Increased Risk of COVID-19-Related Deaths among General Practitioners in Italy



{kind=link}
{kind=link}
Abstract
1. Introduction
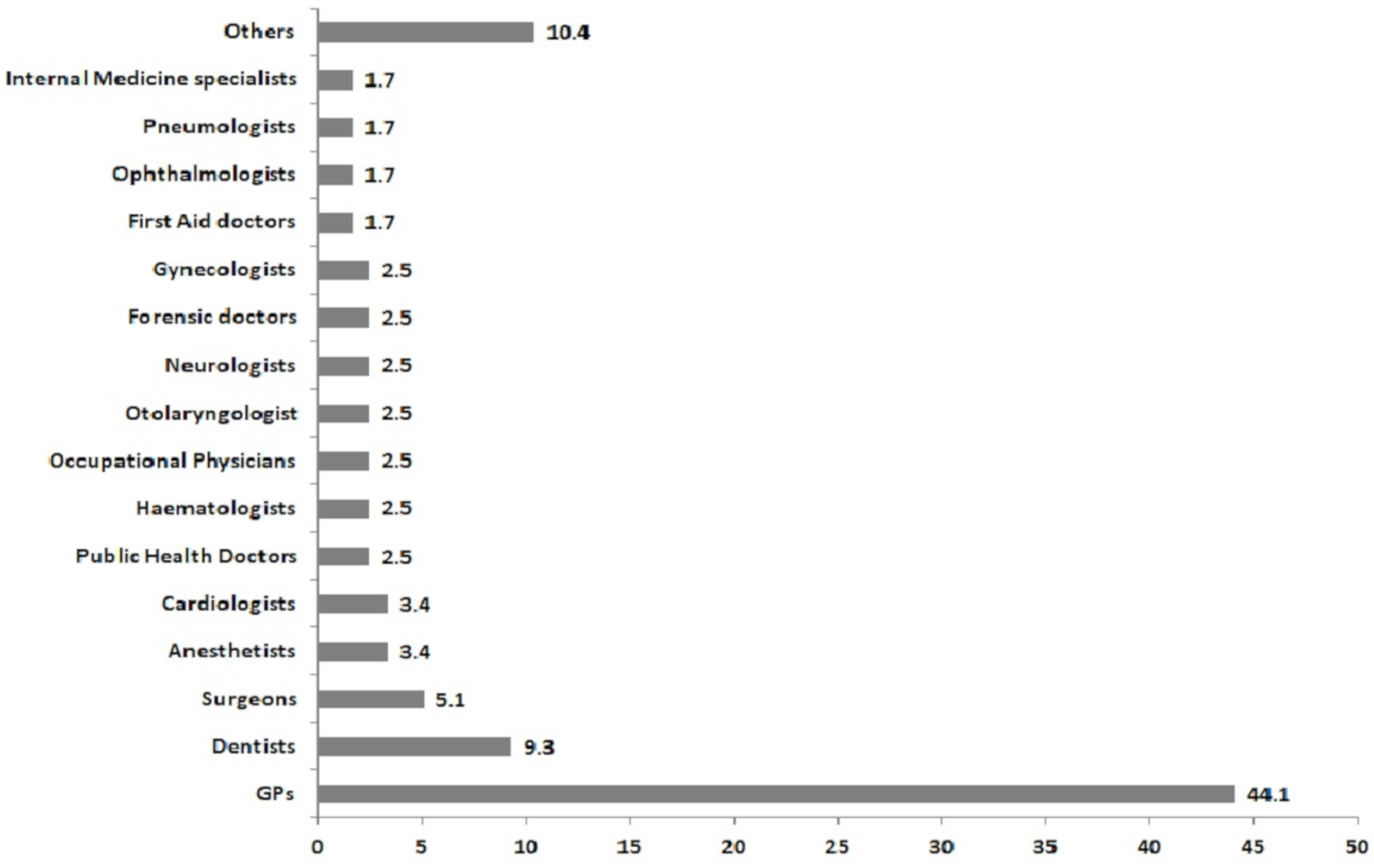
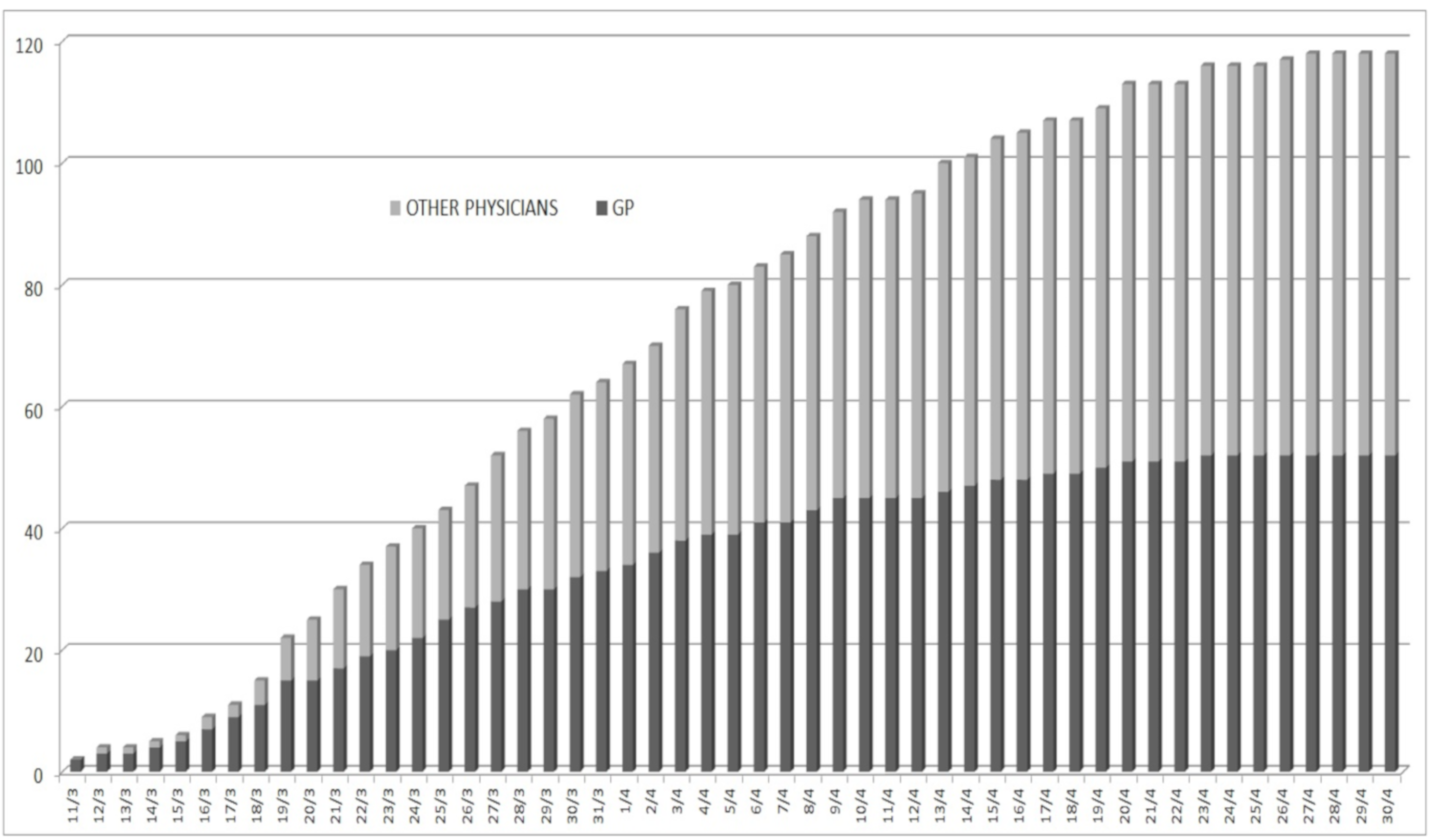
2. Discussion: The Italian Data on COVID-19-Related Deaths among General Practitioners and Other Physicians
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Semple, S.; Cherrie, J.W. Covid-19: Protecting Worker Health. Ann. Work Expo. Health 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Integrated Surveillance of COVID-19 in Italy (Ordinanza n. 640 del 27/02/2020) 25 May 2020 UPDATE. Available online: https://www.epicentro.iss.it/en/coronavirus/bollettino/Infografica_25maggio%20ENG.pdf (accessed on 26 May 2020).
- Guidance for Health Workers. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/health-workers (accessed on 9 May 2020).
- Infection Prevention and Control and Preparedness for COVID-19 in Healthcare Settings—Second Update. Available online: https://www.ecdc.europa.eu/en/publications-data/infection-prevention-and-control-and-preparedness-covid-19-healthcare-settings (accessed on 9 May 2020).
- Information for Healthcare Professionals about Coronavirus (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-nCoV/hcp/index.html (accessed on 9 May 2020).
- Kamerow, D. Covid-19: Don’t forget the impact on US family physicians. BMJ 2020, 368, m1260. [Google Scholar] [CrossRef]
- Elenco dei Medici Caduti nel Corso Dell’epidemia di Covid-19 (List of the Physicians Died during the COVID-19 Epidemic). Available online: https://portale.fnomceo.it/elenco-dei-medici-caduti-nel-corso-dellepidemia-di-covid-19/ (accessed on 9 May 2020).
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Elaborazione di Dati sul Personale in Attività nel Sistema Sanitario Pubblico e Privato (Data Analysis on Active Health Personnel in the Public and Private Health Services). Available online: http://dati.istat.it/Index.aspx?DataSetCode=DCIS_PERS_SANIT (accessed on 9 May 2020).
- To, K.K.; Tsang, O.T.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect Dis. 2020, 20, P565–P574. [Google Scholar] [CrossRef]
- Yang, J.R.; Deng, D.T.; Wu, N.; Yang, B.; Li, H.J.; Pan, X.B. Persistent viral RNA positivity during recovery period of a patient with SARS-CoV-2 infection. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Fiorino, G.; Colombo, M.; Natale, C.; Azzolini, E.; Lagioia, M.; Danese, S. Clinician Education and Adoption of Preventive Measures for COVID-19: A Survey of a Convenience Sample of General Practitioners in Lombardy, Italy. Ann. Intern. Med. 2020, M20-1447. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Yokoe, D.S.; Havlir, D.V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. N. Engl. J. Med. 2020, 382, 2158–2160. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Bahl, P.; Doolan, C.; de Silva, C.; Chughtai, A.A.; Bourouiba, L.; MacIntyre, C.R. Airborne or droplet precautions for health workers treating COVID-19? J. Infect. Dis. 2020, jiaa189. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J. Covid-19: How coronavirus will change the face of general practice forever. BMJ 2020, 368, m1279. [Google Scholar] [CrossRef] [PubMed]
- Garattini, L.; Padula, A. English and Italian national health services: Time for more patient-centered primary care? Eur. J. Intern. Med. 2018, 57, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Modelli di Gestione Territoriale da Parte del MMG di Casi Sospetti o Accertati di COVID-19 (Models for the Management of Suspected and Confirmed COVID-19 Cases in the General Practice). Available online: http://www.fimmg.org/index.php?action=pages&m=view&p=30845&lang=it (accessed on 9 May 2020).
- Guida Pratica per i Medici di Medicina Generale con una Sintesi di Buone Norme di Comportamento Basate Sulle Conoscenze ed Esperienze Pratico-Cliniche per la Gestione del COVID-19 (Summary of Good Practices Based on Current Knowledge and Clinical Experiences for the Management of COVID-19: A Practical Guide for General Practitioners). Available online: https://www.simg.it/Coronavirus/Covid_Gestionepaziente-SIMG_1.5.pdf (accessed on 9 May 2020).
- Disposizioni Urgenti per il Potenziamento del Servizio Sanitario Nazionale in Relazione All’Emergenza COVID-19 (Urgent Measures for the Strengthening of the National Health Service in Relation to the COVID-19 Emergency). Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/09/20G00030/sg (accessed on 9 May 2020).
- Rapporto ISS COVID-19 n. 12/2020—Indicazioni ad Interim per Servizi Assistenziali di Telemedicina Durante L’Emergenza Sanitaria COVID-19 (Italian National Institute of Health (ISS), COVID-19 Report n. 12/2020—Interim Indications for Telemedicine Assistance Services during the COVID-19 Health Emergency). Available online: https://www.iss.it/documents/20126/0/Rapporto+ISS+COVID-19+n.+12_2020+telemedicina.pdf/387420ca-0b5d-ab65-b60d-9fa426d2b2c7?t=1587107170414 (accessed on 9 May 2020).


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modenese, A.; Gobba, F. Increased Risk of COVID-19-Related Deaths among General Practitioners in Italy. Healthcare 2020, 8, 155. https://doi.org/10.3390/healthcare8020155
Modenese A, Gobba F. Increased Risk of COVID-19-Related Deaths among General Practitioners in Italy. Healthcare. 2020; 8(2):155. https://doi.org/10.3390/healthcare8020155
Chicago/Turabian StyleModenese, Alberto, and Fabriziomaria Gobba. 2020. "Increased Risk of COVID-19-Related Deaths among General Practitioners in Italy" Healthcare 8, no. 2: 155. https://doi.org/10.3390/healthcare8020155
APA StyleModenese, A., & Gobba, F. (2020). Increased Risk of COVID-19-Related Deaths among General Practitioners in Italy. Healthcare, 8(2), 155. https://doi.org/10.3390/healthcare8020155