1. Introduction
The world is currently facing a serious aging trend, and the speed of aging is rapidly accelerating. For example, it took 150 years for the population over 60 years old in France to go from 10% to 20%. However, it took only around 20 years for countries such as Brazil, China, and India to reach the same level [
1]. The “2019 Revision of World Population Prospects” launched by the United Nations pointed out that the world is facing three major trends: a decrease in the new population, a rapid increase in the elderly population, and a decline in population in many countries [
2]. According to data from the World Health Organization, in the period from 2015 to 2050, the proportion of the world’s population over 60 will be almost double, from 12% to 22%. The aging population structure has become a major challenge for the entire world. In 2016, the World Health Organization and its members formulated the Global Aging and Health Strategy and Action Plan in the World Health Assembly (Document A69/17) [
3]. In addition to focusing on healthy aging, providing a good supportive environment so that the elderly can walk easily is also one of the key points of continuous promotion, which include providing a barrier-free environment or the use of assistive devices. At the same time, the elderly can perform regular exercises to improve their physical and mental functions. It can help the elderly to delay aging [
1].
According to the report, “Taiwan Population Estimates (2018–2065)” [
4], released by the National Development Council, Taiwan is currently facing three major trends. First, the total population will turn to negative growth in 3–10 years. Second, if the total fertility rate remains the same, the number of births in 2065 will be halved. Third, Taiwan will become an overaged society in the next eight years. The rate of aging has surpassed developed countries such as European nations, America, and Japan. Moreover, once the number of births in the future decreases and the average age of the population increases, this means that the dependency ratio will continue to increase. In addition to major changes in the demographic structure, the social burden will also increase. Moreover, the report pointed out that in the future, the proportion of people over 65 in the total population will rise from 14.5% in 2018 to 41.2% in 2065. This means that four out of 10 people will be elderly [
5]. Therefore, in order to deal with the aging social structure, Taiwan is currently actively improving the friendly environment for the elderly, including elderly-friendly workplaces, long-term care programs, and the economic security of the elderly.
The National Health Interview Survey, conducted by Taiwan’s National Health Administration [
6], interviewed 3280 elderly people in 2017. It stated that one out of six elderly people fell in the past year (495 people, 15.5%). As the physical functions of the elderly, including muscle strength and balance ability, etc., decline, they are gradually going downhill. Moreover, the survey also mentioned that the most common places to fall at home are the bedroom, living room, and bathroom. Among the top 10 causes of death among the elderly in Taiwan in 2019, accidents ranked sixth [
7], even higher than kidney disease or high blood pressure. In addition to deaths in traffic accidents, the most common accidents are caused by falls.
Because of the deterioration of the body, many abilities of the elderly are not as good as when they were young, including vision, hearing, balance, reaction time, muscle strength, or endurance. Yang et al. conducted a study on elderly people with mild to moderate difficulties living in institutions [
8]. The survey found that the functions affected by the activities of daily living (ADLs) of these elderly people included climbing stairs (62.9%), bathing (47.2%), and walking (40.4%). At the same time, it was also found that functional movements such as knee extension muscle strength, 3-m timed up and go, 30-s sitting and standing, and 2-min stance stepping were worse than in other normal elderly people.
Therefore, with age the performance of the elderly in ADLs is most often affected by the ability to walk. Suwannarat et al. conducted interviews and surveys on 343 elderly people over 65 years old in rural Thailand in 2015 [
9]. The types of walking aids used by these elderly people and their mobile functions were discussed. The elders who participated in the survey had a significant correlation with the need for walking aids, especially the elderly over 75. The ability of daily living can be obviously improved through walking aids.
Some studies have mentioned that the elderly encounter several major obstacles when using assistive technologies, including privacy violations, insufficient trust in technical assistance tools, lack of value-added features, consideration of purchase costs, and lack of training or embarrassment [
10]. Related researches tend to focus on high-tech assistive technologies, and rarely mention low-tech walking aids such as canes or walkers. On the topic of preventing the elderly from falling, researchers found out that many elderly people do not want to be associated with health problems. They think that the problem is “not for me” or they are afraid to feel stigmatized after using assistive devices [
11]. The elderly do not want to use assistive devices because of their worry about dependence [
12].
Simpson and Richardson [
13] suggested that when a patient needs to use walking aids, medical staff should actively check the walking aids used by the patient and his or her health promotion needs. At the same time, the elderly are encouraged to seek professional advice before using walking aids. However, it can be observed in Taiwan that there are still many elders who have difficulty in moving and are reluctant to use walking aids such as canes or walkers, whether or not they need disability care services or are provided assistive device purchase subsidies. They are concerned about their social image and are afraid of being laughed at by others or being labeled as “disabled.” They would rather struggle to walk or use umbrellas to assist themselves in walking. There is still a lack of relevant empirical research on the phenomenon of elderly people resisting the use of walking aids from the perspective of social image.
In 2014, the Technology Acceptance Model (TAM) was used to study the technology acceptance of the elderly in Hong Kong [
14]. The results of the study pointed out that because Chinese people are more introverted and afraid of being laughed at for poor performance, it is easy to influence the intention of the elderly to use technology. In addition, Tural, Lu, and Cole [
15] also discussed the attitudes and intentions of elderly people who use staircase-assisted design at home. Among them, if the appearance or aesthetics of the related equipment is well-designed, the elderly will still regard it as a continuous stigma of disability due to the association of negative images. For example, poor social acceptance or loss of independence [
16] will affect their willingness to use related equipment. It can be seen that the elderly want to look like ordinary elderly people but do not want to be regarded as dependent or disabled, which will affect their behavioral intentions and attitudes when using assistive devices.
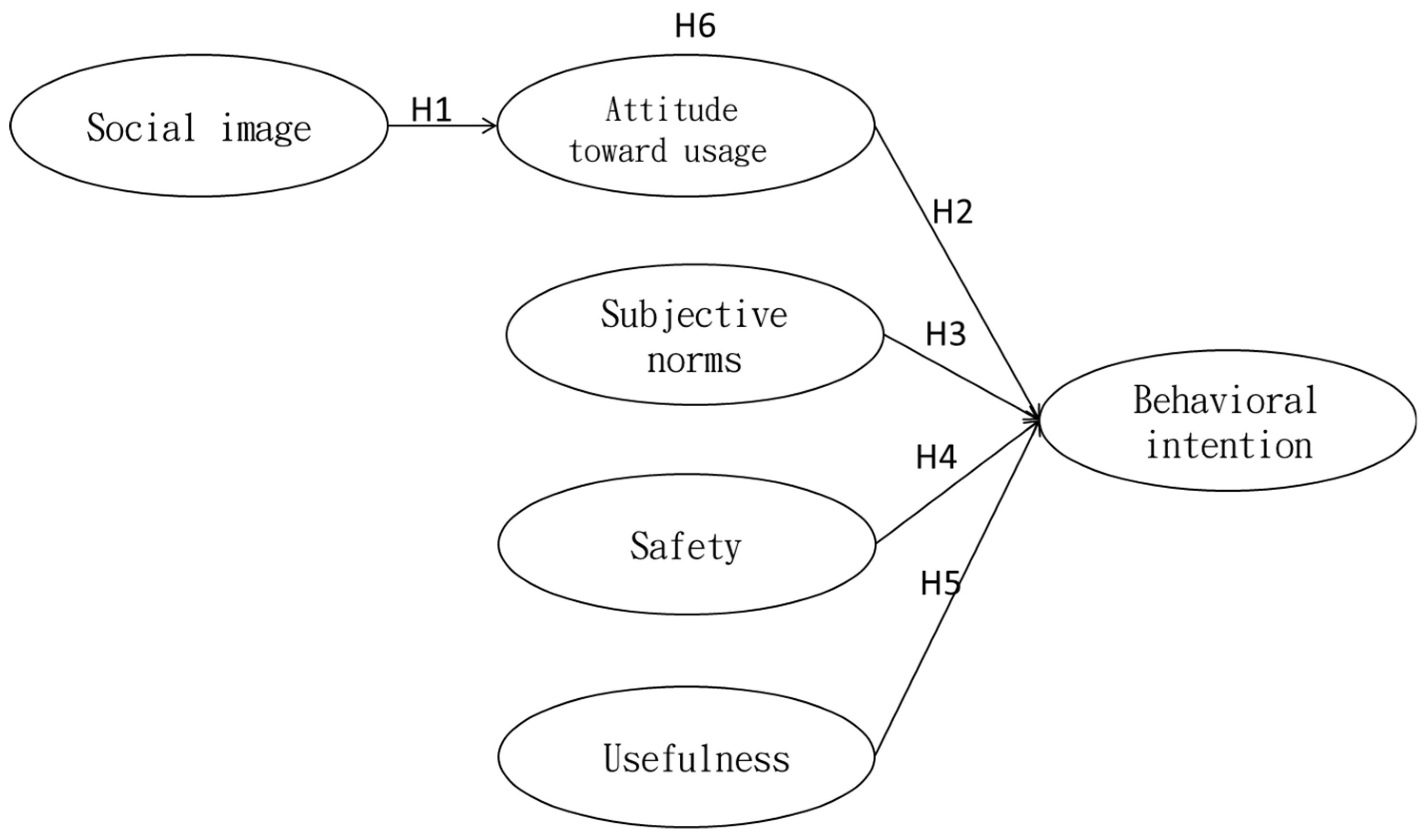
Therefore, this research will focus on the factors that influence the behavior of middle-aged (45–64 years old) and elderly (65 years and older) people toward using walking aids in Taiwan. The subjects of the study were not people with severe walking disabilities, but people with mild walking disabilities or those who needed walking supporters because of old age. As Asians live in a closely connected social environment, middle-aged and elderly people are more concerned with social image. Based on the rational behavior theory, the relationship between “social image”, “attitude toward usage”, “subjective norm”, “safety level”, “usefulness”, and “behavior intention” will be verified by a survey investigation. According to the results of this study, it can provide a reference for government agencies and private manufactories to promote walking aids for middle-aged and elderly people.
5. Discussion
This research was mainly to investigate the behavioral intention of middle-aged and elderly people to use walking aids and to explore its influencing factors. Based on the Theory of Reasoned Action (TRA), combined with the social image and attitude toward usage as mediating variables, the research framework and related hypotheses were proposed. After collecting data through a questionnaire survey, the structural equation model was used to test the model and verify related hypotheses. Based on the Theory of Reasoned Action (TRA), this research attempted to explore the factors affecting the behavior of middle-aged and elderly users from the perspective of social image. Therefore, integrating factors such as safety, usefulness, and social image dimensions were used to discuss the influence on middle-aged and elderly people’s intention to use walking aids. The research results are as follows.
5.1. The Influence of Social Image on the Attitude toward Using Walking Aids
The results of the study showed that social image has a significant positive impact on attitudes toward using walking aids. This result was consistent with the previous research [
43]. The average score of social image measurement was 4.876, which was the lowest score of all constructs. It could be that the middle-aged and elderly people think that the use of walking aids cannot be socially recognized. They are obviously worried about the external image of using a walker, so they have reservations about using a walker, and even have a sense of resistance. At the same time, the standard deviation of the social image item “I use walking aids to make a good impression” was greater than 1.3, indicating that users’ opinions varied greatly. Moreover, the item “I can get the envy of my friends by using advanced walking aids” had the lowest mean score, 4.57, and the highest standard deviation, 1.5. The low score may show that on the issue of the use of walking aids, the users thought that even choosing high-end-style walking aids would not necessarily reverse the social image. Therefore, they could not gain support and recognition for using walking aids. At the same time, the high standard deviation may indicate that users had greatly inconsistent opinions, and it also may show that the public has unequal attitudes and opinions toward people who use walking aids.
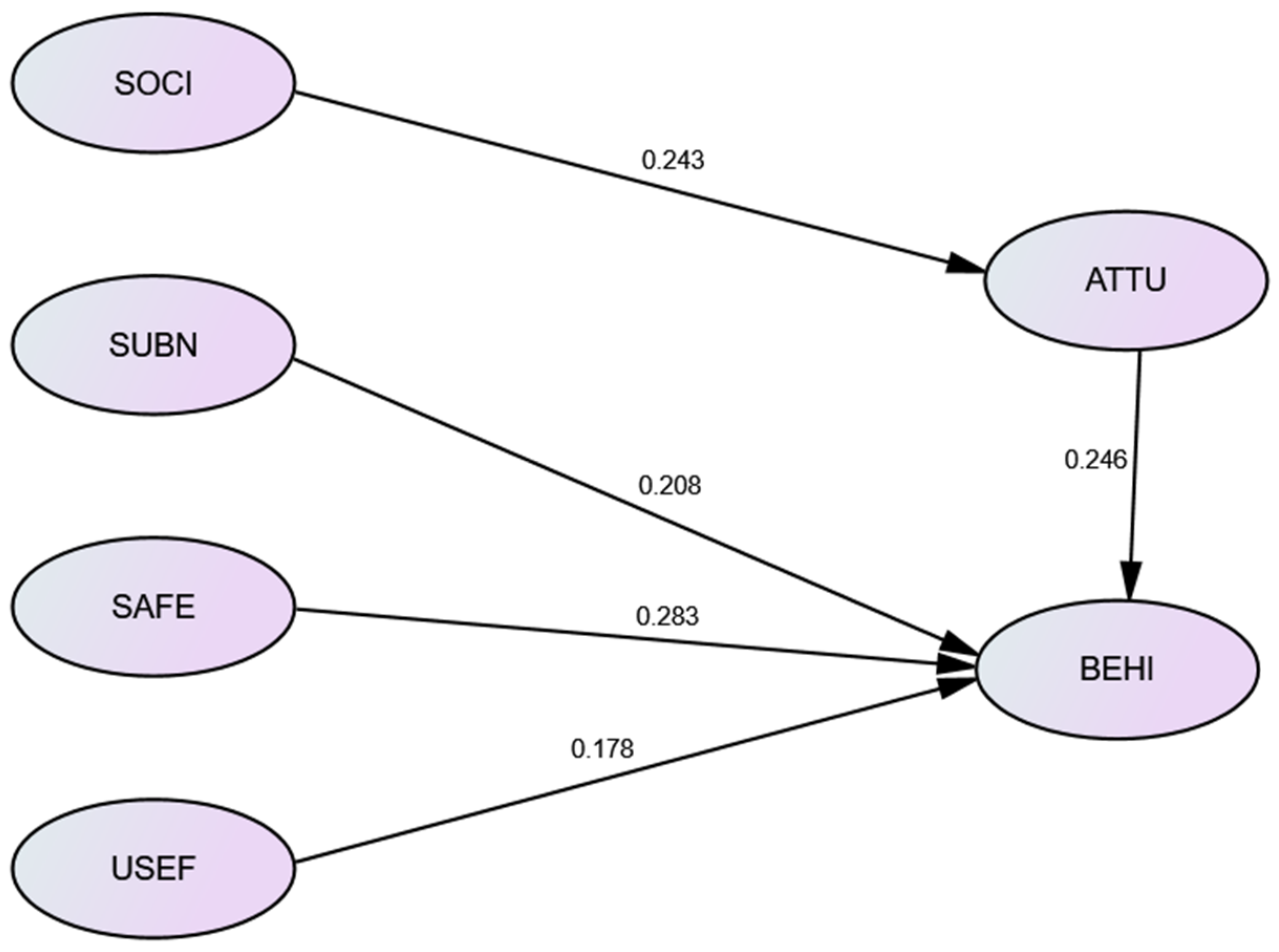
In the path analysis of the influence of social image on use attitude, the non-standardized regression coefficient reached 0.243, indicating that social image factors had a high proportion of influence on use attitude. It also confirms the hypothesis of this study that social image has a significant influence on the attitude toward using walking aids. Therefore, it is also proved that middle-aged and elderly users are obviously concerned about the social impression of disability, aging, and the dependence caused by the use of walking aids. This differs from ordinary people, so it affects their attitude toward using mobility aids. At the same time, if they were to choose a more advanced walker, whether it was for a change in function or appearance, it would not enhance the attitude toward using a walker.
5.2. The Influence of Attitude and Subjective Norms on the Behavioral Intention of Walking Aids
The results of this study showed that the attitude toward using walking aids has a significant positive effect on behavioral intentions. This result was similar to the results of previous studies [
55]. In addition, subjective norms have a significant positive effect on the behavioral intention of using walking aids. This result was also consistent with the results of previous studies [
39,
84], and all fit into the framework of the TRA.
In the attitude toward usage construct, a positive view appeared, which meant that users agree that if their walking function was affected in the future, they would be open and willing to accept using walkers. The behavioral intention construct reached the highest average score of 6.324, indicating that if having difficulty walking in the future, the participants would use walking aids to assist walking, and even to convey positive messages or to recommend it to others. The subjective norm item “I will try to use it because the professional recommended the benefits of walking aids” gained the highest average score, 6.36, and its standard deviation value was 0.77. That means not only high agreement among the participants on this question, but also that as long as the use of walking aids is recommended by professionals, the user’s willingness to use it will be greatly increased.
5.3. The Impact of Safety and Usefulness on the Behavioral Intention of Using Walking Aids
The intensity of the perception of safety has a significant impact on the behavioral intention of using walking aids. This result was similar to the results of previous studies [
46,
47]. In addition, the usefulness of walking aids also has a significant positive impact on behavioral intentions. This result was also similar to the results of previous studies [
19,
85].
For users, the average score of the safety aspect was 5.838, which meant that they are less worried about the safety of walking aids. At the same time, in the safety construct, the non-standardized regression coefficient of behavioral intention reached 0.283. In addition to being an important influencing factor on the behavioral intention of using walking aids, it also meant that after users feel that safety is guaranteed, their willingness to use walking aids will increase significantly. In addition, the score of related items in usefulness also reached 6.01, and standard deviation was 0.85, indicating that users agree that walking aids are useful. However, since the regression coefficient was 0.178, the lowest of all factors, the degree it affected the behavioral intention of using walking aids was not so obvious.
5.4. Social Image Influences Behavioral Intention through Attitude toward Usage
Social image affects the attitude toward usage, and the attitude toward usage significantly positively affects the behavior intention, that is, the social image of using walking aids indirectly affects the behavioral intention. The attitude toward usage had a mediating effect, and this result was similar to the previous studies [
19,
42]. It can be seen that if middle-aged and elderly people are more concerned about their social image, it will affect their attitudes to using walking aids, which, in turn, will affect their behavioral intention to use walking aids.
6. Conclusions
The World Health Organization (WHO) proposed the Global Aging and Health Strategy and Action Plan in 2016 [
3], which mentioned that the physical and mental functions of the elderly are rapidly decreasing. The impact of the elderly on the whole of society is very important. If the elderly can maintain their functional capacity through their interaction with the environment, and be provided with adequate support for improving their health, then the life span of the elderly can be extended. The elderly can participate in society and improve their own health and well-being. Therefore, the use of assistive equipment and a barrier-free environment are the best supports for maintaining the functions of the elderly.
Taiwan began to implement National Ten-year Long-term Care Plan in 2008, providing assistive equipment and barrier-free environment improvement subsidies, including crutches, walking aids, or walkers. In 2018, the National Ten-year Long-term Care Plan 2.0 was promoted [
86], and the “Reablement” service was updated. Professional medical staff provide daily life function training, physical function training and maintenance, assistive devices use training, and other services. The goals of the program include improving the individual’s ability to live independently, achieving ability recovery, and increasing the ability to act independently.
As many elderly people get older, the function of their lower limbs deteriorates, which affects their walking function. However, they are afraid of being laughed at, their external image becoming morbid or weak. This may be why the middle-aged and elderly are reluctant to use walking aids. Instead, they will walk with umbrellas or bamboo poles, which is not only very laborious but also prone to danger. Therefore, it is very important to understand the influence of “social image” on users for the research on the use of walking aids by middle-aged and elderly people. In the past, research on assistive devices mostly focused on the design of the mechanics, functional aspects, and appearance of walking assistive devices. The behavior of assistive devices from the perspective of the user’s mentality and the relationship between related influencing variables were rarely studied.
Therefore, improving life functions through assistive devices is very important in an aging society. According to the present study, for these middle-aged or elderly people who are facing gradual degradation of functions, if the use of assistive devices cannot overcome the existing poor social image, no matter how sophisticated the assistive device is, it still cannot increase the willingness to use it. The group between the ages of 45–55, especially, was more concerned with social image than other elderly groups. It also becomes impossible to use assistive devices to achieve social participation, thereby delaying aging and increasing physical and mental health.
This study mainly sampled the middle-aged and elderly people in the urban area. The results of the study indicated that the sampled subjects had relatively high academic qualifications; a college degree or above accounted for 74.4%. However, the higher the level of education, the higher the ability to absorb information about assistive devices, and the higher the proportion of self-help ability in understanding the use of assistive devices. This study may not be able to fully present the attitudes and intentions of other people with lower academic qualifications. In addition, the majority of the subjects were under 65 years old (85%), and the elderly group sample (65 years old or above) was relatively small. Future research can improve in the sampling process. In addition, this research focuses on walking aids. In the future, research can focus on the intention of using other types of assistive devices, such as wheelchairs, hearing aids, or visual-impairment-related assistive devices, providing more about the use of various assistive devices.








{kind=link}
{kind=link}
{kind=link}
{kind=link}