Changes in Physical Function and Effects on QOL in Patients after Pancreatic Cancer Surgery

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Methods
2.2. Rehabilitation Program
2.3. Body Composition
2.4. Physical Function
2.5. Gait Assessments
2.6. Quality of Life
2.7. Statistical Analysis
3. Results
3.1. Socio-Demographic and Clinical Characteristics
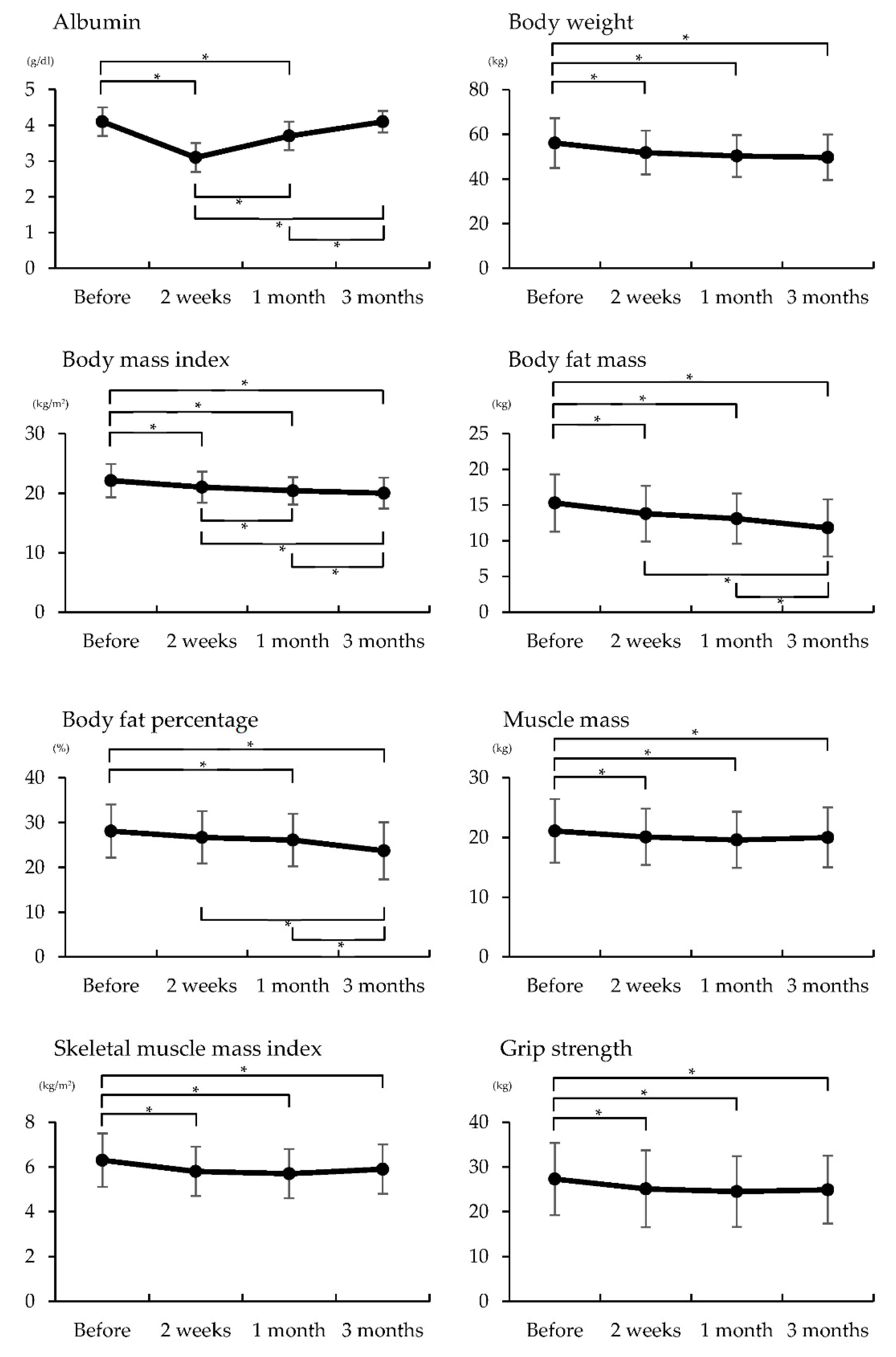
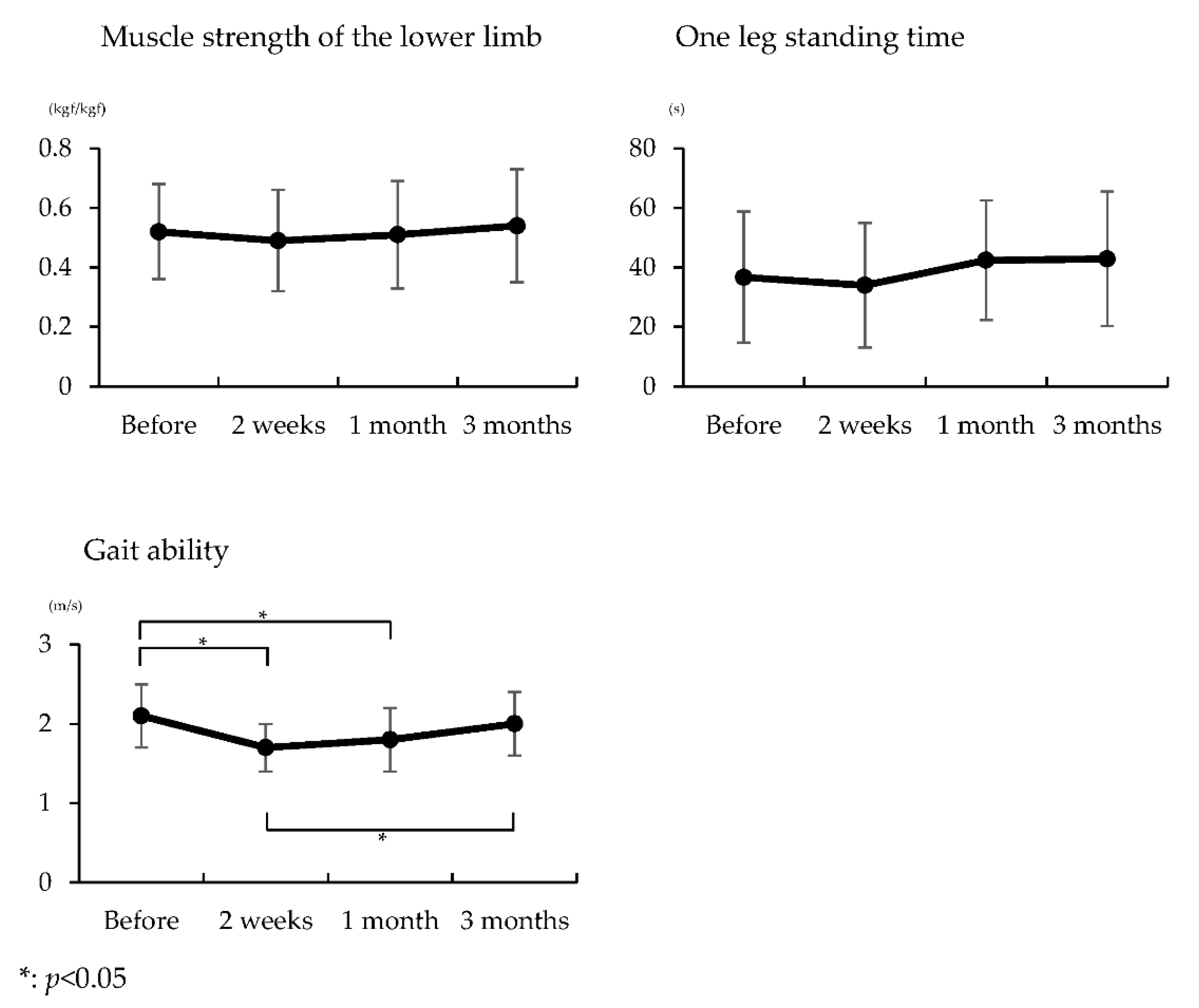
3.2. Differences in Nutritional Status, Body Composition, Physical Function, and Gait Assessment before, Two Weeks, One Month, and Three Months after Surgery
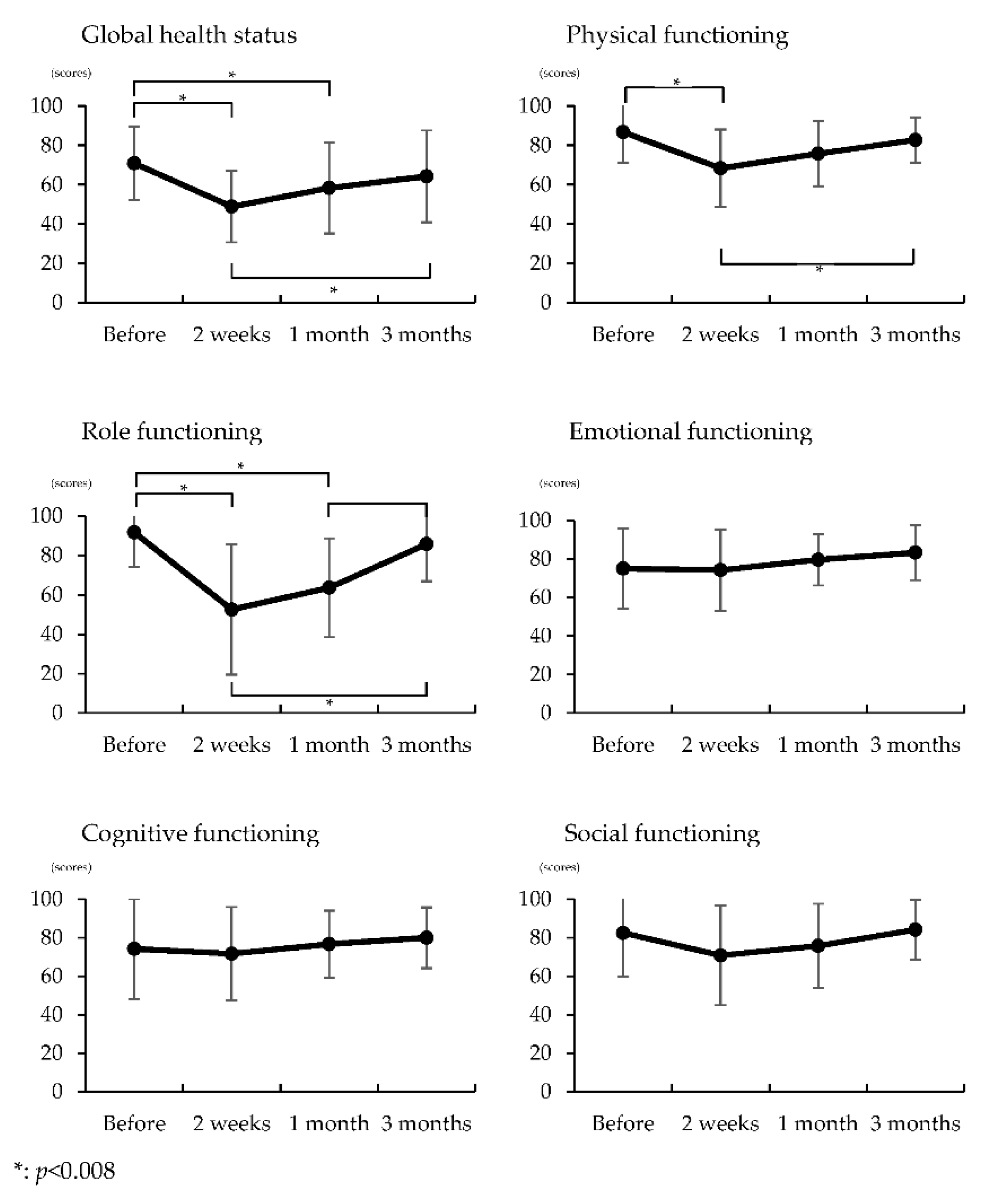
3.3. Differences in Quality of Life Scores before, Two Weeks, One Month, and Three Months after Surgery
3.4. Factors Predicting Quality of Life at Three Months after Surgery
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saad, A.M.; Turk, T.; Al-Husseini, M.J.; Abdel-Rahman, O. Trends in pancreatic adenocarcinoma incidence and mortality in the United States in the last four decades; a SEER-based study. BMC Cancer 2018, 18, 688. [Google Scholar] [CrossRef] [PubMed]
- Okumura, S.; Kaido, T.; Hamaguchi, Y.; Fujimoto, Y.; Masui, T.; Mizumoto, M.; Hammad, A.; Mori, A.; Takaori, K.; Uemoto, S. Impact of preoperative quality as well as quantity of skeletal muscle on survival after resection of pancreatic cancer. Surgery 2015, 157, 1088–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clauss, D.; Tjaden, C.; Hackert, T.; Schneider, L.; Ulrich, C.M.; Wiskemann, J.; Steindorf, K. Cardiorespiratory fitness and muscle strength in pancreatic cancer patients. Support. Care Cancer 2017, 25, 2797–2807. [Google Scholar] [CrossRef]
- Bachmann, J.; Heiligensetzer, M.; Krakowski-Roosen, H.; Büchler, M.W.; Friess, H.; Martignoni, M.E. Cachexia worsens prognosis in patients with resectable pancreatic cancer. J. Gastrointest. Surg. 2008, 12, 1193–1201. [Google Scholar] [CrossRef]
- Dewys, W.D.; Begg, C.; Lavin, P.T.; Band, P.R.; Bennett, J.M.; Bertino, J.R.; Cohen, M.H.; Douglass, H.O., Jr.; Engstrom, P.F.; Ezdinli, E.Z.; et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Am. J. Med. 1980, 69, 491–497. [Google Scholar] [CrossRef]
- Sun, V.; Ruel, N.; Chung, V.; Singh, G.; Leong, L.; Fakih, M.; Fong, Y.; Ferrell, B. Pilot study of an interdisciplinary supportive care planning intervention in pancreatic cancer. Support. Care Cancer 2016, 24, 3417–3424. [Google Scholar] [CrossRef] [Green Version]
- Cormie, P.; Spry, N.; Jasas, K.; Johansson, M.; Yusoff, I.F.; Newton, R.U.; Galvão, D.A. Exercise as medicine in the management of pancreatic cancer: A case study. Med. Sci. Sports Exerc. 2014, 46, 664–670. [Google Scholar] [CrossRef]
- Tatematsu, N.; Hasegawa, S.; Tanaka, E.; Sakai, Y.; Tsuboyama, T. Impact of oesophagectomy on physical fitness and health-related quality of life in patients with oesophageal cancer. Eur. J. Cancer Care 2013, 22, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, S.; Osugi, H.; Higashino, M.; Tokuhara, T.; Takada, N.; Takemura, M.; Lee, S.; Kinoshita, H. Comparison of three-field esophagectomy for esophageal cancer incorporating open or thoracoscopic thoracotomy. Surg. Endosc. 2003, 17, 1445–1450. [Google Scholar] [CrossRef]
- Sullivan, P.A.; Still, C.D.; Jamieson, S.T.; Dixon, C.B.; Irving, B.A.; Andreacci, J.L. Evaluation of multi-frequency bioelectrical impedance analysis for the assessment of body composition in individuals with obesity. Obes. Sci. Pract. 2018, 5, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Owashi, K.; Kanauchi, Y.; Mura, N.; Takahara, M.; Ogino, T. The short-term reliability of grip strength measurement and the effects of posture and grip span. J. Hand Surg. Am. 2005, 30, 603–609. [Google Scholar] [CrossRef]
- Hirano, M.; Katoh, M.; Gomi, M.; Arai, S. Validity and reliability of isometric knee extension muscle strength measurements using a belt-stabilized hand-held dynamometer: A comparison with the measurement using an isokinetic dynamometer in a sitting posture. J. Phys. Ther. Sci. 2020, 32, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Kita, K.; Hujino, K.; Nasu, T.; Kawahara, K.; Sunami, Y. A simple protocol for preventing falls and fractures in elderly individuals with musculoskeletal disease. Osteoporos. Int. 2007, 18, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Van de Port, I.G.; Kwakkel, G.; Lindeman, E. Community ambulation in patients with chronic stroke: How is it related to gait speed? J. Rehabil. Med. 2008, 40, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Wiskemann, J.; Clauss, D.; Tjaden, C.; Hackert, T.; Schneider, L.; Ulrich, C.M.; Steindorf, K. Progressive resistance training to impact physical fitness and body weight in pancreatic cancer patients: A randomized controlled trial. Pancreas 2019, 48, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Yeo, T.P.; Burrell, S.A.; Sauter, P.K.; Kennedy, E.P.; Lavu, H.; Leiby, B.E.; Yeo, C.J. A progressive postresection walking program significantly improves fatigue and health-related quality of life in pancreas and periampullary cancer patients. J. Am. Coll. Surg. 2012, 214, 463–475. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moses, A.W.G.; Slater, C.; Preston, T.; Barber, M.D.; Fearon, K.C.H. Reduced total energy expenditure and physical activity in cachectic patients with pancreatic cancer can be modulated by an energy and protein dense oral supplement enriched with n-3 fatty acids. Br. J. Cancer 2004, 90, 996–1002. [Google Scholar] [CrossRef]
- Hendifar, A.E.; Chang, J.I.; Huang, B.Z.; Tuli, R.; Wu, B.U. Cachexia, and not obesity, prior to pancreatic cancer diagnosis worsens survival and is negated by chemotherapy. J. Gastrointest. Oncol. 2018, 9, 17–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, A.A.; Gonen, M.; Karanicolas, P.; Jarnagin, W.R.; D’Angelica, M.I.; DeMatteo, R.; Kingham, T.P.; Allen, P.J. Health-Related Quality of Life After Pancreatectomy: Results from a Randomized Controlled Trial. Ann. Surg. Oncol. 2016, 23, 2137–2145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schniewind, B.; Bestmann, B.; Henne-Bruns, D.; Faendrich, F.; Kremer, B.; Kuechler, T. Quality of life after pancreaticoduodenectomy for ductal adenocarcinoma of the pancreatic head. Br. J. Surg. 2006, 93, 1099–1107. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Parameters | |
|---|---|
| Sex (male/female) a | 8/12 |
| Age (y) b | 69.8 ± 7.4 |
| Height (cm) b | 156.8 ± 9.0 |
| Comorbidities a | |
| Bronchial asthma | 1 |
| Interstitial pneumonia | 1 |
| Diabetes mellitus | 3 |
| Hypertension | 1 |
| Knee Osteoarthritis | 1 |
| Item | Included Variable † | B | Standard. Error | β | t | R | Adjusted R2 | p Value |
|---|---|---|---|---|---|---|---|---|
| GHS | Grip strength three months after surgery | 1.834 | 0.579 | 0.598 | 3.166 | 0.598 | 0.322 | p < 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurokawa, H.; Akezaki, Y.; Tominaga, R.; Okamoto, M.; Kikuuchi, M.; Hamada, M.; Mikuriya, Y.; Ohta, K.; Sugihara, S. Changes in Physical Function and Effects on QOL in Patients after Pancreatic Cancer Surgery. Healthcare 2021, 9, 882. https://doi.org/10.3390/healthcare9070882
Kurokawa H, Akezaki Y, Tominaga R, Okamoto M, Kikuuchi M, Hamada M, Mikuriya Y, Ohta K, Sugihara S. Changes in Physical Function and Effects on QOL in Patients after Pancreatic Cancer Surgery. Healthcare. 2021; 9(7):882. https://doi.org/10.3390/healthcare9070882
Chicago/Turabian StyleKurokawa, Hideaki, Yoshiteru Akezaki, Ritsuko Tominaga, Masaki Okamoto, Masato Kikuuchi, Makiko Hamada, Yoshihiro Mikuriya, Koji Ohta, and Shinsuke Sugihara. 2021. "Changes in Physical Function and Effects on QOL in Patients after Pancreatic Cancer Surgery" Healthcare 9, no. 7: 882. https://doi.org/10.3390/healthcare9070882
APA StyleKurokawa, H., Akezaki, Y., Tominaga, R., Okamoto, M., Kikuuchi, M., Hamada, M., Mikuriya, Y., Ohta, K., & Sugihara, S. (2021). Changes in Physical Function and Effects on QOL in Patients after Pancreatic Cancer Surgery. Healthcare, 9(7), 882. https://doi.org/10.3390/healthcare9070882