
Effect of Rehabilitation Nutrition on a Post-Acute Severe COVID-19 Patient: A Case Report

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Information
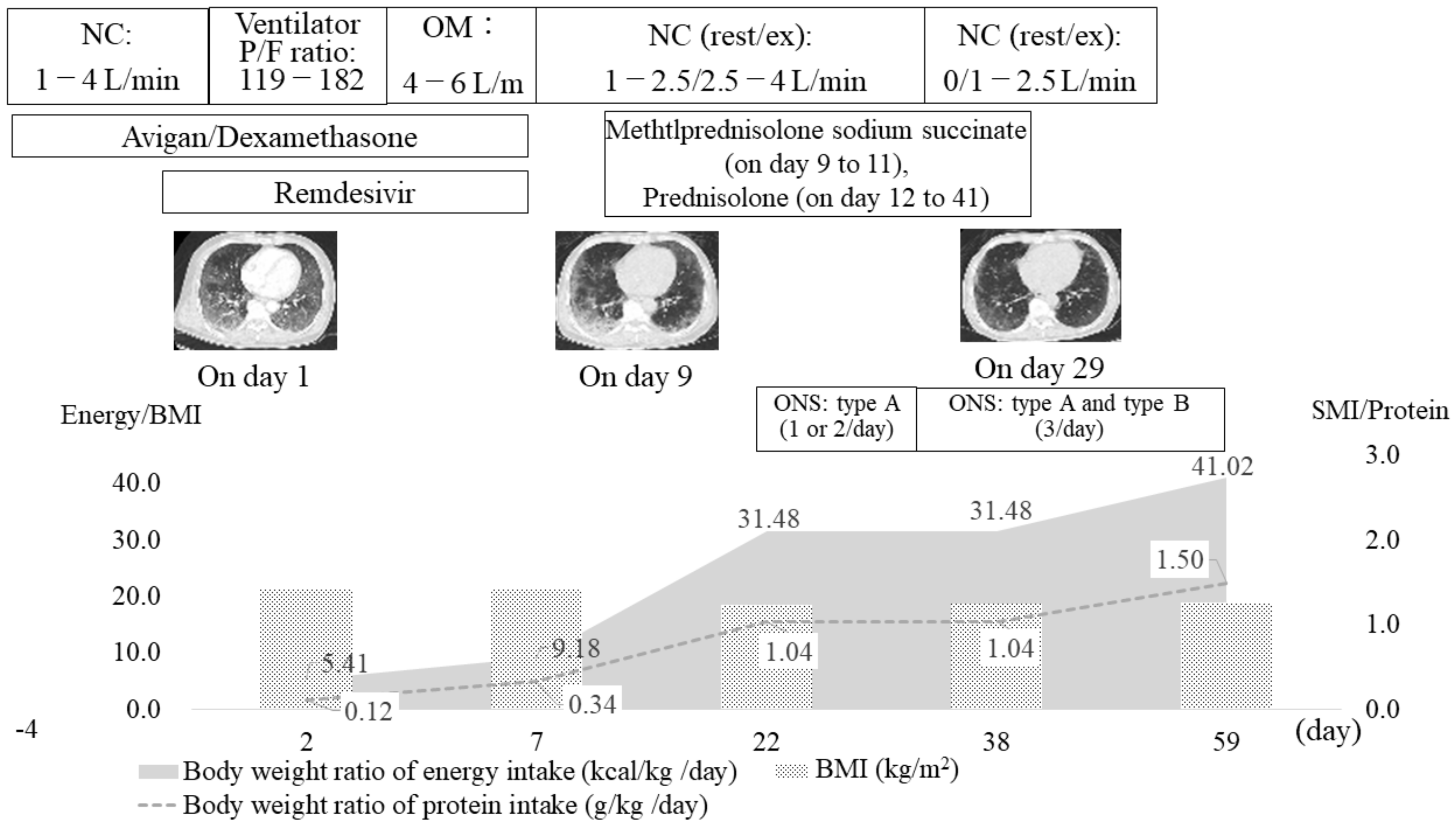
2.2. Course of Treatment
2.3. Rehabilitation Nutrition Assessment, Diagnostic Reasoning, and Diagnosis
2.4. Rehabilitation Nutrition Goal Setting, Intervention, and Monitoring
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Thomas, P.; Baldwin, C.; Bissett, B.; Boden, I.; Gosselink, R.; Granger, C.L.; Hodgson, C.; Jones, A.Y.; Kho, M.E.; Moses, R.; et al. Physiotherapy management for COVID-19 in the acute hospital setting: Clinical practice recommendations. J. Physiother. 2020, 66, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Ceravolo, M.G.; Arienti, C.; de Sire, A.; Andrenelli, E.; Negrini, F.; Lazzarini, S.G.; Patrini, M.; Negrini, S. Rehabilitation and COVID-19: The Cochrane Rehabilitation 2020 rapid living systematic review. Eur. J. Phys. Rehabil. Med. 2020, 56, 642–651. [Google Scholar] [CrossRef] [PubMed]
- Paneroni, M.; Simonelli, C.; Saleri, M.; Bertacchini, L.; Venturelli, M.; Troosters, T.; Ambrosino, N.; Vitacca, M. Muscle Strength and physical performance in patients without previous disabilities recovering from COVID-19 pneumonia. Am. J. Phys. Med. Rehabil. 2021, 100, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Dal Negro, F.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef] [PubMed]
- Udina, C.; Ars, J.; Morandi, A.; Vilaró, J.; Cáceres, C.; Inzitari, M. Rehabilitation in adult post-COVID-19 patients in post-acute care with therapeutic exercise. J. Frailty. Aging 2021, 10, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Krznaric, Z.; Nitzan, D.; Pirlich, M.; Singer, P. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection. Clin. Nutr. 2020, 39, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Hegerová, P.; Dědková, Z.; Sobotka, L. Early nutritional support and physiotherapy improved long-term self-sufficiency in acutely ill older patients. Nutrition 2015, 31, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H. Rehabilitation nutrition in general and family medicine. J. Gen. Fam. Med. 2017, 18, 153–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.D.; Marshall, S.A.; Cornblath, D.R.; Hoke, A.; Needham, D.M.; de Jonghe, B.; Ali, N.A.; Sharshar, T. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit. Care Med. 2009, 37, S299–S308. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.M.; Elmes, P.C.; Fairbairn, A.S.; Wood, C.H. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. Br. Med. J. 1959, 2, 257–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life. Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muza, S.R.; Silverman, M.T.; Gilmore, G.C.; Hellerstein, H.K.; Kelsen, S.G. Comparison of scales used to quantitate the sense of effort to breathe in patients with chronic obstructive pulmonary disease. Am. Rev. Respir. Dis. 1990, 141, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Tohara, H.; Saitoh, E.; Mays, K.A.; Kuhlemeier, K.; Palmer, J.B. Three tests for predicting aspiration without videofluorography. Dysphagia 2003, 18, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Brugliera, L.; Spina, A.; Castellazzi, P.; Cimino, P.; Arcuri, P.; Negro, A.; Houdayer, E.; Alemanno, F.; Giordani, A.; Mortini, P.; et al. Nutritional management of COVID-19 patients in a rehabilitation unit. Eur. J. Clin. Nutr. 2020, 74, 860–863. [Google Scholar] [CrossRef] [PubMed]
- Rooney, S.; Webster, A.; Paul, L. Systematic review of changes and recovery in physical function and fitness after severe acute respiratory syndrome-related coronavirus infection: Implications for COVID-19 rehabilitation. Phys. Ther. 2020, 100, 1717–1729. [Google Scholar] [CrossRef] [PubMed]
- Shirado, K.; Wakabayashi, H.; Maeda, K.; Nishiyama, A.; Asada, M.; Isse, H.; Saito, S.; Kakitani, C.; Momosaki, R. Impact of Energy intake at one week after hospitalization on prognosis for older adults with pneumonia. J. Nutr. Health Aging 2020, 24, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Number of Days of Hospitalization | 2 | 7 | 22 | 38 | 59 | Variation Rate |
|---|---|---|---|---|---|---|
| (Day 22–59) | ||||||
| Body weight (kg) | 61.4 | 60.6 | 53.2 | 53.4 | 54.2 | 1.88% |
| BMI (kg/m2) | 21.5 | 21.2 | 18.6 | 18.7 | 19 | 2.15% |
| SMI (kg/m2) | NC | NC | 5.6 | 5.8 | 6.1 | 8.93% |
| Body fat (kg) | NC | NC | 12.9 | 12.1 | 12.7 | −1.55% |
| ECW/TBW | NC | NC | 0.392 | 0.393 | 0.399 | 1.79% |
| ICU MRC score (point) | NC | 40 | 46 | 48 | 60 | 30.43% |
| Grip strength, Rt (kg) | NC | NC | 21.5 | NC | 30.7 | 42.79% |
| Grip strength, Lt (kg) | NC | NC | 22.3 | NC | 27.7 | 24.22% |
| Gait speed (m/s) | NC | NC | 1.12 | NC | 1.20 | 6.59% |
| FIM, motor items (points) | 13 | 22 | 43 | 78 | 88 | |
| FIM, cognitive items (points) | 12 | 35 | 12 | 35 | 35 | |
| mMRC dyspnea scale | NC | 4 | 4 | 2 | 0 | |
| EQ-5D-5L | NC | NC | 0.35 | NC | 0.842 | |
| eGFR | 69.33 | 61.39 | 74.09 | 83.14 | 89.95 | |
| CRP (mg/dL) | 6.81 | 1.7 | 0.02 | 1.33 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirado, K.; Furuno, Y.; Kanamaru, K.; Kawabata, N.; Okuno, S.; Yamashita, T. Effect of Rehabilitation Nutrition on a Post-Acute Severe COVID-19 Patient: A Case Report. Healthcare 2021, 9, 1034. https://doi.org/10.3390/healthcare9081034
Shirado K, Furuno Y, Kanamaru K, Kawabata N, Okuno S, Yamashita T. Effect of Rehabilitation Nutrition on a Post-Acute Severe COVID-19 Patient: A Case Report. Healthcare. 2021; 9(8):1034. https://doi.org/10.3390/healthcare9081034
Chicago/Turabian StyleShirado, Kengo, Yuji Furuno, Kozue Kanamaru, Naoto Kawabata, Shota Okuno, and Toshihiro Yamashita. 2021. "Effect of Rehabilitation Nutrition on a Post-Acute Severe COVID-19 Patient: A Case Report" Healthcare 9, no. 8: 1034. https://doi.org/10.3390/healthcare9081034
APA StyleShirado, K., Furuno, Y., Kanamaru, K., Kawabata, N., Okuno, S., & Yamashita, T. (2021). Effect of Rehabilitation Nutrition on a Post-Acute Severe COVID-19 Patient: A Case Report. Healthcare, 9(8), 1034. https://doi.org/10.3390/healthcare9081034