
Constraint-Induced Movement Therapy Versus Bimanual Training to Improve Upper Limb Function in Cerebral Palsy: A Systematic Review and Meta-Analysis of Follow-Ups

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
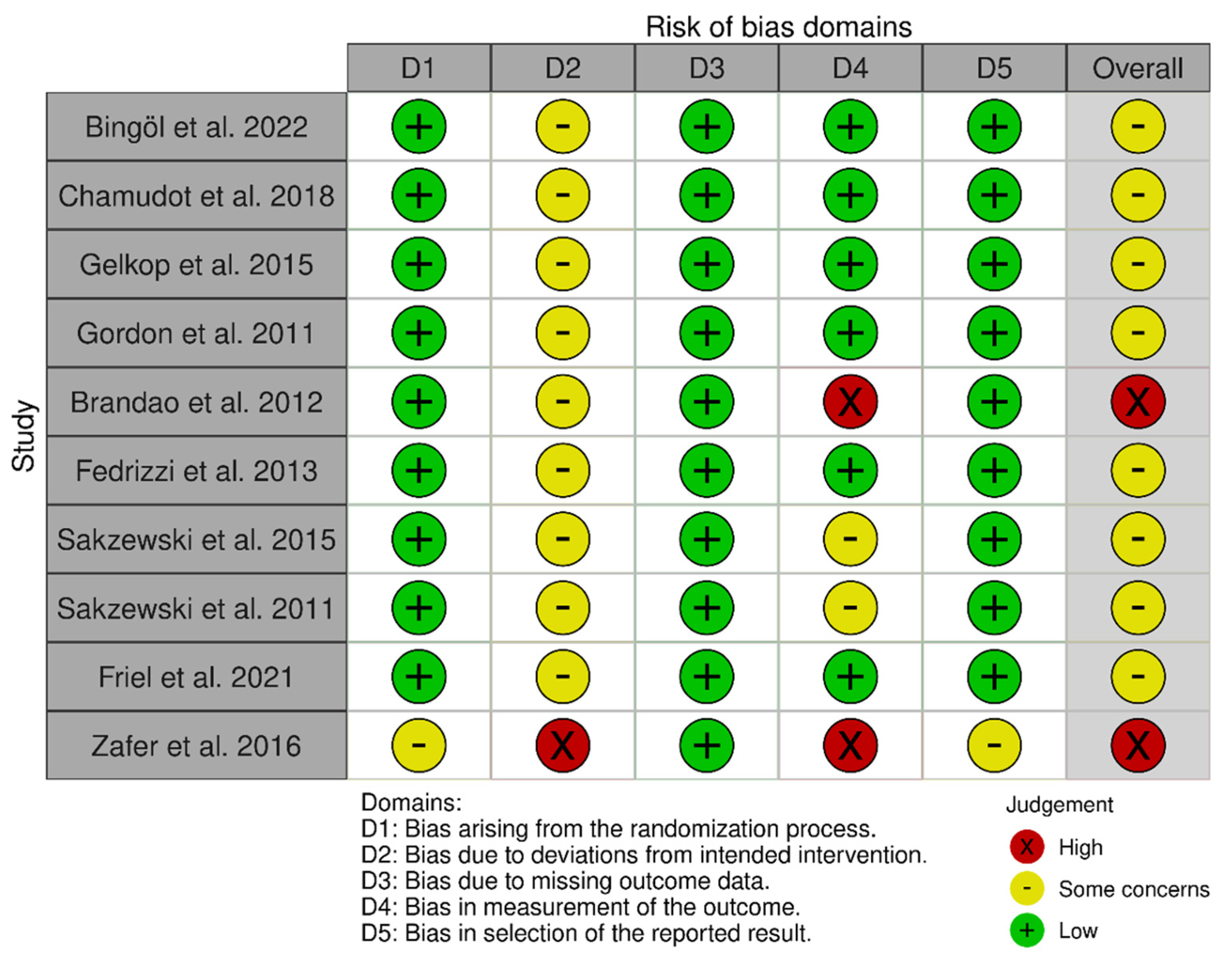
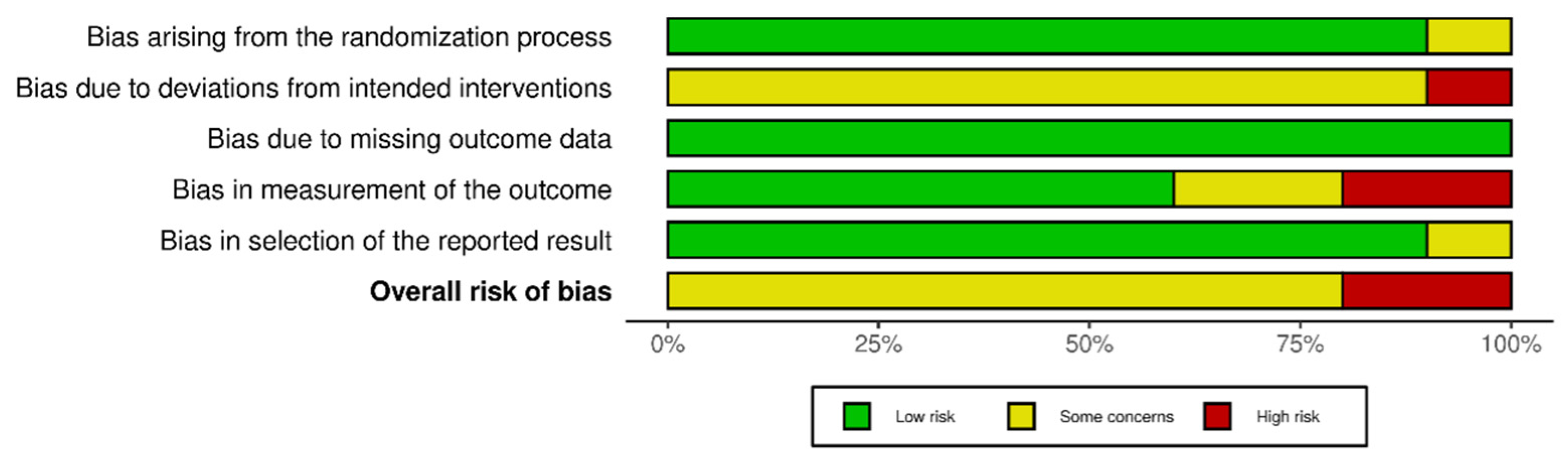
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Data Extraction
3.3. Risk of Bias Assessment
3.4. Synthesis of Results
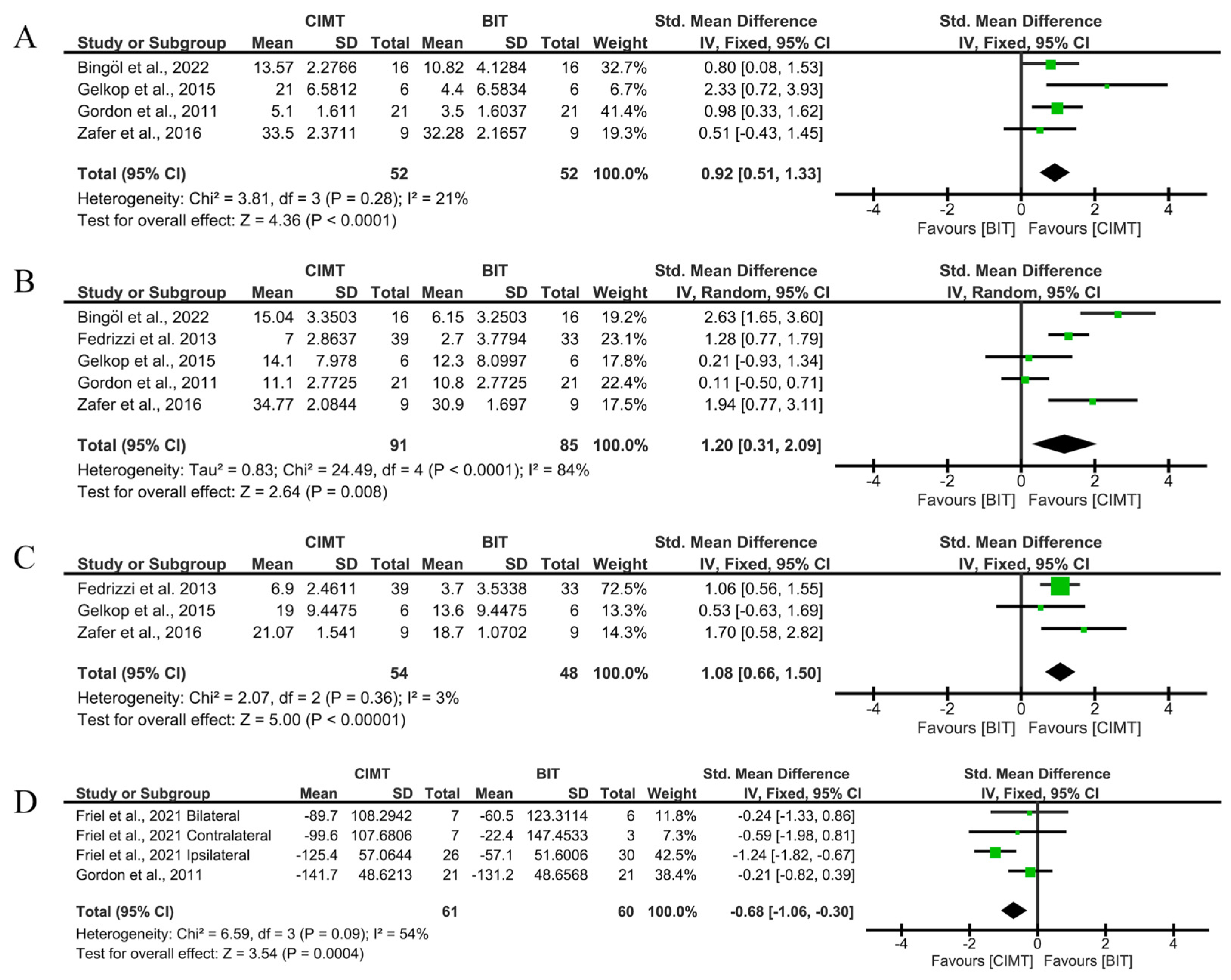
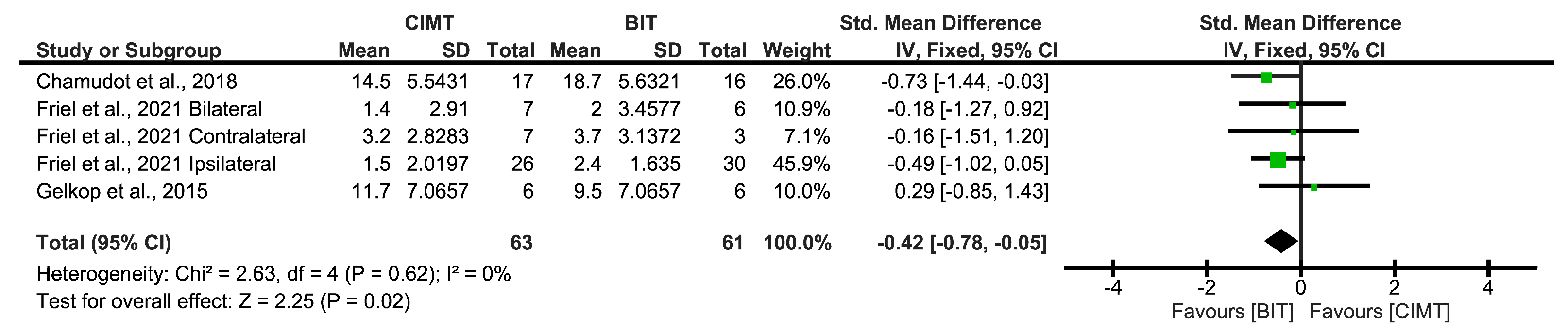
3.4.1. Immediate, Short-Term, and Long-Term Effects
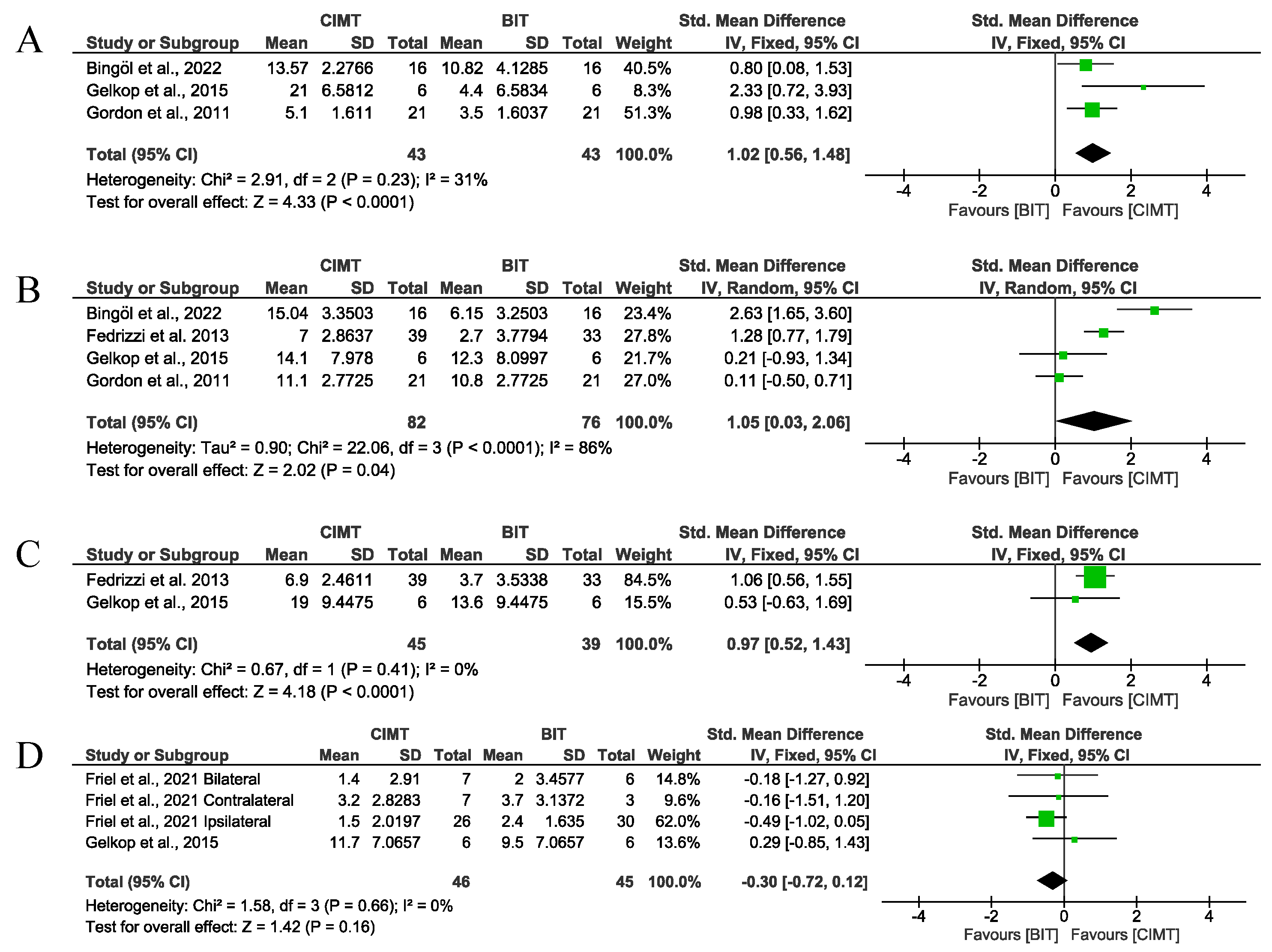
Immediate Term
- Unimanual upper limb function.
- Bimanual upper limb function.
- Occupational performance and disability.
Short Term
- Unimanual upper limb function.
- Bimanual upper limb function.
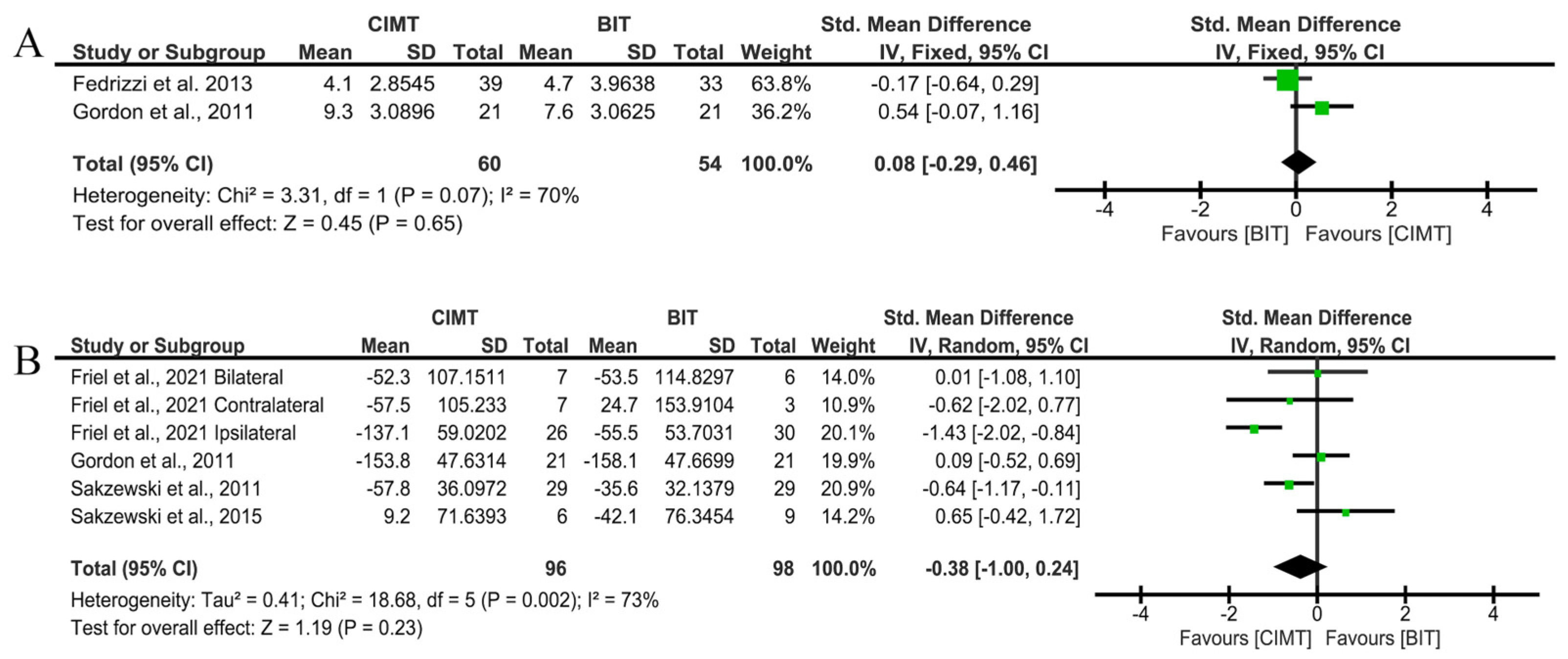
Long Term
- Unimanual upper limb function.
- Bimanual upper limb function.
3.4.2. Total Intervention Hours (>90)
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADL | Activities of daily living |
| AHA | Assisting Hand Assessment |
| BIT | Bimanual training |
| CIMT | Constraint-induced movement therapy |
| COPM | Canadian Occupational Performance Measure |
| CP | Cerebral palsy |
| HABIT | Hand–Arm Bimanual Intensive Training |
| JTHFT | Jebsen-Taylor Hand Function Test |
| mCIMT | Modified constraint-induced movement therapy |
| PEDI | Paediatric Evaluation of Disability Inventory |
| QUEST | Quality of Upper Extremity Test |
| RCT | Randomised controlled trial |
| ULF | Upper limb function |
References
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral palsy. Nat. Rev. Dis. Primers 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- Jackman, M.; Sakzewski, L.; Morgan, C.; Boyd, R.N.; Brennan, S.E.; Langdon, K.; Toovey, R.A.M.; Greaves, S.; Thorley, M.; Novak, I. Interventions to improve physical function for children and young people with cerebral palsy: International clinical practice guideline. Dev. Med. Child Neurol. 2022, 64, 536–549. [Google Scholar] [CrossRef] [PubMed]
- James, S.; Ziviani, J.; Ware, R.S.; Boyd, R.N. Randomized controlled trial of web-based multimodal therapy for unilateral cerebral palsy to improve occupational performance. Dev. Med. Child Neurol. 2015, 57, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.B.; Chatterji, S.; Bickenbach, J.; Kostanjsek, N.; Schneider, M. The International Classification of Functioning, Disability and Health: A new tool for understanding disability and health. Disabil. Rehabil. 2003, 25, 565–571. [Google Scholar] [CrossRef]
- Eliasson, A.C.; Krumlinde-Sundholm, L.; Gordon, A.M.; Feys, H.; Klingels, K.; Aarts, P.B.M.; Rameckers, E.; Autti-Rämö, I.; Hoare, B.; European network for Health Technology Assessment (EUnetHTA). Guidelines for future research in constraint-induced movement therapy for children with unilateral cerebral palsy: An expert consensus. Dev. Med. Child Neurol. 2014, 56, 125–137. [Google Scholar] [CrossRef]
- Hoare, B.J.; Wallen, M.A.; Thorley, M.N.; Jackman, M.L.; Carey, L.M.; Imms, C. Constraint-induced movement therapy in children with unilateral cerebral palsy. Cochrane Database Syst. Rev. 2019, 4, CD004149. [Google Scholar] [CrossRef]
- Charles, J.; Gordon, A.M. Development of hand-arm bimanual intensive training (HABIT) for improving bimanual coordination in children with hemiplegic cerebral palsy. Dev. Med. Child Neurol. 2006, 48, 931–936. [Google Scholar]
- Sakzewski, L.; Gordon, A.; Eliasson, A.C. The state of the evidence for intensive upper limb therapy approaches for children with unilateral cerebral palsy. J. Child Neurol. 2014, 29, 1077–1090. [Google Scholar] [CrossRef]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.M.; Paton, M.C.; Popat, H.; et al. State of the Evidence Traffic Lights 2019: Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef]
- Dong, V.A.Q.; Tung, I.H.H.; Siu, H.W.Y.; Fong, K.N.K. Studies comparing the efficacy of constraint-induced movement therapy and bimanual training in children with unilateral cerebral palsy: A systematic review. Dev. Neurorehabilit. 2013, 16, 133–143. [Google Scholar] [CrossRef]
- Tervahauta, M.; Girolami, G.; Øberg, G. Efficacy of constraint-induced movement therapy compared with bimanual intensive training in children with unilateral cerebral palsy: A systematic review. Clin. Rehabil. 2017, 31, 1445–1456. [Google Scholar] [CrossRef] [PubMed]
- Klepper, S.E.; Clayton Krasinski, D.; Gilb, M.C.; Khalil, N. Comparing Unimanual and Bimanual Training in Upper Extremity Function in Children with Unilateral Cerebral Palsy. Pediatr. Phys. Ther. 2017, 29, 288–306. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Charrois, T.L. Systematic Reviews: What Do You Need to Know to Get Started? Can. J. Hosp. Pharm. 2015, 68, 144–148. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmi, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; ACADEMIC PRESS, INC.: Cambridge, MA, USA, 1988. [Google Scholar]
- Higgins, J.P.T.; Green, S. Identifying and Measuring Heterogeneity. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration. 2011. Available online: https://training.cochrane.org/sites/training.cochrane.org/files/public/uploads/resources/Handbook5_1/Handbook4.2.6Sep2006.pdf (accessed on 12 June 2025).
- Gordon, A.M.; Hung, Y.C.; Brandao, M.; Ferre, C.L.; Kuo, H.C.; Friel, K.; Petra, E.; Chinnan, A.; Charles, J.R. Bimanual training and constraint-induced movement therapy in children with hemiplegic cerebral palsy: A randomized trial. Neurorehabilit. Neural Repair 2011, 25, 692–702. [Google Scholar] [CrossRef]
- Brandao, M.D.B.; Gordon, A.M.; Mancini, M.C. Functional Impact of Constraint Therapy and Bimanual Training in Children with Cerebral Palsy: A Randomized Controlled Trial. Am. J. Occup. Ther. 2012, 66, 672–681. [Google Scholar] [CrossRef]
- Sakzewski, L.; Provan, K.; Ziviani, J.; Boyd, R.N. Comparison of dosage of intensive upper limb therapy for children with unilateral cerebral palsy: How big should the therapy pill be? Res. Dev. Disabil. 2015, 37, 9–16. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Abbott, D.F.; MacDonell, R.A.L.; Jackson, G.D.; Boyd, R.N. Equivalent retention of gains at 1 year after training with constraint-induced or bimanual therapy in children with unilateral cerebral palsy. Neurorehabilit. Neural Repair 2011, 25, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Friel, K.M.; Ferre, C.L.; Brandao, M.; Kuo, H.C.; Chin, K.; Hung, Y.C.; Robert, M.T.; Flamand, V.H.; Smorenburg, A.; Bleyenheuft, Y.; et al. Improvements in Upper Extremity Function Following Intensive Training Are Independent of Corticospinal Tract Organization in Children With Unilateral Spastic Cerebral Palsy: A Clinical Randomized Trial. Front. Neurol 2021, 12, 660780. [Google Scholar] [CrossRef] [PubMed]
- Fedrizzi, E.; Rosa-Rizzotto, M.; Turconi, A.C.; Pagliano, E.; Fazzi, E.; Pozza, L.V.D.; Facchin, P.; GIPCI Study Group. Unimanual and bimanual intensive training in children with hemiplegic cerebral palsy and persistence in time of hand function improvement: 6-month follow-up results of a multisite clinical trial. J. Child Neurol. 2013, 28, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Zafer, H.; Amjad, I.; Malik, A.N.; Shaukat, E. Effectiveness of constraint induced movement therapy as compared to bimanual therapy in upper motor function outcome in child with hemiplegic cerebral palsy. Pak. J. Med. Sci. 2016, 32, 181–184. [Google Scholar]
- Bingöl, H.; Günel, M.K. Comparing the effects of modified constraint-induced movement therapy and bimanual training in children with hemiplegic cerebral palsy mainstreamed in regular school: A randomized controlled study. Arch. Pediatr. 2022, 29, 105–115. [Google Scholar] [CrossRef]
- Chamudot, R.; Parush, S.; Rigbi, A.; Horovitz, R.; Gross-Tsur, V. Effectiveness of modified constraint-induced movement therapy compared with bimanual therapy home programs for infants with hemiplegia: A randomized controlled trial. Am. J. Occup. Ther. 2018, 72, 7206205010. [Google Scholar] [CrossRef]
- Gelkop, N.; Burshtein, D.G.; Lahav, A.; Brezner, A.; Al-Oraibi, S.; Ferre, C.L.; Gordon, A.M. Efficacy of Constraint-Induced Movement Therapy and Bimanual Training in Children with Hemiplegic Cerebral Palsy in an Educational Setting. Phys. Occup. Ther. Pediatr. 2015, 35, 24–39. [Google Scholar] [CrossRef]
- Chen, H.C.; Chen, C.L.; Kang, L.J.; Wu, C.Y.; Chen, F.C.; Hong, W.H. Improvement of upper extremity motor control and function after home-based constraint induced therapy in children with unilateral cerebral palsy: Immediate and long-term effects. Arch. Phys. Med. Rehabil. 2014, 95, 1423–1432. [Google Scholar] [CrossRef]
- Hoare, B.J.; Imms, C.; Rawicki, H.B.; Carey, L. Modified constraint-induced movement therapy or bimanual occupational therapy following injection of Botulinum toxin-A to improve bimanual performance in young children with hemiplegic cerebral palsy: A randomised controlled trial methods paper. BMC Neurol. 2010, 10, 58. [Google Scholar] [CrossRef]
- Geerdink, Y.; Aarts, P.; Geurts, A.C. Motor learning curve and long-term effectiveness of modified constraint-induced movement therapy in children with unilateral cerebral palsy: A randomized controlled trial. Res. Dev. Disabil. 2013, 34, 923–931. [Google Scholar] [CrossRef]
- Gee, B.M.; Leonard, S.; Lloyd, K.G.; Gerber, L.D.; Quick, H.; Raschke, T.; Yardley, J.; Earl, J.D. Exploring the Intensity, Frequency, and Duration of Pediatric Constraint Induced Movement Therapy Published Research: A Content Analysis. Children 2022, 9, 700. [Google Scholar] [CrossRef]
- Sakzewski, L.; Ziviani, J.; Boyd, R. Systematic review and meta-analysis of therapeutic management of upper-limb dysfunction in children with congenital hemiplegia. Pediatrics 2009, 123, e1111–e1122. [Google Scholar] [CrossRef] [PubMed]
- Sterling, C.; Taub, E.; Davis, D.; Rickards, T.; Gauthier, L.V.; Griffin, A.; Uswatte, G. Structural Neuroplastic Change After Constraint-Induced Movement Therapy in Children With Cerebral Palsy. Pediatrics 2013, 131, e1664–e1669. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Khan, B.; Hervey, N.; Tian, F.; Delgado, M.R.; Clegg, N.J.; Smith, L.; Roberts, H.; Tulchin-Francis, K.; Alexandrakis, G. Evaluation of cortical plasticity in children with cerebral palsy undergoing constraint-induced movement therapy based on functional near-infrared spectroscopy. J. Biomed. Opt. 2015, 20, 046009. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.W.; Kang, Y.N.; Tseng, S.H. Effects of therapeutic exercise intensity on cerebral palsy outcomes: A systematic review with meta-regression of randomized clinical trials. Front. Neurol. 2019, 10, 657. [Google Scholar] [CrossRef]
- Miot, H.A. Sample size in clinical and experimental trials. J. Vasc. Bras. 2011, 10, 275–278. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Participants | Intervention Protocol (Duration and Frequency) | |||
|---|---|---|---|---|---|
| Total N Gender Proportion | Mean Age | PC Type | Unimanual | Bimanual | |
| Bingöl et al. [27], 2022 Turkey | N = 32 (16/16); Girls/boys: 15/17 | Age (years, months): 10.43 ± 2.9 | Spastic hemiplegia | mCIMT: restriction with glove, gross and fine motor tasks, and manipulation. 2.5 h/day; 3 days/week; 10 weeks + home: 1 h/day; 5 days/week; 10 weeks; 125 h. | BIT: gross motor tasks regarding bimanual coordination. 2.5 h/day; 3 days/week; 10 weeks + home: 1 h/day; 5 days/week; 10 weeks; 125 h. |
| Chamudot et al. [28], 2018 Israel | N = 33 (17/16); Girls/boys: 14/19 | Age (months): 11.1 ± 2.2 | Spastic hemiplegia | mCIMT: at home, restriction with glove, functional activities/tasks. 1 h/day; 7 days/week; 8 weeks; 46.7 h ± 9.9 | BIT: at home, symmetric and asymmetric bimanual tasks. 1 h/day; 7 days/week; 8 weeks; 46.7 h ± 9.9 |
| Gelkop et al. [29], 2015 Israel | N = 12 (6/6); Girls/boys: 10/2 | Unimanual group: 4.25 ± 1.58 Bimanual group: 4.33 ± 1.86 | Spastic hemiplegia | mCIMT: restriction with glove, gross and fine motor tasks, fragmented. 2 h/day (1 h individual/1 h group; 6 days/week; 8 weeks; 96 h | HABIT: gross and fine motor bimanual tasks. 2 h/day (1 h individual/1 h group; 6 days/week; 8 weeks; 96 h |
| Gordon et al. [20], 2011 USA | N = 42, (21/21); Girls/boys: 22/20 | Age (years, months) Unimanual group: 6.3 ± 2.2 Bimanual group: 6.4 ± 1.11 | Congenital hemiplegia | mCIMT: day camp, restriction with sling, gross and fine motor tasks. 6 h/day; 15 consecutive days; 90 h | HABIT: gross and fine symmetric and asymmetric motor tasks. 6 h/day; 15 consecutive days; 90 h |
| Brandao et al. [21], 2012 Brazil | N = 16 (8/8); Girls/boys: 6/10 | Age (years, months) Unimanual group: 6.11 ± 2.12 Bimanual group: 6.55 ± 2.13 | Hemiplegia | mCIMT: day camp, restriction with sling, gross and fine motor tasks. 6 h/day; 15 consecutive days; 90 h | HABIT: gross and fine symmetric and asymmetric motor tasks. 6 h/day; 15 consecutive days; 90 h |
| Fedrizzi et al. [25], 2013 Italy | N = 105 (39/33/33) | Age (years, months): 4 ± 8 | Hemiplegia | CIMT: restriction with glove and plastic splint, manipulation, grasp, balance, and functional tasks. 3 h/day; 3 days/week; 10 weeks; 90 h | BIT: bimanual manipulation, grasp, balance, and functional tasks. 3 h/day; 3 days/week; 10 weeks; 90 h |
| Sakzewski et al. [22], 2015 Australia | N = 17 (8/9) | Age (years, months) Unimanual group: 8.5 ± 1.5 Bimanual group: 8.9 ± 1.5 | Spastic hemiplegia | mCIMT: group, day camp, restriction with glove and splint, gross and fine motor tasks, functional activities, and games. 6 h/day; 5 consecutive days; 30 h | BIT: group, day camp, bimanual coordination repetitive tasks, and gross and fine motor tasks. 6 h/day; 5 consecutive days; 30 h |
| Sakzewski et al. [23], 2011 Australia | N = 64 (26/26); Girls/boys: 31/33 | Age (years, months): 10.2 ± 2.7 | Spastic hemiplegia | CIMT: group, day camp, restriction with glove and splint, gross and fine motor tasks, functional activities, and games. 6 h/day; 10 consecutive days; 60 h | BIT: group, day camp, bimanual coordination repetitive tasks, gross and fine motor tasks. 6 h/day; 10 consecutive days; 60 h |
| Friel et al. [24], 2021 USA | N = 79 (40/39); Girls/boys: 31/48 | Age (years, months) Unimanual group: 9.4 ± 2.10 Bimanual group: 9.7 ± 3.5 | Spastic hemiplegia | CIMT: restriction with sling, gross and fine motor functional tasks. 6 h/day; 15 consecutive days; 90 h | HABIT: gross and fine motor bimanual tasks. 6 h/day; 15 consecutive days; 90 h |
| Zafer et al. [26], 2016 Pakistan | N = 18 (9/9); Girls/boys: 3/15 | Age (years, months): 8.75 ± 3.06 | Spastic hemiplegia | CIMT: at home, restriction with glove and sling, reach, grasp, and weight bearing tasks. 2 h/day; 6 days/week; 2 weeks; 24 h | BIT: at home, bimanual reach, grasp, and weight bearing tasks. 2 h/day; 6 days/week; 2 weeks; 24 h |
| Study | Outcomes | Assessment Tools | Follow-Up | Results (<0.05) | |
|---|---|---|---|---|---|
| Between Groups | Intragroups | ||||
| Bingöl et al. [27], 2022 Turkey | Primary:
|
| Before IT; after IT; 16 weeks. | Grasp strength: mCIMT (p < 0.001) Unimanual ability: mCIMT (p < 0.001) and in the follow-up (p < 0.001) Bimanual hand use: BT (p < 0.001). Affected limb use: mCIMT (p < 0.001). Participation: mCIMT (p < 0.001). | - |
| Chamudot et al. [28] 2018 Israel | Primary:
|
| Before and after IT | No significant differences between groups. | Both in mini AHA and FI (p < 0.01). |
| Gelkop et al. [29], 2015 Israel | Primary:
|
| 2 months before IT; before IT; after IT; 2-month follow-up. | Dissociated movements in CIMT (p < 0.05) before and after IT. | Both in AHA (p < 0.05) and QUEST (p < 0.05). |
| Gordon et al. [20], 2011 USA | Primary:
|
| Before IT; 2 days after IT; 1-month follow-up; 6-month follow-up. | HABIT in goal attainment and transfer to non-established goals (p < 0.05). | Both in QUEST (p < 0.001) and JTHFT (p < 0.001). |
| Brandao et al. [21], 2012 Brazil | Primary:
Not specified |
| Before and after IT. | No significant differences between groups. | Both in PEDI functional independence (p = 0.0001) and caregiver assistance (p = 0.01). Both in COPM performance (p < 0.000) and satisfaction (p = 0.0001). Both in practised goals (p = 0.003) and unpractised (p = 0.0001) |
| Fedrizzi et al. [25], 2013 Italy | Primary:
Not specified |
| Before IT; after IT; 3-month follow-up; 6-month follow-up. | BIT in Besta Scale (p = 0.0139). -CIMT affected hand (p = 0.0019); BIT in the follow-ups (p = 0.0270). BIT non-affected hand (p = 0.0280); CIMT (p = 0.0154) at 3-month follow-up. | Both in QUEST and Besta Scale (p < 0.001) |
| Sakzewski et al. [22], 2015 Australia | Primary:
|
| Before IT; 3 weeks after IT; 26-week follow-up. | No significant differences between groups. | Both (p < 0.005) in COPM |
| Sakzewski et al. [23], 2011 Australia | Primary:
|
| Before IT; 3 weeks after IT; 26-week follow-up; 1-year follow-up. | CIMT in unimanual capacity (p = 0.005). | CIMT in quality and efficacy of movement at 26-week and 1-year follow-ups (p < 0.001). BIT in efficacy between 26-week and 1-year follow-ups (p = 0.001). Both in COPM (p < 0.001) 1-year follow-up. |
| Friel et al. [24], 2021 USA | Primary:
|
| Before IT; after IT; 6 month follow-up. | Both in AHA, JTHFT and BBT (p < 0.001) maintained at 6 months. | Both in hand use in ADLs, COPM and PEDI (p < 0.001). |
| Zafer et al. [26], 2016 Pakistan | Primary:
Not specified |
| Before and after IT. | CIMT in dissociated movements, grasp and QUEST total (p < 0.05). | Both in dissociated movements and grasp (p < 0.05). |
| Time Effects | Outcome Measures | Measuring Instruments | Studies |
|---|---|---|---|
| Immediate | Unimanual ULF | QUEST dissociate domain | Bingöl et al., 2022 [27]; Gelkop et al., 2015 [29]; Gordon et al., 2011 [20]; Zafer et al., 2016 [26] |
| QUEST grasp domain | Bingöl et al., 2022 [27]; Fedrizzi et al., 2013 [25]; Gelkop et al., 2015 [29]; Gordon et al., 2011 [20]; Zafer et al., 2016 [26] | ||
| QUEST total score | Fedrizzi et al., 2013 [25]; Gelkop et al., 2015 [29]; Zafer et al., 2016 [26] | ||
| JTHFT | Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral; Gordon et al., 2011 [20] | ||
| Bimanual ULF | AHA | Chamudot et al., 2018 [28]; Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral; Gelkop et al., 2015 [29] | |
| Occupational performance and disability | COPM Performance | Brandao et al., 2012 [21]; Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral; Sakzweski et al., 2011 [23]; Sakzweski et al., 2015 [22] | |
| COPM Satisfaction | Brandao et al., 2012 [21]; Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral; Sakzweski et al., 2015 [22] | ||
| PEDI functional skills | Brandao et al., 2012 [21]; Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral | ||
| PEDI independence | Brandao et al., 2012 [21]; Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral | ||
| Short term | Unimanual ULF | QUEST dissociate domain | Bingöl et al., 2022 [27]; Gelkop et al., 2015 [29]; Gordon et al., 2011 [20] |
| QUEST grasp domain | Bingöl et al., 2022 [27]; Fedrizzi et al., 2013 [25]; Gelkop et al., 2015 [29]; Gordon et al., 2011 [20] | ||
| QUEST total score | Fedrizzi et al., 2013 [25]; Gelkop et al., 2015 [29] | ||
| JTHFT | Gordon et al., 2011 [20]; Sakzweski et al., 2011 [23]; Sakzweski et al., 2015 [22] | ||
| Bimanual ULF | AHA | Gelkop et al., 2015 [29]; Sakzweski et al., 2011 [23]; Sakzweski et al., 2015 [22] | |
| Long term | Unimanual ULF | QUEST grasp domain | Fedrizzi et al., 2013 [25]; Gordon et al., 2011 [20] |
| JTHFT | Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral; Gordon et al., 2011 [20]; Sakzweski et al., 2011 [23]; Sakzweski et al., 2015 [22] | ||
| Bimanual ULF | AHA | Friel et al., 2021 [24] Bilateral; Friel et al., 2021 [24] Contralateral; Friel et al., 2021 [24] Ipsilateral; Sakzweski et al., 2011 [23]; Sakzweski et al., 2015 [22] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin-Moreno, G.; Moreno-Ligero, M.; Salazar, A.; Lucena-Anton, D.; Moral-Munoz, J.A. Constraint-Induced Movement Therapy Versus Bimanual Training to Improve Upper Limb Function in Cerebral Palsy: A Systematic Review and Meta-Analysis of Follow-Ups. Children 2025, 12, 804. https://doi.org/10.3390/children12060804
Martin-Moreno G, Moreno-Ligero M, Salazar A, Lucena-Anton D, Moral-Munoz JA. Constraint-Induced Movement Therapy Versus Bimanual Training to Improve Upper Limb Function in Cerebral Palsy: A Systematic Review and Meta-Analysis of Follow-Ups. Children. 2025; 12(6):804. https://doi.org/10.3390/children12060804
Chicago/Turabian StyleMartin-Moreno, Gabriel, Marta Moreno-Ligero, Alejandro Salazar, David Lucena-Anton, and Jose A. Moral-Munoz. 2025. "Constraint-Induced Movement Therapy Versus Bimanual Training to Improve Upper Limb Function in Cerebral Palsy: A Systematic Review and Meta-Analysis of Follow-Ups" Children 12, no. 6: 804. https://doi.org/10.3390/children12060804
APA StyleMartin-Moreno, G., Moreno-Ligero, M., Salazar, A., Lucena-Anton, D., & Moral-Munoz, J. A. (2025). Constraint-Induced Movement Therapy Versus Bimanual Training to Improve Upper Limb Function in Cerebral Palsy: A Systematic Review and Meta-Analysis of Follow-Ups. Children, 12(6), 804. https://doi.org/10.3390/children12060804