

Cutaneous Involvement of Extranodal NK/T Cell Lymphoma, Nasal Type, a Clinical and Histopathological Mimicker of Various Skin Diseases

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Materials and Histopathological Criteria
2.2. Immunohistochemical Study and Epstein–Barr-Virus-Encoded Small RNA (EBER) In Situ Hybridization (ISH)
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
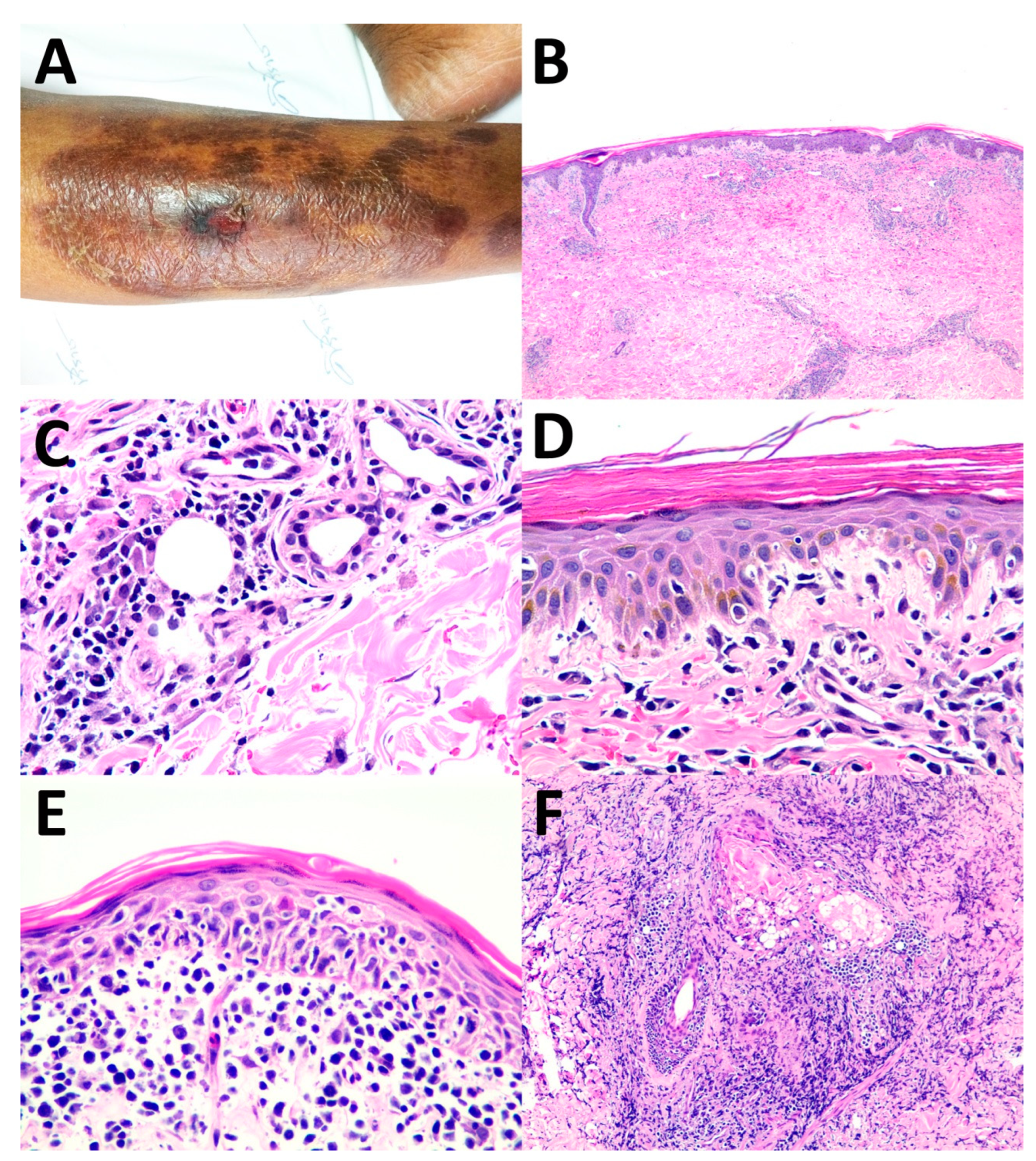
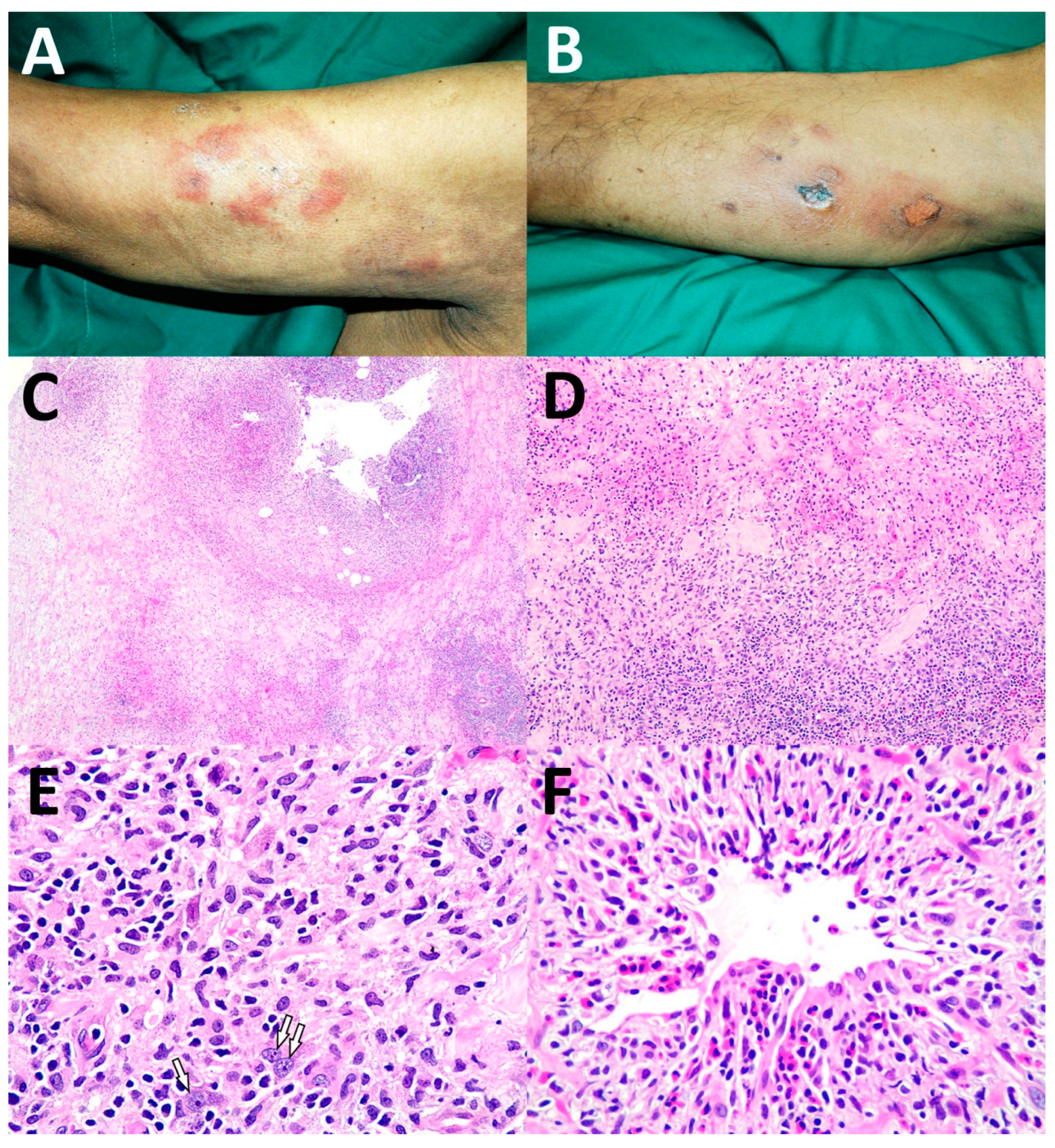
3.2. Histopathology, Immunohistochemistry, and EBER ISH
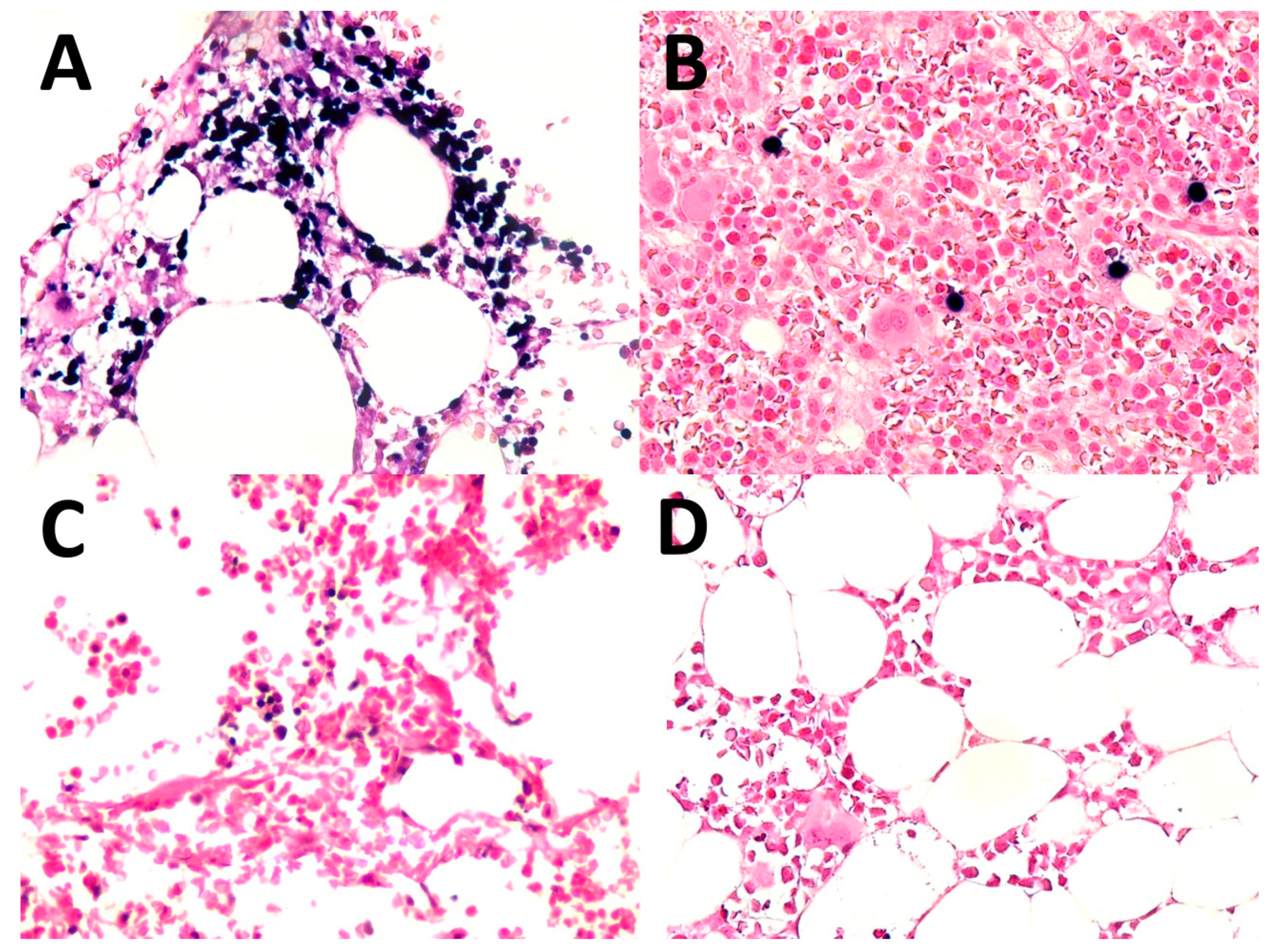
3.3. Bone Marrow Status
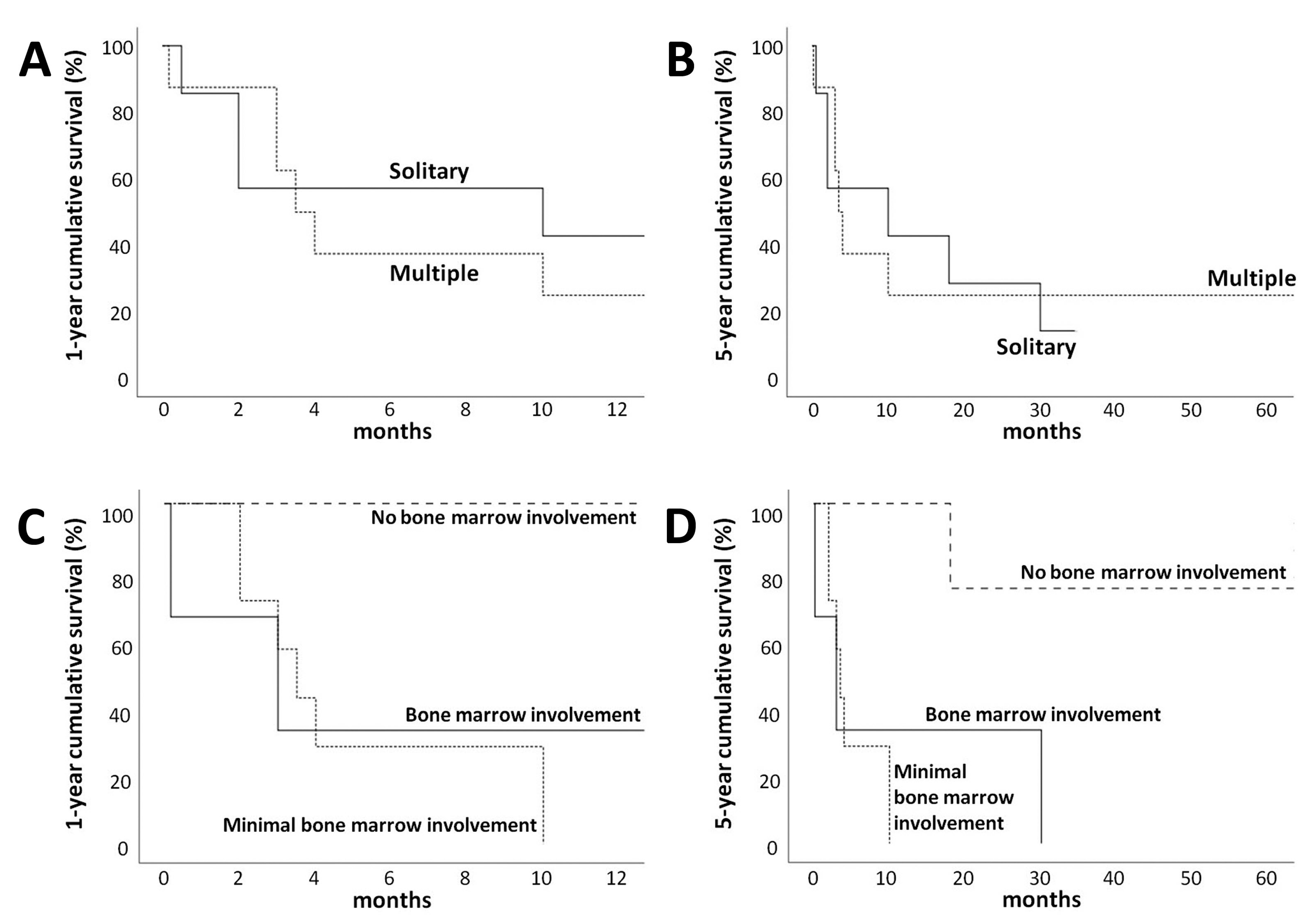
3.4. Treatment and Survival Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Elder, D.E.; Massi, D.; Scolyer, R.A.; Willemze, R. WHO Classification of Skin Tumours, 4th ed.; International Agency for Research on Cancer: Lyon, France, 2018; pp. 245–246. [Google Scholar]
- Assaf, C.; Gellrich, S.; Whittaker, S.; Robson, A.; Cerroni, L.; Massone, C.; Kerl, H.; Rose, C.; Chott, A.; Chimenti, S.; et al. CD56-positive haematological neoplasms of the skin: A multicentre study of the Cutaneous Lymphoma Project Group of the European Organisation for Research and Treatment of Cancer. J. Clin. Pathol. 2007, 60, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Chow, K.F.; Ritchie, E.; Husain, S.; Alobeid, B.; Bhagat, G. Lethal T- and NK-cell lymphomas mimicking granulomatous panniculitidies: A clinicopathologic study of three cases. J. Cutan. Pathol. 2011, 38, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, N.; Takahashi, T.; Yamashita, M.; Nakanishi, G.; Okabe, H.; Tanaka, T. Extranodal natural killer/T-cell lymphoma, nasal type, with prominent granulomatous reaction. J. Dermatol. 2014, 41, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Sitthinamsuwan, P.; Pongpruttipan, T.; Chularojmontri, L.; Pattanaprichakul, P.; Khuhapinant, A.; Sukpanichnant, S. Extranodal NK/T cell lymphoma, nasal type, presenting with primary cutaneous lesion mimicking granulomatous panniculitis: A case report and review of literature. J. Med. Assoc. Thai. 2010, 93, 1001–1007. [Google Scholar] [PubMed]
- Yamashita, Y.; Tsuzuki, T.; Nakayama, A.; Fujino, M.; Mori, N. A case of natural killer/T cell lymphoma of the subcutis resembling subcutaneous panniculitis-like T cell lymphoma. Pathol. Int. 1999, 49, 241–246. [Google Scholar] [CrossRef]
- Massone, C.; Chott, A.; Metze, D.; Kerl, K.; Citarella, L.; Vale, E.; Helmut, K.; Cerroni, L. Subcutaneous, blastic natural killer (NK), NK/T-cell, and other cytotoxic lymphomas of the skin: A morphologic, immunophenotypic, and molecular study of 50 patients. Am. J. Surg. Pathol. 2004, 28, 719–735. [Google Scholar] [CrossRef] [PubMed]
- Soylu, S.; Gul, U.; Kilic, A.; Heper, A.O.; Kuzu, I.; Minareci, B.G. A case with an indolent course of subcutaneous panniculitis-like T-cell lymphoma demonstrating Epstein-Barr virus positivity and simulating dermatitis artefacta. Am. J. Clin. Dermatol. 2010, 11, 147–150. [Google Scholar] [CrossRef]
- Yang, S.J.; Ng, C.Y.; Yang, C.H.; Lu, P.H. Doubly Dangerous: Extranodal NK/T-Cell Lymphoma. Am. J. Med. 2017, 130, 669–672. [Google Scholar] [CrossRef]
- Gill, H.; Liang, R.H.; Tse, E. Extranodal natural-killer/t-cell lymphoma, nasal type. Adv. Hematol. 2010, 2010, 627401. [Google Scholar] [CrossRef]
- Au, W.Y. Current management of nasal NK/T-cell lymphoma. Oncology (Williston Park) 2010, 24, 352–358. [Google Scholar]
- Tse, E.; Kwong, Y.L. Diagnosis and management of extranodal NK/T cell lymphoma nasal type. Expert Rev. Hematol. 2016, 9, 861–871. [Google Scholar] [CrossRef] [PubMed]
- Berti, E.; Recalcati, S.; Girgenti, V.; Fanoni, D.; Venegoni, L.; Vezzoli, P. Cutaneous extranodal NK/T-cell lymphoma: A clinicopathologic study of 5 patients with array-based comparative genomic hybridization. Blood 2010, 116, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, T.; Yoshino, T.; Takehisa, T.; Hagari, Y.; Mihara, M. Cutaneous presentation of nasal/nasal type T/NK cell lymphoma: Clinicopathological findings of four cases. Br. J. Dermatol. 1998, 139, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Charli-Joseph, Y.V.; Gatica-Torres, M.; Pincus, L.B. Approach to Cutaneous Lymphoid Infiltrates: When to Consider Lymphoma? Indian J. Dermatol. 2016, 61, 351–374. [Google Scholar] [CrossRef]
- Pongpruttipan, T.; Sukpanichnant, S.; Assanasen, T.; Wannakrairot, P.; Boonsakan, P.; Kanoksil, W.; Kayasut, K.; Mitarnun, W.; Khuhapinant, A.; Bunworasate, U.; et al. Extranodal NK/T-cell Lymphoma, Nasal Type, Includes Cases of Natural Killer Cell and αβ, γδ, and αβ/γδ T-cell Origin: A Comprehensive Clinicopathologic and Phenotypic Study. Am. J. Surg. Pathol. 2012, 36, 481–499. [Google Scholar] [CrossRef]
- Stoll, J.R.; Willner, J.; Oh, Y.; Pulitzer, M.; Moskowitz, A.; Horwitz, S.; Myskowski, P.; Noor, S.J. Primary cutaneous T-cell lymphoma other than mycosis fungoides and Sezary syndrome. Part I: Clinical and histologic features and diagnosis. J. Am. Acad. Dermatol. 2021, 85, 1073–1090. [Google Scholar] [CrossRef]
- Gallardo, F.; Garcia-Muret, M.P.; Servitje, O.; EstraMoskoch, T.; Bielsa, I.; Salar, A.; Abella, E.; Barranco, C.; Pujol, R.M. Cutaneous lymphomas showing prominent granulomatous component: Clinicopathological features in a series of 16 cases. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 639–647. [Google Scholar] [CrossRef]
- Ma, L.; Bandarchi, B.; Glusac, E.J. Fatal subcutaneous panniculitis-like T-cell lymphoma with interface change and dermal mucin, a dead ringer for lupus erythematosus. J. Cutan. Pathol. 2005, 32, 360–365. [Google Scholar] [CrossRef]
- Aguilera, P.; Mascaro, J.M.; Martinez, A.; Esteve, J.; Puig, S.; Campo, E.; Estrach, T. Cutaneous gamma/delta T-cell lymphoma: A histopathologic mimicker of lupus erythematosus profundus (lupus panniculitis). J. Am. Acad. Dermatol. 2007, 56, 643–647. [Google Scholar] [CrossRef]
- Larocca, C.; Larocca, C. Mycosis Fungoides and Sézary Syndrome: An Update. Hematol. Oncol. Clin. N. Am. 2019, 33, 103–120. [Google Scholar] [CrossRef]
- Geller, S.; Myskowski, P.L.; Pulitzer, M. NK/T-cell lymphoma, nasal type, γδ T-cell lymphoma, and CD8-positive epidermotropic T-cell lymphoma—Clinical and histopathologic features, differential diagnosis, and treatment. Semin. Cutan. Med. Surg. 2018, 37, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Suh, C.; Huh, J.; Jun, H.J.; Kim, K.; Jung, C.; Park, K.; Park, Y.H.; Ko, Y.H.; Kim, W.S. Effect of positive bone marrow EBV in situ hybridization in staging and survival of localized extranodal natural killer/T-cell lymphoma, nasal-type. Clin. Cancer Res. 2007, 13, 3250–3254. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Analyzed Cases | ||
|---|---|---|---|
| Age in years, median (range) | 22 | 52 (25–87) | |
| Sex, n (%) | 22 | ||
| Male | 15 (68.2) | ||
| Female | 7 (31.8) | ||
| Presenting symptoms a, n (%) | 17 | ||
| Fever | 7 (41.2) | ||
| Mass or nodule | 4 (23.5) | ||
| Nasal congestion | 2 (11.8) | ||
| Skin lesion | 2 (11.8) | ||
| Orbital cellulitis | 2 (11.8) | ||
| Others | 4 (23.5) | ||
| B symptoms, n (%) | 17 | 8 (47.1) | |
| Cutaneous ulcer, n (%) | 17 | 4 (23.5) | |
| Visceral organ involvement b, n (%) | 17 | 6 (35.3) | |
| Bone marrow involvement, n (%) | 17 | 5 (29.4) | |
| Treatment response, n (%) | 14 | ||
| Complete remission | 8 (57.1) | ||
| Partial remission | 4 (28.6) | ||
| No response | 2 (14.3) | ||
| Relapse, n (%) | 8 | 6 (75.0) | |
| 1-year survival, n (%) | 16 c | 5 (31.3) | |
| 5-year survival, n (%) | 15 d | 2 (13.3) | |
| Case No. | Type | Distribution | Lesion | Location | Cutaneous Presentation | Histopathological Pattern |
|---|---|---|---|---|---|---|
| 1 | Secondary | Localized | Solitary | Hand, left | Ulcer | Dermal and subcutaneous nodular infiltration pattern |
| 2 | Secondary | Localized | Solitary | Upper eyelid | Cellulitis-like | Dermal and subcutaneous nodular infiltration pattern |
| 3 | Secondary | Generalized | Multiple | Extremities | Subcutaneous nodules | Dermal and subcutaneous nodular infiltration pattern |
| 4 | Secondary | Generalized | Multiple | Eyebrow, chin, and chest | Subcutaneous nodules | Dermal and subcutaneous nodular infiltration pattern |
| 5 | Secondary | Generalized | Multiple | Trunk and back | Plaques patches | Dermal nodular infiltration pattern |
| Periorbital | Cellulitis-like | Dermal nodular infiltration pattern | ||||
| 6 | Secondary | Generalized | Multiple | Arm, right | Dermal nodules | Dermal nodular infiltration pattern |
| 7 | Secondary | Localized | Solitary | Abdomen | Subcutaneous nodule | Lobular panniculitis pattern |
| 8 | Secondary | Localized | Solitary | Nasolabial fold | Skin nodule | Lobular panniculitis pattern |
| 9 | Secondary | Generalized | Multiple | Extremities | Plaques and subcutaneous nodules | Lobular panniculitis pattern |
| 10 | Secondary | Localized | Multiple | Leg, right | Papules and plaques | Interface dermatitis pattern |
| 11 | Secondary | Generalized | Multiple | Trunk and face | Papules | Interface dermatitis pattern |
| 12 | Secondary | Generalized | Multiple | Thighs and abdomen | Subcutaneous nodules | Granulomatous dermatitis pattern |
| 13 | Unclassified | Localized | Solitary | Shoulder, right | Skin nodule | Dermal and subcutaneous nodular infiltration pattern |
| 14 | Unclassified | Generalized | Multiple | Trunk, upper and lower extremities | Skin nodules | Dermal and subcutaneous nodular infiltration pattern |
| 15 | Unclassified | Generalized | Multiple | Upper and lower extremities | Nodules | Dermal and subcutaneous nodular infiltration pattern |
| 16 | Unclassified | Localized | Solitary | Arm, right | Cellulitis-like | Lobular panniculitis pattern |
| 17 | Unclassified | Localized | Solitary | Abdomen | Subcutaneous nodule | Lobular panniculitis pattern |
| Case No. | Tumor Necrosis | Vascular Invasion | Epidermotropism | Tumor Cell Size | CD3 | CD4 | CD5 | CD8 | CD20 | CD30 | CD56 | TIA-1 | BetaF1 | TCR-γ | EBER |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dermal/Subcutaneous nodular and diffuse infiltration pattern | |||||||||||||||
| 1 | + | + | + | M to L | + | - | NA | - | - | NA | - | + | - | - | + |
| 2 | - | - | - | M to L | + | NA | NA | NA | NA | NA | - | + | NA | NA | + |
| 3 | + | + | - | Mto L | + # | NA | - | - | NA | + * | + | + | NA | NA | + |
| 4 | - | + | - | M to L | + | - | + * | - | - | + | + | + | - | NA | + |
| 5 | - | - | - | M to L | + | - | - | - | - | + * | + # | + | NA | NA | + |
| 6 | - | + | + | L | + | - | - | - | - | + * | + | + | - | - | + |
| 13 | - | - | - | L | + | - | - | - | - | NA | + # | + | - | - | + |
| 14 | - | - | + | S to M | + | - | - | - | - | + * | + | + | - | NA | + |
| 15 | + | + | - | L | + | - | - | - | - | + * | + | + | - | NA | + |
| X1 | + | + | - | L | + | NA | - | NA | - | + | + | + | - | NA | + |
| X2 | + | - | - | L | + | - | - | - | - | NA | + | + | - | NA | + |
| Lobular panniculitis pattern | |||||||||||||||
| 7 | + | + | - | M to L | + | NA | - | NA | - | NA | + | + | NA | NA | + |
| 8 | + | - | + | M with L | + | + | + | + | - | NA | + * | + | + * | + | + |
| 9 | + | + | - | L | + | - | NA | - | - | + | + | + | NA | - | + |
| 16 | - | + | + | S, M, L | + | - | NA | + | - | - | + | + | + | - | + |
| 17 | + | + | - | M to L | + | NA | NA | NA | - | NA | + | + | + | NA | + |
| X3 | + | + | - | M to L | + | - | NA | NA | - | + * | + | + | NA | NA | + |
| Interface dermatitis pattern | |||||||||||||||
| 10 | - | + | + | M to L | + | - | + | - | NA | + * | + | + | NA | NA | + |
| 11 | - | + | + | L | + | - | - | - | - | + | + # | + | NA | NA | + |
| X4 | - | - | + | S to M | + | - | NA | - | - | NA | + | + | NA | - | + |
| X5 | + | + | + | M to L | + | - | - | - | - | + | + | + | - | NA | + |
| Granulomatous dermatitis pattern | |||||||||||||||
| 12 | + | + | - | L | + | - | - | + | - | + | + | + | NA | NA | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngamdamrongkiat, P.; Sukpanichnant, S.; Chairatchaneeboon, M.; Khuhapinant, A.; Sitthinamsuwan, P. Cutaneous Involvement of Extranodal NK/T Cell Lymphoma, Nasal Type, a Clinical and Histopathological Mimicker of Various Skin Diseases. Dermatopathology 2022, 9, 307-320. https://doi.org/10.3390/dermatopathology9030037
Ngamdamrongkiat P, Sukpanichnant S, Chairatchaneeboon M, Khuhapinant A, Sitthinamsuwan P. Cutaneous Involvement of Extranodal NK/T Cell Lymphoma, Nasal Type, a Clinical and Histopathological Mimicker of Various Skin Diseases. Dermatopathology. 2022; 9(3):307-320. https://doi.org/10.3390/dermatopathology9030037
Chicago/Turabian StyleNgamdamrongkiat, Preeyawat, Sanya Sukpanichnant, Manasmon Chairatchaneeboon, Archrob Khuhapinant, and Panitta Sitthinamsuwan. 2022. "Cutaneous Involvement of Extranodal NK/T Cell Lymphoma, Nasal Type, a Clinical and Histopathological Mimicker of Various Skin Diseases" Dermatopathology 9, no. 3: 307-320. https://doi.org/10.3390/dermatopathology9030037
APA StyleNgamdamrongkiat, P., Sukpanichnant, S., Chairatchaneeboon, M., Khuhapinant, A., & Sitthinamsuwan, P. (2022). Cutaneous Involvement of Extranodal NK/T Cell Lymphoma, Nasal Type, a Clinical and Histopathological Mimicker of Various Skin Diseases. Dermatopathology, 9(3), 307-320. https://doi.org/10.3390/dermatopathology9030037