
Incidence, Predictors and Outcomes of Noninvasive Ventilation Failure in Very Preterm Infants



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Outcomes and Variables
2.2. Respiratory Management
2.3. Statistical Analysis
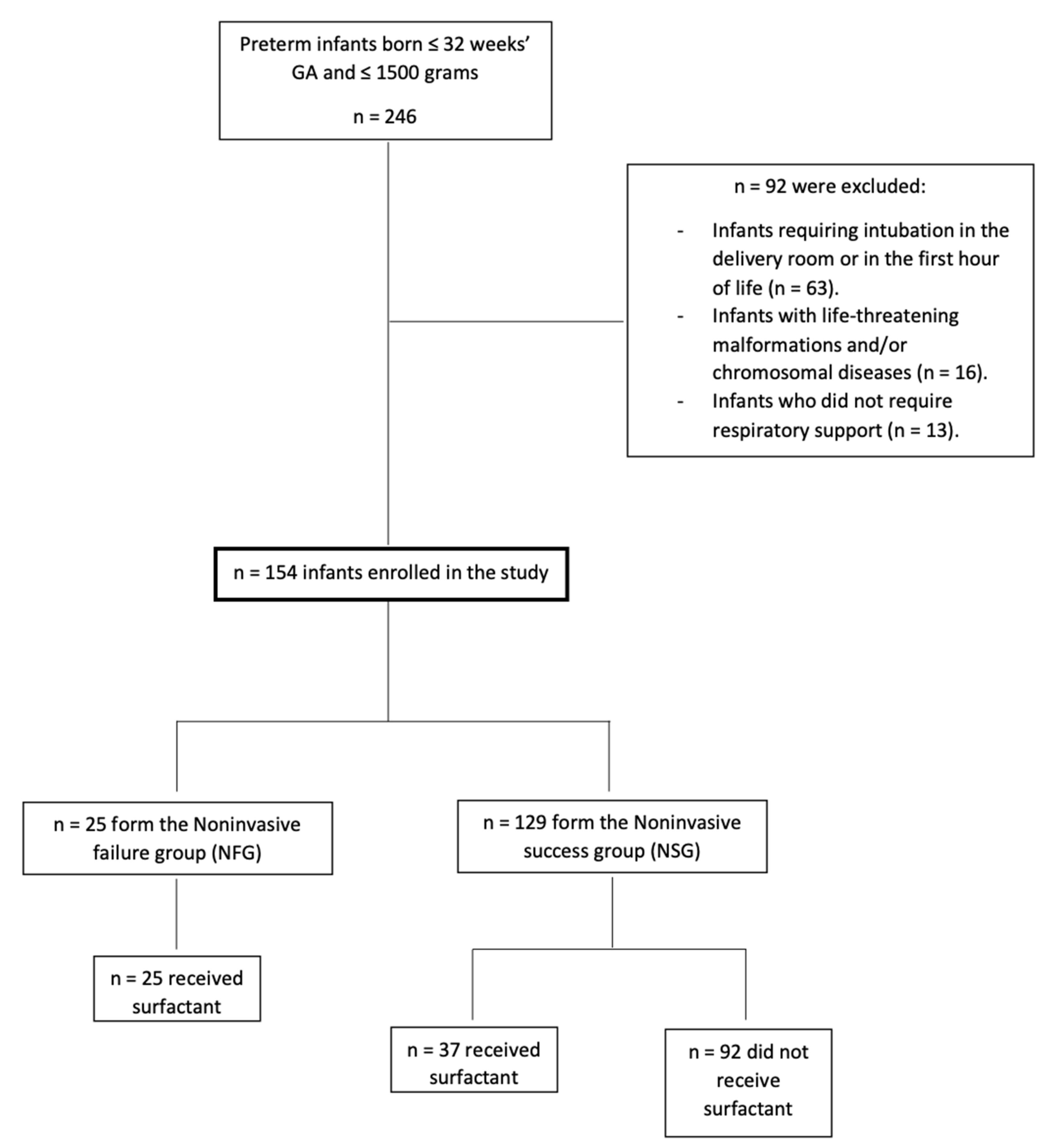
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sardesai, S.; Biniwale, M.; Wertheimer, F.; Garingo, A.; Ramanathan, R. Evolution of surfactant therapy for respiratory distress syndrome: Past, present, and future. Pediatr. Res. 2017, 81, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Dargaville, P.A.; Gerber, A.; Johansson, S.; De Paoli, A.G.; Kamlin, C.O.F.; Orsini, F.; Davis, P.G. Incidence and Outcome of CPAP Failure in Preterm Infants. Pediatrics 2016, 138, e20153985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, C.T.; Owen, L.S.; Frøisland, D.H.; Doyle, L.W.; Davis, P.G.; Manley, B.J. Predictors and Outcomes of Early Intubation in Infants Born at 28-36 Weeks of Gestation Receiving Noninvasive Respiratory Support. J. Pediatr. 2020, 216, 109–116.e1. [Google Scholar] [CrossRef] [PubMed]
- Fischer, H.S.; Bührer, C. Avoiding endotracheal ventilation to prevent bronchopulmonary dysplasia: A meta-analysis. Pediatrics 2013, 132, e1351–e1360. [Google Scholar] [CrossRef] [Green Version]
- Carlo, W.A.; Polin, R.A.; Papile, L.A.; Tan, R.; Kumar, P.; Benitz, W.; Eichenwald, E.; Cummings, J.; Baley, J. Respiratory support in preterm infants at birth. Pediatrics 2014, 133, 171–174. [Google Scholar] [CrossRef] [Green Version]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef] [Green Version]
- Avila-Alvarez, A.; Zozaya, C.; Pértega-Diaz, S.; Sanchez-Luna, M.; Iriondo-Sanz, M.; Elorza, M.D.; García-Muñoz Rodrigo, F. Temporal trends in respiratory care and bronchopulmonary dysplasia in very preterm infants over a 10-year period in Spain. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 107, 143–149. [Google Scholar] [CrossRef]
- Aguar, M.; Cernada, M.; Brugada, M.; Gimeno, A.; Gutierrez, A.; Vento, M. Minimally invasive surfactant therapy with a gastric tube is as effective as the intubation, surfactant, and extubation technique in preterm babies. Acta Paediatr. 2014, 103, e229–e233. [Google Scholar] [CrossRef]
- Dargaville, P.A.; Aiyappan, A.; De Paoli, A.G.; Dalton, R.G.B.; Kuschel, C.A.; Kamlin, C.O.; Orsini, F.; Carlin, J.B.; Davis, P.G. Continuous positive airway pressure failure in preterm infants: Incidence, predictors and consequences. Neonatology 2013, 104, 8–14. [Google Scholar] [CrossRef]
- Gulczyńska, E.; Szczapa, T.; Hożejowski, R.; Borszewska-Kornacka, M.K.; Rutkowska, M. Fraction of Inspired Oxygen as a Predictor of CPAP Failure in Preterm Infants with Respiratory Distress Syndrome: A Prospective Multicenter Study. Neonatology 2019, 116, 171–178. [Google Scholar] [CrossRef]
- Bancalari, E.; Claure, N. Definitions and diagnostic criteria for bronchopulmonary dysplasia. Semin. Perinatol. 2006, 30, 164–170. [Google Scholar] [CrossRef] [PubMed]
- De Luca, D.; Autilio, C.; Pezza, L.; Shankar-Aguilera, S.; Tingay, D.G.; Carnielli, V. Personalized Medicine for the Management of RDS in Preterm Neonates. Neonatology 2021, 118, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Thébaud, B.; Goss, K.N.; Laughon, M.; Whitsett, J.A.; Abman, S.H.; Steinhorn, R.H.; Aschner, J.L.; Davis, P.G.; McGrath-Morrow, S.A.; Soll, R.F.; et al. Bronchopulmonary dysplasia. Nat. Rev. Dis. Prim. 2019, 5, 78. [Google Scholar] [CrossRef]
- Gregory, K.E.; Deforge, C.E.; Natale, K.M.; Phillips, M.V.M.L. Necrotizing enterocolitis in the premature infant: Neonatal nursing assessment, disease pathogenesis, and clinical presentation. Adv. Neonatal. Care 2011, 11, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Volpe, J.J. Perinatal brain injury: From pathogenesis to neuroprotection. Ment. Retard. Dev. Disabil. Res. Rev. 2001, 7, 56–64. [Google Scholar] [CrossRef]
- Castro Conde, J.R.; Echániz Urcelay, I.; Botet Mussons, F.; Pallás Alonso, C.R.; Narbona, E.; Sánchez Luna, M. Retinopathy of prematurity. Prevention, screening and treatment guidelines. An. Pediatr. 2009, 71, 514–523. [Google Scholar] [CrossRef]
- Zeballos Sarrato, G.; Salguero García, E.; Aguayo Maldonado, J.; Gómez Robles, C.; Thió Lluch, M.; Iriondo Sanz, M. Adaptación de las recomendaciones internacionales en estabilización y reanimación neonatal 2015. Anal. Pediatría 2017, 86, 51.e1–51.e9. [Google Scholar] [CrossRef]
- Rademaker, K.J.; Uiterwaal, C.S.P.M.; Groenendaal, F.; Venema, M.M.A.T.U.; van Bel, F.; Beek, F.J.; van Haastert, I.C.; Grobbee, D.E.; de Vries, L.S. Neonatal Hydrocortisone Treatment: Neurodevelopmental Outcome and MRI at School Age in Preterm-born Children. J. Pediatr. 2007, 150, 351–357. [Google Scholar] [CrossRef]
- Kakkilaya, V.; Jubran, I.; Mashruwala, V.; Ramon, E.; Simcik, V.N.; Marshall, M.; Brown, L.S.; Jaleel, M.A.; Kapadia, V.S. Quality improvement project to decrease delivery room intubations in preterm infants. Pediatrics 2019, 143, e20180201. [Google Scholar] [CrossRef] [Green Version]
- Raschetti, R.; Centorrino, R.; Letamendia, E.; Benachi, A.; Marfaing-Koka, A.; De Luca, D. Estimation of early life endogenous surfactant pool and CPAP failure in preterm neonates with RDS. Respir. Res. 2019, 20, 75. [Google Scholar] [CrossRef]
- Álvarez-Fuente, M.; Arruza, L.; Muro, M.; Zozaya, C.; Avila, A.; López-Ortego, P.; González-Armengod, C.; Torrent, A.; Gavilán, J.L.; Del Cerro, M.J. The economic impact of prematurity and bronchopulmonary dysplasia. Eur. J. Pediatr. 2017, 176, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Isayama, T.; Iwami, H.; McDonald, S.; Beyene, J. Association of noninvasiveventilation strategies withmortality and bronchopulmonarydysplasiaamong preterm infants: A systematic review and meta-analysis. JAMA J. Am. Med. Assoc. 2016, 316, 611–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sucasas Alonso, A.; Pértega Díaz, S.; Sáez Soto, R.; Ávila-Álvarez, A. Epidemiología y factores de riesgo asociados a displasia broncopulmonar en prematuros menores de 32 semanas de edad gestacional. Anal. Pediatría 2021, S1695–4033, 00153-3. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W. Postnatal Corticosteroids to Prevent or Treat Bronchopulmonary Dysplasia. Neonatology 2021, 118, 244–251. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| ± DS .... | Total n = 154 | NSG n = 129 | NFG n = 25 | p-Value |
| Gestational age Birth weight Temperature at admission Apgar score at 1 min Apgar score at 5 min | 29.79 ± 2.00 | 30.09 ± 1.79 | 28.22 ± 2.33 | 0.001 |
| 1185 (960–1410) | 1200 (975–1420) | 1000 (860–1245) | 0.003 | |
| 35.86 ± 0.64 | 35.85 ± 0.61 | 35.92 ± 0.82 | 0.616 | |
| 6.97 ± 1.27 | 6.95 ± 1.18 | 7.04 ± 1.70 | 0.805 | |
| 8.29 ± 0.97 | 8.25 ± 0.93 | 8.48 ± 1.12 | 0.280 | |
| Maximum FiO2 during DR stabilization | 36.41 ± 15.39 | 31.61 ± 6.52 | 52.56 ± 23.79 | <0.001 |
| Age at surfactant administration (hours) n = 62 | 5.24 ± 9.16 | 6.27 ± 11.25 | 3.72 ± 4.43 | 0.287 |
| FiO2 before surfactant administration n = 62 | 33.49 ± 7.80 | 31.72 ± 6.08 | 36.33 ± 9.47 | 0.077 |
| FiO2 after surfactant n = 62 | 27.67 ± 9.41 | 24.35 ± 5.01 | 33.52 ± 12.27 | 0.003 |
| FiO2 decrease after surfactant n = 62 | 5.47 ± 7.37 | 7.13 ± 4.73 | 2.64 ± 10 | 0.097 |
| n (%) | Total n = 154 | NSG n = 129 | NFG n = 25 | p-Value |
| GA ≤ 28 | 48 (31,2) | 32 (24,8) | 16 (64) | <0.001 |
| IVF | 44 (28.6) | 35 (27.1) | 9 (36) | 0.468 |
| PIH | 41 (26.6) | 34 (26.4) | 7 (28) | 1 |
| Female infant | 76 (49.4) | 66 (51.2) | 10 (40) | 0.384 |
| ANS | 153 (99.4) | 128 (99.2) | 25 (100) | 1 |
| Multiple birth | 59 (38.3) | 47 (36.4) | 12 (48) | 0.369 |
| Cesarean section | 120 (77.9) | 101 (78.3) | 19 (76) | 1 |
| SGA | 17 (11) | 14 (10,9) | 3 (12) | 0.867 |
| Chorioamnionitis | 23 (14.9) | 17 (13.2) | 6 (24) | 0.220 |
| Surfactant | 62 (40.3) | 37 (28.7) | 25 (100) | <0.001 |
| NIPPV as initial support | 52 (33.8) | 38 (29.5) | 14 (56) | 0.032 |
| Caffeine | 145 (94.2) | 126 (97.7) | 19 (76) | <0.001 |
| n (%) | Total n = 154 | NSG n = 129 | NFG n = 25 | p-Value |
| Died | 10 (6.5) | 0 (0) | 10 (40) | <0.001 |
| BPD | 24 (15.6) | 16 (12.4) | 8 (32) | 0.022 |
| BPD moderate-to-severe | 7 (4.5) | 3 (2.3) | 4 (16) | 0.014 |
| Survival without BPD | 120 (77.9) | 113 (87.6) | 7 (28) | <0.001 |
| Survival without moderate-to-severe BPD | 137 (89) | 126 (97.7) | 11 (44) | <0.001 |
| Home supplementary oxygen | 10 (6.5) | 1 (0.8) | 9 (36) | <0.001 |
| IMV during admission | 35 (22.7) | 11 (8.5) | 25 (100) | <0.001 |
| Steroids for BPD | 11 (7.1) | 4 (3.1) | 7 (28) | <0.001 |
| Pneumothorax | 5 (3.2) | 1 (0.8) | 4 (16) | 0.002 |
| IVH > II | 11 (7.1) | 4 (3.1) | 7 (28) | <0.001 |
| PVL | 6 (3.9) | 4 (3.1) | 2 (8) | 0.250 |
| ROP > II | 5 (3.8) | 3 (2.5) | 2 (13.3) | 0.097 |
| PDA | 22 (14.3) | 17 (13.2) | 5 (20) | 0.532 |
| Surgery for PDA | 6 (3.9) | 4 (3.1) | 2 (8) | 0.251 |
| Ibuprofen for PDA | 13 (8.4) | 10 (7.8) | 3 (12) | 0.445 |
| NEC (≥ stage 2) | 7 (4.5) | 5 (3.9) | 2 (8) | 0.610 |
| Isolated intestinal perforation | 3 (1.9) | 0 (0) | 3 (12) | 0.004 |
| Culture positive sepsis | 46 (29.9) | 38 (29.5) | 8 (32) | 0.810 |
| ± DS | Total n = 154 | NSG n = 129 | NFG n = 25 | p-Value |
| Weight at discharge | 2256.21 ± 436.36 | 2313.13 ± 319.23 | 1925 ± 774.64 | 0.033 |
| Weight Z-Score at discharge | −1.49 ± 1.15 | −1.50 ± 1.19 | −1.38 ± 0.88 | 0.652 |
| Age at first intubation (hours) n = 35 | 42.85 ± 83.35 | 210 ± 124.52 | 13.78 ± 11.54 | 0.051 |
| Duration of hospitalization (days) * | 57.51 ± 63.57 | 56.91 ± 66.84 | 62.60 ± 21.35 | 0.744 |
| NICU length of stay (days) * | 21.79 ± 14.34 | 20.84 ± 13.45 | 29.80 ± 19.20 | 0.022 |
| MV (hours) * | 96 (34–216) | 72(36–168) | 96 (31–306) | 0.221 |
| NIV (hours) * | 96 (48v168) | 96 (48–168) | 72 (48–216) | 0.210 |
| Supplemental oxygen (hours) * | 192 (68–648) | 192 (72–564) | 120 (65–972) | 0.009 |
| Number of doses of surfactant | 1 (1–1.25) | 1 (1–1) | 1 (1–2) | 0.003 |
| Unadjusted | Adjusted by GA | Adjusted by GA, SGA, Sex, Postnatal Steroids ** | ||||
| OR | CI95% | OR | CI95% | OR | CI95% | |
| Birth weight * | 0.78 | 0.66–0.93 | 1.03 | 0.80–1.32 | 0.97 | 0.69–1.37 |
| NIPPV as initial support | 2.83 | 1.16–6.87 | 1.03 | 0.34–3.06 | 0.97 | 0.32–2.92 |
| Maximum FiO2 during DR stabilization | 1.15 | 1.08–1.23 | 1.14 | 1.06–1.22 | 1.15 | 1.07–1.24 |
| FiO2 after surfactant | 1.16 | 1.04–1.29 | 1.17 | 1.05–1.31 | 1.17 | 1.05–1.30 |
| Outcomes | ||||||
| BPD | 3.32 | 1.23–8.94 | 1.49 | 0.49–4.55 | 0.53 | 0.10–2.74 |
| Moderate-to-severe BPD | 8.00 | 1.67–38.3 | 6.07 | 1.07–34.4 | 3.77 | 0.61–23.1 |
| Survival without BPD | 0.05 | 0.02–0.15 | 0.07 | 0.02–0.25 | 0.08 | 0.02–0.32 |
| Survival without moderate-to-severe BPD | 0.01 | 0.00–0.07 | 0.02 | 0.00–0.12 | 0.02 | 0.00–0.11 |
| Home supplementary oxygen | 72.0 | 8.55–606.0 | 37.7 | 4.22–337.2 | 96.7 | 8.26–1131.5 |
| Pneumothorax | 24.3 | 2.59–228.8 | 20.2 | 2.01–204.7 | 17.8 | 1.65–192.9 |
| IVH > II | 12.1 | 3.23–45.6 | 5.43 | 1.31–22.4 | 6.22 | 1.36–28.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandez-Gonzalez, S.M.; Sucasas Alonso, A.; Ogando Martinez, A.; Avila-Alvarez, A. Incidence, Predictors and Outcomes of Noninvasive Ventilation Failure in Very Preterm Infants. Children 2022, 9, 426. https://doi.org/10.3390/children9030426
Fernandez-Gonzalez SM, Sucasas Alonso A, Ogando Martinez A, Avila-Alvarez A. Incidence, Predictors and Outcomes of Noninvasive Ventilation Failure in Very Preterm Infants. Children. 2022; 9(3):426. https://doi.org/10.3390/children9030426
Chicago/Turabian StyleFernandez-Gonzalez, Sara M., Andrea Sucasas Alonso, Alicia Ogando Martinez, and Alejandro Avila-Alvarez. 2022. "Incidence, Predictors and Outcomes of Noninvasive Ventilation Failure in Very Preterm Infants" Children 9, no. 3: 426. https://doi.org/10.3390/children9030426
APA StyleFernandez-Gonzalez, S. M., Sucasas Alonso, A., Ogando Martinez, A., & Avila-Alvarez, A. (2022). Incidence, Predictors and Outcomes of Noninvasive Ventilation Failure in Very Preterm Infants. Children, 9(3), 426. https://doi.org/10.3390/children9030426