

Effects of a Diabetes Sports Summer Camp on the Levels of Physical Activity and Dimensions of Health-Related Quality of Life in Young Patients with Diabetes Mellitus Type 1: A Randomized Controlled Trial



Abstract
1. Introduction
2. Materials and Methods
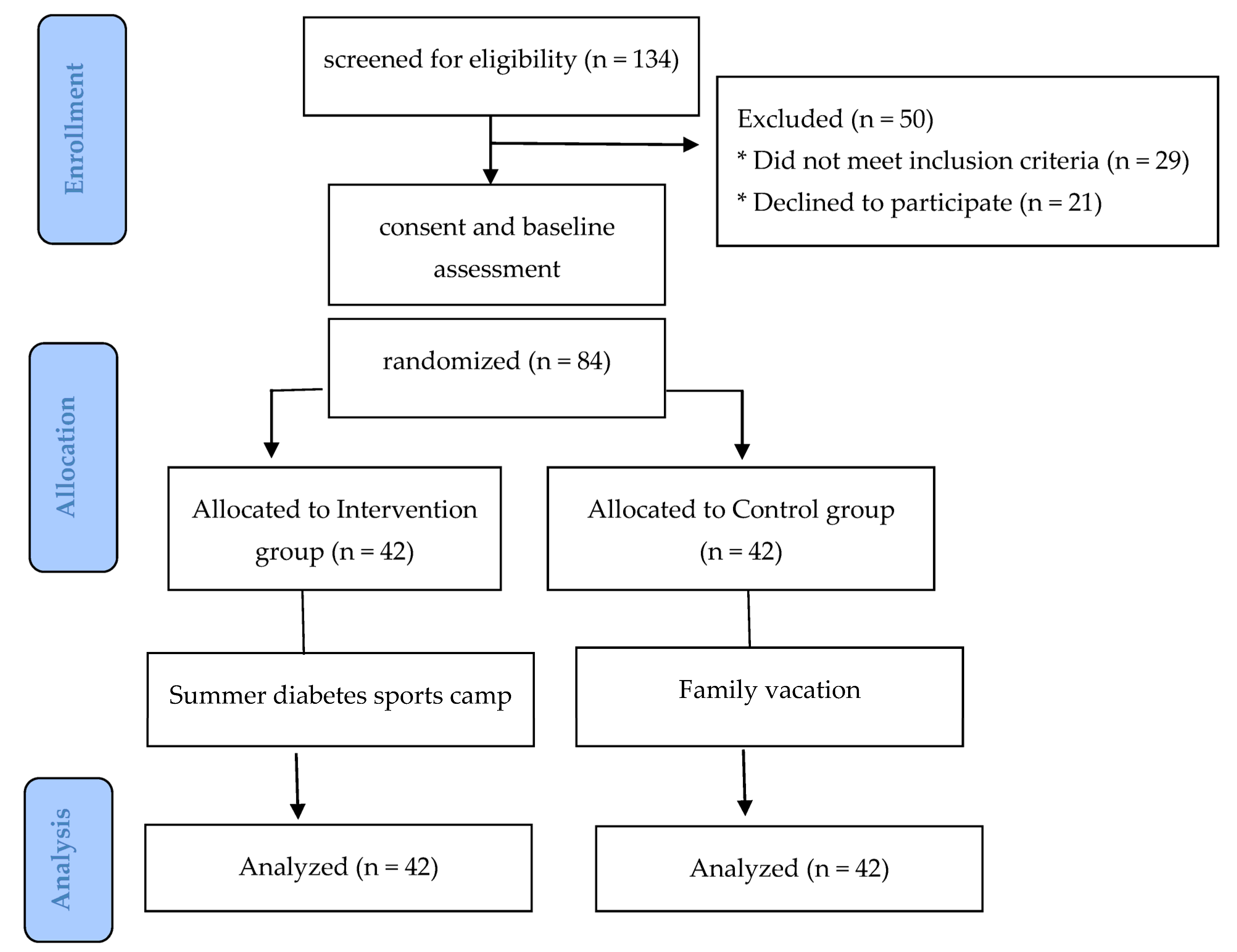
2.1. Participants
2.2. Design and Procedure
2.3. Measurements
2.3.1. Physical Activity
2.3.2. Life Satisfaction
2.3.3. Self-Esteem
2.3.4. Depression
2.3.5. Health Status and Its Treatment and Intent to Change Health-Related Behaviour (HAPA)
2.4. Intervention Design
2.5. Statistical Analysis
3. Results
3.1. Preliminary Analyses
3.2. Effectiveness of the Intervention
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mobasseri, M.; Shirmohammadi, M.; Amiri, T.; Vahed, N.; Hosseini Fard, H.; Ghojazadeh, M. Prevalence and incidence of type 1 diabetes in the world: A systematic review and meta-analysis. Health Promot. Perspect. 2020, 10, 98–115. [Google Scholar] [CrossRef]
- Melendez-Ramirez, L.Y.; Richards, R.J.; Cefalu, W.T. Complications of type 1 diabetes. Endocrinol. Metab. Clin. N. Am. 2010, 39, 625–640. [Google Scholar] [CrossRef]
- Blanz, B.J.; Rensch-Riemann, B.S.; Fritz-Sigmund, D.I.; Schmidt, M.H. IDDM is a risk factor for adolescent psychiatric disorders. Diabetes Care 1993, 16, 1579–1587. [Google Scholar] [CrossRef]
- Kovacs, M.; Goldston, D.; Obrosky, D.S.; Bonar, L.K. Psychiatric disorders in youths with IDDM: Rates and risk factors. Diabetes Care 1997, 20, 36–44. [Google Scholar] [CrossRef]
- Grey, M.; Whittemore, R.; Tamborlane, W. Depression in type 1 diabetes in children. J. Psychosom. Res. 2002, 53, 907–911. [Google Scholar] [CrossRef]
- Buchberger, B.; Huppertz, H.; Krabbe, L.; Lux, B.; Mattivi, J.T.; Siafarikas, A. Symptoms of depression and anxiety in youth with type 1 diabetes: A systematic review and meta-analysis. Psychoneuroendocrinology 2016, 70, 70–84. [Google Scholar] [CrossRef]
- Samuels, S.; Menand, E.V.; Mauer, E.A.; Hernandez, S.; Terekhova, D.; Mathews, T.L.; Albright, M.S.; Antal, M.D.; Kanellopoulos, D. Anxiety and type 1 diabetes management: Guardian and child report in a pediatric endocrinology clinic. Psychosomatics 2020, 61, 231–237. [Google Scholar] [CrossRef]
- Pita, R.; Grigoriadou, E.; Marina, Ε.; Kouvatsou, Z.; Didaggelos, T.; Karamitsos, D. Quality of life and type 1 diabetes mellitus (Greek ed.). Greek Diabetol. Ann. 2006, 19, 282–294. [Google Scholar]
- Hoey, H.; Aanstoot, H.-J.; Chiarelli, F.; Daneman, D.; Danne, T.; Dorchy, H.; Fitzgerald, M.; Garandeau, P.; Greene, S.; Holl, R.; et al. Good metabolic control is associated with better quality of life in 2,101 adolescents with type 1 diabetes. Diabetes Care 2001, 24, 1923–1928. [Google Scholar] [CrossRef]
- Kalyva, E.; Malakonaki, E.; Eiser, C.; Mamoulakis, D. Health-related quality of life (hrqol) of children with type 1 diabetes mellitus (T1DM): Self and parental perceptions. Pediatr. Diabetes 2011, 12, 34–40. [Google Scholar] [CrossRef]
- Leclair, E.; de Kerdanet, M.; Riddell, M.; Heymen, E. Type 1 diabetes and physical activity in children and adolescents. J. Diabetes Metab. 2013, 1, 1163–1173. [Google Scholar] [CrossRef]
- Quirk, H.; Blake, H.; Tennyson, R.; Randell, T.L. Physical activity interventions in children and young people with Type 1 diabetes mellitus: A systematic review with meta-analysis. Diabet. Med. 2014, 31, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.; Adolfsson, P.; Scheiner, G.; Hanas, R.; Riddell, M.C. Exercise in children and adolescents with diabetes. Pediatr. Diabetes 2009, 10, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Valerio, G.; Spagnuolo, M.I.; Lombardi, F.; Spadaro, R.; Siano, M.; Franzese, A. Physical activity and sports participation in children and adolescents with type 1 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 376–382. [Google Scholar] [CrossRef]
- Barone, M.T.; Vivolo, M.A.; Madden, P.B. Are diabetes camps effective? Diabetes Res. Clin. Pract. 2016, 114, 15–22. [Google Scholar] [CrossRef]
- Tumini, S.; Anzellotti, M.T.; Chiarelli, F. Camps for children with T1DM. Acta Biomed. 2003, 74, 32–34. [Google Scholar] [PubMed]
- Hasan, I.; Chowdhury, A.B.; Haque, M.I.; Patterson, C.C. Changes in glycated hemoglobin, diabetes knowledge, quality of life, and anxiety in children and adolescents with type 1 diabetes attending summer camps: A systematic review and meta-analysis. Pediatr. Diabetes 2020, 22, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.; Caruso-Nicoletti, M. Summer camps and quality of life in children and adolescents with type 1 diabetes. Acta Biomed. 2003, 74, 35–37. [Google Scholar] [CrossRef]
- Correale, L.; Ferraro, O.E.; Pellino, V.C.; Ricagno, E.; Liberali, G.; Puci, M.V.; Vandoni, M. Educational physical activity camp in type 1 diabetes: Can be useful to promote an active lifestyle? Afr. J. Diabetes Med. 2020, 28, 1–3. [Google Scholar] [CrossRef]
- Sikora, M.; Zwierzchowska, A.; Jaworska, M.; Solich-Talanda, M.; Mikolajczyk, R.; Zebrowska, A. The effects of physical activity on glycaemic control in children and adolescents with type 1 diabetes mellitus participating in diabetes camp. Balt. J. Health Phys. Act. 2018, 10, 151–161. [Google Scholar] [CrossRef]
- García-Pérez, L.; Perestelo-Pérez, L.; Serrano-Aguilar, P.; Trujillo-Martín, M. del Effectiveness of a psychoeducative intervention in a summer camp for children with type 1 diabetes mellitus. Diabetes Educ. 2010, 36, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Santiprabhob, J.; Kiattisakthavee, P.; Likitmaskul, S.; Chaichanwattanakul, K.; Wekawanich, J.; Dumrongphol, H.; Sriwijitkamol, A.; Peerapatdit, T.; Nitiyanant, W. Glycemic control, quality of life and self-care behavior among adolescents with type 1 diabetes who attended a diabetes camp. Southeast Asian J. Trop. Med. Public Health 2012, 43, 172–184. [Google Scholar] [PubMed]
- Anarte, M.T.; Carreira, M.; Gea, A.L.; Varela, E.; Mateo-Anarte, M.; López Siguero, J.P.; Gea, I.L. Diabetes summer camp in children and adolescents with type 1 diabetes: Effects on well-being and quality of life. Endocrinol. Diabetes Nutr. (Engl. ed.) 2020, 67, 326–332. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, Behavioral, and Biomedical Sciences. Beh. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical Power analyses using G*Power 3.1: Tests for correlation and regression analyses. Beh. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Kechagia, C. Association of Physical Activity and Psychological Parameters with Quality of life in Patients with Diabetes Mellitus. Master’s Thesis, Aristotle University of Thessaloniki, Thessaloniki, Greece, 2019. [Google Scholar]
- Godin, G.; Shephard, R.J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E.; Colvin, C.R.; Sandvik, E. Further validation of the satisfaction with life scale: Evidence for the cross-method convergence of well-being measures. J. Pers. Assess. 1991, 57, 149–161. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2016. [Google Scholar]
- Radloff, L.S. The CES-D scale. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Beekman, A.T.; Deeg, D.J.; Van Limbeek, J.; Braam, A.W.; De Vries, M.Z.; Van Tilburg, W. Criterion validity of the Center for Epidemiologic Studies Depression scale (CES-D): Results from a community-based sample of older subjects in The Netherlands. Psychol. Med. 1997, 27, 231–235. [Google Scholar] [CrossRef]
- Schwarzer, R. Health Action Process Approach (HAPA) as a theoretical framework to understand behavior change. Actual. Psicol. 2016, 30, 119. [Google Scholar] [CrossRef]
- Bolu, S.; Danis, A.; Arslanoglu, I.; Bolu, F.; Akcali, F.; Aytar, G. Assesment of the effect of summer camp on the life quality of diabetic children. J. Turgut. Ozal. Med. Cent. 2017, 24, 305–309. [Google Scholar] [CrossRef]
- Török, S.; Kökönyei, G.; Károlyi, L.; Ittzés, A.; Tomcsányi, T. Outcome effectiveness of therapeutic recreation camping program for adolescents living with cancer and diabetes. J. Adolesc. Health 2006, 39, 445–447. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, H.; Knappstein, M.; Ajzen, I.; Schmidt, P.; Kabst, R. How effective are behavior change interventions based on the theory of planned behavior? Z. Psychol. 2016, 224, 216–233. [Google Scholar] [CrossRef]


{kind=link}
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 | Day 8 | Day 9 | Day 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 8:00 | Wake-up call | Wake-up call | Wake-up call | Wake-up call | Wake-up call | Wake-up call | Wake-up call | Wake-up call | Wake-up call | Wake-up call |
| 8:30 | Breakfast | Breakfast | Breakfast | Breakfast | Breakfast | Breakfast | Breakfast | Breakfast | Breakfast | Breakfast |
| 9:00 | Medical supervision | Medical supervision | Medical supervision | Medical supervision | Medical supervision | Medical supervision | Medical supervision | Medical supervision | Medical supervision | Medical supervision |
| 9:30 | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA | Education about the importance of PA |
| 10:15 | Swimming | Swimming | Swimming | Excursion | Swimming | Swimming | Swimming | Swimming | Swimming | Swimming |
| 11:45 | Climbing | Football | Athletics | Excursion | Volleyball | Archery | Ping pong | Basketball | Sport games | Tennis |
| 13:15 | Lunch | Lunch | Lunch | Lunch | Lunch | Lunch | Lunch | Lunch | Lunch | Lunch |
| 14:00 | Free time | Free time | Free time | Free time | Free time | Free time | Free time | Free time | Free time | Free time |
| 14:45 | Rest | Rest | Rest | Rest | Rest | Rest | Rest | Rest | Rest | Rest |
| 16:15 | Light meal | Light meal | Light meal | Light meal | Light meal | Light meal | Light meal | Light meal | Light meal | Light meal |
| 16:30 | Sailing | Canoe | Diving | Swimming | Seamanship | Sailing | Canoe | Excursion | Swimming | Diving |
| 18:00 | Basketball | Tennis | Volleyball | Archery | Handball | Athletics | Football | Excursion | Climbing | Sport games |
| 19:30 | Dinner | Dinner | Dinner | Dinner | Dinner | Dinner | Dinner | Dinner | Dinner | Dinner |
| 20:15 | Free time | Free time | Free time | Free time | Free time | Free time | Free time | Free time | Free time | Free time |
| 21:00 | Singing | Theater | Group activities | Dancing | Singing | Theater | Dancing | Group activities | Singing | Group activities |
| 22:30 | Bedtime | Bedtime | Bedtime | Bedtime | Bedtime | Bedtime | Bedtime | Bedtime | Bedtime | Bedtime |
| Total Sample | Intervention Group | Control Group | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Age (years) | 12.65 | 2.20 | 12.64 | 1.82 | 12.67 | 2.50 |
| Disease duration (months) | 59.05 | 37.33 | 63.45 | 38.03 | 54.54 | 36.50 |
| BMI | 20.15 | 3.77 | 20.15 | 3.36 | 20.15 | 4.39 |
| HbA1c (%) | 7.52 | 1.11 | 7.53 | 1.28 | 7.5 | 0.94 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| −0.07 | 0.04 | −0.00 | −0.00 | 0.06 | −0.03 | 0.06 | 0.12 | 0.05 | |
| 0.04 | 0.21 | −0.18 | 0.31 ** | 0.03 | −0.23 ** | −0.01 | 0.13 | 0.15 | |
| −0.01 | 0.68 ** | −0.43 ** | 0.36 ** | −0.31 ** | −0.36 ** | −0.12 | 0.11 | 0.05 | |
| −0.07 | −0.46 ** | −0.54 ** | −0.16 | 0.15 | 0.14 | 0.10 | −0.11 | −0.00 | |
| −0.04 | 0.59 ** | 0.48 ** | −0.30 ** | 0.22 * | −0.11 | 0.22 * | 0.03 | 0.01 | |
| −0.08 | 0.04 | −0.06 | 0.01 | 0.08 | 0.25 * | 0.15 | −0.08 | 0.03 | |
| 0.02 | −0.24 * | −0.28 * | 0.28 * | −0.18 | 0.17 | −0.15 | −0.21 | −0.06 | |
| −0.08 | 0.32 ** | 0.09 | 0.10 | 0.30 ** | −0.05 | −0.16 | 0.24 * | 0.14 | |
| −0.05 | 0.06 | 0.19 | −0.01 | −0.01 | −0.21 | −0.20 | 0.30 ** | 0.52 ** | |
| 0.09 | −0.01 | 0.06 | 0.19 | 0.07 | −0.14 | 0.04 | 0.20 | 0.59 ** |
| Total Sample | Intervention Group | Control Group | ||||
|---|---|---|---|---|---|---|
| First Measurement Mean (SD) | Second Measurement Mean (SD) | First Measurement Mean (SD) | Second Measurement Mean (SD) | First Measurement Mean (SD) | Second Measurement Mean (SD) | |
| PA | 47.18 (21.99) | 49.80 (23.24) | 49.45 (25.11) | 53.83 (26.65) | 44.90 (18.38) | 45.76 (18.70) |
| Satisfaction | 5.80 (1.93) | 5.65 (1.15) | 5.86 (2.55) | 5.66 (1.09) | 5.74 (1.03) | 5.64 (1.22) |
| Self-esteem | 32.33 (4.30) | 32.44 (5.16) | 31.33 (4.00) | 32.12 (4.62) | 33.33 (4.39) | 32.76 (5.69) |
| Depression | 0.93 (0.32) | 0.95 (0.34) | 0.91 (0.28) | 0.95 (0.32) | 0.94 (0.36) | 0.96 (0.36) |
| Health status | 3.66 (0.69) | 3.62 (0.83) | 3.78 (0.64) | 3.69 (0.76) | 3.54 (0.73) | 3.56 (0.90) |
| Changes in health | 2.75 (1.29) | 2.74 (1.34) | 3.12 (1.27) | 2.88 (1.53) | 2.38 (1.21) | 2.60 (1.34) |
| Relationship of health with everyday life | 2.60 (1.45) | 2.62 (1.34) | 2.60 (1.53) | 2.64 (1.48) | 2.60 (1.38) | 2.60 (1.21) |
| Intention | 4.78 (1.09) | 4.82 (1.27) | 4.91 (0.87) | 4.89 (1.11) | 4.64 (1.27) | 4.75 (1.42) |
| Activities planning | 3.16 (0.78) | 2.99 (0.90) | 3.18 (0.68) | 2.09 (0.81) | 3.14 (0.87) | 2.98 (0.98) |
| Planning to address difficulties | 2.74 (0.66) | 2.64 (0.80) | 2.79 (0.63) | 2.68 (0.78) | 2.68 (0.69) | 2.59 (0.84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skoufa, L.; Makri, E.; Barkoukis, V.; Papagianni, M.; Triantafyllou, P.; Kouidi, E. Effects of a Diabetes Sports Summer Camp on the Levels of Physical Activity and Dimensions of Health-Related Quality of Life in Young Patients with Diabetes Mellitus Type 1: A Randomized Controlled Trial. Children 2023, 10, 456. https://doi.org/10.3390/children10030456
Skoufa L, Makri E, Barkoukis V, Papagianni M, Triantafyllou P, Kouidi E. Effects of a Diabetes Sports Summer Camp on the Levels of Physical Activity and Dimensions of Health-Related Quality of Life in Young Patients with Diabetes Mellitus Type 1: A Randomized Controlled Trial. Children. 2023; 10(3):456. https://doi.org/10.3390/children10030456
Chicago/Turabian StyleSkoufa, Lida, Eleni Makri, Vassilis Barkoukis, Maria Papagianni, Panagiota Triantafyllou, and Evangelia Kouidi. 2023. "Effects of a Diabetes Sports Summer Camp on the Levels of Physical Activity and Dimensions of Health-Related Quality of Life in Young Patients with Diabetes Mellitus Type 1: A Randomized Controlled Trial" Children 10, no. 3: 456. https://doi.org/10.3390/children10030456
APA StyleSkoufa, L., Makri, E., Barkoukis, V., Papagianni, M., Triantafyllou, P., & Kouidi, E. (2023). Effects of a Diabetes Sports Summer Camp on the Levels of Physical Activity and Dimensions of Health-Related Quality of Life in Young Patients with Diabetes Mellitus Type 1: A Randomized Controlled Trial. Children, 10(3), 456. https://doi.org/10.3390/children10030456