
Left Atrial Geometry and Phasic Function Determined by Cardiac Magnetic Resonance Are Independent Predictors for Outcome in Non-Ischaemic Dilated Cardiomyopathy

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients’ Characteristics
2.2. CMR Imaging
2.3. CMR Analysis
2.3.1. Quantitative Assessment of the LV Functions
2.3.2. Quantitative Assessment LA Volume and Function
2.4. Follow-Up of Clinical Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Characterization of LV Systolic and Diastolic Functions
3.3. Characterization of LA Phasic Function and Geometry
3.4. Correlations between LA Function, Geometry, and LV Function Parameters in Patients with NIDCM
3.5. Univariate and Multivariate Analysis of LA Function and Geometry Parameters
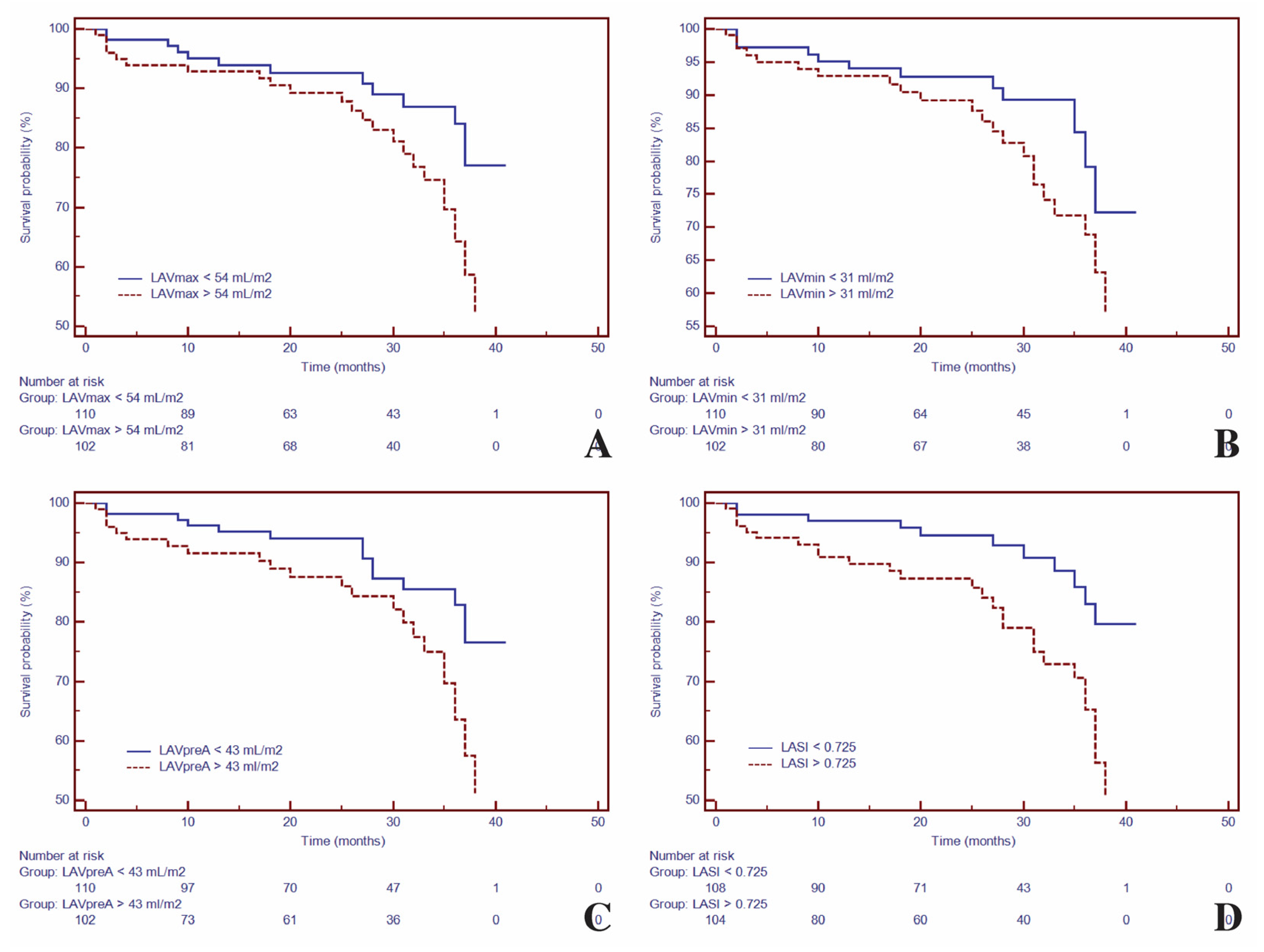
3.6. Time to Event Analysis and Incremental Predictive Ability of LA Function and Geometry Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Pinto, Y.M.; Elliott, P.M.; Arbustini, E.; Adler, Y.; Anastasakis, A.; Böhm, M.; Duboc, D.; Gimeno, J.; de Groote, P.; Imazio, M.; et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: A position statement of the ESC working group on myocardial and pericardial diseases. Eur. Heart J. 2016, 37, 1850–1858. [Google Scholar] [CrossRef]
- Modena, M.G.; Muia, N.; Sgura, F.A.; Molinari, R.; Castelli, A.; Rossi, R. Left atrial size is the major predictor of cardiac death and overall clinical outcome in patients with dilated cardiomyopathy: A long-term follow-up study. Clin. Cardiol. 1997, 20, 553–560. [Google Scholar] [CrossRef]
- Dini, F.L.; Cortigiani, L.; Baldini, U.; Boni, A.; Nuti, R.; Barsotti, L.; Micheli, G. Prognostic value of left atrial enlargement in patients with idiopathic dilated cardiomyopathy and ischemic cardiomyopathy. Am. J. Cardiol. 2002, 89, 518–523. [Google Scholar] [CrossRef]
- Kuchynka, P.; Podzimkova, J.; Masek, M.; Lambert, L.; Cerny, V.; Danek, B.; Palecek, T. The Role of Magnetic Resonance Imaging and Cardiac Computed Tomography in the Assessment of Left Atrial Anatomy, Size, and Function. Biomed Res. Int. 2015, 2015, 1–13. [Google Scholar] [CrossRef][Green Version]
- Blume, G.G.; Mcleod, C.J.; Barnes, M.E.; Seward, J.B.; Pellikka, P.A.; Bastiansen, P.M.; Tsang, T.S.M. Left atrial function: Physiology, assessment, and clinical implications. Eur. J. Echocardiogr. 2011, 12, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Hear. J.–Cardiovasc. Imaging 2015, 16, 233–271. [Google Scholar] [CrossRef]
- Matsuda, Y.; Toma, Y.; Ogawa, H.; Matsuzaki, M.; Katayama, K.; Fujii, T.; Yoshino, F.; Moritani, K.; Kumada, T.; Kusukawa, R. Importance of left atrial function in patients with myocardial infarction. Circulation 1983, 67, 566–571. [Google Scholar] [CrossRef]
- Gan, G.C.H.; Ferkh, A.; Boyd, A.; Thomas, L. Left atrial function: Evaluation by strain analysis. Cardiovasc. Diagn. Ther. 2018, 8, 29–46. [Google Scholar] [CrossRef]
- Truong, V.T.; Palmer, C.; Wolking, S.; Sheets, B.; Young, M.; Ngo, T.N.M.; Taylor, M.; Nagueh, S.F.; Zareba, K.M.; Raman, S.; et al. Normal left atrial strain and strain rate using cardiac magnetic resonance feature tracking in healthy volunteers. Eur. Hear. J.–Cardiovasc. Imaging 2019. [Google Scholar] [CrossRef] [PubMed]
- Rosca, M.; Lancellotti, P.; Popescu, B.A.; Pierard, L.A. Left atrial function: Pathophysiology, echocardiographic assessment, and clinical applications. Heart 2011, 97, 1982–1989. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Sardana, M.; Ansari, B.; Satija, V.; Kuriakose, D.; Edelstein, I.; Oldland, G.; Miller, R.; Gaddam, S.; Lee, J.; et al. Left Atrial Phasic Function by Cardiac Magnetic Resonance Feature Tracking Is a Strong Predictor of Incident Cardiovascular Events. Circ. Cardiovasc. Imaging 2018, 11. [Google Scholar] [CrossRef]
- Kowallick, J.T.; Kutty, S.; Edelmann, F.; Chiribiri, A.; Villa, A.; Steinmetz, M.; Sohns, J.M.; Staab, W.; Bettencourt, N.; Unterberg-Buchwald, C.; et al. Quantification of left atrial strain and strain rate using Cardiovascular Magnetic Resonance myocardial feature tracking: A feasibility study. J. Cardiovasc. Magn. Reson. 2014, 16, 60. [Google Scholar] [CrossRef]
- Thomas, L.; Marwick, T.H.; Popescu, B.A.; Donal, E.; Badano, L.P. Left Atrial Structure and Function, and Left Ventricular Diastolic Dysfunction. J. Am. Coll. Cardiol. 2019, 73, 1961–1977. [Google Scholar] [CrossRef] [PubMed]
- Hoit, B.D. Left Atrial Size and Function. J. Am. Coll. Cardiol. 2014, 63, 493–505. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Hear. J.–Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Patel, D.A.; Lavie, C.J.; Gilliland, Y.E.; Shah, S.B.; Dinshaw, H.K.; Milani, R.V. Prediction of All-Cause Mortality by the Left Atrial Volume Index in Patients With Normal Left Ventricular Filling Pressure and Preserved Ejection Fraction. Mayo Clin. Proc. 2015, 90, 1499–1505. [Google Scholar] [CrossRef]
- Khan, M.A.; Yang, E.Y.; Zhan, Y.; Judd, R.M.; Chan, W.; Nabi, F.; Heitner, J.F.; Kim, R.J.; Klem, I.; Nagueh, S.F.; et al. Association of left atrial volume index and all-cause mortality in patients referred for routine cardiovascular magnetic resonance: A multicenter study. J. Cardiovasc. Magn. Reson. 2019, 21, 4. [Google Scholar] [CrossRef]
- Bisbal, F.; Guiu, E.; Calvo, N.; Marin, D.; Berruezo, A.; Arbelo, E.; Ortiz-Pérez, J.; de Caralt, T.M.; Tolosana, J.M.; Borràs, R.; et al. Left Atrial Sphericity: A New Method to Assess Atrial Remodeling. Impact on the Outcome of Atrial Fibrillation Ablation. J. Cardiovasc. Electrophysiol. 2013, 24, 752–759. [Google Scholar] [CrossRef]
- Nakamori, S.; Ngo, L.H.; Tugal, D.; Manning, W.J.; Nezafat, R. Incremental Value of Left Atrial Geometric Remodeling in Predicting Late Atrial Fibrillation Recurrence After Pulmonary Vein Isolation: A Cardiovascular Magnetic Resonance Study. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef]
- Yazaki, M.; Nabeta, T.; Inomata, T.; Maemura, K.; Oki, T.; Fujita, T.; Ikeda, Y.; Ishii, S.; Naruke, T.; Inoue, Y.; et al. Clinical significance of left atrial geometry in dilated cardiomyopathy patients: A cardiovascular magnetic resonance study. Clin. Cardiol. 2021, 44, 222–229. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J. Cardiovasc. Magn. Reson. 2013, 15, 91. [Google Scholar] [CrossRef]
- Bollache, E.; Redheuil, A.; Clément-Guinaudeau, S.; Defrance, C.; Perdrix, L.; Ladouceur, M.; Lefort, M.; De Cesare, A.; Herment, A.; Diebold, B.; et al. Automated left ventricular diastolic function evaluation from phase-contrast cardiovascular magnetic resonance and comparison with Doppler echocardiography. J. Cardiovasc. Magn. Reson. 2010, 12, 63. [Google Scholar] [CrossRef]
- Liang, Y.; Li, W.; Zeng, R.; Sun, J.; Wan, K.; Xu, Y.; Cao, Y.; Zhang, Q.; Han, Y.; Chen, Y. Left Ventricular Spherical Index Is an Independent Predictor for Clinical Outcomes in Patients With Nonischemic Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2019, 12, 1578–1580. [Google Scholar] [CrossRef]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart. Circulation 2002, 105, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Bondarenko, O.; Beek, A.; Hofman, M.; Kühl, H.; Twisk, J.; van Dockum, W.; Visser, C.; van Rossum, A. Standardizing the Definition of Hyperenhancement in the Quantitative Assessment of Infarct Size and Myocardial Viability Using Delayed Contrast-Enhanced CMR. J. Cardiovasc. Magn. Reson. 2005, 7, 481–485. [Google Scholar] [CrossRef]
- Habibi, M.; Zareian, M.; Ambale Venkatesh, B.; Samiei, S.; Imai, M.; Wu, C.; Launer, L.J.; Shea, S.; Gottesman, R.F.; Heckbert, S.R.; et al. Left Atrial Mechanical Function and Incident Ischemic Cerebrovascular Events Independent of AF. JACC Cardiovasc. Imaging 2019, 12, 2417–2427. [Google Scholar] [CrossRef]
- Reiber, J.H.C.; Alaiti, A.; Bezerra, H.G.; De Sutter, J.; Schoenhagen, P.; Stillman, A.E.; Van de Veire, N.R.L. Cardiovascular imaging 2017 in the International Journal of Cardiovascular Imaging. Int. J. Cardiovasc. Imaging 2018, 34, 833–848. [Google Scholar] [CrossRef]
- Farhad, H.; Seidelmann, S.B.; Vigneault, D.; Abbasi, S.A.; Yang, E.; Day, S.M.; Colan, S.D.; Russell, M.W.; Towbin, J.; Sherrid, M.V.; et al. Left Atrial structure and function in hypertrophic cardiomyopathy sarcomere mutation carriers with and without left ventricular hypertrophy. J. Cardiovasc. Magn. Reson. 2017, 19, 107. [Google Scholar] [CrossRef]
- Liu, S.; Ma, C.; Ren, W.; Zhang, J.; Li, N.; Yang, J.; Zhang, Y.; Qiao, W. Regional left atrial function differentiation in patients with constrictive pericarditis and restrictive cardiomyopathy: A study using speckle tracking echocardiography. Int. J. Cardiovasc. Imaging 2015, 31, 1529–1536. [Google Scholar] [CrossRef]
- Welles, C.C.; Ku, I.A.; Kwan, D.M.; Whooley, M.A.; Schiller, N.B.; Turakhia, M.P. Left Atrial Function Predicts Heart Failure Hospitalization in Subjects With Preserved Ejection Fraction and Coronary Heart Disease. J. Am. Coll. Cardiol. 2012, 59, 673–680. [Google Scholar] [CrossRef]
- Zhu, M.; Chen, H.; Liu, Y.; Shu, X. Clinical implication of disturbed left atrial phasic functions in the heterogeneous population associated with hypertension or atrial fibrillation. Cardiovasc. Ultrasound 2019, 17, 25. [Google Scholar] [CrossRef] [PubMed]
- Yamano, M.; Yamano, T.; Iwamura, Y.; Nakamura, T.; Shiraishi, H.; Shirayama, T.; Matoba, S. Impact of Left Ventricular Diastolic Property on Left Atrial Function from Simultaneous Left Atrial and Ventricular Three-Dimensional Echocardiographic Volume Measurement. Am. J. Cardiol. 2017, 119, 1687–1693. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.-C.; Huang, Y.-Y.; Liu, Y.-W.; Shih, J.-Y.; Lin, C.-C.; Tsai, L.-M. Changes of Left Atrial Phasic Function Assessed by Speckle Tracking Echocardiography in Untreated Hypertension. J. Med. Ultrasound 2012, 20, 220–227. [Google Scholar] [CrossRef]
- Yang, Y.; Yin, G.; Jiang, Y.; Song, L.; Zhao, S.; Lu, M. Quantification of left atrial function in patients with non-obstructive hypertrophic cardiomyopathy by cardiovascular magnetic resonance feature tracking imaging: A feasibility and reproducibility study. J. Cardiovasc. Magn. Reson. 2020, 22, 1. [Google Scholar] [CrossRef]
- Nappo, R.; Degiovanni, A.; Bolzani, V.; Sartori, C.; Di Giovine, G.; Cerini, P.; Fossaceca, R.; Kovács, S.J.; Marino, P.N. Quantitative assessment of atrial conduit function: A new index of diastolic dysfunction. Clin. Res. Cardiol. 2016, 105, 17–28. [Google Scholar] [CrossRef]
- Tadic, M.; Vukomanovic, V.; Cuspidi, C.; Suzic-Lazic, J.; Stanisavljevic, D.; Celic, V. Left atrial phasic function and heart rate variability in asymptomatic diabetic patients. Acta Diabetol. 2017, 54, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Tadic, M.; Genger, M.; Cuspidi, C.; Belyavskiy, E.; Frydas, A.; Dordevic, A.; Morris, D.A.; Völkl, J.; Parwani, A.S.; Pieske, B.; et al. Phasic Left Atrial Function in Cancer Patients Before Initiation of Anti-Cancer Therapy. J. Clin. Med. 2019, 8, 421. [Google Scholar] [CrossRef]
- Carluccio, E.; Biagioli, P.; Mengoni, A.; Francesca Cerasa, M.; Lauciello, R.; Zuchi, C.; Bardelli, G.; Alunni, G.; Coiro, S.; Gronda, E.G.; et al. Left Atrial Reservoir Function and Outcome in Heart Failure With Reduced Ejection Fraction. Circ. Cardiovasc. Imaging 2018, 11. [Google Scholar] [CrossRef]
- Yazaki, M.; Nabeta, T.; Inomata, T.; Maemura, K.; Oki, T.; Fujita, T.; Ikeda, Y.; Ishii, S.; Naruke, T.; Ako, J. Clinical significance of left atrial geometry in patients with dilated cardiomyopathy: A cardiovascular magnetic resonance study. Eur. Heart J. 2020, 41. [Google Scholar] [CrossRef]
- Shi, J.; Xu, S.; Chen, L.; Wu, B.; Yang, K.; Chen, S.; Zhou, D.; Zhang, B.; Xuan, T.; Hu, X. Impact of Left Atrial Sphericity Index on the Outcome of Catheter Ablation for Atrial Fibrillation. J. Cardiovasc. Transl. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Quail, M.; Grunseich, K.; Baldassarre, L.A.; Mojibian, H.; Marieb, M.A.; Cornfeld, D.; Soufer, A.; Sinusas, A.J.; Peters, D.C. Prognostic and functional implications of left atrial late gadolinium enhancement cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2019, 21, 2. [Google Scholar] [CrossRef]
- Habibi, M.; Chahal, H.; Opdahl, A.; Gjesdal, O.; Helle-Valle, T.M.; Heckbert, S.R.; McClelland, R.; Wu, C.; Shea, S.; Hundley, G.; et al. Association of CMR-Measured LA Function With Heart Failure Development. JACC Cardiovasc. Imaging 2014, 7, 570–579. [Google Scholar] [CrossRef]
- Gulati, A.; Ismail, T.F.; Jabbour, A.; Ismail, N.A.; Morarji, K.; Ali, A.; Raza, S.; Khwaja, J.; Brown, T.D.H.; Liodakis, E.; et al. Clinical utility and prognostic value of left atrial volume assessment by cardiovascular magnetic resonance in non-ischaemic dilated cardiomyopathy. Eur. J. Heart Fail. 2013, 15, 660–670. [Google Scholar] [CrossRef] [PubMed]
- Habibi, M.; Samiei, S.; Ambale Venkatesh, B.; Opdahl, A.; Helle-Valle, T.M.; Zareian, M.; Almeida, A.L.C.; Choi, E.-Y.; Wu, C.; Alonso, A.; et al. Cardiac Magnetic Resonance–Measured Left Atrial Volume and Function and Incident Atrial Fibrillation. Circ. Cardiovasc. Imaging 2016, 9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NIDCM All Patients n = 212 | Healthy Volunteers n = 106 | p-Value | |
|---|---|---|---|
| Clinical characteristics | |||
| - Age, mean (SD), years | 49 (14.2) | 49 (11.8) | NS |
| - Male gender, n (%) | 156 (73.5) | 75 (70.2) | NS |
| - Body-mass index, kg/m2 | 27.4 (4.7) | 27.8 (4.8) | NS |
| - Heart rate, mean (SD), bpm | 73 (12.8) | 73 (15.8) | NS |
| - Systolic blood pressure, mean (SD), mmHg | 134 (19.1) | 122 (17.2) | |
| - Hypertension, n (%) | 51 (24.0) | 20 (18.9) | <0.01 |
| - Diabetes mellitus, n (%) | 40 (18.8) | 15 (14.1) | <0.01 |
| - Dyslipidemia, n (%) | 96 (45.2) | 49 (46.2) | NS |
| - Smoking, n (%) | 64 (30.2) | 37 (34.9) | NS |
| Biomarker levels | |||
| - NT-proBNP, median (IQR), pg/mL | 2679 (378–11,960) | 223 (60–391) | <0.001 |
| - eGFR, mean (SD), mL/min/1.73 m2 | 86.4 (20.1) | 87.4 (16.8) | NS |
| - PICP, median (IQR), ng/mL | 1.45 (0.42–9.2) | 0.47 (0.31–5.1) | <0.001 |
| - PIIINP, median (IQR), ng/mL | 15.6 (2.7–79.1) | 8.2 (2.1–23.5) | <0.001 |
| - Galectin-3, median (IQR), ng/mL | 13.9 (2.2–21.6) | 4.8 (1.2–12.8) | <0.001 |
| Variables | NIDCM All Patients n = 212 | Healthy Volunteers n = 106 | p-Value |
|---|---|---|---|
| LV and RV systolic parameters | |||
| - LVEDV index, mL/m2 | 131.5 (36.5) | 63.1 (18.6) | <0.001 |
| - LVESV index, mL/m2 | 87.1 (36.2) | 21.6 (7.4) | <0.001 |
| - LVM index, g/m2 | 86.1 (20.1) | 58.4 (14.1) | <.001 |
| - LVEF, % | 35.5 (10.1) | 65.7 (5.6) | <0.001 |
| - LAS, % | −9.5 (5.4) | −20.0 (2.7) | <0.001 |
| - LVSI | 0.40 (0.12) | 0.18 (0.05) | <0.001 |
| - LV-LGE mass, g | 34.4 (13.1) | - | NA |
| - LV-LGE mass/LVM, % | 18.1 (7.7) | - | NA |
| - RVEDV index, mL/m2 | 57.1 (24.0) | 59.0 (19.3) | NS |
| - RVESV index, mL/m2 | 31.2 (17.6) | 22.5 (8.1) | <0.001 |
| - RVEF, % | 46.8 (9.5) | 61.8 (5.7) | <0.001 |
| - TAPSE, mm | 16.6 (5.1) | 21.2 (2.9) | <0.001 |
| LV diastolic parameters | |||
| - E, cm/s | 52.1 (12.2) | 75.5 (9.3) | <0.001 |
| - A, cm/s | 34.5 (9.4) | 47.2 (6.9) | NS |
| - DT, ms | 210 (80.3) | 182 (58.5) | <0.001 |
| - IVRT, ms | 60 (18.7) | 88 (18.1) | NS |
| - E’, cm/s | 6.2 (2.3) | 5.8 (2.2) | <0.01 |
| - A’, cm/s | 4.7 (1.2) | 3.4 (1.3) | NS |
| - E/A ratio | 1.46 (0.93) | 1.85 (0.73) | <0.05 |
| - E/E’ratio | 9.5 (2.8) | 6.5 (1.5) | <0.001 |
| - EQ, mL/s | 243 (112.8) | 344 (90.7) | <0.001 |
| - AQ, mL/s | 213 (122.5) | 205 (75.2) | NS |
| - EQ/LVEDV, s−1 | 1.99 (0.61) | 3.83 (1.42) | <0.001 |
| - EQ /FV, s−1 | 4.01 (1.2) | 4.9 (0.82) | NS |
| - FV, mL | 61.9 (21.4) | 71.7 (20.1) | NS |
| Variables | NIDCM All Patients n = 212 | Healthy Volunteers n = 106 | p-Value |
|---|---|---|---|
| LA volumes indexed | |||
| - LAVmax index, mL/m2 | 56.1 (21.7) | 34.0 (6.2) | <0.001 |
| - LAVmin index, mL/m2 | 32.4 (9.5) | 14.0 (2.7) | <0.001 |
| - LAVpre-A index, mL/m2 | 45.3 (11.1) | 24.1 (4.7) | <0.001 |
| Reservoir function | |||
| - LATF, % | 43.7 (8.5) | 58.9 (2.9) | <0.001 |
| - LA-εt, (%) | 31.5 (2.4) | 39.8 (2.8) | <0.001 |
| Conduit function | |||
| - LAPF, % | 20.9 (7.2) | 29.1 (8.4) | <0.001 |
| - LA-εp, (%) | 16.0 (4.1) | 17.9 (2.7) | <0.001 |
| Atrial booster function | |||
| - LAAF, % | 28.6 (9.6) | 41.3 (8.3) | <0.001 |
| - LA-εa, (%) | 20.6 (2.5) | 29.2 (3.6) | <0.001 |
| LA geometry | |||
| - LASI | 0.77 (0.23) | 0.39 (0.06) | <0.001 |
| - LA-LGE +, n (%) | 121 (57) | - | NA |
| Severe mitral regurgitation, n (%) | 60 (28.3) | - | NA |
| LA Phasic Function Parameters | ||||||
|---|---|---|---|---|---|---|
| LATF | LAPF | LAAF | LA-εt | LA-εp | LA-εa | |
| LA geometry parameters | ||||||
| LAVmax index, mL/m2 | −0.489 (<0.0001) | −0.201 (0.003) | −0.464 (<0.0001) | −0.459 (<0.0001) | −0.222 (0.001) | −0.394 (<0.0001) |
| LAVmin index, mL/m2 | −0.817 (<0.0001) | −0.419 (<0.0001) | −0.713 (<0.0001) | −0.663 (<0.0001) | −0.273 (<0.001) | −0.597 (<0.0001) |
| LAVpre-A index, mL/m2 | −0.682 (<0.0001) | −0.519 (<0.0001) | −0.484 (<0.0001) | −0.641 (<0.0001) | −0.208 (0.002) | −0.602 (<0.0001) |
| LASI | −0.587 (<0.0001) | −0.263 (<0.001) | −0.546 (<0.0001) | −0.635 (<0.0001) | −0.277 (<0.001) | −0.565 (<0.0001) |
| LV conventional function | ||||||
| LVEDV index, mL/m2 | −0.583 (<0.0001) | −0.336 (<0.0001) | −0.500 (<0.0001) | −0.655 (<0.0001) | −0.199 (0.004) | −0.627 (<0.0001) |
| LVESV index, mL/m2 | −0.593 (<0.0001) | −0.343 (<0.0001) | −0.506 (<0.0001) | −0.661 (<0.0001) | −0.201 (0.003) | −0.634 (<0.0001) |
| LVEF, % | 0.673 (<0.0001) | 0.386 (<0.0001) | 0.576 (<0.0001) | 0.765 (<0.0001) | 0.223 (0.001) | 0.736 (<0.0001) |
| LVSI | −0.150 (0.02) | −0.170 (0.01) | −0.058 (0.39) | −0.156 (0.02) | −0.073 (0.28) | −0.114 (0.09) |
| LAS, % | −0.618 (<0.0001) | −0.336 (<0.0001) | −0.537 (<0.0001) | −0.628 (<0.0001) | −0.175 (0.018) | −0.619 (<0.0001) |
| E/E’ ratio | −0.400 (<0.0001) | −0.260 (<0.001) | −0.313 (<0.0001) | −0.387 (<0.0001) | −0.063 (0.26) | −0.399 (<0.0001) |
| Univariate HR (95%CI) | Multivariate | ||||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | ||
| LAVmax index | 1.02 (1.01–1.03) p < 0.01 | 1.01 (1.00–1.02) p < 0.01 | 1.02 (1.00–1.03) p < 0.01 | 1.01 (1.01–1.03) p < 0.01 | 1.02 (1.00–1.05) p < 0.001 |
| LAVmin index | 1.03 (1.00–1.04) p < 0.01 | 1.04 (1.01–1.07) p <0.01 | 1.05 (1.02–1.08) p <0.001 | 1.03 (1.00–1.07) p < 0.01 | 1.04 (1.02–1.07) p < 0.001 |
| LAVpre-A index | 1.03 (1.01–1.05) p < 0.01 | 1.06 (1.01–1.06) p < 0.01 | 1.07 (1.02–1.12) p < 0.001 | 1.05 (1.01–1.07) p < 0.001 | 1.06 (1.04–1.11) p < 0.001 |
| LASI | 2.07 (1.37–4.52) p < 0.001 | 1.83 (1.22–4.10) p < 0.001 | 1.74 (1.02–3.77) p < 0.001 | 1.76 (1.14–3.18) p < 0.001 | 1.16 (1.03–1.32) p < 0.01 |
| LA-LGE | 3.83 (1.90–7.71) p < 0.001 | 4.12 (2.03–8.31) p = 0.0001 | 4.03 (1.95–8.31) p < 0.001 | 4.04 (1.95–8.33) p < 0.001 | 4.52 (2.03–10.06) p = 0.0001 |
| LA-εt | 4.14 (2.09–8.18) p < 0.0001 | 4.46 (2.23–8.91) p < 0.0001 | 4.38 (2.18–8.77) p < 0.0001 | 4.61 (2.27–9.36) p < 0.0001 | 3.81 (1.78–8.12) p < 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cojan-Minzat, B.O.; Zlibut, A.; Muresan, I.D.; Orzan, R.-I.; Cionca, C.; Horvat, D.; David, L.; Visan, A.C.; Florea, M.; Agoston-Coldea, L. Left Atrial Geometry and Phasic Function Determined by Cardiac Magnetic Resonance Are Independent Predictors for Outcome in Non-Ischaemic Dilated Cardiomyopathy. Biomedicines 2021, 9, 1653. https://doi.org/10.3390/biomedicines9111653
Cojan-Minzat BO, Zlibut A, Muresan ID, Orzan R-I, Cionca C, Horvat D, David L, Visan AC, Florea M, Agoston-Coldea L. Left Atrial Geometry and Phasic Function Determined by Cardiac Magnetic Resonance Are Independent Predictors for Outcome in Non-Ischaemic Dilated Cardiomyopathy. Biomedicines. 2021; 9(11):1653. https://doi.org/10.3390/biomedicines9111653
Chicago/Turabian StyleCojan-Minzat, Bianca Olivia, Alexandru Zlibut, Ioana Danuta Muresan, Rares-Ilie Orzan, Carmen Cionca, Dalma Horvat, Liliana David, Alexandru Ciprian Visan, Mira Florea, and Lucia Agoston-Coldea. 2021. "Left Atrial Geometry and Phasic Function Determined by Cardiac Magnetic Resonance Are Independent Predictors for Outcome in Non-Ischaemic Dilated Cardiomyopathy" Biomedicines 9, no. 11: 1653. https://doi.org/10.3390/biomedicines9111653
APA StyleCojan-Minzat, B. O., Zlibut, A., Muresan, I. D., Orzan, R.-I., Cionca, C., Horvat, D., David, L., Visan, A. C., Florea, M., & Agoston-Coldea, L. (2021). Left Atrial Geometry and Phasic Function Determined by Cardiac Magnetic Resonance Are Independent Predictors for Outcome in Non-Ischaemic Dilated Cardiomyopathy. Biomedicines, 9(11), 1653. https://doi.org/10.3390/biomedicines9111653