Abstract
Background/Objective: Early-onset diabetes (EOD), diagnosed at ≤35 years, is a growing public health crisis in low- and middle-income countries, including Pakistan. Identifying modifiable and non-modifiable risk factors is critical for developing effective prevention strategies. This study aimed to investigate the risk factors associated with EOD in Sindh, Pakistan, focusing on genetic, lifestyle, and metabolic determinants. Methods: A multicenter cross-sectional study was conducted across diabetic clinics in Sindh, with primary data collection at Baqai Institute of Diabetology and Endocrinology (Karachi, Pakistan) and secondary sites in Hyderabad, Larkana, and Sukkur. Following institutional ethical approval and informed consent, we enrolled 754 individuals (type 1 and type 2 diabetes, age at diagnosis: 15–35 years). Data on anthropometric, clinical, biochemical, and lifestyle parameters were collected via structured questionnaires. Statistical analyses included Pearson’s Chi Square tests and multivariate logistic regression in determining associations. Results: Logistic regression revealed key predictors of early-onset diabetes (EOD). A two-generation diabetes family history showed a strong association (aOR:1.86, 1.12–3.43). Significant lifestyle risks included physical inactivity (OR:1.40, 1.03–1.90), frequent sugary beverage intake (OR:1.93, 1.89–1.98), and abnormal sleep duration (<6 h: OR:1.58, 1.04–2.40; >8 h: OR:1.86, 1.21–2.85). Hypertension was a major metabolic predictor (elevated BP: OR:1.79, 1.28–1.54; Stage I: OR:1.81, 1.34–1.77). Cardiovascular disease and uncontrolled fasting glucose lost significance after adjustment, indicating confounding effects. Conclusions: This study highlights familial predisposition, sedentary behavior, poor diet, sleep disturbances, and hypertension as key contributors to EOD in young Pakistani adults. Early screening and targeted lifestyle interventions are urgently needed to mitigate this escalating epidemic.
1. Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia resulting from impaired insulin secretion, insulin resistance, or both [1]. This dysregulation disrupts carbohydrate, lipid, and protein metabolism, leading to systemic complications such as microvascular damage, accelerated atherosclerosis, and end-organ dysfunction [2]. The global burden of DM has reached epidemic proportions, with an estimated 537 million cases (10.5% of adults) reported in 2021, disproportionately affecting low- and middle-income countries (LMICs), which account for 81% of cases [3,4]. Rapid urbanization, obesogenic environments, and sedentary lifestyles have fueled this rise, particularly in regions undergoing nutritional and epidemiological transitions [5].
Of particular concern is the increasing incidence of early-onset diabetes (EOD; diagnosis ≤35 years), which poses distinct clinical and public health challenges [6]. Younger patients face accelerated disease progression, higher risks of micro- and macrovascular complications (e.g., nephropathy, retinopathy, and premature cardiovascular disease), and greater lifetime healthcare demands [7,8]. The etiology of EOD is multifactorial, driven by genetic predisposition (e.g., familial aggregation, epigenetic modifications), modifiable lifestyle factors (e.g., physical inactivity, excessive sugar-sweetened beverage consumption), and developmental origins (e.g., maternal diabetes, intrauterine metabolic programming) [9,10,11].
According to the International Diabetes Federation (IDF), Pakistan ranks third globally in terms of the number of adults with diabetes, with an estimated 33 million people affected and an overall national prevalence of 26.7% among adults aged 20–79 years [12,13]. While national data indicate a growing tendency of diabetes among younger individuals in Pakistan, with nearly 18% of diagnosed cases occurring in those under the age of 40 [14], there is a significant lack of region-specific data on early-onset diabetes (EOD). In particular, no large-scale study has been conducted to investigate the onset of diabetes in the 15–35-year age group within the province of Sindh. A prior study, however, identified generalized risk factors (e.g., obesity, smoking, urbanicity); data on population-specific determinants of EOD remain scarce [15]. This gap is critical, as ethnic and regional variations in genetic susceptibility, dietary patterns, and healthcare access may modulate risk [16].
This study investigated the risk factors for EOD (ages 15–35 years) in Sindh, Pakistan, with a focus on behavioral, clinical, and sociodemographic predictors. We hypothesized that specific modifiable factors such as poor dietary habits, physical inactivity, obesity, smoking, and socioeconomic status are significantly associated with an increased risk of developing EOD in this population. By elucidating these determinants, our findings aim to inform targeted prevention strategies, mitigate long-term complications, and reduce the economic burden of DM in high-risk populations.
2. Materials and Methods
A multicentre, cross-sectional observational study was conducted across tertiary-care diabetic clinics in Sindh, Pakistan, with primary data collection at the Baqai Institute of Diabetology and Endocrinology (Karachi, Pakistan) and secondary sites in Hyderabad, Larkana, and Sukkur. Participants aged 15–35 years with a confirmed diagnosis of type 1 or type 2 diabetes (per ADA criteria) were enrolled. Exclusion criteria included neonatal diabetes mellitus, hypoglycemia of infancy, and maternally inherited diabetes and deafness (MIDD) to minimize confounding genetic influences.
Given the absence of prior prevalence data for this age group in Sindh, a conservative estimate of 50% prevalence was assumed. Using OpenEpi v3.0 (95% CI, 5% margin of error), the minimum sample size was n = 348. To enhance statistical power and generalizability, n = 754 participants were recruited. The study protocol was approved by the Institutional Review and Ethics Board (IREB) of Baqai Medical University (BMU-IREB/03-2023). Written informed consent was obtained from all participants prior to enrolment.
A structured questionnaire administered by trained personnel captured the sociodemographic and clinical data, including demographics (age, sex, education, occupation, household income), family history (diabetes in first- and second-degree relatives), lifestyle behaviors (physical activity per WHO guidelines), dietary habits (fruit/vegetable intake, junk food frequency), tobacco use, sleep duration, and stress levels. Anthropometric and blood pressure measurements were also recorded, like height/weight measured barefoot using a Viva Stadiometer and Beurer digital scale [17]; BMI was calculated as kg/m2 (adults) or percentiles (adolescents; WHO standards) [18]. Blood pressures were measured as averaged from three seated readings (5 min intervals) via a mercury sphygmomanometer, classified per ACC/AHA 2017 guidelines.
Fasting blood glucose (FBG) measured via GOD-PAP method (Selectra Pro-S analyzer, ELITech Group Inc., Puteaux, France) [19]. HbA1c quantified by HPLC (EDTA tubes) [20] by transporting the samples are 4 °C and analyzed within 24 h.
Data were analyzed using IBM SPSS v23.0 by means of descriptive statistics using frequencies, mean ± SD. Bivariate analysis was performed using Pearson’s χ2 tests for categorical variables. Multivariate analysis was conducted using binary logistic regression (adjusted for age and BMI) to estimate adjusted odds ratios (ORs) with 95% CIs. Statistical significance was set at p < 0.05. The following operational definitions were used in this study: BMI categories: underweight (<18.5 kg/m2), normal (18.5–24.9), overweight (25–29.9), obese (≥30) [21]; hypertension staging: per ACC/AHA criteria [22] (Normal, Elevated, Stage I/II); glycemic control: ADA-defined thresholds (HbA1c >7%; FBG 80–130 mg/dL) [23]; physical activity: WHO recommendations (≥150 min/week moderate or ≥75 min vigorous) [24]; dietary adequacy: WHO’s ≥400 g/day (5 portions) of fruits/vegetables [25].
3. Results
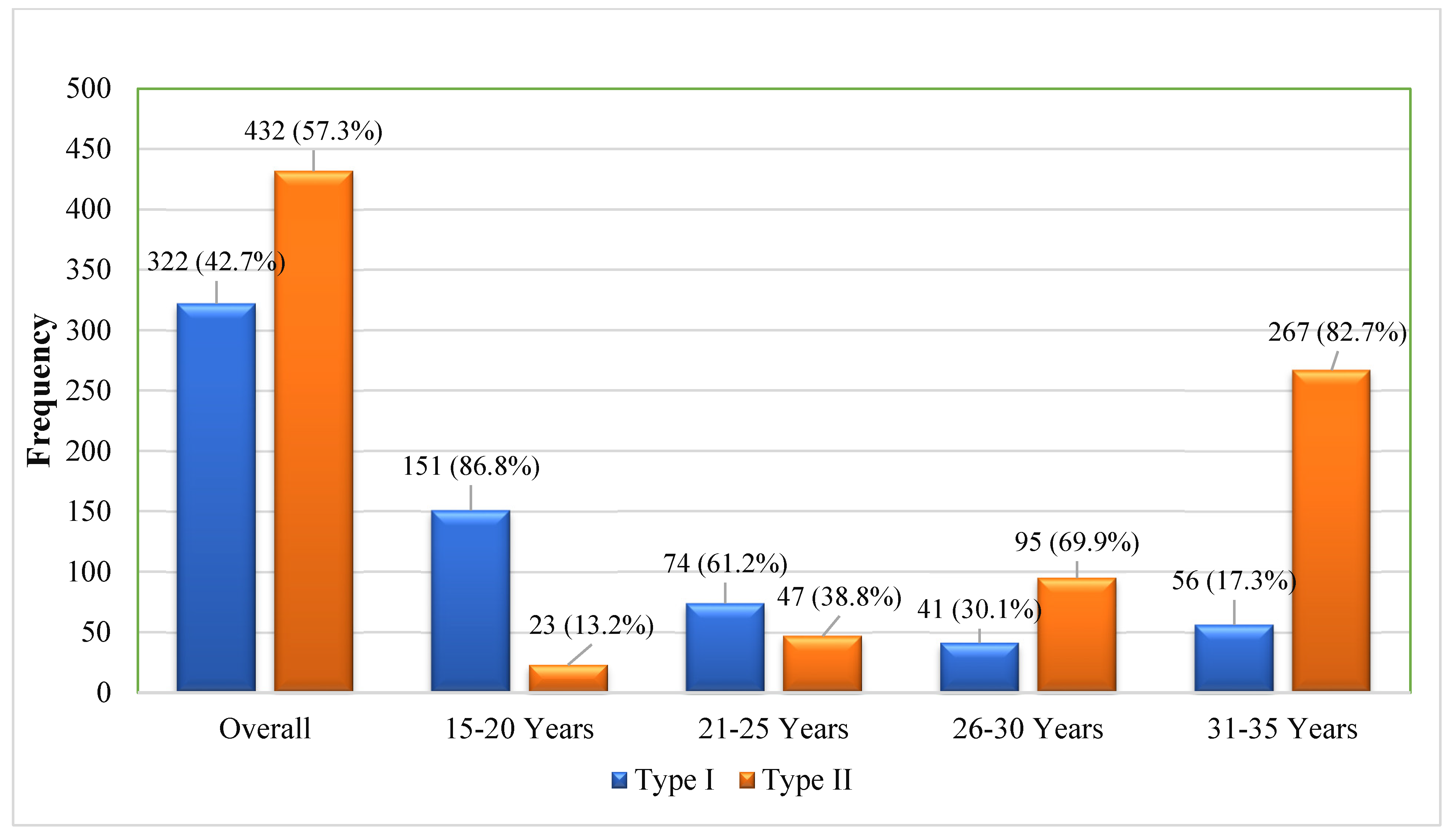
The study population (N = 754) comprised 322 cases (42.7%) of type 1 diabetes mellitus (T1DM) and 432 cases (57.3%) of type 2 diabetes mellitus (T2DM), with a mean age at diagnosis of 26.14 ± 6.53 years. Age-stratified analysis revealed the expected predominance of T1DM in younger cohorts (15–19 years) and T2DM in older participants (31–35 years; 86.7%). Notably, we observed atypical presentations, including T1DM in older age groups and T2DM in younger individuals (Figure 1).
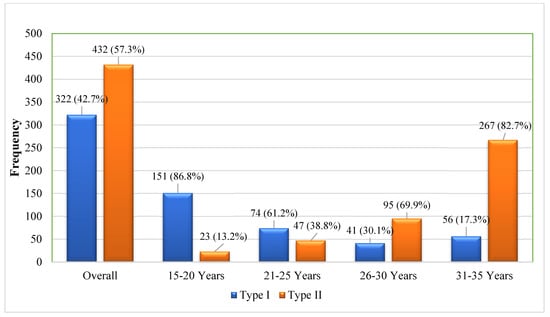
Figure 1.
Distribution of diabetes by age group.
The participant’s characteristics, categorized by age groups (15–19, 20–24, 25–29, and 30–35 years) are given in Table 1. No significant difference was seen for gender and ethnicity across the age groups, with a slightly high ratio of males (51.7%). However, a significant difference was observed in educational levels (p < 0.001), marital status (p < 0.001), and occupation (p < 0.001). Similarly, the family history of diabetes also showed a significant difference (p = 0.023). It was noted that no history of diabetes was mostly seen in the age group of 15–19 years (32.2%), while a family history of diabetes in two generations was found in the age group of 31–35 years (58.5%).

Table 1.
Baseline characteristics of EOD (age of diagnosis <35 years).
Overall, 78 (10.0%) of the participants were smokers, 83 (11.0%) were using smokeless tobacco, and 149 (19.8%) were former smokers. However, no significant difference was seen. Similarly, 501 (66.4%) participants were physically inactive, and a significant association among age groups was seen (p = 0.006), with inadequate physical activity being more prevalent in the older age group (30–35 years) at 71.8% compared with other age groups (Table 1).
The consumption of sugar-added beverages, fruit and vegetable intake, junk food consumption, and diabetes medications did not show statistically significant associations with age groups. 548 (72.7%) participants were having 6–8 optimal sleep. Sleep duration also showed a significant association (p = 0.003), with a higher percentage of participants 259 (80.2%) in the age group of 31–35 years as shown in Table 2.
Table 2.
Analysis of behavioral factors among EOD (age of diagnosis <35 years).
The study population demonstrated significant variations in weight status across age groups (p < 0.001). Among participants, 29.8% (n = 225) were classified as overweight and 25.7% (n = 194) as obese. Younger age groups showed a higher prevalence of underweight (22.4%) and normal weight (49.4%) status, while older participants (31–35 years) exhibited greater proportions of overweight (34.7%) and obesity (36.4%).
Blood pressure measurements revealed significant age-related differences (p < 0.001). Elevated blood pressure was identified in 41.0% (n = 309) of participants, with Stage I hypertension in 19.1% (n = 144) and Stage II hypertension in 1.5% (n = 11). Notably, the highest prevalence of elevated blood pressure (47.4%) and Stage I hypertension (19.8%) occurred in the 31–35 years age group.
Metabolic abnormalities were prevalent in the study population, with hypercholesterolemia present in 48.4% (n = 365) of participants, though without significant age-related variation (p = 0.176). Cardiovascular disease affected 15.6% (n = 118) of the cohort and demonstrated significant association with age (p = 0.01), showing peak prevalence (24.8%) in the 20–25 years age group. Glycemic control analysis revealed uncontrolled fasting blood glucose levels across all age groups (p = 0.043). In contrast, elevated HbA1c levels (>7%) were consistently observed throughout the population without significant age-related differences (p = 0.357) (Table 3).
Table 3.
Analysis of metabolic and biochemical factors among EOD (age of diagnosis <35 years).
Univariate analysis identified several significant predictors of early-onset diabetes (all p < 0.05), including a two-generation family history of diabetes, physical inactivity, excessive sugary beverage consumption, abnormal sleep duration (<6 or >8 h/night), elevated blood pressure, stage I/II hypertension, cardiovascular disease, and uncontrolled fasting blood sugar. While the male gender showed a non-significant trend toward increased risk (p > 0.05), the remaining associations were statistically significant. In the multivariate model adjusted for age and BMI, only a two-generation family history of diabetes (OR: 1.96, 95% CI: 1.12–3.43) and abnormal sleep duration (OR: 1.84, 95% CI: 1.14–2.97) maintained strong independent associations. Several factors that were significant in univariate analysis—including elevated blood pressure, sugary beverage consumption, and physical inactivity—showed attenuated associations after adjustment (p < 0.05), suggesting potential confounding effects of age and BMI (Table 4).
Table 4.
Risk assessment of EOD with studied factors.
4. Discussion
This study provides critical insights into the epidemiology of early-onset diabetes in Sindh, Pakistan, revealing a multifaceted interplay of genetic, metabolic, and lifestyle risk factors. The high prevalence of type 2 diabetes (57.3%) among young adults (15–35 years) aligns with the Second National Diabetes Survey of Pakistan, which reported the highest provincial diabetes prevalence (32.2%) in Sindh, suggesting unique regional pathophysiological mechanisms may be at play [26]. In contrast with global patterns where type 1 diabetes typically predominates under 20 years and type 2 diabetes tends to emerge after 35 years [27], our findings regarding type 1 diabetes distribution challenge conventional paradigms. While type 1 diabetes represented 42.7% of cases overall, its prevalence in adults (20–35 years) was substantial (17.3–61.2%), supporting emerging evidence of significant adult-onset type 1 diabetes. This has important diagnostic implications, as adult-onset type 1 diabetes may initially present with clinical features resembling type 2 diabetes. The absence of comprehensive epidemiological data on adult-onset type 1 diabetes in Pakistan underscores the urgent need for population-based studies incorporating autoantibody testing.
The strong association between two-generation family history and early-onset diabetes, which persisted after multivariate adjustment, reinforces the crucial role of genetic predisposition. This finding extends previous research demonstrating familial aggregation of diabetes risk and suggests that in this population, multigenerational exposure may confer greater risk than single-generation family history [28]. Notably, this association remained significant even after controlling for BMI, indicating that genetic susceptibility operates independently of adiposity in this cohort.
Physical inactivity (prevalence: 66.4%) and excessive sugary beverage consumption emerged as significant modifiable risk factors, particularly among younger participants (15–25 years). These findings highlight the need for targeted lifestyle interventions in this demographic. Abnormal sleep duration (<6 or >8 h) showed a U-shaped association with diabetes risk, supporting growing evidence [29] of circadian disruption in metabolic dysregulation.
The relationship between blood pressure abnormalities and diabetes risk revealed important nuances. While elevated blood pressure and hypertension stages I–II showed strong univariate associations, these attenuated after multivariate adjustment, suggesting that they may mediate rather than independently predict diabetes risk in this population. Cardiovascular disease demonstrated complex associations, with significant univariate but attenuated multivariate effects, aligning with recent findings on the interplay between familial cardiovascular risk and diabetes [30].
These findings have important clinical and public health implications. The high prevalence of modifiable risk factors suggests that targeted lifestyle interventions could substantially reduce diabetes incidence in this vulnerable population. Lifestyle interventions at this stage can effectively delay or prevent the progression of diabetes and its long-term complications, such as cardiovascular disease, nephropathy, and neuropathy. The emphasis on these preventable factors is essential for reducing both individual and public health burdens in the future. The significant burden of adult-onset type 1 diabetes calls for improved diagnostic protocols incorporating autoantibody testing in young adults. Family history assessment should be prioritized in clinical screening, particularly for normal-weight individuals, and integrated cardiometabolic risk reduction programs should be developed for high-risk youth.
To the best of our knowledge, this is the first study to comprehensively explore the risk factors associated with EOD among individuals aged 15–35 years across major districts of Sindh, Pakistan. No prior research from this region has specifically targeted this age group or assessed risk factors with a focus on modifiable components. Moreover, previous regional data have not clearly differentiated between types of diabetes in this age group, often leading to misclassification or underreporting. Our study explicitly distinguishes and documents confirmed cases of type 1 and type 2 diabetes based on ADA criteria and clinical follow-up, thus contributing to accurate epidemiological data and supporting the maintenance of more precise health records for young individuals with diabetes.
Several study limitations warrant consideration, including the cross-sectional design, potential recall bias in self-reported measures, lack of autoantibody testing, and single-region sampling. Nevertheless, this study provides compelling evidence that early-onset diabetes in Sindh results from complex interactions between genetic susceptibility and modifiable lifestyle factors. The findings underscore the urgent need for enhanced screening protocols, culturally tailored prevention strategies, and further research into adult-onset type 1 diabetes epidemiology to address the growing burden of early-onset diabetes in Pakistan and similar populations undergoing rapid epidemiological transition.
5. Conclusions and Recommendations
This study elucidates the multifactorial etiology of early-onset diabetes in Sindh, Pakistan, demonstrating significant contributions from both non-modifiable (genetic predisposition) and modifiable (lifestyle-related) risk factors. The predominance of type 2 diabetes in young adults, coupled with substantial rates of adult-onset type 1 diabetes, underscores the complex diabetes phenotype in this population. Our findings highlight the critical need for a dual approach to diabetes prevention and management in Pakistan: (1) enhanced clinical recognition of atypical presentations through improved diagnostic protocols, including family history assessment and autoantibody testing where indicated, and (2) population-level interventions targeting modifiable risk factors such as physical inactivity, unhealthy dietary patterns, and sleep hygiene. The persistent association of two-generation family history with diabetes risk, independent of BMI, suggests that genetic and epigenetic factors may play an especially important role in this population. These results call for immediate public health action, including the development of culturally appropriate, age-specific prevention programs and the integration of diabetes screening with cardiovascular risk assessment.
Future longitudinal studies incorporating objective measures of lifestyle factors and genetic markers are warranted to better understand the temporal relationships and gene-environment interactions underlying early-onset diabetes in South Asian populations. Addressing this growing epidemic will require coordinated efforts across healthcare systems, policymakers, and community organizations to implement effective prevention strategies and reduce the future burden of diabetes-related complications in Pakistan’s young population.
Author Contributions
Conceptualization, E.A. and M.A.N.S.; methodology, E.A. and I.A.S.; software, M.A.; validation, E.A., M.A. and M.S.A.; formal analysis, E.A.; investigation, E.A. and A.F.; resources, A.F.; data curation, E.A. and M.A.N.S.; writing—original draft preparation, E.A. and S.M.S.; writing—review and editing, E.A. and S.M.S.; visualization, M.A.; supervision, M.A.N.S. and I.A.S.; project administration, E.A.; funding acquisition, M.A.N.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Higher Education Commission (HEC), Pakistan through NRPU Grant No. 15917.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review and Ethics Board (IREB) of Baqai Medical University (BMU) vide approval # BMU-IREB/03-2023 (7 August 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed at the corresponding author.
Acknowledgments
The authors acknowledge all participants of the study for their time. We are deeply thankful to the team members and laboratory staff at Baqai Institute of Diabetology and Endocrinology (BIDE), Baqai Medical University (BMU) for their endless support in data collection.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cloete, L. Diabetes mellitus: An overview of the types, symptoms, complications and management. Nurs. Stand. 2022, 37, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Gangwar, R.; Zargar, A.A.; Kumar, R.; Sharma, A. Prevalence of Diabetes in India: A Review of IDF Diabetes Atlas 10th Edition. Curr. Diabetes Rev. 2024, 20, e130423215752. [Google Scholar] [CrossRef] [PubMed]
- Kengne, A.P.; Ramachandran, A. Feasibility of prevention of type 2 diabetes in low- and middle-income countries. Diabetologia 2024, 67, 763–772. [Google Scholar] [CrossRef] [PubMed]
- Golovaty, I.; Ritchie, N.D.; Tuomilehto, J.; Mohan, V.; Ali, M.K.; Gregg, E.W.; Bergman, M.; Moin, T. Two decades of diabetes prevention efforts: A call to innovate and revitalize our approach to lifestyle change. Diabetes Res. Clin. Pract. 2023, 198, 110195. [Google Scholar] [CrossRef]
- Hossain, M.J.; Al-Mamun, M.; Islam, M.R. Diabetes mellitus, the fastest growing global public health concern: Early detection should be focused. Health Sci. Rep. 2024, 7, e2004. [Google Scholar] [CrossRef]
- Pan, J.; Jia, W. Early-onset diabetes: An epidemic in China. Front. Med. 2018, 12, 624–633. [Google Scholar] [CrossRef]
- Kyrou, I.; Tsigos, C.; Mavrogianni, C.; Cardon, G.; Van Stappen, V.; Latomme, J.; Kivelä, J.; Wikström, K.; Tsochev, K.; Nanasi, A.; et al. Sociodemographic and lifestyle-related risk factors for identifying vulnerable groups for type 2 diabetes: A narrative review with emphasis on data from Europe. BMC Endocr. Disord. 2020, 20 (Suppl. 1), 134. [Google Scholar] [CrossRef]
- Serbis, A.; Giapros, V.; Kotanidou, E.P.; Galli-Tsinopoulou, A.; Siomou, E. Diagnosis, treatment and prevention of type 2 diabetes mellitus in children and adolescents. World J. Diabetes 2021, 12, 344–365. [Google Scholar] [CrossRef]
- Schnurr, T.M.; Jakupović, H.; Carrasquilla, G.D.; Ängquist, L.; Grarup, N.; Sørensen, T.I.A.; Tjønneland, A.; Overvad, K.; Pedersen, O.; Hansen, T.; et al. Obesity, unfavourable lifestyle and genetic risk of type 2 diabetes: A case-cohort study. Diabetologia 2020, 63, 1324–1332. [Google Scholar] [CrossRef]
- Negrato, C.A.; Martins, R.L.M.; Louro, M.D.; Medeiros, G.A.; Lanzarin, J.V.M.; Zajdenverg, L.; Lopes, L.C.P. Association between perinatal and obstetric factors and early age at diagnosis of type 1 diabetes mellitus: A cohort study. J. Pediatr. Endocrinol. Metab. 2024, 37, 673–679. [Google Scholar] [CrossRef]
- Azeem, S.; Khan, U.; Liaquat, A. The increasing rate of diabetes in Pakistan: A silent killer. Ann. Med. Surg. 2022, 79, 103901. [Google Scholar] [CrossRef] [PubMed]
- Internet. Available online: https://diabetesatlas.org/data/en/region/7/sea.html (accessed on 23 October 2024).
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; IDF Diabetes Atlas: Brussels, Belgium, 2021; Available online: https://www.diabetesatlas.org (accessed on 15 January 2025).
- Basit, A.; Mustafa, N.; Waris, N.; Askari, S.; Fawwad, A.; NDSP members. Predicting the risk of type 2 diabetes through anthropometric indices in Pakistani adults- A sub-analysis of second National diabetes survey of Pakistan 2016–2017 (NDSP-07). Diabetes Metab. Syndr. 2021, 15, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Condie, A.M.; Allen, T.V.; Ogle, G.D. Incidence and characteristics of childhood- and youth-onset diabetes in the Qalandarabad area in northern Pakistan. Diabetes Res. Clin. Pract. 2020, 163, 108155. [Google Scholar] [CrossRef]
- Greenwood, S.; Newland-Jones, P.; Hicks, D.; Yousef, Z.; Moore, J.; Kelly, B.; Davies, S.; Dashora, U. Risk Prediction of the Diabetes Missing Million: Identifying Individuals at High Risk of Diabetes and Related Complications. Diabetes Ther. 2021, 12, 87–105. [Google Scholar] [CrossRef]
- Cao, L.; Zhou, J.; Chen, Y.; Wu, Y.; Wang, Y.; Liu, T.; Fu, C. Effects of Body Mass Index, Waist Circumference, Waist-to-Height Ratio and Their Changes on Risks of Dyslipidemia among Chinese Adults: The Guizhou Population Health Cohort Study. Int. J. Environ. Res. Public Health 2021, 19, 341. [Google Scholar] [CrossRef]
- World Health Organization. BMI-for-Age (5–19 Years). Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/bmi-for-age (accessed on 15 January 2025).
- Alzahrani, N.; Alouffi, S.; Almutairi, K.; Almutairi, M.; Almutairi, T.; Alwan, I.A.; Otaibi, N.; Tamimi, W. Can Fasting Blood Sugar be Used as an Indicator of Long-Term Diabetic Control Instead of Estimated Average Glucose? Clin. Lab. 2020, 66. [Google Scholar] [CrossRef]
- Dildar, S.; Imran, S.; Naz, F. Method comparison of Particle Enhanced Immunoturbidimetry (PEIT) with High Performance Liquid Chromatography (HPLC) for glycated hemoglobin (HbA1c) analysis. Clin. Diabetes Endocrinol. 2021, 7, 10. [Google Scholar] [CrossRef]
- Weir, C.B.; Jan, A. BMI Classification Percentile and Cut Off Points. [Updated 26 June 2023]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (accessed on 19 January 2025).
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 6. Glycemic Goals and Hypoglycemia: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47 (Suppl. S1), S111–S125. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. Available online: https://www.who.int/initiatives/behealthy/physical-activity (accessed on 31 January 2025).
- World Health Organization. Increasing Fruit and Vegetable Consumption to Reduce the Risk of Noncommunicable Diseases. Last Updated: 9 August 2023. Available online: https://www.who.int/tools/elena/interventions/fruit-vegetables-ncds (accessed on 31 January 2025).
- Basit, A.; Fawwad, A.; Qureshi, H.; Shera, A.S.; NDSP Members. Prevalence of diabetes, pre-diabetes and associated risk factors: Second National Diabetes Survey of Pakistan (NDSP), 2016–2017. BMJ Open 2018, 8, e020961, Erratum in BMJ Open 2019, 8, e020961corr1. https://doi.org/10.1136/bmjopen-2017-020961corr1. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Lawrence, J.M.; Dabelea, D.; Divers, J.; Isom, S.; Dolan, L.; Imperatore, G.; Linder, B.; Marcovina, S.; Pettitt, D.J.; et al. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002–2012. N. Engl. J. Med. 2017, 376, 1419–1429. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Moran, M.; Guerrero-Romero, F.; Aradillas-García, C.; Violante, R.; Simental-Mendia, L.E.; Monreal-Escalante, E.; Mendoza Ede, L. Obesity and family history of diabetes as risk factors of impaired fasting glucose: Implications for the early detection of prediabetes. Pediatr. Diabetes 2010, 11, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.O.; Dashti, H.S.; Lane, J.M.; Windred, D.P.; Burns, A.; Jones, S.E.; Sofer, T.; Purcell, S.M.; Zhu, X.; Ollila, H.M.; et al. Causal Association Between Subtypes of Excessive Daytime Sleepiness and Risk of Cardiovascular Diseases. J. Am. Heart Assoc. 2023, 12, e030568. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Yeung, S.L.A.; Sharp, S.J.; Wang, M.; Jang, H.; Luo, S.; Brage, S.; Wijndaele, K. Genetic susceptibility, screen-based sedentary activities and incidence of coronary heart disease. BMC Med. 2022, 20, 188. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).