

Path Analysis of the Relationships between the Eruption Time of the First Primary Teeth and Various Factors in Twins

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Samples Collection
2.1.2. Ethical Approval
2.2. Zygosity Determination
2.3. Maternal Surveys and Clinical Information
2.3.1. Birth Weight and Gestational Age
2.3.2. Eruption Timing of the First Primary Tooth
2.4. Statistical Analysis
2.5. Hypotheses
3. Results
4. Discussion
5. Conclusions
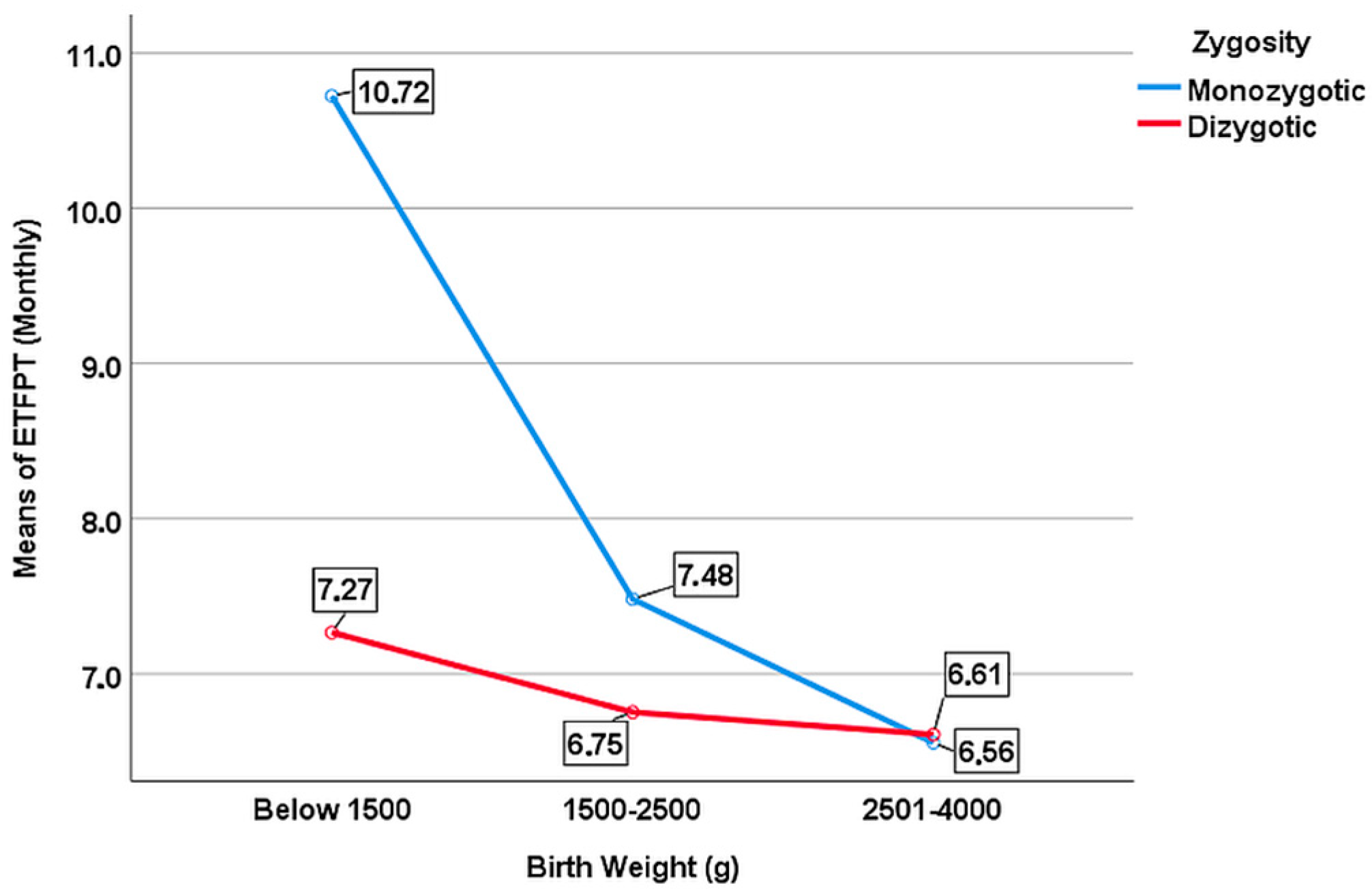
- Birth weight affects tooth development in the prenatal period and has an effect on ETFPT;
- The variation of the eruption age according to birth weight was much more pronounced among MZ twins;
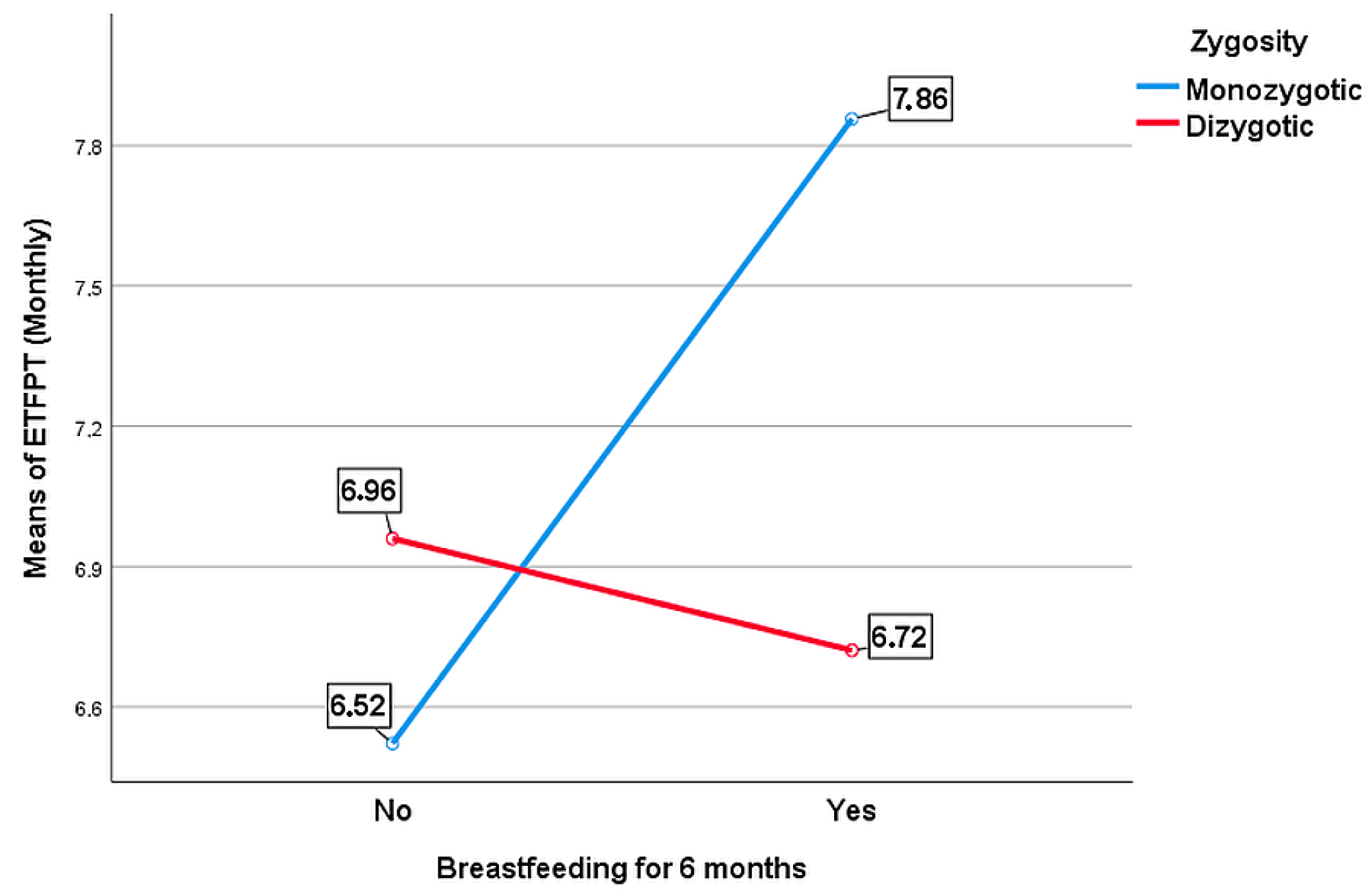
- A moderating effect of zygosity was found between breastfeeding and ETFPT.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Georgiadou, A.I.; Ritsas, A.; Arhakis, A. The impact of maternal, perinatal and early infancy period on the eruption timing of the first primary tooth. Eur. J. Dent. Oral Health 2021, 2, 28–33. [Google Scholar] [CrossRef]
- Shaweesh, A.I.; Al-Batayneh, O.B. Association of weight and height with timing of deciduous tooth emergence. Arch. Oral Biol. 2017, 87, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Alnemer, K.A.; Pani, S.C.; Althubaiti, A.M.; Bawazeer, M. Impact of birth characteristics, breast feeding and vital statistics on the eruption of primary teeth among health infants in Saudi Arabia: An observational study. BMJ Open 2017, 7, e018621. [Google Scholar] [CrossRef] [PubMed]
- Sajjadian, N.; Shajari, H.; Jahadi, R.; Barkett, M.G.; Sajjadian, A. Relationship between birth weight and time of first deciduous tooth eruption in 143 consecutively born infants. Pediatr. Neonatol. 2010, 51, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.U.; Stephen Hsu, C.Y.; Yee, R.; Koh, D.; Lee, Y.S.; Chong, M.F.F.; Cai, M.; Kwek, K.; Saw, S.M.; Godfrey, K.; et al. Influence of metabolic-linked early life factors on the eruption timing of the first primary tooth. Clin. Oral Investig. 2016, 20, 1871–1879. [Google Scholar] [CrossRef]
- Zadzinska, E.; Sitek, A.; Rosset, I. Relationship between pre-natal factors, the perinatal environment, motor development in the first year of life and the timing of first deciduous tooth emergence. Ann. Hum. Biol. 2016, 43, 25–33. [Google Scholar] [CrossRef]
- Madiraju, G.; Basavaraja, H. A cross sectional study of eruption time of primary teeth in south Indian children. J. Clin. Diag. Res. 2020, 14, 7–9. [Google Scholar] [CrossRef]
- Badruddin, I.A.; Auerkari, E.I.; Darwita, R.R.; Stiawati, F.; Adiatman, M.; Maharani, D.A.; Rahardjo, A. Genetics aspects of tooth eruption: A systematic review. J. Int. Dent. Med. Res. 2020, 13, 1585–1591. [Google Scholar]
- Silva Castro, C.R.; Sousa Cabral, M.B.B.; Mota, A.L.A.; Cangussu, M.C.T.; Vianna, M.I.P. Low birth weight and the delay on the eruption of deciduous teething in children. Rev. Bras. Saude Mater. Infant. 2019, 19, 701–710. [Google Scholar] [CrossRef]
- Choi, N.K.; Yang, K.H. A study on the eruption timing of primary teeth in Korean children. ASDC J. Dent. Child. 2001, 68, 244–249. [Google Scholar]
- Holman, D.J.; Jones, R.E. Longitudinal analysis of deciduous tooth emergence: III. Sexual dimorphism in Bangladeshi, Guatemalan, Japanese, and Javanese children. Am. J. Phys. Anthropol. 2003, 122, 269–278. [Google Scholar] [CrossRef]
- Haddad, A.E.; Correa, M. The relationship between deciduous teeth eruption, birth weight, birth length, weight and length for age. J. Dent. Res. 2002, 81, 198. [Google Scholar]
- Sadauskaitė, N.; Almonaitienė, R.; Brukienė, V. The timing of tooth eruption in preterm children: A systematic review. Australas. Med. J. 2021, 14, 96–107. [Google Scholar]
- Oziegbe, E.O.; Adekoya-Sofowora, C.A.; Esan, T.A.; Owotade, F.J.; Folayan, M.O. Breastfeeding pattern and eruption of primary teeth in Nigerian children. Pediatr. Dent. J. 2010, 20, 1–6. [Google Scholar] [CrossRef]
- Viggiano, D.; Fasano, D.; Monaco, G.; Strohmenger, L. Breast feeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch. Dis. Child. 2004, 89, 1121–1123. [Google Scholar] [CrossRef]
- Ahn, C.H.; MacLean Jr, W.C. Growth of the exclusively breast-fed infant. Am. J. Clin. Nutr. 1980, 33, 183–192. [Google Scholar] [CrossRef]
- Pavicin, I.S.; Dumancic, J.; Badel, T.; Vodanovic, M. Timing of emergence of the first primary tooth in preterm and full-term infants. Ann. Anat. 2016, 203, 9–23. [Google Scholar] [CrossRef]
- Ramos, S.R.; Gugisch, R.C.; Fraiz, F.C. The influence of gestational age and birthweight of the newborn on tooth eruption. J. Appl. Oral Sci. 2006, 14, 228–232. [Google Scholar] [CrossRef]
- Neto, P.G.; Falcao, M. Eruption chronology of the first deciduous teeth in children born prematurely with birth weight less than 1500g. Rev. Paul. Pediatr. 2014, 32, 17–23. [Google Scholar] [CrossRef]
- Koch, G.; Poulsen, S.; Espelid, I.; Haubek, D. Tooth Development and Disturbances in Number and Shape of Teeth. In Pediatric Dentistry: A Clinical Approach; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 28–40. [Google Scholar]
- Aktoren, O.; Tuna, E.B.; Guven, Y.; Gokcay, G. A study on neonatal factors and eruption time of primary teeth. Community Dent. Health 2010, 27, 52. [Google Scholar]
- WHO. Nutrition Landscape Information System (NLİS). Available online: https://www.who.int/data/nutrition/nlis/info/low-birth-weight#:~:text=Low%20birth%20weight%20has%20been,2500%20grams%20(5.5%20pounds) (accessed on 1 March 2023).
- Fieß, A.; Elbaz, H.; Korb, C.A.; Nickels, S.; Schulz, A.; Münzel, T.; Wild, P.S.; Beutel, M.E.; Schmidtmann, I.; Lackner, K.J.; et al. Low birth weight is linked to age-related macular degeneration: Results from the population-based Gutenberg Health Study (GHS). Investig. Ophthalmol. Vis. Sci. 2019, 60, 4943–4950. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.; Hult, G.; Ringle, C.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (Pls-Sem); Thousand Oaks: Sage, CA, USA, 2017; pp. 128–230. [Google Scholar]
- Henseler, J.; Ringle, C.; Sarsted, M. A new criterion for assesing discriminant validity in variance-based structural equation modeling. J. Acad. Market. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R.; Tatham, R. Multivariate Data Analysis; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Clarke, M.; Locker, D.; Berall, G.; Pencharz, P.; Kenny, D.J.; Judd, R. Malnourishment in a population of young children with severe early childhood caries. Pediatr. Dent. 2006, 28, 254–259. [Google Scholar] [PubMed]
- Takaoka, L.A.; Goulart, A.L.; Kopelman, B.I.; Weiler, R.M. Enamel defects in the complete primary dentition of children born at term and preterm. Pediatr. Dent. 2011, 33, 171–176. [Google Scholar]
- Targino, A.G.; Rosenblatt, A.; Oliveira, A.F.; Chaves, A.M.; Santos, V.E. The relationship of enamel defects and caries: A cohort study. Oral Dis. 2011, 17, 420–426. [Google Scholar] [CrossRef]
- Chan, E.; Bockmann, M.; Hughes, T.; Mihailidis, S.; Townsend, G. Do feeding practices, gestation length, and birth weight affect the timing of emergence of the first primary tooth. In New Directions in Dental Anthropology: Paradigms, Methodologies and Outcomes; Townsend, G., Kanazawa, E., Takayama, H., Eds.; University of Adalaide Press: Adelaide, Australia, 2012; pp. 35–45. [Google Scholar]
- Ntani, G.; Day, P.F.; Baird, J.; Godfrey, K.M.; Robinson, S.M.; Cooper, C.; Inskip, H.M. Maternal and early life factors of tooth emergence patterns and number of teeth at 1 and 2 years of age. J. Dev. Orig. Health Dis. 2015, 6, 299–307. [Google Scholar] [CrossRef]
- Wang, X.Z.; Sun, X.Y.; Quan, J.K.; Zhang, C.Y.; Zhao, M.; Shi, X.R.; Si, Y.; Zheng, S.G. Effects of premature delivery and birth weight on eruption pattern of primary dentition among Beijing children. Chin. J. Dent. Res. 2019, 22, 131–137. [Google Scholar]
- Memarpour, M.; Golkari, A.; Ahmadian, R. Association of characteristics of delivery and medical conditions during the first month of life with developmental defects of enamel. BMC Oral Health 2014, 1, 1–7. [Google Scholar] [CrossRef]
- Zadzinska, E.; Kurek, M.; Borowska-Struginska, B.; Lorkiewicz, W.; Rosset, I.; Sitek, A. The effect of the season of birth and of selected maternal factors on linear enamel thickness in modern human deciduous incisors. Arch. Oral Biol. 2013, 58, 951–963. [Google Scholar] [CrossRef]
- Wagner, Y. Developmental defects of enamel in primary teeth-findings of a regional German birth cohort study. BMC Oral Health 2017, 17, 1–8. [Google Scholar] [CrossRef]
- Mendonça Zina, G.F.; Espinosa, M.M.; Shitsuka, C.; Imparato, J.C.P.; Duarte, D.A. Developmental defects of enamel, sociodemographic aspects and systemic diseases: Is there association? Res. Soc. Develop. 2021, 10, e13110212150. [Google Scholar] [CrossRef]
- Wu, H.; Chen, T.; Ma, Q.; Xu, X.; Xie, K.; Chen, Y. Associations of maternal, perinatal and postnatal factors with the eruption timing of the first primary tooth. Sci. Rep. 2019, 9, 2645. [Google Scholar] [CrossRef]
- Holman, D.J.; Yamaguchi, K. Longitudinal analysis of deciduous tooth emergence: IV. Covariate effects in Japanese children. Am. J. Phys. Anthropol. 2005, 3, 352–358. [Google Scholar] [CrossRef]
- Sahin, F.; Camurdan, A.D.; Camurdan, M.O.; Olmez, A.; Oznurhan, F.; Beyazova, U. Factors affecting the timing of teething in healthy Turkish infants: A prospective cohort study. Int. J. Paediatr. Dent. 2008, 18, 262–266. [Google Scholar] [CrossRef]
- Folayan, M.O.; Sowole, C.A. Association between breastfeeding and eruption of the first tooth in preschool children in Nigeria. Eur. J. Paediatr. Dent. 2013, 14, 51–54. [Google Scholar]
- Thompson, B. The use of statistical significance tests in research: Bootstrap and other alternatives. J. Exp. Educ. 1993, 61, 361–377. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Birth Weight | Breastfeeding | ETFPT | Gender | Pregnancy Term | Type of Delivery | Zygosity | |
|---|---|---|---|---|---|---|---|
| Birth Weight | |||||||
| Breastfeeding | 0.083 | ||||||
| ETFPT | −0.162 | 0.045 | |||||
| Gender | 0.142 | 0.091 | 0.057 | ||||
| Pregnancy Term | 0.542 | 0.044 | −0.028 | 0.094 | |||
| Type of Delivery | 0.047 | −0.037 | −0.108 | −0.050 | −0.065 | ||
| Zygosity | −0.056 | 0.068 | −0.109 | −0.005 | −0.081 | 0.022 |
| Criterion Variable | |
|---|---|
| Predictors | ETFPT (Monthly) |
| Birth Weight | 1.455 |
| Breastfeeding | 1.020 |
| Gender | 1.031 |
| Pregnancy Term | 1.437 |
| Type of Delivery | 1.019 |
| Zygosity | 1.013 |
| Number of Siblings: 404 Number of Twin Pairs: 202 | |||
|---|---|---|---|
| Variable | Group | n | % |
| Birth Weight (g) | Below 1500 | 39 | 9.7 |
| 1500–2500 | 198 | 49.0 | |
| 2501–4000 | 167 | 41.3 | |
| Gender | Male | 204 | 50.5 |
| Female | 200 | 49.5 | |
| Zygosity | Monozygotic | 118 | 29.2 |
| Dizygotic | 286 | 70.8 | |
| Type of Birth | Normal | 47 | 11.6 |
| Caesarean | 357 | 88.4 | |
| Breastfeeding For First 6 Months | No | 133 | 32.9 |
| Yes | 251 | 62.1 | |
| Missing | 20 | 5.0 | |
| M | SD | ||
| Chronological Age (Yearly) | Monozygotic | 9.10 | ±3.04 |
| Dizygotic | 8.63 | ±3.29 | |
| Male | 8.53 | ±3.27 | |
| Female | 9.01 | ±3.15 | |
| Total | 8.77 | ±3.22 | |
| ETFPT (Monthly) | Monozygotic | 7.31 | ±3.25 |
| Dizygotic | 6.75 | ±1.84 | |
| Male | 7.05 | ±2.74 | |
| Female | 6.78 | ±1.88 | |
| Total | 6.91 | ±2.35 | |
| Pregnancy Term (Weekly) | Monozygotic | 36.02 | ±3.18 |
| Dizygotic | 35.44 | ±3.26 | |
| Male | 35.91 | ±3.10 | |
| Female | 35.30 | ±3.37 | |
| Total | 35.61 | ±3.25 |
| Relationships | Original Sample (O) | SD | t | p | Confidence Intervals Bias Corrected | |||
|---|---|---|---|---|---|---|---|---|
| Bias | 2.5% | 97.5% | ||||||
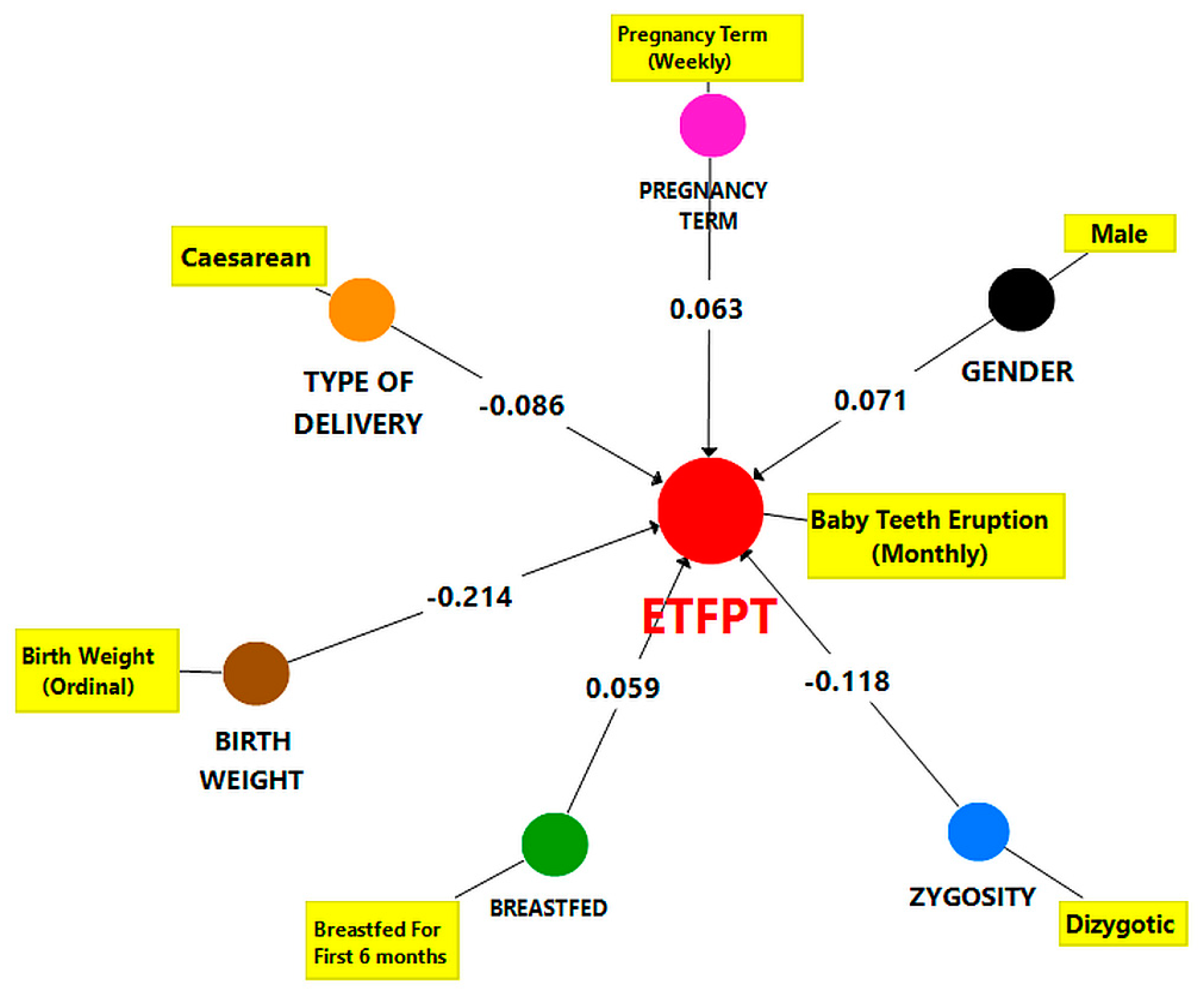
| Birth Weight → ETFPT | −0.214 | −0.214 | −0.214 | −0.214 | −0.214 | −0.214 | −0.214 | −0.214 |
| Zygosity → ETFPT | −0.210 | −0.210 | −0.210 | −0.210 | −0.210 | −0.210 | −0.210 | −0.210 |
| Gender → ETFPT | 0.072 | 0.072 | 0.072 | 0.072 | 0.072 | 0.072 | 0.072 | 0.072 |
| Type of Delivery → ETFPT | 2.964 | 2.964 | 2.964 | 2.964 | 2.964 | 2.964 | 2.964 | 2.964 |
| Breastfeeding For First 6 Months → ETFPT | 0.003 * | 0.003 * | 0.003 * | 0.003 * | 0.003 * | 0.003 * | 0.003 * | 0.003 * |
| Pregnancy Term → ETFPT | 0.004 | 0.004 | 0.004 | 0.004 | 0.004 | 0.004 | 0.004 | 0.004 |
| Dizygotic vs. Monozygotic | ||
|---|---|---|
| Path Coefficient | p | |
| Breastfeeding For First 6 Months →ETFPT | −0.200 | 0.029 * |
| Birth Weight → ETFPT | 0.286 | 0.043 * |
| Type of Delivery → ETFPT | 0.118 | 0.365 |
| Pregnancy Term (Weekly) → ETFPT | −0.022 | 0.845 |
| Relationships | Zygosity Group | Original Sample (O) | Sample Mean (M) | SD | t | p | Confidence Intervals Bias Corrected | ||
|---|---|---|---|---|---|---|---|---|---|
| Bias | 2.5% | 97.5% | |||||||
| Breastfeeding → ETFPT | Dizygotic | −0.051 | −0.050 | 0.064 | 0.789 | 0.422 | −0.001 | −0.176 | 0.073 |
| Monozygotic | 0.149 | 0.148 | 0.063 | 2.366 | 0.019 * | −0.002 | 0.019 | 0.269 | |
| Birth Weight → ETFPT | Dizygotic | −0.082 | −0.084 | 0.075 | 1.091 | 0.275 | −0.002 | −0.231 | 0.067 |
| Monozygotic | −0.368 | −0.359 | 0.107 | 3.443 | 0.001 * | 0.009 | −0.551 | −0.128 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Birant, S.; Veznikli, M.; Kasimoglu, Y.; Koruyucu, M.; Evren, A.A.; Seymen, F. Path Analysis of the Relationships between the Eruption Time of the First Primary Teeth and Various Factors in Twins. Children 2023, 10, 683. https://doi.org/10.3390/children10040683
Birant S, Veznikli M, Kasimoglu Y, Koruyucu M, Evren AA, Seymen F. Path Analysis of the Relationships between the Eruption Time of the First Primary Teeth and Various Factors in Twins. Children. 2023; 10(4):683. https://doi.org/10.3390/children10040683
Chicago/Turabian StyleBirant, Sinem, Mert Veznikli, Yelda Kasimoglu, Mine Koruyucu, Atıf Ahmet Evren, and Figen Seymen. 2023. "Path Analysis of the Relationships between the Eruption Time of the First Primary Teeth and Various Factors in Twins" Children 10, no. 4: 683. https://doi.org/10.3390/children10040683
APA StyleBirant, S., Veznikli, M., Kasimoglu, Y., Koruyucu, M., Evren, A. A., & Seymen, F. (2023). Path Analysis of the Relationships between the Eruption Time of the First Primary Teeth and Various Factors in Twins. Children, 10(4), 683. https://doi.org/10.3390/children10040683