-reported practices, and microbiological hand hygiene of food handlers. Int. J. Environ. Res. Public Health 2017, 14, 55. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5295306/ (accessed on 16 October 2021). [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Frequency (n) Percentage (%) | |
|---|---|---|
| Age | 18–29 30–39 40–49 50–59 60 and more | 300 (52.5%) 156 (27.3%) 65 (11.4%) 38 (6.7%) 12 (2.1%) |
Gender Marital Status Governorate of Lebanon Nationality Educational Level Total Household Income How Do You Rate Your Food Safety Knowledge? | Female Male Single Married Divorced, Widowed, and Separated Mount Lebanon Beirut South North Bekaa Lebanese Non-Lebanese School Certificate University Bachelor Master/PhD Technical School Less than LBP 1,000,000 LBP 1,000,000–5,000,000 LBP 5,000,000–10,000,000 More than LBP 10,000,000 Excellent Good Weak | 348 (60.9%) 223 (39.1%) 328 (57.4%) 222 (38.9%) 21 (3.8%) 279 (48.9%) 165 (28.9%) 56 (9.8%) 48 (8.4%) 23 (4.0%) 524 (91.8%) 47 (8.2%) 140 (24.5%) 270 (47.3%) 134 (23.5%) 27 (4.7%) 13 (2.3%) 131 (22.9%) 186 (32.6%) 241 (42.2%) 95 (16.6%) 389 (68.1%) 87 (15.2%) |
| Question Statement | Variables | Frequency (n) Percentage (%) |
|---|---|---|
| Are you the primary food handler in your household? | Yes No | 262 (45.9%) 309 (54.1%) |
| Are you involved in food preparation at your house? | Yes No | 415 (72.7%) 156 (27.3%) |
| How many hours per day do you experience electricity cut-off at your house? | I don’t experience electricity cut-off Less than 2 h 2–4 h More than 4 h | 34 (6.0%) 23 (4.0%) 76 (13.3% 438 (76.7%) |
| How often do you check the temperature of your fridge/freezer? | Once/day Twice/day More than 3 times/day I don’t check it | 126 (22.1%) 60 (10.5%) 46 (8.1%) 339 (59.4%) |
| Did you experience diarrhea, vomiting, fever, or abdominal pain in the past 6 months? | Yes No | 309 (54.1%) 262 (45.9%) |
| Have you been hospitalized because of food poisoning in the past 6 months? | Yes No | 79 (13.8%) 492 (86.2%) |
| Do you know anyone (other than yourself) who got food poisoning in the past 6 months? | Yes No | 373 (65.3%) 198 (34.7%) |
| How do you usually eat your meat? | Well-done Medium-rare Rare I don’t eat meat | 342 (59.9%) 167 (29.2%) 39 (6.8%) 23 (4.0%) |
| With the electricity cutoff and with the increase in food poisoning cases in Lebanon, did you shift from ordering medium-rare meat to order well-done meat? | Yes No | 372 (65.1%) 199 (34.9%) |
| What food are you afraid the most to eat from outside your house (restaurant) during the electricity cut-off? | Burgers/sandwiches Sushi Salads Everything Nothing | 49 (8.6%) 207 (36.3%) 47 (8.2%) 182 (31.9%) 86 (15.1%) |
| Did the electricity cuts change your perishable food (foods that need a refrigerator: meat, chicken, dairy) storage habits? | Yes No | 424 (74.3%) 147 (25.7%) |
| Question Statement | Correct Answer | Wrong Answer |
|---|---|---|
| Do you know that foodborne pathogens can multiply on food that was not refrigerated? Food poisoning can happen as a result of consuming contaminated food on the same day or the day before only If the smell and color of food seem okay, that means the food is not contaminated Storing raw chicken in the fridge without proper precaution can contaminate other food What is the optimal temperature of frozen food? What is the optimal temperature of fridge? Is freezing enough to eliminate foodborne bacteria and viruses? Choose the best way to reduce the risk of contaminated food (cooking, washing the food, refrigeration, I don’t know) | 69.9% (399) 34.9% (199) 58.3% (333) 71.5% (408) 43.3% (247) 48.7% (278) 59.5% (340) 59.2% (338) | 30.1% (172) 65.1% (372) 41.7% (238) 28.5% (163) 56.7% (324) 51.3% (293) 40.5% (231) 40.8% (233) |
| Question Statement | Response | Frequency (n) Percentage (%) |
|---|---|---|
| Do you know what Escherichia coli is? Do you know what Campylobacter is? Do you know what Listeria is? Do you know what Salmonella is? Do you know what Staphylococcus aureus is? | Yes No Yes No Yes No Yes No Yes No | 207 (36.3%) 364 (63.7%) 119 (20.8%) 452 (79.2%) 172 (30.1%) 399 (69.9%) 479 (83.9%) 92 (16.1%) 204 (35.7%) 367 (64.3%) |
| Question Statement | Correct Answer | Wrong Answer |
|---|---|---|
| During a long electricity cut-off, for how long do you think the fridge will keep the food safely cool? During a long electricity cut-off, for how long do you think a full-packed freezer will keep the food safely frozen? During a long electricity cut-off, for how long do you think a half-packed freezer will keep the food safely frozen? How do you know if food is cooked enough? | 44.8% (256) 25.2% (144) 46.2% (264) 34.7% (198) | 55.2 (315) 74.8% (427) 53.8% (307) 65.3% (373) |
| Question Statement | Response | Frequency (n) Percentage (%) |
|---|---|---|
| During the electricity crises, did you limit your visits to restaurants for fear of getting food poisoning? | Yes No | 407 (71.3%) 164 (28.7%) |
| During the electricity crises, did you strictly eat at home because you know that food has been safely stored (frozen/refrigerated)? | Yes No | 326 (57.1%) 245 (42.9%) |
| In the electricity crises, for purchasing high-risk food (dairy, meat, chicken, fish), do you use big chain supermarkets instead of small local grocery stores since they are safer? | Yes No | 410 (71.8%) 161 (28.2%) |
| Do you believe that being vegan or vegetarian now in Lebanon will reduce the chance of getting food poisoning? | Yes No | 309 (54.1%) 262 (45.9%) |
| Question Statement | Response | Frequency (n) Percentage (%) |
|---|---|---|
| After the economic crisis and electricity shortages, did you reduce your purchasing of certain food (meat, chicken, fish, cheese, milk)? Have you ever eaten food that was not refrigerated properly because you had no other food? Have you ever eaten food that was not refrigerated properly because you don’t like to throw food away? During electricity cut-off, do you take the temperature of food inside fridge/freezer? | Yes No Yes No Yes No Yes No | 468 (82%) 103 (18%) 158 (27.7%) 413 (72.3%) 215 (37.7%) 356 (62.3%) 116 (20.3%) 455 (79.7%) |
| Question Statement | Correct Answer | Wrong Answer |
|---|---|---|
| After preparing and cooking the food that you will eat 3–4 h later, what do you usually do? During extended electricity cut-off (more than 4 h), do you discard or keep leftover cooked meals inside fridge? During extended electricity cut-off (more than 4 h), do you discard or keep raw chicken/meat inside fridge? During extended electricity cut-off (more than 4 h), do you discard or keep soft cheeses inside fridge? During extended electricity cut-off (more than 4 h), do you discard or keep hard cheeses inside fridge? During extended electricity cut-off (more than 4 h), do you discard or keep cut vegetables inside fridge? During extended electricity cut-off (more than 4 h), do you discard or keep uncut vegetables inside fridge? During extended electricity cut-off (more than 4 h), do you discard or keep thawed meat/chicken without ice crystals inside freezer? | 42.2% (241) 44.8% (256) 61.5% (351) 45.9% (262) 72.3% (413) 29.8% (170) 94.6% (540) 62.7% (358) | 57.8 (330) 55.2% (315) 38.5% (220) 54.1% (309) 27.7% (158) 70.2% (401) 5.4% (31) 37.3% (213) |
| Knowledge | Belief | Practice | ||||
|---|---|---|---|---|---|---|
| Simple Logistic Regression OR, (95% CI), p-Value | Multiple Logistic Regression OR, (95% CI), p-Value | Simple Logistic Regression OR, (95% CI), p-Value | Multiple Logistic Regression OR, (95% CI), p-Value | Simple Logistic Regression OR, (95% CI), p-Value | Multiple Logistic Regression OR, (95% CI), p-Value | |
| Gender Female Male | 1 1.217 (0.867, 1.710), p = 0.256 | 1 0.823 (0.536, 1.264), p = 0.374 | 1 0.899 (0.557, 1.451), p = 0.662 | |||
| Age 18–29 30–39 40–49 50–59 60+ | 1 0.884 (0.597, 1.310), p = 0.539 0.491 (0.285, 0.844), p = 0.010 * 0.232 (0.108, 0.494), p < 0.001 * 0.648 (0.204, 2.058), p = 0.462 | 1 0.993 (0.602, 1.639), p = 0.980 0.579 (0.292, 1.147), p = 0.117 0.242 (0.094, 0.621), p = 0.003 * 0.725 (0.199,2.634), p = 0.625 | 1 1.067 (0.669, 1.701), p = 0.786 0.518 (0.235, 1.140), p = 0.102 0.691 (0.277, 1.726), p = 0.429 0.000 (0.000), p = 0.999 | 1 0.608 (0.342, 1.079) p = 0.089 0.749 (0.349, 1.608) p = 0.458 0.259 (0.060, 1.109) p = 0.069 0.932, (0.198, 4.378) p = 0.929 | ||
| Governorate of Lebanon Beirut South North Mount Lebanon Bekaa | 1 0.333 (0.173, 0.642), p = 0.001 * 0.500 (0.258, 0.967), p = 0.039 * 1.589 (1.072, 2.355), p = 0.021 * 0.536 (0.220, 1.307), p = 0.170 | 1 0.588 (0.277, 1.249), p = 0.167 0.542 (0.240, 1.221), p = 0.139 1.889 (1.201, 2.974), p = 0.006 * 0.640 (0.226, 1.811), p = 0.400 | 1 0.693 (0.298, 1.608), p = 0.393 0.831 (0.355, 1.948), p = 0.671 1.212 (0.752, 1.954), p = 0.429 0.396 (0.088, 1.776), p = 0.226 | 1 0.605 (0.219, 1.676), p = 0.334 1.625 (0.713, 3.704), p = 0.248 1.125 (0.651, 1.945), p = 0.673 0.926 (0.255,3.368), p = 0.907 | ||
| Educational level School Bachelor’s Degree Master/PhD Technical School Nationality Lebanese Non-Lebanese | 1 1.592 (1.054, 2.405), p = 0.027 * 3.322 (2.015, 5.478), p < 0.001 * 4.948 (1.880, 13.022), p = 0.001 * 1 0.471 (0.255, 0.869), p = 0.016 * | 1 1.107 (0.662, 1.851), p = 0.699 2.390 (1.282, 4.455), p = 0.006 * 3.069 (1.012, 9.310), p = 0.048 * 1 0.733 (0.351, 1.533), p = 0.409 | 1 2.120 (1.168, 3.849), p = 0.013 * 2.635 (1.376, 5.047), p = 0.003 * 1.761 (0.585, 5.301), p = 0.314 1 1.264 (0.622, 2.569), p = 0.517 | 1 2.104 (1.139, 3.886), p = 0.017 * 2.510 (1.273, 4.949), p = 0.008 * 1.396 (0.447, 4.361), p = 0.566 | 1 0.783 (0.443, 1.382), p = 0.398 0.892 (0.465, 1.714), p = 0.732 1.156 (0.397, 3.367), p = 0.790 1 0.837 (0.344, 2.037), p = 0.695 | |
| Household Income >LBP 10,000,000 LBP 5,000,000–10,000,000 LBP 1,000,000–5,000,000 <LBP 1000,000 | 1 1.404 (0.954, 2.065), p = 0.085 1.556 (1.009, 2.398), p = 0.045 * 0.850 (0.278, 2.603), p = 0.776 | 1 1.212 (0.745, 1.972), p = 0.439 1.024 (0.593, 1.767) p = 0.932 0.764 (0.199, 2.940), p = 0.696 | 1 1.340 (0.829, 2.166), p = 0.233 1.173 (0.681, 2.020), p = 0.564 2.106 (0.619, 7.161), p = 0.233 | 1 1.718 (0.984, 3.000), p = 0.057 1.855 (1.017, 3.384), p = 0.044 * 1.503 (0.316, 7.159), p = 0.609 | 1 1.344 (0.748, 2.417), p = 0.323 1.276 (0.677, 2.406), p = 0.451 1.311 (0.265, 6.489), p = 0.740 | |
| Knowledge Rating Excellent Good Weak | 1 0.182 (0.096, 0.345), p < 0.001 * 0.033 (0.014, 0.073), p < 0.001 * | 1 0.228 (0.112, 0.463), p < 0.001 * 0.049 (0.020, 0.121), p < 0.001 | 1 0.836 (0.493, 1.419), p = 0.507 0.317 (0.133, 0.753), p = 0.009 * | 1 1.258 (0.705,2.247), p = 0.437 0.582 (0.229, 1.481), p = 0.256 | 1 0.487 (0.283, 0.839), p = 0.010 * 0.180 (0.065, 0.498), p = 0.001 * | 1 0.711 (0.397, 1.275), p = 0.253 0.350 (0.120, 1.022), p = 0.055 |
| Are You The Primary Food Handler In Your Household? Yes No Checking the Temperature of Fridge/Freezer I don’t check it Once/day Twice/day >3 times/day Total Hours Of Electricity Cut-Off Experienced Per Day In Households: >4 h 2–4 h <2 h I Don’t Experience Electricity Cut-off | 1 1.409 (1.011, 1.963), p = 0.043 * 1 2.043 (1.343, 3.109), p = 0.001 * 3.075 (1.686, 5.608), p < 0.001 * 9.969 (3.845, 25.847), p < 0.001 * - | 1 1.296 (0.837, 2.008), p = 0.246 1 1.712 (1.045, 2.805), p = 0.033 * 1.539 (0.763, 3.106), p = 0.229 5.135 (1.803, 14.625), p = 0.002 * - | 1 0.993 (0.657, 1.501), p = 0.975 1 1.278 (0.756, 2.159), p = 0.359 2.989 (1.642, 5.443), p < 0.001 * 1.623 (0.777, 3.389), p = 0.198 1 2.034 (1.185, 3.492), p = 0.010 * 0.420 (0.096, 1.826), p = 0.247 0.944 (0.379, 2.356), p = 0.902 | 1 1.191 (0.693, 2.049), p = 0.527 2.951 (1.535, 5.674), p = 0.001 * 2.095 (0.925, 4.746), p = 0.076 1 1.963 (1.111, 3.469), p = 0.020 * 0.342 (0.077, 1.526), p = 0.160 0.912 (0.360,2.315), p = 0.847 | 1 0.975 (0.613, 1.551), p = 0.914 1 2.515 (1.401, 4.516), p = 0.002 * 4.226 (2.145, 8.328), p < 0.001 * 4.677 (2.244, 9.747), p < 0.001 * - | 1 2.177 (1.193, 3.972), p = 0.011 * 3.247 (1.576, 6.692), p = 0.001 * 3.437 (1.579, 7.480), p = 0.002 * |
| Total (n = 571) | Poor Practices n (%) | Good Practices n (%) | Significance; OR (CI) | Poor Beliefs n (%) | Good Beliefs n (%) | Significance; OR (CI) | |
|---|---|---|---|---|---|---|---|
| Bad Knowledge | 255 | 227 (89%) | 28 (11%) | 0.024 *; 1.746 (1.073; 2.843) | 221 (86.7%) | 34 (13.3%) | 0.001 *; 2.167 (1.393; 3.37) |
| Good Knowledge | 316 | 260 (82.3%) | 56 (17.7%) | 237 (75%) | 79 (25%) | ||
| Bad Practices | 487 | 400 (82.1%) | 87 (17.9%) | 0.005 *; 2.061 (1.228; 3.458) | |||
| Good Practices | 84 | 58 (69%) | 26 (31%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subuh, N.; Ballout, R.; Toufeili, I.; Kassem, I.I.; Kharroubi, S.A. Beliefs, Practices, and Knowledge of Household Food Handlers Regarding the Impact of Electricity Outages on Food Safety: Findings from a National Cross-Sectional Study in Lebanon. Foods 2025, 14, 855. https://doi.org/10.3390/foods14050855
Subuh N, Ballout R, Toufeili I, Kassem II, Kharroubi SA. Beliefs, Practices, and Knowledge of Household Food Handlers Regarding the Impact of Electricity Outages on Food Safety: Findings from a National Cross-Sectional Study in Lebanon. Foods. 2025; 14(5):855. https://doi.org/10.3390/foods14050855
Chicago/Turabian StyleSubuh, Noura, Rouba Ballout, Imad Toufeili, Issmat I. Kassem, and Samer A. Kharroubi. 2025. "Beliefs, Practices, and Knowledge of Household Food Handlers Regarding the Impact of Electricity Outages on Food Safety: Findings from a National Cross-Sectional Study in Lebanon" Foods 14, no. 5: 855. https://doi.org/10.3390/foods14050855
APA StyleSubuh, N., Ballout, R., Toufeili, I., Kassem, I. I., & Kharroubi, S. A. (2025). Beliefs, Practices, and Knowledge of Household Food Handlers Regarding the Impact of Electricity Outages on Food Safety: Findings from a National Cross-Sectional Study in Lebanon. Foods, 14(5), 855. https://doi.org/10.3390/foods14050855