Abstract
Background: In 2010, the World Health Organization issued a clarion call for action on interprofessional education and collaboration. This call came forty years after the concept of interprofessional collaboration (IPC) was introduced. Aim: To conduct an integrative review of interprofessional collaboration in health care education in order to evaluate evidence and build the case for university support and resources and faculty engagement, and propose evidence-based implications and recommendations. Search Strategy: A literature search was conducted by an interprofessional faculty from a college of nursing and health sciences. Databases searched included CINAHL, Medline, Eric, Pubmed, Psych Info Lit., and Google Scholar. Keywords were interdisciplinary, interprofessional, multidisciplinary, transdisciplinary, health care team, teamwork, and collaboration. Inclusion criteria were articles that were in the English language, and published between 1995 and 2019. Review Methods: Thirteen interprofessional team members searched assigned databases. Based on key words and inclusion criteria, over 216,885 articles were identified. After removing duplicates, educational studies, available as full text were reviewed based on titles, and abstracts. Thirty-two articles were further evaluated utilizing the Sirriyeh, Lawton, Gardner, and Armitage (2012) review system. Faculty agreed that an inclusion score of 20 or more would determine an article’s inclusion for the final review. Eighteen articles met the inclusion score and the data was reduced and analyzed using the Donabedian Model to determine the structure, processes, and outcomes of IPC in health care education. Results: Structure included national and international institutions of higher education and focused primarily on undergraduate and graduate health care students’ experiences. The IPC processes included curricular, course, and clinical initiatives, and transactional and interpersonal processes. Outcomes were positive changes in faculty and health care students’ knowledge, attitudes, and skills regarding IPC, as well as challenges related to structure, processes, and outcomes which need to be addressed. Implications/Recommendations/Conclusions: The creation of a culture of interprofessional collaboration requires a simultaneous “top–down” and “bottom–up” approach with commitment by the university administration and faculty. A university Interprofessional Strategic Plan is important to guide the vision, mission, goals, and strategies to promote and reward IPC and encourage faculty champions. University support and resources are critical to advance curricular, course, and clinical initiatives. Grassroots efforts of faculty to collaborate with colleagues outside of their own disciplines are acknowledged, encouraged, and established as a normative expectation. Challenges to interprofessional collaboration are openly addressed and solutions proposed through the best thinking of the university administration and faculty. IPC in health care education is the clarion call globally to improve health care.
1. Introduction
In 2010, the World Health Organization (WHO) [1] issued a clarion call titled: Framework for Action on Interprofessional Education and Collaborative Practice. The WHO framework came forty years after the concepts of interprofessional education (IPE) and interprofessional collaboration (IPC) were introduced [2]. The concept of interprofessional education (IPE) is as an essential combination of knowledge, attitudes, values, skills, and behaviors that make up collaborative practice. IPE allows for team-based problem solving and promotes the best thinking of health professionals in offering quality health care [1]. IPC represents the interaction between the professionals from various disciplines who share the same goals with collective action [3]. The Canadian Interprofessional Health Collaborative [4] describe IPC as the process of developing and maintaining effective working relationships to obtain optimal health outcomes.
Currently, health care systems are faced with significant issues of preventable mortality and morbidity, increasing medical errors, inadequacies in costly and fragmented systems of care, as well as lack of patient-centered care [5,6]. Thus, IPE and IPC are deemed critical to clinicians, researchers, professional groups, and government [7,8]. Institutions of higher learning are being called to lead transformational change in health care education beginning with a review of the curricula and educational outcomes of the various health disciplines and areas where IPC naturally align. The WHO [1] report emphasized that educational and health care systems must coordinate to develop educator and curricula mechanisms which support IPC.
To address implementation issues, the WHO [1] report also emphasized the importance of institutional support and working culture mechanisms, such as communication strategies, conflict resolution policies, and shared decision making. Additionally, issues were discussed related to the need for building space and facilities that accommodate IPC. The WHO [1] report suggested that activities conducted during formal education programs could provide future health care providers with critical knowledge. Such knowledge would hopefully motivate students to provide interprofessional services when students become part of the health care workforce.
The WHO [1] framework not only identified mechanisms to shape successful teamwork but also outlined actions to be applied in academic and health care systems. In accordance with the Interprofessional Education Collaborative (IPEC) [9], faculty in Colleges of Health Professions were encouraged to develop core competencies for collaborative practice in all professional curricula. Such core competencies would embed essential content of interprofessional communication, patient-family centered care, role clarification, collaborative leadership, and conflict resolution. Students who engage in IPE are more likely to collaborate and implement interprofessional health care [10,11,12,13,14], with the proposed ultimate outcomes as improvement in the experience of health care, and quality of health care with a reduction in cost [1,8].
In addition, an Institute of Medicine Report (IOM) provided an interprofessional learning continuum model to implement and evaluate interprofessional educational efforts focused on preparing future health practitioners with interprofessional collaboration skills in the workplace. The WHO framework and the IOM model address the growing body of evidence that well-planned interprofessional learning is the antecedent of patient-centered, cost-effective, efficient, safer, timelier, and more equitable health care [1,8,15,16]. Through interprofessional education and training, health professionals may come to recognize shared values and codes of conduct, and move from a sense of independence to interdependence to provide patient-centered, holistic health care [16]. A paradigm shift in the education emphasizes the critical fit between interprofessional education and real-world interprofessional collaborative practice across health care settings [16,17].
The aim of this integrative review was to evaluate evidence related to interprofessional education in health care education and identify structures, processes, and outcomes that may serve to build the case for university support and resources and faculty engagement, and propose evidence-based implications and recommendations.
2. Review Methodology
Cooper’s [18] five-stage integrative review method, as modified by Whittemore and Knalf [19], was used to guide the review, including (1) problem identification (defining the problem); (2) searching the literature (data collection); (3) quality appraisal (evaluation of the data); (4) data analysis and interpretation (data abstraction); and (5) presentation of the results (data synthesis).
2.1. Problem Identification
The interprofessional committee of a college of nursing and health sciences identified the need to evaluate evidence related to the outcomes of interprofessional collaboration (IPC) in health care education. The committee acknowledged that the strategic plans of universities often address the importance of IPC. However, moving the idea of IPC in health care education from the thought phase to the planning and implementation phases requires the buy in of several stakeholder groups including individual learners, educators, health care professionals, researchers and very importantly administrators. Furthermore, the resources and funds allocated to promote interprofessional initiatives are dependent on providing the evidence which supports not only the efficacy of IPC in terms of learning outcomes and health care outcomes, but of the context through which those outcomes are achieved.
2.2. Searching the Literature
To identify articles relevant to the literature review, thirteen members from six health professions of the college interprofessional (IP) committee formed teams and conducted an initial search of the following databases: CINAHL, Medline, Pubmed, Eric, Psych Info Lit, and Google Scholar. Search keywords were: interdisciplinary, interprofessional, transdisciplinary, multidisciplinary, collaborative, health care team, and teamwork. Inclusion criteria were English language, and published from 1995 to 2019. Although the concept of interprofessional education can be found in the literature as early as the 1970′s, we speculated, based on knowledge of the health sciences, that research studies would most likely be published from 1995 and beyond.
Based on key words and inclusion criteria, over 216,885 articles were identified. After removing duplicates, educational studies that were full text were identified and reviewed first by title and then based on their abstracts. Sixty-three articles were uploaded into a Google drive database to be accessible for review by the entire team. Six systematic reviews were reviewed, as reference points, but 32 single studies were included for an in-depth appraisal (refer to Figure 1: Search Strategy).
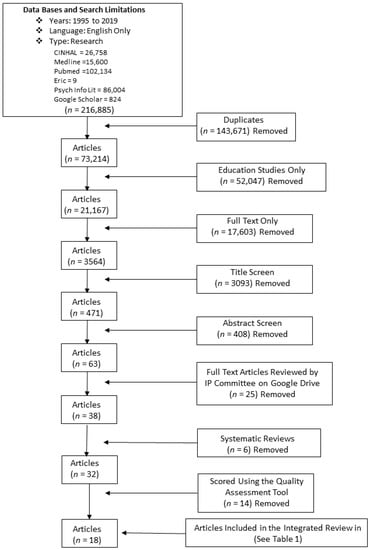
Figure 1.
Search Strategy.
2.3. Quality Appraisal/Evaluation
The articles were then assigned to teams to evaluate the strength of the 32 studies using the Quality Assessment Tool (QAT) developed by Sirriyeh, Lawton, Gardner, and Armitage [20]. This tool ranked the studies on 14 criteria for both quantitative and qualitative studies and two additional criteria added to the score for mixed-methods studies. The scoring of each of the 14 criteria was between zero and three points with the range of scores from 0 to 42. Each member of the team individually scored their team’s assigned articles. The assigned team then met to discuss their individual scorings. If there was a discrepancy between scores, the criteria for scoring was discussed and the team members established inter-rater reliability of each article reviewed so that a single score could be cited on the QAT.
After inter-rater reliability was achieved on the 32 educational articles, the IP committee met, and each review team presented the scoring of their assigned articles. The IP committee determined that educational research articles with a score of equal to or greater than 20 points would be included in the integrative review as this was the median value of the range of scores. Eighteen articles met the criteria for inclusion in the review having a score of 20 or greater.
2.4. Data Analysis and Interpretation
Studies to be included in the review were then entered into a table which identified the article’s authors, year of publication, country, journal, title, study aim, design, sample/setting, educational intervention, findings/outcomes, and implications (refer to Table 1).

Table 1.
Articles Selected for Inclusion in the Integrative Review
To further reduce and analyze the data, Tavares de Souza, Dias da Silva, and de Carvalho [21] suggested to categorize the data based on a pre-determined conceptual classification. Accordingly, the Donabedian Model [22,23], which identifies the structure, processes, and outcomes, was used to analyze the selected articles regarding IPC in health care education. According to Donabedian [23], structure speaks to the setting or context, including the organizational characteristics, as well as to the attributes of the provider in which the service is provided. Structure also includes the physical facility and human resources. Process denotes the transactions between groups which may be classified as technical processes or interpersonal processes and contains all health care initiatives. Outcomes are the effects on various populations, such as changes in knowledge, behavior, attitudes, and sense of satisfaction or improvement in the quality of care.
3. Presentation of the Results in Accordance with the Donabedian Model
3.1. Structure
Based on the 18 articles which met the inclusion criteria, structure was identified with regard to the country of origin, settings, participants, disciplines represented, and study designs.
With regard to the country of origin, of the 18 studies, ten were in the United States, two in Canada, and one each in Germany, Sweden, and one across Europe. The settings for 18 studies were in universities or public colleges, while one also involved military medics on a military base, and one study was conducted by 16 health professional institutions at a Student-Run Clinic Conference. Study participants included (1) undergraduate students who were in nursing programs or health science programs; (2) graduate students in the health professions; (3) military medics; (4) faculty members; and (5) administrative and academic staff. The vast majority represented were graduate students. Disciplines represented included undergraduate and graduate nursing students, medical students, and students and practitioners of occupational therapy (OT), physical therapy (PT), physician’s assistants (PA), respiratory therapists (RT), public health, dental, pharmacy, social work, nutrition/dietetics, rehabilitation, psychology, mental health, medical administration, family therapy, speech pathology, exercise, osteopathic students, chiropractors, physiotherapists, medical technicians, orthoptics, paramedics, military medics, and laboratory assistants. Study designs included three qualitative, exploratory case studies, four descriptive, correlational surveys, one retrospective secondary analysis, eight intervention studies, one mixed-methods descriptive study, and one simulation case study (refer to Table 1).
3.2. Processes
A review of processes, as described by the Donabedian Model [23], identified three types of interprofessional initiatives, specifically curricular, course, and clinical initiatives, as well as descriptions of various transactions or interpersonal processes (Refer to Table 2).
Table 2.
Processes Related to IPC in Health Care Education.
3.3. Outcomes
The outcomes of this integrative review have been identified as positive changes in knowledge, attitudes, behaviors, and skills associated with interprofessional collaboration in health care education, as well as identifying the challenges associated with structure, processes, and achieving positive outcomes (Refer to Table 3).
Table 3.
Positive Outcomes and Challenges Related to IPC in Health Care Education.
4. Discussion
A synthesis of the evidence regarding the structure of IPC in health care education highlights that faculty, and supporting staff, in universities and colleges, both in the United States and abroad, are conducting high-quality research studies regarding IPC in health care education. Institutions of higher learning are involving undergraduate and graduate students, across the spectrum of health care professions, as well as professionals already in practice, in response to the WHO [1] call for transformational change in health care education. An integration of high quality descriptive, correlational, intervention, qualitative, and mixed-methods research studies is important to create the science base related to IPC in health care education [4]. In the competitive world of academics, faculty emphasis on leading-edge concepts, such as interprofessional collaboration, may move the needle towards a keen interest of university administrations in the support and funding of interprofessional initiatives. This may be particularly true, if interprofessional collaboration is linked with other benchmarking criteria of institutions, such as occurs in state university systems.
This integrative review has identified the processes of IPC in health care education with successful outcomes, specifically positive changes in knowledge, attitudes, and behaviors/skills of participants. This evidence may be used to build the case for university administration support and resources for curricular, course, and clinical initiatives, as well as faculty engagement. First, curriculum across the university should raise the concept of interprofessional collaboration to a high level of awareness. To do this, administrators can fund faculty to develop an independent interprofessional course, develop interprofessional modules within a curriculum, or make a curricular shift to fund interprofessional teaching of a course. Secondly, within courses in a college or department, administrators can call for the weaving of interprofessional objectives through each course, with associated course readings and assignments, or even the development of specific course modules in which content is tested. In any course, a case study methodology can be used to discuss the roles and competencies of the various health professionals and their expected contributions to the quality of care offered. Role playing the role of another professional provides a learning opportunity to change the lens from which a plan of care is developed. Thirdly, administrators can establish relationships with external clinical agencies to provide student with learning opportunities to experience interprofessional collaboration, such as shadowing of differing health professions. Additionally, administrative funding of large-scale clinical disaster simulations, or cased-based educational simulations in a clinical simulation lab are opportunities which may be planned to engage different health care students (i.e., medicine, nursing and health sciences, public health, psychology). This may pave the way for a cultural shift and normative expectations of the university regarding interprofessional collaboration. The involvement of an interprofessional faculty across departments or colleges showcases the transactions and interpersonal, as well as interprofessional processes as reported by the studies of the integrative review (Refer to Table 1 and Table 2). Faculty role modeling of coordination, communication, cohesion, team planning, decision making, and performance feedback is an important learning strategy for undergraduate and graduate students and junior faculty.
In 2008, Berwick, Nolan and Whittington [42] proposed a Triple Aims framework to evaluate outcomes of interprofessional health care teams, specifically the evaluating the experience, access to, and the cost of health care. Using this framework, Brandt, Lutfiyya, King, and Chioreso [2] conducted a systematic review of IPC and IPE with 20 disciplines. Although the outcomes of quality and cost of health care could not be explicitly mapped to the Triple aims, the results indicated an impact on changes in readiness, attitudes and perceptions of health care providers regarding interprofessional collaboration. Brandt et al. [2] emphasized the importance of exploring further the processes of collaboration and measuring outcomes.
Gathering university-wide data, obtained through varying testing methods, including quantitative tests, as well as qualitative data through observations, and participant narratives, can be used to measure the IPC outcomes of curricular, course and clinical initiatives, and the related transitions and interpersonal processes. This integrative review highlights the resultant positive changes in knowledge, attitudes, skills/behaviors of health care students, faculty, staff and other practicing health professionals regarding interprofessional collaboration, as was also reported by Brandt and colleagues [2]. Given the importance of evidence-based education and practice, the results of educational research studies, as presented in Table 1 and synthesized in Table 3 as positive outcomes, helps to build a case for university administrative support and resources to further interprofessional collaboration in health care education. However, the outcomes also highlight the challenges of interprofessional collaboration in health care education, related to structure, processes and outcomes, which need to be analyzed by the university administration in collaboration with university faculty and with acknowledgment of staff and student perceptions. Through their active engagement, there is an opportunity to create a cultural shift at a university and move toward the institutionalization and normalization of IPC in health care education.
5. Implications and Recommendations
The value of diverse integrative reviews is that each may provide a varying lens with which to view the phenomenon of interprofessional collaboration in health care education and substantiate similar or differing implications. Through the lens of the Donabedian Model [23], the articles included in this integrated review were examined for structure, processes, and outcomes. Our goal was to provide evidence to build the case for university support and resources related to interprofessional collaboration in health care education, further generating valuable ideas and important implications for university administrations and engaging faculty across colleges and units.
First, to promote successful interprofessional collaboration, what is needed is a simultaneous top–down and bottom–up approach that involves commitment from university and college administration, chairs and directors of departments and programs, faculty, staff, students, and colleagues from affiliated health care institutions [43]. Interprofessional initiatives must illustrate commitment to the advancement of each health discipline, allowing their ability to practice to their full extent of their scope of practice, yet with optimal team cooperation, and collaboration [43]. Transformative change in education and clinical practice involves interprofessional networking of colleagues within, across, and beyond the university and those within health care systems and agencies.
Second, the Faculty Senate of a University may create a Senate Interprofessional Committee focused on interprofessional collaboration. This committee may be charged with developing an Interprofessional Strategic Plan, which includes clear vision and mission statements related to interprofessional collaboration in education, research/scholarship, and clinical practice/service, with identified and measurable goals, strategies, tactics, timeline, and products. With administrative support at the university and college levels, signature IP events may be hosted each year, with an invitation to renowned speakers, showcasing successful and exemplary IP initiatives that are occurring at the university and colleges, and conducting focus group discussions of event participants to answer strategic questions with regard to facilitating the processes of collaboration, while overcoming barriers or challenges. At the university or college level, funding may be offered to support formal collaborations for interprofessional research, educational, or practice/service initiatives. Centers for academic teaching may structure workgroups to learn strategies that promote interprofessional collaboration. In university online platforms, such as Blackboard or Canvas, an online non-credit course may be developed with support of administration to serve as a repository for documents, videos, PowerPoint presentations, lectures, discussion boards, and Linked in Learning or YouTube videos related to interprofessional collaboration. Eventually, this course may be developed as a professional development course for university/college students, faculty or staff and eventually be opened to the public for continuing education.
Third, at the college or unit levels, it is important to strategically map IP collaboration across the curriculum by reviewing existing courses, which may already emphasize interprofessional collaboration and practice, or be identified as a course in which common or shared competencies of health professionals provide a valuable venue for interprofessional teaching-learning strategies. All existing courses may be reviewed and modified with the intent to embed essential content of interprofessional communication, patient-family-centered care, role clarification, collaborative leadership, and conflict resolution, as well as including course readings, assignments, and assessment strategies that focus on interprofessional collaboration.
Fourth, it may also be of value to develop an interprofessional course with joint teaching assignments by an interprofessional faculty. The course may extend beyond a didactic course to have a clinical component to promote the practice of interprofessional knowledge and skills in a real-world setting. The course potentially may include clinical assignments in which students may receive feedback from patients and families regarding the care offered by an interprofessional student team. In the proposed interprofessional course, there would be an opportunity to discuss important topics from an interprofessional, as well as discipline specific lens. For example, in the interprofessional course, one goal may be to develop a case study using a comprehensive, interprofessional assessment template. This template may offer the opportunity to recognize shared or unique competencies of various health providers. During initial classes, students may role play a different discipline than their own to appreciate their expertise. Students may participate in panel discussions of a case from an IP perspective, and reflect on personal experiences when a team approach is used to achieve a goal.
As suggested in multiple articles reviewed (Refer to Table 1) [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41], environment is an important aspect in promoting IPC. Besides formal strategies to promote IPC in health care education, colleges or units may provide collaborative environments or learning space, such as shared lounges, shared classrooms, shared simulation labs, and the availability of classroom or community/practice setting for team activities. Department chairs and program directors may suggest opportunities for collaboration with colleagues within or external to the unit. Interprofessional collaborations on research submissions, academic publications or presentations, building online courses and websites, or constructing evaluation tools and exams can be opportunities to support collaboration.
At the university, college and unit levels, it is important to identify individuals who champion IPC and who recognize the value of IPC and IPE in terms of their own professional development, and academic and health care outcomes. Equally important is to share best practices regarding IPC. This may take the form of creating a university online repository of research and best-practice articles published by leading organizations in IPE and IPC. Lastly, the university, colleges, and units may develop normative expectations related to IPC with documentation of IPC in the tenure and promotion process and the annual merit review process, as well as developing formal mechanisms to reward collaborative efforts.
6. Limitations to the Approach
The undertaking of an integrative review by a large team of faculty members is challenging as the experience and expertise of team members may vary. For example, members of the interprofessional committee may be faculty on a clinical track, a tenured-earning track or be tenured faculty with different or similar professional expectations set by the university or college administration. Team members may also have varying professional experience related to interprofessional collaboration, as well as experience with the review methodology, and expertise with library searches and search strategies. It is acknowledged that such limitations may result in the omission of valuable articles relevant to the review identified by colleagues well-versed in the literature regarding interprofessional collaboration. There are faculty team champions who have the knowledge to set up google drives and upload documents, while other team members have less technological savvy. In addition, an integrative review is a relatively long process of scholarship, which requires ongoing commitment and dedication to the review process. Limitations to the approach may also relate to the ability of team members to be flexible in the scheduling of multiple full team meetings, as well as individual group meetings, as the faculty team moves forward from conceptualization of the project, to accepting various administrative roles, participating in all aspects of the search methodology, documentation of results and analysis. Individuals involved in writing of the review article depend on timely feedback from all team members and a thorough critique and editing of the article to the point of journal submission. The limitations to the approach can be overcome by the ongoing commitment of each team member to the project and to each other as colleagues involved in a process of collaboration.
7. Conclusions
This literature review regarding interprofessional collaboration in health care has applied the Donabedian Model [23] lens of structure, processes, and outcomes to analyze the evidence and build the case for university support and resources and faculty engagement. Equally important, it has stimulated valuable ideas and important implications and recommendations for university administration and faculty across colleges and units to promote interprofessional collaboration in health care education. The essential message is that the creation of a culture of interprofessional collaboration requires a simultaneous “top–down” and “bottom–up” approach. When valued by the university administration, opportunities can be created to promote and very importantly, reward collaboration in education, clinical practice, and research/scholarship. The university administration, in collaboration with the Faculty Senate, can lead the way by creating and supporting a Faculty Senate university committee, seeking the support of senate champions who are influencers of faculty across colleges, units, and departments. The grassroots efforts of faculty to collaborate with colleagues outside of their own disciplines are not remanded, and confined in silent silos, but rather are acknowledged, encouraged, and perhaps, established as a normative expectation. Challenges to interprofessional collaboration are openly addressed and solutions proposed through the best thinking of the university administration and faculty, as well as staff and students. Interprofessional strategic planning, involving all stakeholders, has the potential to serve as a catalyst for the synergistic interface of interprofessional collaboration in health care education, clinical practice and research/scholarship. Interprofessional collaboration may become a critical force in the transformation of global health care.
Author Contributions
D.W.S., project administration, conceptualization, methodology, formal analysis, writing original draft preparation, and writing—review and editing; M.F. and A.R.A., project administration, conceptualization, methodology, formal analysis, writing—review and editing; F.A., M.D.L.S., H.E., A.G., J.H., N.H., T.M., A.R., and S.S., conceptualization, methodology, formal analysis, writing—review and editing; S.W., writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We thank Francisco Fajardo for his assistance as an Information and Instruction Services Librarian at Florida International University, Miami, FL.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization (WHO). Framework for Action on Interprofessional Education and Collaborative Practice; World Health Organization: Geneva, Switzerland, 2010; Available online: https://whqlibdoc.who.int/hq/2010/WHO_HRH_HPN_10.3_eng.pdf (accessed on 11 April 2011).
- Brandt, B.; Lutfiyya, M.; King, J.; Chioreso, C. A scoping review of interprofessional collaborative practice and education using the lens of the Triple Aim. J. Interprof. Care 2014, 28, 393–399. [Google Scholar] [CrossRef] [PubMed]
- D’Amour, D.; Oandson, I. Interprofessionality as the field of interprofessional practice and interprofessional education: An emerging concept. J. Interprof. Care 2005, 19, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Canadian Interprofessional Health Collaborative. A National Interprofessional Competency Framework; University of British Columbia: Vancouver, BC, Canada, 2010; Available online: http://www.cihc.ca/files/CIHC_IPCompetencies_Feb1210.pdf (accessed on 21 January 2020).
- Olenick, M.; Allen, L.; Smego, R. Interprofessional education: Concept analysis. Adv. Med. Educ. Pract. 2010, 1, 75. [Google Scholar] [PubMed]
- Sherman, D.W.; Wilkinson, A. Interprofessional collaboration. In Palliative Care Nursing: Quality Care through the End of Life, 2nd ed.; Matzo, M., Sherman, D.W., Eds.; Springer: New York, NY, USA, 2019; p. 37. [Google Scholar]
- Engel, J.; Prentice, D. The ethics of interprofessional collaboration. Nurs. Ethics 2013, 20, 426–435. [Google Scholar] [CrossRef]
- Gilbert, J.; Yan, J.; Hoffman, S. A WHO report: Framework for action on interprofessional education and collaborative practice. J. Allied Health 2010, 39, 96–197. [Google Scholar]
- Interprofessional Education Collaborative (IPEC). Core Competencies for Interprofessional Collaborative Practice: Report of an Expert Panel; Interprofessional Education Collaborative: Washington, DC, USA, 2011. [Google Scholar]
- Abu-Rish, E.; Kim, S.; Choe, L.; Varpio, L.; Malik, E.; White, A.; Craddick, K. Current trends in interprofessional education in health science students: A literature review. J. Interprof. Care 2012, 26, 144–451. [Google Scholar] [CrossRef]
- Norby, B. Healthcare students as innovative partners in the development of future healthcare services: An action research approach. Nurse Educ. Today 2016, 46, 4–9. [Google Scholar] [CrossRef]
- Pype, P.; Symons, L.; Wens, J.; Van den Eynden, B.; Tess, A.; Cherry, G.; Deveugele, M. Healthcare professionals’ perceptions toward interprofessional collaboration in palliative home care: A view from Belgium. J. Interprof. Care 2010, 27, 313–319. [Google Scholar] [CrossRef]
- Rodger, S.; Hoffman, S. Where in the world is interprofessional collaboration? A global environmental scan. J. Interprof. Care 2010, 24, 479–491. [Google Scholar] [CrossRef]
- Verhaegh, K.; Seller-Boersma, A.; Simons, R.; Steenbruggen, J.; Geerlings, S.; de Rooil, J.; Buurman, B. An exploratory study of healthcare professionals’ perceptions of interprofessional communication and collaboration. J. Interprof. Care 2017, 31, 397–400. [Google Scholar] [CrossRef]
- Institute of Medicine (IOM). Measuring the impact of interprofessional education on collaborative practice and patient outcomes. Rep. Brief 2015, 30, 23–26. Available online: http://www.nationalacademies.org/hmd/Reports/2015/Impact-of-IPE.aspx (accessed on 11 August 2018).
- Karstadt, L. Does interprofessional education provide a global template? Br. J. Nurs. 2012, 21, 522–530. [Google Scholar] [CrossRef]
- Milton, C. Ethical issues surrounding interprofessional collaboration. Nurs. Sci. Q. 2013, 26, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Cooper, H. Scientific guidelines for conducting integrative research reviews. Rev. Educ. Res. 1982, 52, 291–302. [Google Scholar] [CrossRef]
- Whittemore, J.; Knalf, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Sirriyeh, R.; Lawton, R.; Gardner, P.; Armitage, G. Reviewing studies with diverse designs: The development and evaluation of a new tool. J. Eval. Clin. Pract. 2012, 18, 746–752. Available online: http://www.who.int/hrh/resources/framework_action/en/ (accessed on 22 September 2019). [CrossRef] [PubMed]
- Souza, M.T.D.; Silva, M.D.D.; Carvalho, R.D. Integrative review: What is it? How to do it? Einstein 2010, 8, 102–106. [Google Scholar] [CrossRef]
- Donabedian, A. The quality of care. How can it be assessed? Arch. Pathol. Lab. Med. 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Donabedian, A. An Introduction to Quality Assurance in Health Care, 1st ed.; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Murray, F.; Judge, E.; Morris, T.; Opsahl, A. Interprofessional education: A disaster response simulation activity for military medics, nursing, & paramedic science students. Nurse Educ. Pract. 2019, 39, 67–72. [Google Scholar]
- Chen, K.; Kruger, J.; McCarther, N.; Meah, Y. Interprofessional, learner-driven collaboration for innovative solutions to healthcare delivery in student-run clinics. J. Interprof. Care 2019, 34, 137–139. [Google Scholar] [CrossRef]
- Mahler, C.; Schwarzbeck, V.; Mink, J.; Goetz, K. Students’ perception of interprofessional education in the bachelor programme “Interprofessional Health Care” in Heidelberg, Germany: An exploratory case study. BMC Med. Educ. 2018, 18, 19. [Google Scholar] [CrossRef] [PubMed]
- Achkar, M.; Hanauer, M.; Colavecchia, C.; Seehuser, D. Interprofessional education in graduate medical education: Survey study of residency program directors. BMC Med. Educ. 2018, 18, 11. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Brommelsiekv, M.; Amelung, S. An interprofessional education project to address veterans’ healthcare needs. Int. J. High. Educ. 2017, 6, 1–16. [Google Scholar] [CrossRef]
- Reed, C.; Garcia, L.; Slusser, M.; Konowitz, S.; Yep, J. Linking essential learning outcomes and interprofessional collaborative practice competency in health science undergraduates. J. Scholarsh. Teach. Learn. 2017, 17, 15–33. [Google Scholar] [CrossRef][Green Version]
- Shagrir, L. Collaborating with colleagues for the sake of academic and professional development in higher education. Int. J. Acad. Dev. 2017, 22, 331–342. [Google Scholar] [CrossRef]
- Nagge, J.; Lee-Poy, M.; Richard, C. Evaluation of a unique interprofessional education program involving medical and pharmacy students. J. Interprof. Care 2017, 81, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, S.; Harnish, D. The merit of mandatory interprofessional education for pre-health professional students. Med. Teach. 2007, 29, e235–e242. [Google Scholar] [CrossRef]
- Renchler, L.; Rhodes, D.; Cox, C. Effect of interprofessional clinical education programme length on students’ attitudes towards teamwork. J. Interprof. Care 2016, 30, 338–346. [Google Scholar] [CrossRef]
- Townsend, T.; Pisapia, J.; Razzaq, J. Fostering interdisciplinary research in universities: A case study of leadership, alignment, and support. Stud. High. Educ. 2015, 40, 658–675. [Google Scholar] [CrossRef]
- Arenson, C.; Umland, E.; Collins, L.; Kern, S.; Hweston, L.; Jerpbak, C.; Antony, R.; Rose, M.; Lyons, K. The health mentors program: Three years experiences with longitudinal patient-centered interprofessional education. J. Interprof. Care 2015, 29, 138–143. [Google Scholar] [CrossRef]
- Borrego, M.; Boden, D.; Newswander, L. Sustained change: Institutionalizing interdisciplinary graduate education. J. High. Educ. 2014, 85, 858–884. [Google Scholar] [CrossRef]
- Ekmekci, O. Promoting collaboration in health care teams through interprofessional education: A simulated case study. Int. J. High. Educ. 2013, 2, 78–83. [Google Scholar] [CrossRef]
- Hylin, U.; Lonka, K.; Ponzer, S. Students’ approaches to learning in clinical interprofessional context. Med. Teach. 2011, 33, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Miers, M.; Rickaby, C.; Clarke, B. Learning to work together: Health and social care students’ learning from interprofessional modules. Assess. Eval. High. Educ. 2009, 34, 673–691. [Google Scholar] [CrossRef]
- Priest, H.; Roberts, P.; Dent, H.; Blincoe, C.; Lawton, D.; Armstrong, C. Interprofessional education and working in mental health; in search of the evidence base. J. Nurs. Manag. 2008, 16, 474–485. [Google Scholar] [CrossRef]
- Florence, J.; Goodrow, B.; Wachs, J.; Grove, S.; Olive, K. Rural health professions education at East Tennessee State University: Survey of graduates from first decade of the community participation program. J. Rural Health 2007, 23, 77–83. [Google Scholar] [CrossRef]
- Berwick, D.; Nolan, T.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef]
- Sherman, D.W.; Maitra, K.; Hough, M.; Restrepo, J.; Barbera, S.; Olenick, M.; Randolph, M.; Simon, S.; Gordon, Y.; Singh, A. Illustrating and analyzing the processes of interprofessional collaboration: Lessons learned from palliative care in deconstructing the concept. J. Palliat. Med. 2017, 20, 227–234. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).