Comparison of Spa Choice between Wellness Tourists and Healthcare/Medical Tourists



Abstract
1. Introduction
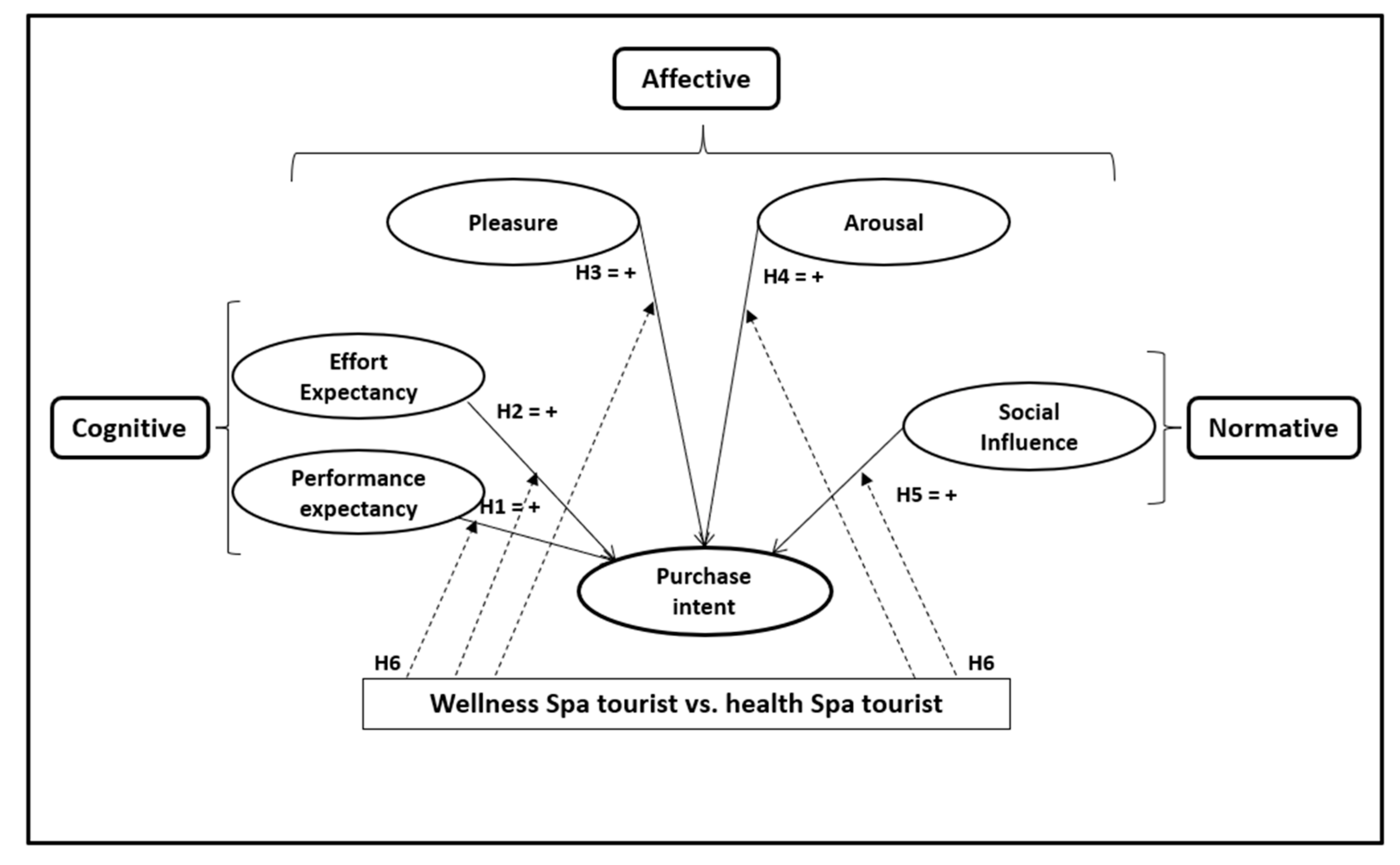
2. Hypothesis Development
2.1. The Influence of Performance Expectancy and Effort Expectancy on Spa Purchase Intention
2.2. Influence of Emotions on Spa Purchase Intention
2.3. Social Influence on Spa Purchase Intention
2.4. Moderating Influence of the Core Benefit Sought: Wellness Spa Tourism vs. Healthcare/Medical Spa Tourism
3. Methodology
3.1. Design
3.2. Measures
3.3. Statistical Analysis
- Step 1: Assessment of the measurement models. Two models were established: the first includes the influence of the CAN model variables on wellness tourists’ spa purchase intention; the second includes the influence of the CAN model variables on healthcare/medical tourists’ spa purchase intention. For the database for each model, the measurement model was assessed by testing the reliability and validity of the measurement scales. Given that for multigroup tests to be comparable, they must use the same model (configural invariance criterion), when an observable variable had to be eliminated, it was eliminated from both models.
- Step 2: Assessment of the structural model. For each of the two models, the R2, path coefficients, and their significance were estimated. For each model, the influence of the CAN model variables on spa purchase intention was tested.
- Step 3: Multigroup comparison of the models. The structure of the two models (wellness and healthcare/medical) was identical, making it possible to proceed to a multigroup comparison. The factorial invariance between the measurement models was verified [82]. For the multigroup comparison, the non-parametric PLS-MGA test proposed by Henseler et al. [82] was performed to determine whether the influence of the different CAN model dimensions on wellness and healthcare/medical tourists’ spa purchase intentions was different or similar.
4. Results
4.1. Assessment of the Measurement Models
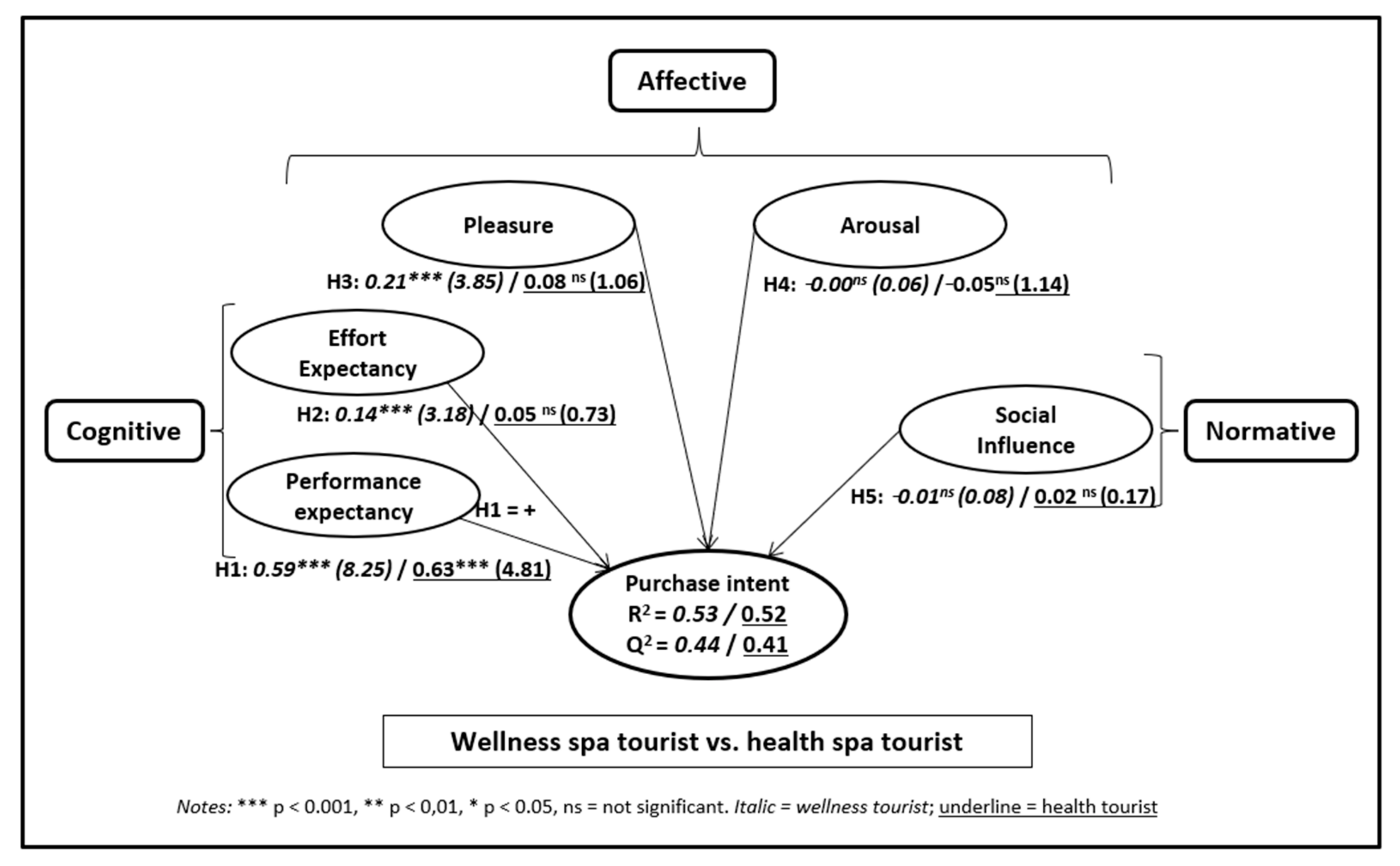
4.2. Assessment of the Structural Model
4.3. Multigroup Analysis
5. Discussion
6. Conclusions and Implications
Author Contributions
Funding
Conflicts of Interest
References
- Global Wellness Institute. Global Wellness Tourism Economy; Global Wellness Institute: Miami, FL, USA, 2018. [Google Scholar]
- UNWTO. The Impact of Covid-19 on International Tourism. UNWTO, 2020. Available online: https://webunwto.s3.eu-west-1.amazonaws.com/s3fs-public/2020-09/TMIC.pdf (accessed on 2 November 2020).
- UNWTO. Exploring Health Tourism. World Tourism Organization. 2018. Available online: https://www.e-unwto.org/doi/pdf/10.18111/9789284420209 (accessed on 5 May 2019).
- Baloglu, S.; Busser, J.; Cain, L. Impact of experience on emotional well-being and loyalty. J. Hosp. Mark. Manag. 2019, 28, 427–445. [Google Scholar] [CrossRef]
- Atanga, C.A.; Amuquandoh, F.E.; Amenumey, E.K. Modelling spa-goers’ choices of therapeutic activities. J. Hosp. Tour. Manag. 2017, 31, 105–113. [Google Scholar] [CrossRef]
- Rodrigues, H.; Brochado, A.; Troilo, M. Listening to the murmur of water: Essential satisfaction and dissatisfaction attributes of thermal and mineral spas. J. Travel Tour. Mark. 2019, 37, 649–661. [Google Scholar] [CrossRef]
- Koh, S.; Jung-Eun Yoo, J.; Boger, C.A. Importance-performance analysis with benefit segmentation of spa goers. Int. J. Contemp. Hosp. Manag. 2010, 22, 718–735. [Google Scholar] [CrossRef]
- Pesonen, J.; Laukkanen, T.; Komppula, R. Benefit segmentation of potential wellbeing tourists. J. Vacat. Mark. 2011, 17, 303–314. [Google Scholar] [CrossRef]
- Chen, C.C.; Petrick, J.F. Health and wellness benefits of travel experiences: A literature review. J. Travel Res. 2013, 52, 709–719. [Google Scholar] [CrossRef]
- Hudson, S.; Thal, K.; Cárdenas, D.; Meng, F. Wellness tourism: Stress alleviation or indulging healthful habits? Int. J. Cult. Tour. Hosp. Res. 2017, 11, 35–52. [Google Scholar] [CrossRef]
- Kelly, C. Wellness Tourism: Retreat Visitor Motivations and Experiences. Tour. Recreat. Res. 2012, 37, 205–213. [Google Scholar] [CrossRef]
- Mak, A.H.; Wong, K.K.F.; Chang, R.C.Y. Health or self-indulgence? The motivations and characteristics of spa-goers. Int. J. Tour. Res. 2008, 11, 185–199. [Google Scholar] [CrossRef]
- Vazquez-Illá, J. Estrategias Competitivas para el Sector Balneario. In Panorama Actual de las Aguas Minerales y Minero-Eedicinales en España; López, J.A., Piragua, J.I., Eds.; Ministerio de Medio Ambiente-ITGE: Madrid, Spain, 2000; pp. 41–61. [Google Scholar]
- Ordabayeva, M.; Yessimzhanova, S. Development of Healthcare and Wellness Tourism Marketing. Int. Rev. Manag. Mark. 2016, 6, 118–124. [Google Scholar]
- Dimitrovski, D.; Todorovic, A.T. Clustering wellness tourists in spa environment. Tour. Manag. Perspect. 2015, 16, 259–265. [Google Scholar] [CrossRef]
- Alegría Quintela, J.; Costa, C.; Correia, A. Health, wellness and medical tourism: A conceptual approach. Enl. Tour. Pathmaking J. 2016, 6, 1–18. [Google Scholar]
- Pelegrín-Borondo, J.; Reinares-Lara, E.; Olarte-Pascual, C.; Garcia-Sierra, M. Assessing the Moderating Effect of the End User in Consumer Behavior: The Acceptance of Technological Implants to Increase Innate Human Capacities. Front. Psychol. 2016, 7, 132. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. MIS Q. 2012, 36, 157. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prenticeó Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Pelegrín-Borondo, J.; Arias-Oliva, M.; Olarte-Pascual, C. Emotions, price and quality expectations in hotel services. J. Vacat. Mark. 2016, 23, 322–338. [Google Scholar] [CrossRef]
- García-Milon, A.; Martínez-Ruiz, M.P.; Olarte-Pascual, C.; Pelegrín-Borondo, J. Does the product test really make a difference? Evidence from the launch of a new wine. Food Qual. Prefer. 2019, 71, 422–430. [Google Scholar] [CrossRef]
- Martínez-Ruiz, M.P.; Izquierdo-Yusta, A.; Olarte-Pascual, C.; Reinares-Lara, E. Do Affective Variables Make a Difference in Consumers Behavior Toward Mobile Advertising? Front. Psychol. 2017, 7, 2018. [Google Scholar] [CrossRef] [PubMed]
- Olarte, C.; Pelegrín, J.; Reinares, E.M. Model of acceptance of a new type of beverage: Application to natural sparkling red wine. Span. J. Agric. Res. 2017, 15, e0102. [Google Scholar] [CrossRef]
- Mehrabian, A.; Russell, J.A. An Approach to Environmental Psychology; The MIT Press: Cambridge, MA, USA, 1974. [Google Scholar]
- Russell, J.A.; Mehrabian, A. Evidence for a three-factor theory of emotions. J. Res. Pers. 1977, 11, 273–294. [Google Scholar] [CrossRef]
- Valentine, N.A. Wellness Tourism: Using Tourists’ Preferences to Evaluate the Wellness Tourism Market in Jamaica. Rev. Soc. Sci. 2016, 1, 25–44. [Google Scholar] [CrossRef]
- Hsieh, M.-T. An Examination of the Mature Spring/Spa Travel Market. In Tourism III: Issues in PhD Research; University of Lincoln: Lincoln, UK, 2009. [Google Scholar]
- Kucukusta, D.; Guillet, B.D. Lifestyle Segmentation of Spa Users: A Study of Inbound Travelers to Hong Kong. Asia Pac. J. Tour. Res. 2015, 21, 1–20. [Google Scholar] [CrossRef]
- Kamenidou, I.; Mamalis, S.; Priporas, C.V.; Samara, I. Motivations for Visiting Smokovo’s Thermal Springs. In Proceedings of the International Conference on Contemporary Marketing Issues (ICCMI), Heraklion, Greece, 22–24 June 2016. [Google Scholar]
- Tan, G.W.H.; Ooi, K.B. Gender and age: Do they really moderate mobile tourism shopping behavior? Telemat. Inform. 2018, 35, 1617–1642. [Google Scholar] [CrossRef]
- Alén, M.E.; Fraiz, J.A.; Rufín, R. Analysis of health Spa customers’ expectations and perceptions: The case of Spanish establishments. Tékhne-Rev. Estud. Politécnicos 2006, 5, 245–262. [Google Scholar]
- Chiu, T.M.L.; Ku, B.P.S. Moderating Effects of Voluntariness on the Actual Use of Electronic Health Records for Allied Health Professionals. JMIR Med. Inform. 2015, 3, e7. [Google Scholar] [CrossRef]
- Scherer, K.R. What are emotions? And how can they be measured? Soc. Sci. Inf. 2005, 44, 695–729. [Google Scholar] [CrossRef]
- Pelegrín-Borondo, J.; Juaneda-Ayensa, E.; González-Menorca, L.; González-Menorca, C. Dimensions and basic emotions: A complementary approach to the emotions produced to tourists by the hotel. J. Vacat. Mark. 2015, 21, 351–365. [Google Scholar] [CrossRef]
- Bagozzi, R.P.; Belanche, D.; Casaló, L.V.; Flavián, C. The Role of Anticipated Emotions in Purchase Intentions. Psychol. Mark. 2016, 33, 629–645. [Google Scholar] [CrossRef]
- Cohen, J.B.; Pham, M.T.; Andrade, E.B. The Nature and Role of Affect in Consumer Behavior. In Handbook of Consumer Psychology; Prentice Hall: Upper Saddle River, NJ, USA, 2008; pp. 297–348. [Google Scholar]
- Sharma, P.; Nayak, J.K. Testing the role of tourists’ emotional experiences in predicting destination image, satisfaction, and behavioral intentions: A case of wellness tourism. Tour. Manag. Perspect. 2018, 28, 41–52. [Google Scholar] [CrossRef]
- Plutchik, R. A General Psychoevolutionary Theory of Emotion. In Theories of Emotion; Elsevier BV: Amsterdam, The Netherlands, 1980; pp. 3–33. [Google Scholar]
- Plutchik, R. Emotions: A general psychoevolutionary theory. Approaches Emot. 1984, 1984, 197–219. [Google Scholar]
- Wirtz, J.; Bateson, J.E. Consumer satisfaction with services: Integrating the environment perspective in services marketing into the traditional disconfirmation paradigm. J. Bus. Res. 1999, 44, 55–66. [Google Scholar] [CrossRef]
- Russell, J.A. A circumplex model of affect. J. Personal. Soc. Psychol. 1980, 39, 1161–1178. [Google Scholar] [CrossRef]
- Russell, J.A.; Pratt, G. A description of the affective quality attributed to environments. J. Personal. Soc. Psychol. 1980, 38, 311. [Google Scholar] [CrossRef]
- Russell, J.A.; Barrett, L.F. Core affect, prototypical emotional episodes, and other things called emotion: Dissecting the elephant. J. Personal. Soc. Psychol 1999, 76, 805. [Google Scholar] [CrossRef]
- Richins, M.L. Measuring Emotions in the Consumption Experience. J. Consum. Res. 1997, 24, 127–146. [Google Scholar] [CrossRef]
- Eroglu, S.A.; Machleit, K.A.; Davis, L.M. Atmospheric qualities of online retailing: A conceptual model and implications. J. Bus. Res. 2001, 54, 177–184. [Google Scholar] [CrossRef]
- Bigné, J.E.; Andreu, L.; Gnoth, J. The theme park experience: An analysis of pleasure, arousal and satisfaction. Tour. Manag. 2005, 26, 833–844. [Google Scholar] [CrossRef]
- Bigné, J.E.; Mattila, A.S.; Andreu, L. The impact of experiential consumption cognitions and emotions on behavioral intentions. J. Serv. Mark. 2008, 22, 303–315. [Google Scholar] [CrossRef]
- Yüksel, A.; Akgül, O. Postcards as affective image makers: An idle agent in destination marketing. Tour. Manag. 2007, 28, 714–725. [Google Scholar] [CrossRef]
- Huh, C.; Lee, M.J.; Lee, S. A profile of spa-goers in the U.S. luxury hotels and resorts: A posteriori market segmentation approach. J. Hosp. Mark. Manag. 2019, 28, 1032–1052. [Google Scholar] [CrossRef]
- Han, H.; Thuong, P.T.M.; Kiatkawsin, K.; Ryu, H.B.; Kim, J.; Kim, W. Spa hotels: Factors promoting wellness travelers’ postpurchase behavior. Soc. Behav. Pers. Int. J. 2019, 47, 1–13. [Google Scholar] [CrossRef]
- Oliveira, T.; Araujo, B.; Tam, C. Why do people share their travel experiences on social media? Tour. Manag. 2020, 78, 104041. [Google Scholar] [CrossRef]
- Ono, A.; Kawamura, S.; Nishimori, Y.; Oguro, Y.; Shimizu, R.; Yamamoto, S. Anime pilgrimage in Japan: Focusing Social Influences as determinants. Tour. Manag. 2020, 76, 103935. [Google Scholar] [CrossRef]
- Klaysung, C. Behaviors and Factors Affecting the Selection of Spa Services among Consumers in Amphawa, Samut Songkhram, Thailand. Int. J. Soc. Tour. Sci. 2016, 10, 3897–3901. [Google Scholar]
- Kim, S.H.; Huh, C.; Knutson, B. A Predictive Model of Behavioral Intention to Spa Visiting: An Extended Theory of Planned Behavior. In Proceedings of the International CHRIE Conference-Refereed Track, Amhert, MA, USA, 28–31 July 2010. [Google Scholar]
- Haley, R.I. Benefit segmentation: A decision-oriented research tool. J. Mark. 1968, 32, 30–35. [Google Scholar] [CrossRef]
- Frochot, I.; Morrison, A.M. Benefit Segmentation: A Review of Its Applications to Travel and Tourism Research. J. Travel Tour. Mark. 2000, 9, 21–45. [Google Scholar] [CrossRef]
- Carrera, P.M.; Bridges, J.F. Globalization and healthcare: Understanding health and medical tourism. Expert Rev. Pharm. Outcomes Res. 2006, 6, 447–454. [Google Scholar] [CrossRef]
- Laing, J.; Weiler, B. Mind, Body and Spirit: Health and Wellness Tourism in Asia. In Asian Tourism: Growth and Change; Cochrane, J., Ed.; Routledge: London, UK, 2007; pp. 379–389. [Google Scholar]
- Romanova, G.; Vetitnev, A.; Dimanche, F. Health and Wellness Tourism. In Tourism in Russia: A Management Handbook; Dimanche, F., Andrades, L., Eds.; Emerald: Bingley, UK, 2015; pp. 231–287. [Google Scholar]
- Dryglas, D.; Salamaga, M. Segmentation by push motives in health tourism destinations: A case study of Polish spa resorts. J. Destin. Mark. Manag. 2018, 9, 234–246. [Google Scholar] [CrossRef]
- Butler, R.; Szromek, A.R. Incorporating the Value Proposition for Society with Business Models of Health Tourism Enterprises. Sustainability 2019, 11, 6711. [Google Scholar] [CrossRef]
- Costa, C.; Quintela, J.; Mendes, J.F.F. Health and Wellness Tourism: A Strategic Plan for Tourism and Thermalism Valorization of São Pedro do Sul. In Health and Wellness Tourism; Peris-Ortiz, P., Álvarez-García, J., Eds.; Springer: Cham, Switzerland, 2015; pp. 21–31. [Google Scholar]
- Koskinen, V.; Wilska, T.-A. Identifying and understanding spa tourists’ wellness attitudes. Scand. J. Hosp. Tour. 2018, 19, 259–277. [Google Scholar] [CrossRef]
- Kamata, H.; Misui, Y. The Difference of Japanese Spa Tourists Motivation in Weekends and Weekdays. Procedia Soc. Behav. Sci. 2015, 175, 210–218. [Google Scholar] [CrossRef][Green Version]
- Lee, C.; King, B. Using the Delphi method to assess the potential of Taiwan’s hot springs tourism sector. Int. J. Tour. Res. 2008, 10, 341–352. [Google Scholar] [CrossRef]
- Ardell, D.B. The history and future of wellness. Health Values 1985, 9, 37–56. [Google Scholar]
- Diener, E.; Seligman, M.E.P. Beyond Money: Toward an Economy of Well-Being. Underst. Investig. Response Process. Valid. Res. 2009, 5, 201–265. [Google Scholar] [CrossRef]
- Konu, H.; Tuohino, A.; Komppula, R. Lake Wellness—A Practical Example of a New Service Development (NSD) Concept in Tourism Industries. J. Vacat. Mark. 2010, 16, 125–139. [Google Scholar] [CrossRef]
- Voigt, C.; Pforr, C. (Eds.) Wellness Tourism: A Destination Perspective; Routledge: London, UK, 2013. [Google Scholar]
- Chen, J.S.; Prebensen, N.K.; Huan, T.C.T. Determining the Motivation of Wellness Travelers. Anatolia 2011, 19, 103–115. [Google Scholar] [CrossRef]
- Boekstein, M. From illness to wellness: Has thermal spring health tourism reached a new turning point? Afr. J. Hosp. Tour. Leis. 2014, 3, 1–11. [Google Scholar]
- Turgalicia. Balnearios de Galicia. 2019. Available online: https://www.turismo.gal/inicio (accessed on 30 May 2019).
- Lara, E.R.; Olarte-Pascual, C.; Pelegrín-Borondo, J. Do you want to be a cyborg? The moderating effect of ethics on neural implant acceptance. Comput. Hum. Behav. 2018, 85, 43–53. [Google Scholar] [CrossRef]
- Miniero, G.; Codini, A.; Bonera, M.; Corvi, E.; Bertoli, G. Being green: From attitude to actual consumption. Int. J. Consum. Stud. 2014, 38, 521–528. [Google Scholar] [CrossRef]
- Loureiro, S.M.C. The Role of Website Quality on PAD, Attitude and Intentions to Visit and Recommend Island Destination. Int. J. Tour. Res. 2015, 17, 545–554. [Google Scholar] [CrossRef]
- Dijkstra, T.K.; Henseler, J. Consistent Partial Least Squares Path Modeling. MIS Q. 2015, 39, 297–316. [Google Scholar] [CrossRef]
- Gefen, D.; Rigdon, E.E.; Straub, D. Editor’s Comments: An Update and Extension to SEM Guidelines for Administrative and Social Science Research. MIS Q. 2011, 35, 3–14. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sinkovics, R.R. The use of partial least squares path modeling in international marketing. Adv. Int. Mark. 2009, 20, 277–319. [Google Scholar]
- Mosquera, A.; Juaneda-Ayensa, E.; Olarte-Pascual, C.; Pelegrín-Borondo, J. Key Factors for In-Store Smartphone Use in an Omnichannel Experience: Millennials vs. Nonmillennials. Complexity 2018, 2018, 1–14. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Research Universe | Spanish Residents Who Do Not Live in Pantón |
|---|---|
| Data collection method | Quantitative survey, administered face-to-face or by phone |
| Sample | 810 people |
| Data collection period | March and April 2019 |
| Sample characteristics | |
| Gender | Men: 50% Women: 50% |
| Age | 20 to 30 years old: 20% 31 to 40 years old: 20% 41 to 50 years old: 20% 51 to 60 years old: 20% 61 years old or more: 20% |
| Formal education | No formal education: 3.5% Primary school: 27.7% Secondary school: 32.2% Higher education: 36.5% |
| Construct | Items | Source |
|---|---|---|
| Performance Expectancy (PE) | PE1. Using the thermal suite would be useful to me PE2. Using the thermal suite would increase my chances of achieving things that are important to me PE3. Using the thermal suite would help me achieve my goals faster PE4. Using the thermal suite would increase my quality of life | [19] |
| Effort Expectancy (EE) | EE1. It will be easy for me to learn how to use the thermal suite EE2. For me, how to use the thermal suite will be clear and comprehensible EE3. It will be easy for me to use the thermal suite EE4. It will be easy for me to be an expert in using the thermal suite | |
| Social Influence (SI) | SI1. The people who are important to me would think that I should use the thermal suite SI2. The people who influence me would think that I should use the thermal suite SI3. The people whose opinions I value would like me to use the thermal suite | |
| Pleasure (PL) | PL1. Unhappy–Happy PL2. Annoyed–Pleased | [79] |
| Arousal (AR) | AR1. Relaxed–Stimulated AR2. Calm–Excited | |
| Purchase Intention (PI) | PI1. If I went to the area, I would intend to use the thermal suite PI2. If I went to the area, I predict that I would use the thermal suite | [21] |
| Construct | Wellness | Healthcare/Medical |
|---|---|---|
| Performance Expectancy | ||
| PE1 | 0.886 (34.15) | 0.801 (16.79) |
| PE2 | 0.804 (63.64) | 0.821 (20.47) |
| PE3 | 0.779 (29.53) | 0.783 (23.67) |
| PE4 | 0.764 (24.51) | 0.777 (19.26) |
| Effort Expectancy | ||
| EE1 | 0.839 (11.61) | 0.835 (7.29) |
| EE2 | 0.934 (14.27) | 0.804 (12.51) |
| EE3 | 0.856 (12.24) | 0.884 (15.62) |
| EE4 | 0.662 (6.643) | 0.881 (10.81) |
| Pleasure | ||
| PL1 | 0.925 (21.75) | 0.896 (20.04) |
| PL2 | 0.803 (15.94) | 0.897 (16.81) |
| Arousal | ||
| AR1 | u.i. | u.i. |
| Social Influence | ||
| SI1 | 0.932 (45.45) | 0.906 (29.99) |
| SI2 | 0.921 (41.71) | 0.951 (53.76) |
| SI3 | 0.924 (49.92) | 0.959 (41.76) |
| Purchase Intention | ||
| PI1 | 0.909 (49.12) | 0.908 (25.18) |
| PI2 | 0.923 (38.61) | 0.937 (36.08) |
| Construct | Composite Reliability > 0.7 | Cronbach’s Alpha | AVE > 0.5 | PE | EE | P | A | SI | PI |
|---|---|---|---|---|---|---|---|---|---|
| WELLNESS | |||||||||
| Performance Expectancy (PE) | 0.89 | 0.88 | 0.66 | 0.81 | 0.19 | 0.32 | 0.25 | 0.73 | 0.67 |
| Effort Expectancy (EE) | 0.90 | 0.90 | 0.69 | 0.19 | 0.83 | 0.39 | 0.08 | 0.26 | 0.33 |
| Pleasure (P) | 0.85 | 0.86 | 0.75 | 0.32 | 0.39 | 0.87 | 0.04 | 0.32 | 0.45 |
| Arousal (A) | 1.00 | 1.00 | 1.00 | 0.25 | −0.07 | −0.03 | 1.00 | 0.19 | 0.13 |
| Social Influence (SI) | 0.95 | 0.95 | 0.86 | 0.73 | 0.26 | 0.32 | 0.19 | 0.93 | 0.53 |
| Purchase Intention (PI) | 0.91 | 0.91 | 0.84 | 0.68 | 0.33 | 0.45 | 0.13 | 0.53 | 0.92 |
| HEALTHCARE/MEDICAL | |||||||||
| Performance Expectancy | 0.87 | 0.87 | 0.63 | 0.80 | 0.47 | 0.51 | 0.09 | 0.77 | 0.71 |
| Effort Expectancy | 0.91 | 0.91 | 0.73 | 0.47 | 0.85 | 0.37 | 0.05 | 0.44 | 0.39 |
| Pleasure | 0.89 | 0.89 | 0.80 | 0.51 | 0.37 | 0.90 | 0.14 | 0.39 | 0.44 |
| Arousal | 1.00 | 1.00 | 1.00 | 0.09 | −0.02 | −0.14 | 1.00 | 0.02 | 0.02 |
| Social Influence | 0.96 | 0.96 | 0.88 | 0.77 | 0.44 | 0.39 | 0.02 | 0.94 | 0.56 |
| Purchase Intention | 0.92 | 0.92 | 0.85 | 0.71 | 0.39 | 0.44 | −0.01 | 0.56 | 0.92 |
| Construct | Path Coefficients-Diff. (Wellness vs. Healthcare/Medical) | p-Value of the Henseler Test |
|---|---|---|
| Performance Expectancy ≥ (+) Purchase Intention | –0.04 | 0.60 |
| Effort Expectancy ≥ (+) Purchase Intention | 0.09 | 0.16 |
| Pleasure ≥ (+) Purchase Intention | 0.13 | 0.08 |
| Arousal ≥ (+) Purchase Intention | 0.05 | 0.21 |
| Social Influence ≥ (+) Purchase Intention | –0.03 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelegrín-Borondo, J.; Araújo-Vila, N.; Fraiz-Brea, J.A. Comparison of Spa Choice between Wellness Tourists and Healthcare/Medical Tourists. Healthcare 2020, 8, 544. https://doi.org/10.3390/healthcare8040544
Pelegrín-Borondo J, Araújo-Vila N, Fraiz-Brea JA. Comparison of Spa Choice between Wellness Tourists and Healthcare/Medical Tourists. Healthcare. 2020; 8(4):544. https://doi.org/10.3390/healthcare8040544
Chicago/Turabian StylePelegrín-Borondo, Jorge, Noelia Araújo-Vila, and Jose A. Fraiz-Brea. 2020. "Comparison of Spa Choice between Wellness Tourists and Healthcare/Medical Tourists" Healthcare 8, no. 4: 544. https://doi.org/10.3390/healthcare8040544
APA StylePelegrín-Borondo, J., Araújo-Vila, N., & Fraiz-Brea, J. A. (2020). Comparison of Spa Choice between Wellness Tourists and Healthcare/Medical Tourists. Healthcare, 8(4), 544. https://doi.org/10.3390/healthcare8040544