



Primary Failure Eruption: Genetic Investigation, Diagnosis and Treatment: A Systematic Review

 , , , , ,
, , , , ,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
- Endocrine Function: it controls parathyroid hormone (PTH) secretion, influencing calcium and phosphate balance in bones, kidneys, and the intestine [27].
- Muscle Function: indirectly, it affects muscle contraction by regulating blood calcium levels [28].
- Nervous System: it indirectly influences nerve function through calcium regulation [29].
- Cardiovascular Health: proper calcium levels are vital for heart function, influenced by PTH1R [30].
- Mineral Metabolism: it affects various metabolic processes beyond bones and teeth [31].
- Immune System: PTH1R may modulate the immune response via calcium signalling [32].
- Latent TGF-Binding Protein 3 Gene: mutations in this gene have been linked to PFE. This gene is involved in the regulation of transforming growth factor-beta (TGF-β), which plays a role in tooth eruption [34].
- Collagen Type I Alpha 1 Chain and Collagen Type I Alpha 2 Chain Genes: mutations in these collagen genes can lead to connective tissue disorders, such as Ehlers–Danlos syndrome, which may, in some cases, be associated with PFE [35].
- Family with Sequence Similarity 20 Member A Gene: mutations in this gene have been linked to amelogenesis imperfecta and gingival fibromatosis syndrome, which can include PFE as a symptom [36].
- WD Repeat Domain 72 Gene: mutations in this gene are associated with a condition known as Raine syndrome, which can manifest with dental anomalies like PFE [37].
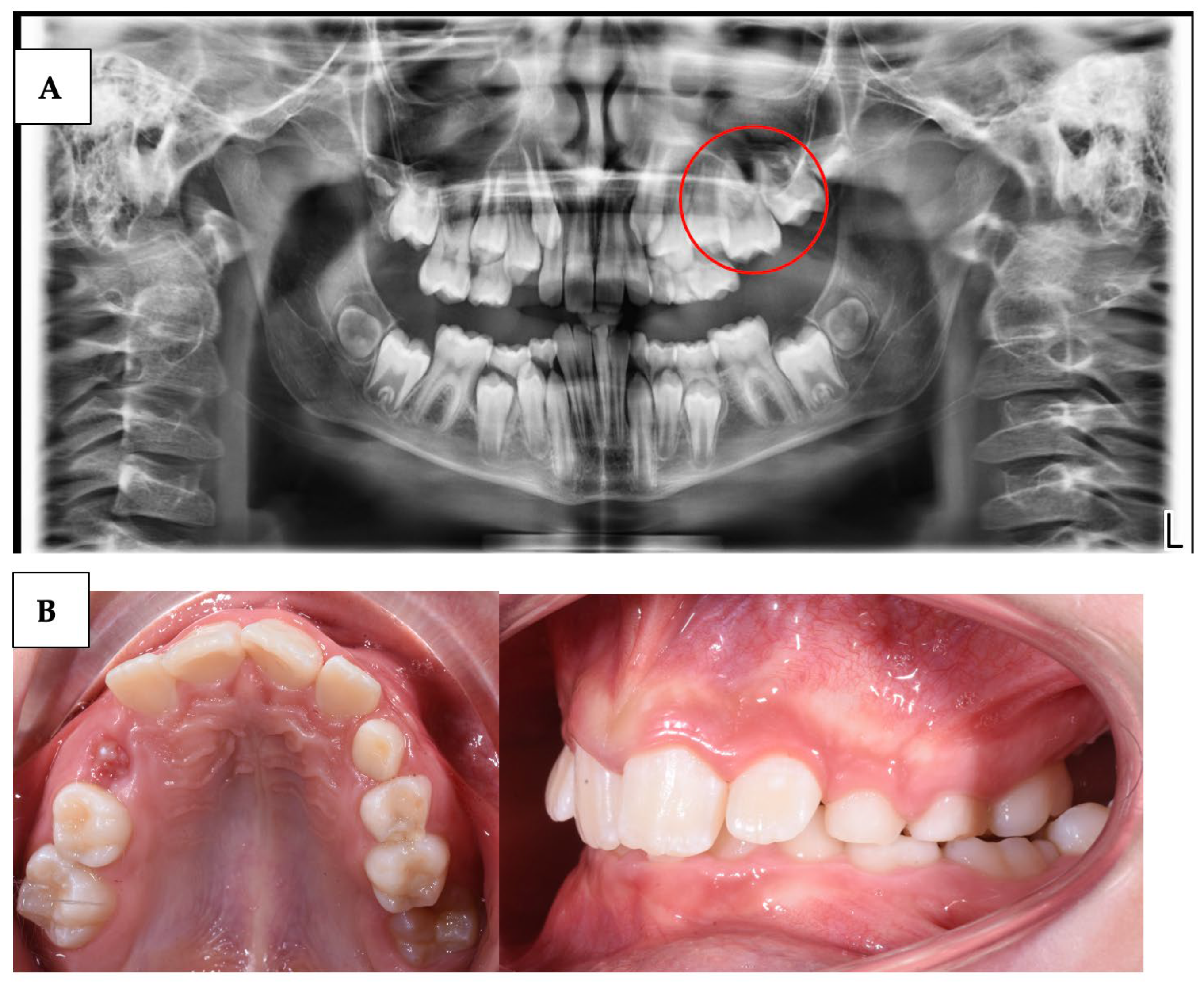
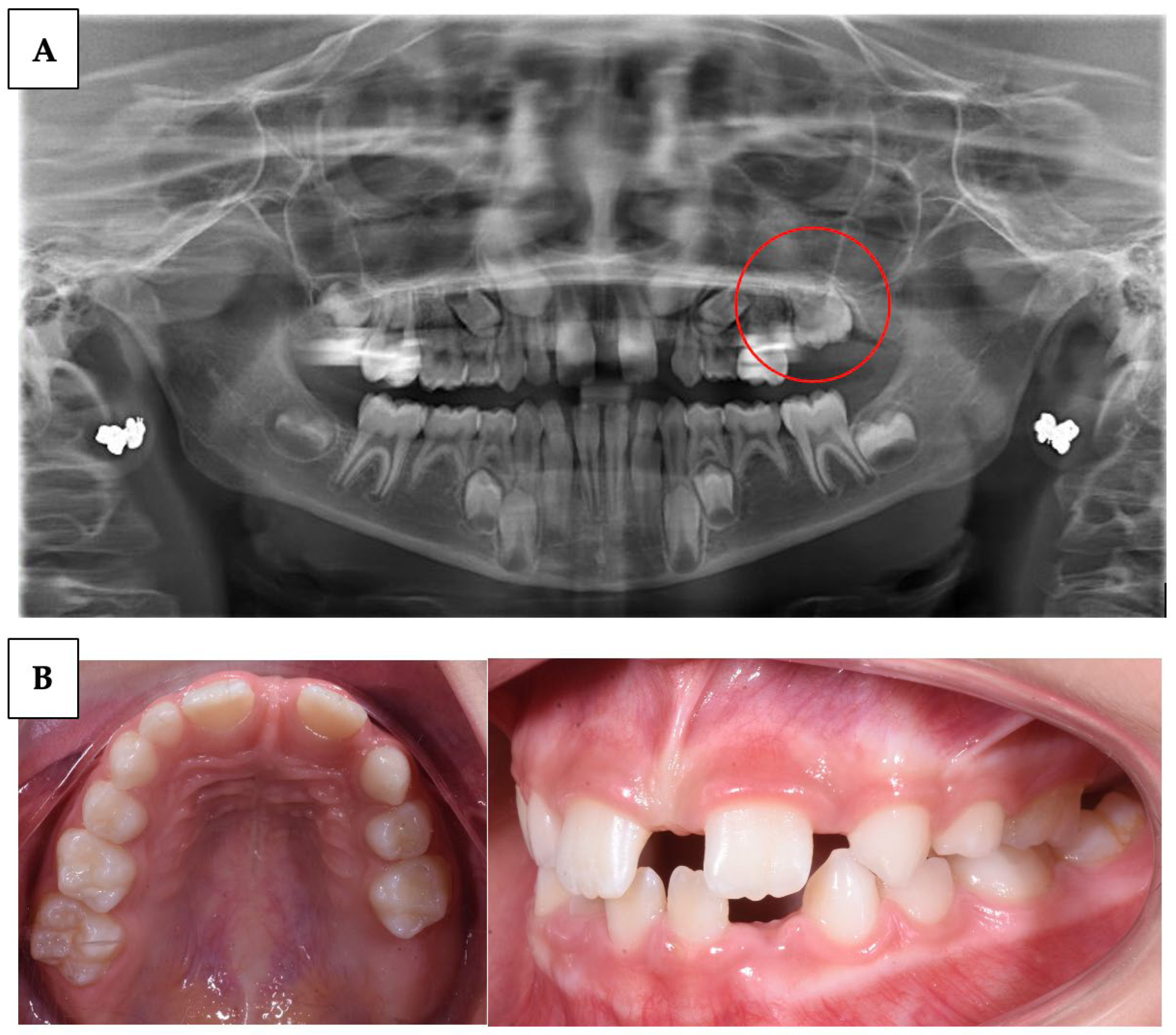
- Delay in tooth eruption: one of the earliest and most obvious signs of PFE is a delay in the eruption of permanent teeth beyond the expected age (Table 1).
- Excess space between teeth: PFE can result in excessive spacing between teeth due to the absence of the unerupted tooth. This can be more noticeable if multiple teeth are involved.
- Malocclusion and dental misalignment: over time, PFE can lead to malocclusion and dental misalignment issues due to the lack of eruptive force on adjacent teeth.
- Tilted or rotated teeth: in some cases, the teeth adjacent to the site of PFE may tilt or rotate in an attempt to fill the space left by the unerupted tooth.
- Pain or sensitivity: in some cases, PFE can be associated with pain or sensitivity (condition in which a sharp, momentary pain is felt in the teeth when they are exposed to certain thermal, chemical, and mechanical stimuli) at the site of failed eruption, although this is not a common sign.
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Sources and Search Strategy
2.3. Study Selection and Characteristics
Quality Assessment
2.4. Results
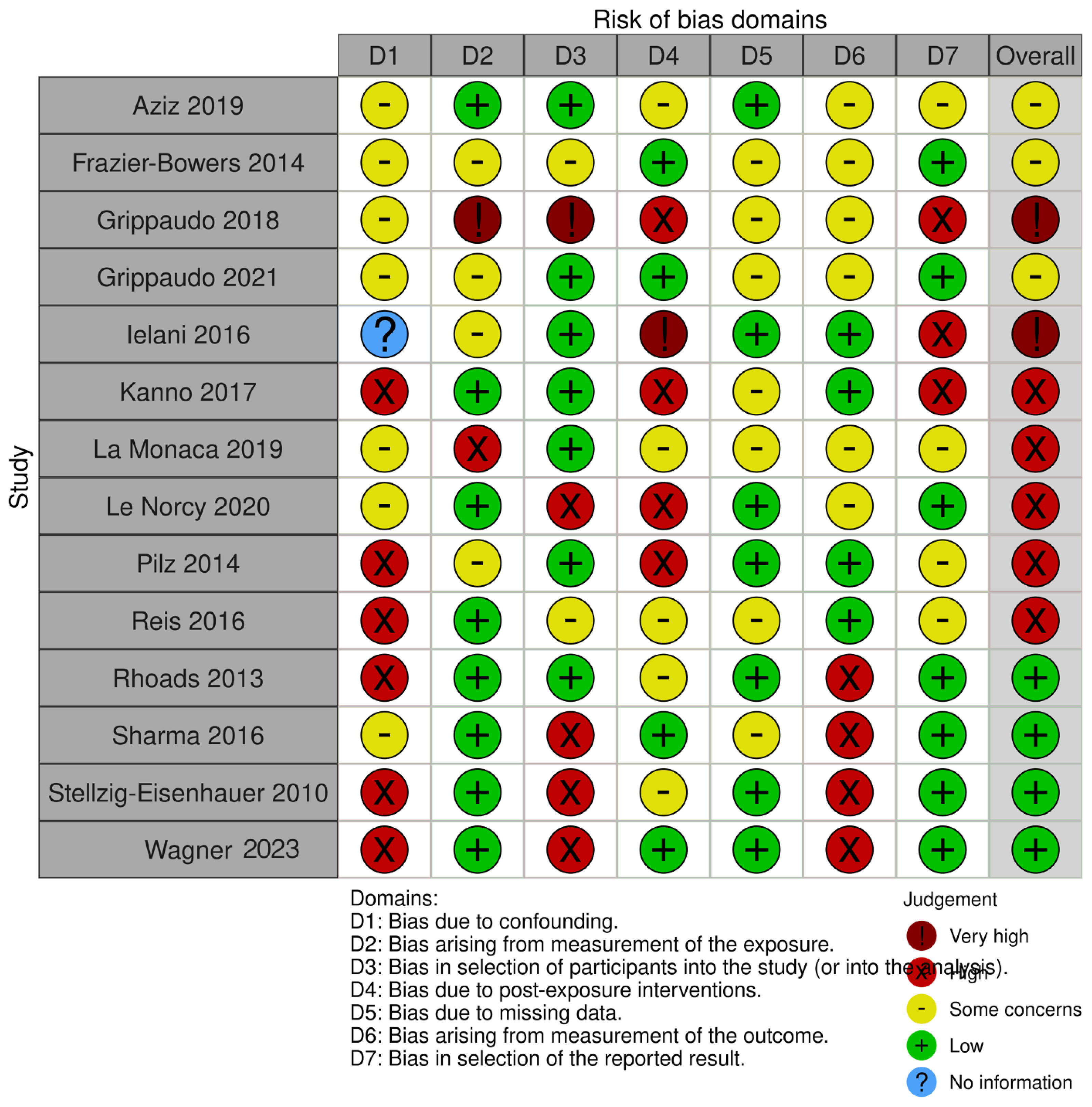
Quality Assessment and Risk of Bias
3. Discussion
3.1. PFE Diagnosis
3.2. Correlation of PFE and PTH1R
3.3. PFE Treatment
4. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PFE | Primary Failure Eruption |
| MFE | Mechanical Failure of Eruption |
| OPT | Orthopantomograph |
| PHP | Pseudohypoparathyroidism |
| PTH | Parathyroid hormone |
| PTHR1 | Parathyroid hormone 1 receptor |
| PTHrP | Parathormone-related protein |
| PTHrP | Parathyroid Hormone related Peptide |
| WSE | Whole-exome sequencing |
References
- Hanisch, M.; Hanisch, L.; Kleinheinz, J.; Jung, S. Primary Failure of Eruption (PFE): A Systematic Review. Head Face Med. 2018, 14, 5. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Med. Kaunas Lith. 2021, 57, 1350. [Google Scholar] [CrossRef]
- Grippaudo, C.; D’Apolito, I.; Cafiero, C.; Re, A.; Chiurazzi, P.; Frazier-Bowers, S.A. Validating Clinical Characteristic of Primary Failure of Eruption (PFE) Associated with PTH1R Variants. Prog. Orthod. 2021, 22, 43. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Inchingolo, A.M.; Dipalma, G. Non-Hodgkin Lymphoma Affecting the Tongue: Unusual Intra-Oral Location. Head Neck Oncol. 2011, 3, 1. [Google Scholar] [CrossRef]
- Baccetti, T. Tooth Anomalies Associated with Failure of Eruption of First and Second Permanent Molars. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 608–610. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Minervini, G.; Lucchese, A.; Perillo, L.; Serpico, R.; Minervini, G. Unilateral Superior Condylar Neck Fracture with Dislocation in a Child Treated with an Acrylic Splint in the Upper Arch for Functional Repositioning of the Mandible. CRANIO® 2017, 35, 337–341. [Google Scholar] [CrossRef]
- Frazier-Bowers, S.A.; Puranik, C.P.; Mahaney, M.C. The Etiology of Eruption Disorders-Further Evidence of a “Genetic Paradigm”. Semin. Orthod. 2010, 16, 180–185. [Google Scholar] [CrossRef]
- Grippaudo, C.; Cafiero, C.; D’Apolito, I.; Ricci, B.; Frazier-Bowers, S.A. Primary Failure of Eruption: Clinical and Genetic Findings in the Mixed Dentition. Angle Orthod. 2018, 88, 275–282. [Google Scholar] [CrossRef]
- Cantore, S.; Mirgaldi, R.; Ballini, A.; Coscia, M.F.; Scacco, S.; Papa, F.; Inchingolo, F.; Dipalma, G.; De Vito, D. Cytokine Gene Polymorphisms Associate with Microbiogical Agents in Periodontal Disease: Our Experience. Int. J. Med. Sci. 2014, 11, 674–679. [Google Scholar] [CrossRef]
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina 2023, 59, 410. [Google Scholar] [CrossRef]
- Vermesan, D.; Inchingolo, F.; Patrascu, J.M.; Trocan, I.; Prejbeanu, R.; Florescu, S.; Damian, G.; Benagiano, V.; Abbinante, A.; Caprio, M.; et al. Anterior Cruciate Ligament Reconstruction and Determination of Tunnel Size and Graft Obliquity. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 357–364. [Google Scholar]
- Dohan Ehrenfest, D.M.; Del Corso, M.; Inchingolo, F.; Sammartino, G.; Charrier, J.-B. Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Human Cell Cultures: Growth Factor Release and Contradictory Results. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2010, 110, 418–421. [Google Scholar] [CrossRef]
- Roulias, P.; Kalantzis, N.; Doukaki, D.; Pachiou, A.; Karamesinis, K.; Damanakis, G.; Gizani, S.; Tsolakis, A.I. Teeth Eruption Disorders: A Critical Review. Children 2022, 9, 771. [Google Scholar] [CrossRef]
- Decker, E.; Stellzig-Eisenhauer, A.; Fiebig, B.S.; Rau, C.; Kress, W.; Saar, K.; Rüschendorf, F.; Hubner, N.; Grimm, T.; Weber, B.H.F. PTHR1 Loss-of-Function Mutations in Familial, Nonsyndromic Primary Failure of Tooth Eruption. Am. J. Hum. Genet. 2008, 83, 781–786. [Google Scholar] [CrossRef]
- Ono, W.; Sakagami, N.; Nishimori, S.; Ono, N.; Kronenberg, H.M. Parathyroid Hormone Receptor Signalling in Osterix-Expressing Mesenchymal Progenitors Is Essential for Tooth Root Formation. Nat. Commun. 2016, 7, 11277. [Google Scholar] [CrossRef]
- Zha, Y.; Li, S.; Yu, Y.; Huang, Z.; Zhang, H.; Kong, W. Identification of a Novel PTH1R Variant in a Family with Primary Failure of Eruption. BMC Oral Health 2023, 23, 509. [Google Scholar] [CrossRef]
- Stellzig-Eisenhauer, A.; Decker, E.; Meyer-Marcotty, P.; Rau, C.; Fiebig, B.S.; Kress, W.; Saar, K.; Rüschendorf, F.; Hubner, N.; Grimm, T.; et al. Primary Failure of Eruption (PFE)–Clinical and Molecular Genetics Analysis. J. Orofac. Orthop. Fortschritte Kieferorthopadie Organ Off. J. Dtsch. Ges. Kieferorthopadie 2010, 71, 6–16. [Google Scholar] [CrossRef]
- Hartsfield, J.K.; Jacob, G.J.; Morford, L.A. Heredity, Genetics and Orthodontics: How Much Has This Research Really Helped? Semin. Orthod. 2017, 23, 336–347. [Google Scholar] [CrossRef]
- Canaff, L.; Zhou, X.; Mosesova, I.; Cole, D.E.C.; Hendy, G.N. Glial Cells Missing-2 (GCM2) Transactivates the Calcium-Sensing Receptor Gene: Effect of a Dominant-Negative GCM2 Mutant Associated with Autosomal Dominant Hypoparathyroidism. Hum. Mutat. 2009, 30, 85–92. [Google Scholar] [CrossRef]
- Pilz, P.; Meyer-Marcotty, P.; Eigenthaler, M.; Roth, H.; Weber, B.H.F.; Stellzig-Eisenhauer, A. Differential Diagnosis of Primary Failure of Eruption (PFE) with and without Evidence of Pathogenic Mutations in the PTHR1 Gene. J. Orofac. Orthop. Fortschritte Kieferorthopadie Organ Off. J. Dtsch. Ges. Kieferorthopadie 2014, 75, 226–239. [Google Scholar] [CrossRef]
- Suri, L.; Gagari, E.; Vastardis, H. Delayed Tooth Eruption: Pathogenesis, Diagnosis, and Treatment. A Literature Review. Am. J. Orthod. Dentofac. Orthop. 2004, 126, 432–445. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Ronsivalle, V.; Shapira, I.; Cicciù, M. Prevalence of Temporomandibular Disorders in Subjects Affected by Parkinson Disease: A Systematic Review and Metanalysis. J. Oral Rehabil. 2023, 50, 877–885. [Google Scholar] [CrossRef]
- Alexander, R.T.; Dimke, H. Effects of Parathyroid Hormone on Renal Tubular Calcium and Phosphate Handling. Acta Physiol. 2023, 238, e13959. [Google Scholar] [CrossRef]
- Lee, J.J.; Plain, A.; Beggs, M.R.; Dimke, H.; Alexander, R.T. Effects of Phospho- and Calciotropic Hormones on Electrolyte Transport in the Proximal Tubule. F1000Research 2017, 6, 1797. [Google Scholar] [CrossRef]
- Dawale, K.; Agrawal, A. Parathyroid Hormone Secretion and Related Syndromes. Cureus 2022, 14, e30251. [Google Scholar] [CrossRef]
- Amberg, G.C.; Navedo, M.F. Calcium Dynamics in Vascular Smooth Muscle. Microcirculation 2013, 20, 281–289. [Google Scholar] [CrossRef]
- Zündorf, G.; Reiser, G. Calcium Dysregulation and Homeostasis of Neural Calcium in the Molecular Mechanisms of Neurodegenerative Diseases Provide Multiple Targets for Neuroprotection. Antioxid. Redox Signal. 2011, 14, 1275–1288. [Google Scholar] [CrossRef]
- Brown, S.J.; Ruppe, M.D.; Tabatabai, L.S. The Parathyroid Gland and Heart Disease. Methodist DeBakey Cardiovasc. J. 2017, 13, 49. [Google Scholar] [CrossRef]
- Suzuki, A.; Minamide, M.; Iwaya, C.; Ogata, K.; Iwata, J. Role of Metabolism in Bone Development and Homeostasis. Int. J. Mol. Sci. 2020, 21, 8992. [Google Scholar] [CrossRef]
- Sato, T.; Courbebaisse, M.; Ide, N.; Fan, Y.; Hanai, J.; Kaludjerovic, J.; Densmore, M.J.; Yuan, Q.; Toka, H.R.; Pollak, M.R.; et al. Parathyroid Hormone Controls Paracellular Ca2+ Transport in the Thick Ascending Limb by Regulating the Tight-Junction Protein Claudin14. Proc. Natl. Acad. Sci. USA 2017, 114, E3344–E3353. [Google Scholar] [CrossRef]
- Khan, M.; Jose, A.; Sharma, S. Physiology, Parathyroid Hormone. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Huckert, M.; Stoetzel, C.; Morkmued, S.; Laugel-Haushalter, V.; Geoffroy, V.; Muller, J.; Clauss, F.; Prasad, M.K.; Obry, F.; Raymond, J.L.; et al. Mutations in the Latent TGF-Beta Binding Protein 3 (LTBP3) Gene Cause Brachyolmia with Amelogenesis Imperfecta. Hum. Mol. Genet. 2015, 24, 3038–3049. [Google Scholar] [CrossRef]
- Malfait, F. Total Absence of the 2(I) Chain of Collagen Type I Causes a Rare Form of Ehlers-Danlos Syndrome with Hypermobility and Propensity to Cardiac Valvular Problems. J. Med. Genet. 2005, 43, e36. [Google Scholar] [CrossRef]
- Wang, S.K.; Reid, B.M.; Dugan, S.L.; Roggenbuck, J.A.; Read, L.; Aref, P.; Taheri, A.P.H.; Yeganeh, M.Z.; Simmer, J.P.; Hu, J.C.-C. FAM20A Mutations Associated with Enamel Renal Syndrome. J. Dent. Res. 2014, 93, 42–48. [Google Scholar] [CrossRef]
- Zhang, H.; Koruyucu, M.; Seymen, F.; Kasimoglu, Y.; Kim, J.-W.; Tinawi, S.; Zhang, C.; Jacquemont, M.L.; Vieira, A.R.; Simmer, J.P.; et al. WDR72 Mutations Associated with Amelogenesis Imperfecta and Acidosis. J. Dent. Res. 2019, 98, 541–548. [Google Scholar] [CrossRef]
- Jain, P.; Rathee, M. Anatomy, Head and Neck, Tooth Eruption. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Roth, H.; Fritsche, L.G.; Meier, C.; Pilz, P.; Eigenthaler, M.; Meyer-Marcotty, P.; Stellzig-Eisenhauer, A.; Proff, P.; Kanno, C.M.; Weber, B.H. Expanding the Spectrum of PTH1R Mutations in Patients with Primary Failure of Tooth Eruption. Clin. Oral Investig. 2014, 18, 377–384. [Google Scholar] [CrossRef]
- Inchingolo, A.M.; Malcangi, G.; Ferrara, I.; Viapiano, F.; Netti, A.; Buongiorno, S.; Latini, G.; Azzollini, D.; De Leonardis, N.; De Ruvo, E.; et al. Laser Surgical Approach of Upper Labial Frenulum: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1302. [Google Scholar] [CrossRef]
- Portales-Castillo, I.; Dean, T.; Khatri, A.; Jüppner, H.; Gardella, T.J. Functional Properties of Two Distinct PTH1R Mutants Associated with Either Skeletal Defects or Pseudohypoparathyroidism. JBMR Plus 2022, 6, e10604. [Google Scholar] [CrossRef]
- Inchingolo, F.; Tatullo, M.; Marrelli, M.; Inchingolo, A.M.; Picciariello, V.; Inchingolo, A.D.; Dipalma, G.; Vermesan, D.; Cagiano, R. Clinical Trial with Bromelain in Third Molar Exodontia. Eur. Rev. Med. Pharmacol. Sci. 2010, 14, 771–774. [Google Scholar]
- Eşian, D.; Bica, C.; Stoica, O.; Dako, T.; Vlasa, A.; Bud, E.; Salcudean, D.; Beresescu, L. Prevalence and Manifestations of Dental Ankylosis in Primary Molars Using Panoramic X-Rays: A Cross-Sectional Study. Children 2022, 9, 1188. [Google Scholar] [CrossRef]
- Chu, F.C.S.; Li, T.K.L.; Lui, V.K.B.; Newsome, P.R.H.; Chow, R.L.K.; Cheung, L.K. Prevalence of Impacted Teeth and Associated Pathologies—A Radiographic Study of the Hong Kong Chinese Population. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2003, 9, 158–163. [Google Scholar]
- Patano, A.; Malcangi, G.; Inchingolo, A.D.; Garofoli, G.; De Leonardis, N.; Azzollini, D.; Latini, G.; Mancini, A.; Carpentiere, V.; Laudadio, C.; et al. Mandibular Crowding: Diagnosis and Management—A Scoping Review. J. Pers. Med. 2023, 13, 774. [Google Scholar] [CrossRef]
- Turner, S.; Harrison, J.E.; Sharif, F.N.; Owens, D.; Millett, D.T. Orthodontic Treatment for Crowded Teeth in Children. Cochrane Database Syst. Rev. 2021, 2022, CD003453. [Google Scholar] [CrossRef]
- Frazier-Bowers, S.A.; Koehler, K.E.; Ackerman, J.L.; Proffit, W.R. Primary Failure of Eruption: Further Characterization of a Rare Eruption Disorder. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2007, 131, 578.e1–578.e11. [Google Scholar] [CrossRef]
- Cahill, D.R. Eruption Pathway Formation in the Presence of Experimental Tooth Impaction in Puppies. Anat. Rec. 1969, 164, 67–77. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies that Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Aziz, S.; Hermann, N.; Duno, M.; Risom, L.; Daugaard-Jensen, J.; Kreiborg, S. Primary Failure of Eruption of Teeth in Two Siblings with a Novel Mutation in the PTH1R Gene. Eur. Arch. Paediatr. Dent. 2019, 20, 295–300. [Google Scholar] [CrossRef]
- Frazier-Bowers, S.A.; Hendricks, H.M.; Wright, J.T.; Lee, J.; Long, K.; Dibble, C.F.; Bencharit, S. Novel Mutations in PTH1R Associated with Primary Failure of Eruption and Osteoarthritis. J. Dent. Res. 2014, 93, 134–139. [Google Scholar] [CrossRef]
- Jelani, M.; Kang, C.; Mohamoud, H.S.A.; Al-Rehaili, R.; Almramhi, M.M.; Serafi, R.; Yang, H.; Al-Aama, J.Y.; Naeem, M.; Alkhiary, Y.M. A Novel Homozygous PTH1R Variant Identified through Whole-Exome Sequencing Further Expands the Clinical Spectrum of Primary Failure of Tooth Eruption in a Consanguineous Saudi Family. Arch. Oral Biol. 2016, 67, 28–33. [Google Scholar] [CrossRef]
- Kanno, C.M.; de Oliveira, J.A.; Garcia, J.F.; Roth, H.; Weber, B.H.F. Twenty-Year Follow-up of a Familial Case of PTH1R-Associated Primary Failure of Tooth Eruption. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 598–606. [Google Scholar] [CrossRef]
- la Monaca, G.; Cristalli, M.P.; Pranno, N.; Galluccio, G.; Annibali, S.; Pippi, R. First and Second Permanent Molars with Failed or Delayed Eruption: Clinical and Statistical Analyses. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2019, 156, 355–364. [Google Scholar] [CrossRef]
- Le Norcy, E.; Reggio-Paquet, C.; de Kerdanet, M.; Mignot, B.; Rothenbuhler, A.; Chaussain, C.; Linglart, A. Dental and Craniofacial Features Associated with GNAS Loss of Function Mutations. Eur. J. Orthod. 2020, 42, 525–533. [Google Scholar] [CrossRef]
- Reis, M.T.A.; Matias, D.T.; de Faria, M.E.J.; Martin, R.M. Failure of Tooth Eruption and Brachydactyly in Pseudohypoparathyroidism Are Not Related to Plasma Parathyroid Hormone-Related Protein Levels. Bone 2016, 85, 138–141. [Google Scholar] [CrossRef]
- Rhoads, S.G.; Hendricks, H.M.; Frazier-Bowers, S.A. Establishing the Diagnostic Criteria for Eruption Disorders Based on Genetic and Clinical Data. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2013, 144, 194–202. [Google Scholar] [CrossRef]
- Sharma, G.; Kneafsey, L.; Ashley, P.; Noar, J. Failure of Eruption of Permanent Molars: A Diagnostic Dilemma. Int. J. Paediatr. Dent. 2016, 26, 91–99. [Google Scholar] [CrossRef]
- Wagner, D.; Rey, T.; Maniere, M.-C.; Dubourg, S.; Bloch-Zupan, A.; Strub, M. Primary Failure of Eruption: From Molecular Diagnosis to Therapeutic Management. J. Oral Biol. Craniofacial Res. 2023, 13, 169–176. [Google Scholar] [CrossRef]
- Subramanian, H.; Döring, F.; Kollert, S.; Rukoyatkina, N.; Sturm, J.; Gambaryan, S.; Stellzig-Eisenhauer, A.; Meyer-Marcotty, P.; Eigenthaler, M.; Wischmeyer, E. PTH1R Mutants Found in Patients with Primary Failure of Tooth Eruption Disrupt G-Protein Signaling. PLoS ONE 2016, 11, e0167033. [Google Scholar] [CrossRef]
- Reddy, L.K.V.; Madithati, P.; Narapureddy, B.R.; Ravula, S.R.; Vaddamanu, S.K.; Alhamoudi, F.H.; Minervini, G.; Chaturvedi, S. Perception about Health Applications (Apps) in Smartphones towards Telemedicine during COVID-19: A Cross-Sectional Study. J. Pers. Med. 2022, 12, 1920. [Google Scholar] [CrossRef]
- Abou Neel, E.; Aljabo, A.; Strange, A.; Ibrahim, S.; Coathup, M.; Young, A.; Bozec, L.; Mudera, V. Demineralization–Remineralization Dynamics in Teeth and Bone. Int. J. Nanomed. 2016, 11, 4743–4763. [Google Scholar] [CrossRef]
- Kamarthi, N.; Venkatraman, S.; Patil, P.B. Dental Findings in the Diagnosis of Idiopathic Hypoparathyroidism. Ann. Saudi Med. 2013, 33, 411–413. [Google Scholar] [CrossRef]
- Karczewski, K.J.; Francioli, L.C.; Tiao, G.; Cummings, B.B.; Alföldi, J.; Wang, Q.; Collins, R.L.; Laricchia, K.M.; Ganna, A.; Birnbaum, D.P.; et al. The Mutational Constraint Spectrum Quantified from Variation in 141,456 Humans. Nature 2020, 581, 434–443. [Google Scholar] [CrossRef]
- Minervini, G.; D’Amico, C.; Cicciù, M.; Fiorillo, L. Temporomandibular Joint Disk Displacement: Etiology, Diagnosis, Imaging, and Therapeutic Approaches. J. Craniofac. Surg. 2023, 34, 1115–1121. [Google Scholar] [CrossRef]
- Tokavanich, N.; Gupta, A.; Nagata, M.; Takahashi, A.; Matsushita, Y.; Yatabe, M.; Ruellas, A.; Cevidanes, L.; Maki, K.; Yamaguchi, T.; et al. A Three-dimensional Analysis of Primary Failure of Eruption in Humans and Mice. Oral Dis. 2020, 26, 391–400. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ferrara, I.; Viapiano, F.; Netti, A.; Campanelli, M.; Buongiorno, S.; Latini, G.; Carpentiere, V.; Ciocia, A.M.; Ceci, S.; et al. Rapid Maxillary Expansion on the Adolescent Patient: Systematic Review and Case Report. Children 2022, 9, 1046. [Google Scholar] [CrossRef]
- Siegel, S.C.; O’Connell, A. Oral Rehabilitation of a Child with Primary Failure of Tooth Eruption. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 1999, 8, 201–207. [Google Scholar] [CrossRef]
- Di Stasio, D.; Romano, A.; Gentile, C.; Maio, C.; Lucchese, A.; Serpico, R.; Paparella, R.; Minervini, G.; Candotto, V.; Laino, L. Systemic and Topical Photodynamic Therapy (PDT) on Oral Mucosa Lesions: An Overview. J. Biol. Regul Homeost Agents 2018, 32, 123–126. [Google Scholar]
- Sehra, B.; Johnson, J. The Prosthetic Management of an Infra-Occluded First Permanent Molar: Case Report. Dent. Update 2016, 43, 482–484, 486. [Google Scholar] [CrossRef]
- Risom, L.; Christoffersen, L.; Daugaard-Jensen, J.; Hove, H.D.; Andersen, H.S.; Andresen, B.S.; Kreiborg, S.; Duno, M. Identification of Six Novel PTH1R Mutations in Families with a History of Primary Failure of Tooth Eruption. PLoS ONE 2013, 8, e74601. [Google Scholar] [CrossRef]
- Aruna, U. Primary Failure of Eruption—A Case Report with Cone Beam Computerized Tomographic Imaging. J. Clin. Diagn. Res. 2014, 8, ZD14. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lower first molars | 6–7 years |
| Upper first molars | 6–7 years |
| Lower central incisors | 6–7 years |
| Upper central incisors | 7–8 years |
| Lateral lower incisors | 7–8 years |
| Upper lateral incisors | 8–9 years |
| Upper canines | 9–10 years |
| Inferior canines | 9–10 years |
| Inferior premolars | 9–10 years |
| Upper premolars | 10–12 years |
| Lower second molars | 11–13 years |
| Upper second molars | 11–13 years |
| Third molars | 17–25 years |
| Author (Year) | Study Design | Number of Patients | Aim of the Study | Material and Methods | Results |
|---|---|---|---|---|---|
| Aziz et al. (2019) [50] | Case series | 3 | To mark a PFE family with mutation of the PTH1R genus in primary and permanent dentition. | Clinical examination, radiological examination, and molecular DNA testing. | Once growth is complete, various multidisciplinary treatment strategies can partially resolve the posterior open bite malocclusion that is characteristic of this disorder. |
| Frazier- Bowers S.A. et al. (2014) [51] | RCT | 61 | Familial PFE genetic variants can be inherited in an insufficiently penetrant way and may be linked to an early start of osteoarthritis. | Polymerase chain reaction-based mutational analysis confirmed PTH1R’s genetic role in 10 families with PFE. Two new autosomal dominant variants (c.996_997insC and C.572delA) were discovered in ten families and seven solitary individuals. | PTH1R autosomal dominant mutations cause PFE and osteoarthritis; a dose-dependent model may explain isolated osteoarthritis and PFE without known skeletal system symptoms. |
| Grippaudo C. et al. (2018) [10] | RCT | 51 | To investigate the possibility that both primary and permanent teeth may be affected by mutations in the parathyroid hormone 1 receptor (PTH1R). | A study of 29 individuals with infraoccluded teeth involved saliva samples, DNA retrieval, and sequencing of PTH1R gene coding regions. Mutations were examined for genetic information. | The PTH1R gene contains novel mutations affecting primary molars affected by PFE, paving the way for early genetic diagnostics and appropriate care. |
| Grippaudo et al. (2021) [3] | RCT | 44 | To interrogate and validate the correlation between clinical features and the presence of PTH1R variants in a cohort of patients with suspected PFE and their family members. | Clinical and genetic analysis (PTH1R sequencing). | Patients with pathogenic variants of the PTH1R gene exhibit clinical traits of PFE. Genetic testing identifies PTH1R variants in about 64% of PFE patients. |
| Jelani M. et al. (2016) [52] | Case Series | 6 | Utilizing whole-exome sequencing (WES) analysis, determine the genetic aetiology of the non-syndromic main failure of dental eruption in a five-generation related Saudi family. | Researchers performed WES on all four afflicted family members using the 51 Mb SureSelect V4 library kit, followed by Illumina HiSeq2000 sequencing. | The results demonstrate the usefulness of WES as a molecular diagnostics tool for this uncommon condition and extend the clinical range of PTH1R pathogenicity. |
| Kanno et al. (2017) [53] | Case series | 18 | Determine the genetic and clinical characteristics of a family with 11 PFE-affected members after 20 years of observation. | Clinical and genetic analysis. | PFE disrupts periodontal ligament metabolism, increasing genetically determined ankylosis. Severe open bites occur earlier, and affected teeth maintain eruptive potential even in adulthood. |
| La Monaca et al. (2019) [54] | Retrospective study | 125 | The objective of this study was to examine information from patients experiencing either unsuccessful or delayed eruption of their first and second permanent molars, with the goal of evaluating the efficacy of the treatment approaches employed. | The authors classified eruption disorders based on root development, using terms like “retention” and “inclusion” to describe molars before and after apical root closure. They also used “early diagnosed condition” to describe anatomical, topographical, or pathological conditions that could interfere with eruption processes. | The article highlights that treatment outcomes are most favourable for younger patients with undeveloped molar roots, with early diagnosis and prompt action significantly impacting effectiveness. Surgery uprighting has the highest success rate, while surgical-orthodontic uprighting has a lower success rate. |
| Le Norcy E. et al. (2020) [55] | RCT | 19 | Researchers investigated dental, oral, and craniofacial characteristics in offspring with iPPSD2 and maternal GNAS inactivating mutations to determine malformation prevalence and specificity. | To determine the prevalence and specificity of the defects, they performed a thorough examination of dental and craniofacial characteristics in 19 individuals with iPPSD2 and maternal GNAS inactivating mutations. | Patients with parental GNAS mutations and iPPSD2 developed particular dental and craniofacial malformations. |
| Pilz et al. (2014) [22] | Retrospective study | 36 | This study’s goal was to determine whether it is possible to distinguish between PTHR1-mutation carriers and noncarriers based on radiological and clinical findings. | This study found that posterior teeth are more frequently affected, with eruption disturbances, resorption of alveolar bone coronal, involvement of both deciduous and permanent teeth, impaired vertical alveolar-process growth, and severe posterior open bite findings. | It Is possible to significantly improve the specificity of selecting non-affected patients from among suspected instances of PFE associated with PTHR1 gene mutations by carefully assessing clinical and radiographic parameters. |
| Reis et al. (2016) [56] | Cross sectional study | 19 | To investigate patients with PTH resistance and molecular diagnosis of PHP and evaluate dental and radiological manifestations associated with the condition. | Genetic tests were conducted on GNAS and STX16 genes linked to PHP syndromes. Biochemical analyses measured serum calcium, phosphate, PTH, and PTHrP levels. Radiological and dental evaluations were performed using DPR to detect FTE and dental anomalies. | Identified mutations and methylation defects in the GNAS gene associated with PTH in a group of patients. Radiological and dental evaluation detected the presence of incomplete tooth eruption and other dental anomalies in patients with the condition. |
| Rhoads et al. (2013) [57] | Retrospective study | 64 | Define the clinical diagnostic criteria that separate PFE from other eruption disorders, particularly ankylosis, by utilizing a special dataset. | PFE is diagnosed by a PTH1R gene mutation, with clinical criteria including permanent first molar involvement, supracrestal presentation, eruption path obstruction, second premolar involvement, multiple adjacent teeth, bilateral presentation, Class III malocclusion, and dental abnormalities. | PFE is a condition affecting first molars, adjacent teeth, and adjacent teeth. It can cause infraoccluded second premolars and bilateral affection. In absence of trauma, treatment history, genetic information, or periodontal ligament obliteration, PFE and ankylosis may be clinically indistinguishable. |
| Sharma et al. (2016) [58] | Retrospective descriptive study | 29 (15 as PFE and 14 as MFE) | Identify management techniques and confirm diagnostic criteria that will help differentiate between PFE MFE of permanent molars. | PFE affects the first molar and can cause unerupted or partially erupted teeth, causing open bites and a clear eruption pathway in patients. It can affect distal teeth, primary dentition, and multiple teeth. | The authors suggest a protocol in the form of a flow diagram based on the findings of the study and current protocols to help with the appropriate diagnosis and management of PFE and MFE. |
| Stellzig-Eisenhauer et al. (2010) [19] | Case series | 15 | Identify a genetically verified diagnosis of PFE to improve treatment choice. | Clinical and Molecular Genetics Analysis | Molecular genetic analysis of the PTHR1 gene revealed three distinct heterozygous mutations. Unaffected patients exhibited no mutations. |
| Wagner et al. (2023) [59] | Case series | 3 | Describe the variability of clinical presentations of PFE associated with pathogenic variants of PTHR1 | Clinical examination, radiological examination, and molecular DNA testing | Multidisciplinary complex treatment, from child to adulthood. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inchingolo, F.; Ferrara, I.; Viapiano, F.; Ciocia, A.M.; Palumbo, I.; Guglielmo, M.; Inchingolo, A.D.; Palermo, A.; Bordea, I.R.; Inchingolo, A.M.; et al. Primary Failure Eruption: Genetic Investigation, Diagnosis and Treatment: A Systematic Review. Children 2023, 10, 1781. https://doi.org/10.3390/children10111781
Inchingolo F, Ferrara I, Viapiano F, Ciocia AM, Palumbo I, Guglielmo M, Inchingolo AD, Palermo A, Bordea IR, Inchingolo AM, et al. Primary Failure Eruption: Genetic Investigation, Diagnosis and Treatment: A Systematic Review. Children. 2023; 10(11):1781. https://doi.org/10.3390/children10111781
Chicago/Turabian StyleInchingolo, Francesco, Irene Ferrara, Fabio Viapiano, Anna Maria Ciocia, Irene Palumbo, Mariafrancesca Guglielmo, Alessio Danilo Inchingolo, Andrea Palermo, Ioana Roxana Bordea, Angelo Michele Inchingolo, and et al. 2023. "Primary Failure Eruption: Genetic Investigation, Diagnosis and Treatment: A Systematic Review" Children 10, no. 11: 1781. https://doi.org/10.3390/children10111781
APA StyleInchingolo, F., Ferrara, I., Viapiano, F., Ciocia, A. M., Palumbo, I., Guglielmo, M., Inchingolo, A. D., Palermo, A., Bordea, I. R., Inchingolo, A. M., Di Venere, D., & Dipalma, G. (2023). Primary Failure Eruption: Genetic Investigation, Diagnosis and Treatment: A Systematic Review. Children, 10(11), 1781. https://doi.org/10.3390/children10111781