Community Empowerment and Community Partnerships in Nursing Decision-Making



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Community Empowerment and Community Health Nursing
3. Community Partnerships and Community Empowerment
4. Discussion and Conclusions
Funding
Conflicts of Interest
References
- República Portuguesa. Competências do Enfermeiro Especialista em Enfermagem Comunitária. Regulamento Nº 428. Diário da República nº135 Série II de 16 de Julho. Ordem dos Enfermeiros; 2018. Available online: https://dre.pt/web/guest/pesquisa/-/search/115698616/details/normal?l=1 (accessed on 19 February 2019).
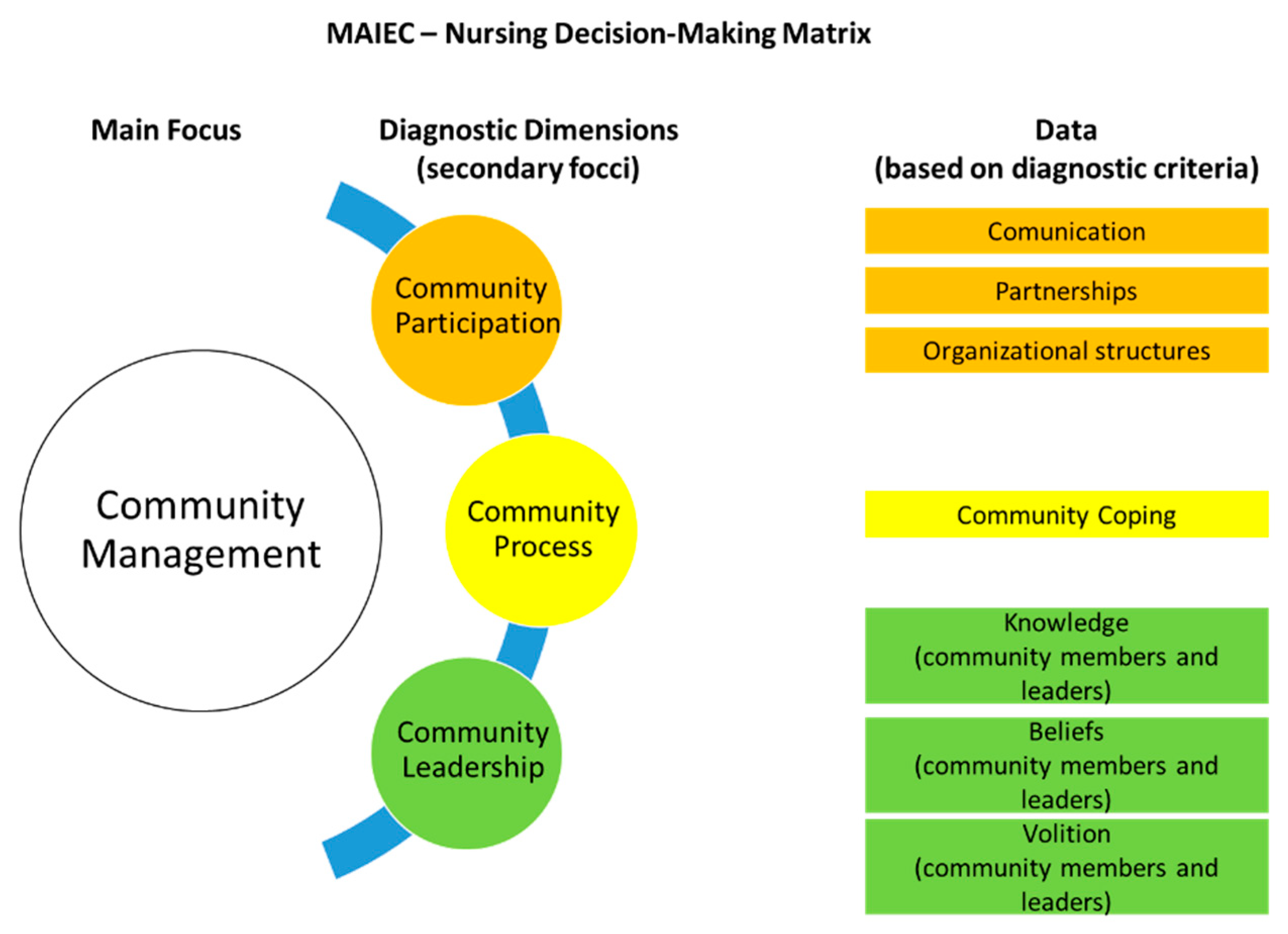
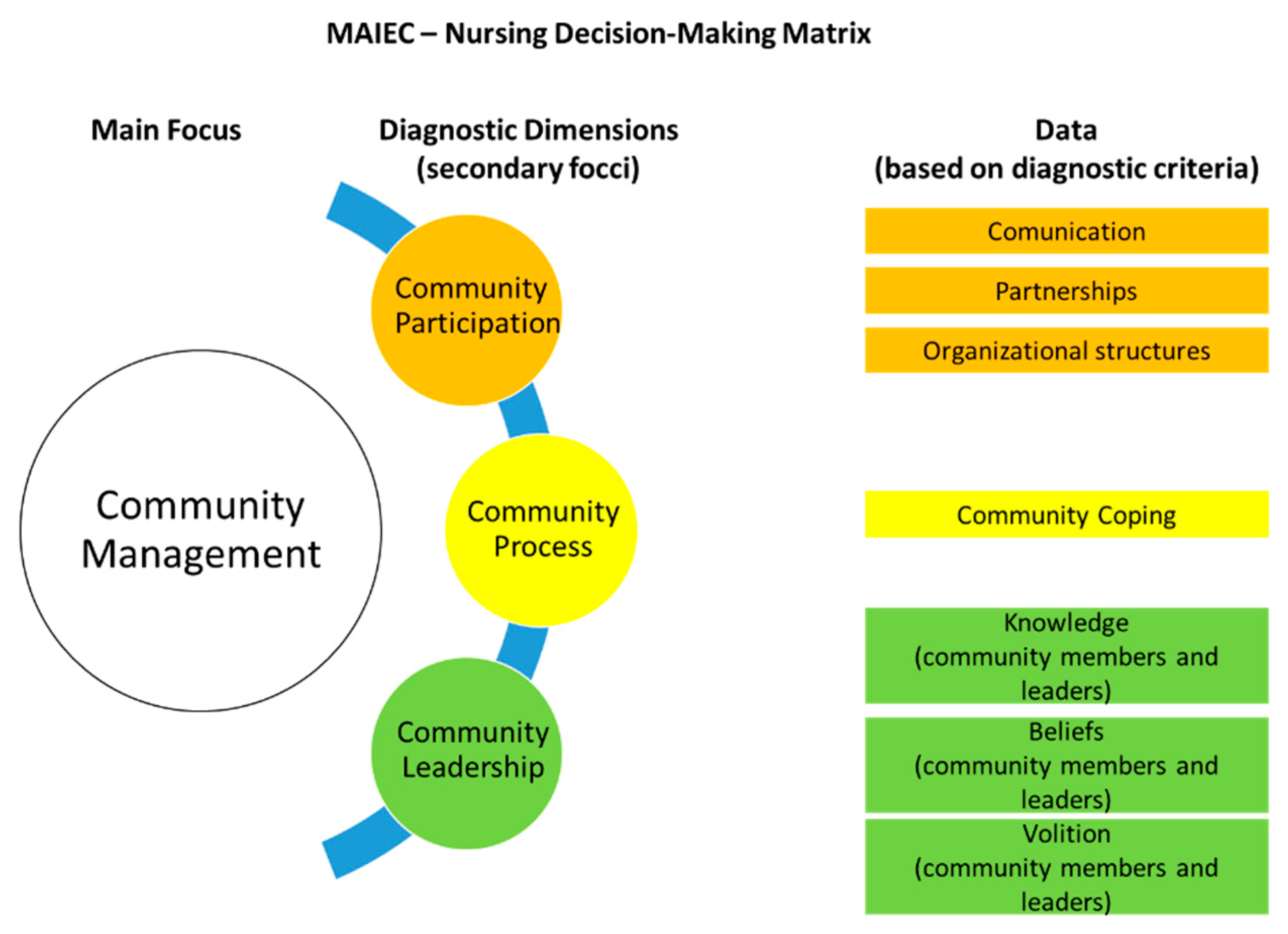
- Melo, P.; Silva, R.; Figueiredo, M.H. Attention foci in community health nursing and community empowerment: A qualitative study. Rev. Enferm. Ref. 2018, 19, 81–90. [Google Scholar] [CrossRef]
- Melo, P. Enfermagem Comunitária Avançada: Um Modelo de Empoderamento Comunitário. Ph.D. Thesis, Universidade Católica Portuguesa, Porto, Portugal, 16 November 2016. [Google Scholar]
- Melo, P. (Ed.) MAIEC-Manual do Utilizador; Porto, Portugal, 2017; Available online: https://issuu.com/pedro.a.melo/docs/maiec-manual_do_utilizador (accessed on 19 February 2019).
- Standing, M. Clinical Judgement and Decision-Making for Nursing Students, 2nd ed.; Sage: London, UK, 2014. [Google Scholar]
- Figueiredo, M.H. Modelo Dinâmico de Avaliação e Intervenção Familiar- uma Abordagem Colaborativa em Enfermagem de Família; Lusodidata: Loures, Portugal, 2012. [Google Scholar]
- Ordem dos Enfermeiros. Classificação Internacional para a Prática de Enfermagem (CIPE) 2015-Edição Portuguesa; Lusodidata: Loures, Portugal, 2015. [Google Scholar]
- Rappaport, J. In praise of paradox: A social policy of empowerment over prevention. Am. J. Community Psychol. 1981, 9, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Checkoway, B.; Schulz, A.; Zimmerman, M. Health education and community empowerment: Conceptualizing and measuring perceptions of individual, organizational and community control. Health Educ. Q. 1994, 21, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Gibbon, M.; Labonté, R.; Laverack, G. Evaluating community capacity. Health Soc. Care Community 2002, 10, 485–491. [Google Scholar] [CrossRef] [PubMed]
- De Vos, P.; De Ceukelaire, W.; Malaise, G.; Pérez, D.; Lefèvre, P.; Van der Stuyft, P. Health through people’s empowerment: A rights-based approach to participation. Health Hum. Rights 2009, 11, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Kasmel, A.; Andersen, P.T. Measurement of community empowerment in three community programs in Rapla (Estonia). Int. J. Environ. Res. Public Health 2011, 8, 799–817. [Google Scholar] [CrossRef] [PubMed]
- Laverack, G. Using a ‘domains’ approach to build community empowerment. Community Dev. J. 2005, 41, 4–12. [Google Scholar] [CrossRef]
- Laverack, G. Health Promotion Practice: Power and Empowerment; Sage: London, UK, 2004. [Google Scholar]
- Falk Rafael, A. Speaking Truth to Power Nursing’s Legacy and Moral Imperative. Adv. Nurs. Sci. 2005, 28, 212–223. [Google Scholar] [CrossRef]
- Velásquez, V.F.G.; Barreto, Y.L.L. Empoderamiento de líderes comunitarias afrocolombianas desde la Atención Primaria de Salud. Avances en Enferm. 2017, 35, 133–147. [Google Scholar] [CrossRef]
- Population Health Interest Group. Public Health Nursing in Ireland: Demonstrating Interventions from Practice; Institute of Community Health Nursing: Dublin, Ireland, 2013. [Google Scholar]
- Tomey, A.M.; Alligood, M.R. Teóricas de Enfermagem e a Sua Obra: Modelos e Teorias de Enfermagem, 5th ed.; Lusociência: Loures, Portugal, 2004. [Google Scholar]
- Molina, M.A.; Gorman, D.M. The Perth Amboy Community Partnership for Youth: Assessing its effects at the environmental and individual levels of analysis. Q. Community Health Educ. 1995, 15, 363–378. [Google Scholar] [CrossRef]
- Zakus, J.D.L.; Lysack, C.L. Revisiting community participation. Health Policy Plan. 1998, 13, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, A.; Pradhan, B. Community participation in health: A brief review and the experience of Kathmandu Medical College with the Duwakot community. Kathmandu Univ. Med. J. 2008, 6, 526–532. [Google Scholar] [CrossRef]
- McNeish, R.; Rigg, K.K.; Tran, Q.; Hodges, S. Community-based behavioral health interventions: Developing strong community partnerships. Eval. Program. Plan. 2019, 73, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Franza, B.; Skinnera, D.; Kerrb, A.M.; Penfoldc, R.; Kelleherd, K. Hospital–Community Partnerships: Facilitating Communication for Population Health on Columbus’ South Side. Health Commun. 2018, 33, 1462–1474. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.M.; Yazel Smith, L.; Haberlin, K.M.; Hannon, T.S. Feasibility of Implementing Community Partnerships to Provide Diabetes Prevention Services to Youth. J. Community Health 2019, 44, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Teufel Shone, N.I.; Schwartz, A.L.; Hardy, L.J.; de Heer, H.D.; Williamson, H.J.; Dunn, D.J.; Polingyumptewa, K.; Chief, C. Supporting New Community-Based Participatory Research Partnerships. Int. J. Environ. Res. Public Health 2019, 16, 44. [Google Scholar] [CrossRef] [PubMed]
- Alves, O.; Santos, P.C.; Fernandes, L.; Moreira, P. Barriers, obstacle, difficulties or challenges in development of health partnerships in community intervention projects: A systematic review. BMC Health Serv. Res. 2018, 18, 165. [Google Scholar]
- Center for Community Health and Development. “Toolkits 1: Creating and Maintaining Partnerships”. Community Tool Box University of Kansas. 2017. Available online: https://ctb.ku.edu/en/creating-and-maintaining-partnerships (accessed on 3 March 2019).
- Habana Hafner, S.; Redd, H.B. Partnerships for Community Development: Resources for Practitioners and Trainers; University of Massachusetts Center for Organizational and Community Development: Amherst, MA, USA, 1989. [Google Scholar]
- Lester, H.; Birchwood, M.; Tait, L.; Shah, S.; England, E.; Smith, J. Barriers and facilitators to partnership working between Early Intervention Services and the voluntary and community sector. Health Soc. Care Community 2008, 16, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Butterfoss, F.D. Coalitions and Partnerships in Community Health; Jossey-Bass: San Francisco, CA, USA, 2007. [Google Scholar]
- Ornelas, J.; Vargas Moniz, M. Parcerias Comunitárias (Community Coalitions); ISPA-IU Coleção Livros Técnicos: Lisboa, Portugal, 2011. [Google Scholar]
- Butterfoss, F.D.; Goodman, R.M.; Wandersman, A. Community coalitions for prevention and health promotion. Health Educ. Res. 1993, 8, 315–330. [Google Scholar] [CrossRef]
- Fawcett, S.B.; Paine Andrews, A.; Francisco, V.T.; Schultz, J.A.; Richter, K.P.; Lewis, R.K.; Williams, E.L.; Harris, K.J.; Berkley, J.Y.; Fisher, J.L.; et al. Using empowerment theory in collaborative partnerships for community health and development. Am. J. Community Psychol. 1995, 23, 677–697. [Google Scholar] [CrossRef]
- Butterfoss, F.D.; Goodman, R.M.; Wandersman, A. Community coalitions for prevention and health promotion: Factors predicting satisfaction, participation, and planning. Health Educ. Q. 1996, 23, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, S.B.; Lewis, R.K.; Paine Andrews, A.; Francisco, V.T.; Richter, K.P.; Williams, E.L.; Copple, B. Evaluating community coalitions for prevention of substance abuse: The case of Project Freedom. Health Educ. Behav. 1997, 24, 812–828. [Google Scholar] [CrossRef] [PubMed]
- National Network for Collaboration. Collaboration Framework, Addressing Community Capacity Fargo, ND: National Network for Collaboration. 1996. Available online: http://www.uvm.edu/crs/nnco/collab/framework.html (accessed on 14 March 2018).
- WHO. Health Promotion. Track 1: Community Empowerment. 7th Global Conference on Health Promotion: Track Themes: World Health Organization. 2018. Available online: http://www.who.int/healthpromotion/conferences/7gchp/track1/en/ (accessed on 17 January 2018).
- Onyenemezu, C.E. The imperative of citizen’s participation in community development. Acad. Res. Int. 2014, 5, 209–215. [Google Scholar]
- Paul, S. Community Participation in Urban renewal and rehabilitation: Comments on Theory and Practices. Community Dev. J. 1987, 16, 105–117. [Google Scholar]
- Williams, M.; Chandra, A.; Spears, A.; Varda, D.; Wells, K.; Plough, A.; Eisenman, D. Evaluating Community Partnerships Addressing Community Resilience in Los Angeles, California. Int. J. Environ. Res. Public Health 2018, 15, 610. [Google Scholar] [CrossRef] [PubMed]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melo, P.; Alves, O. Community Empowerment and Community Partnerships in Nursing Decision-Making. Healthcare 2019, 7, 76. https://doi.org/10.3390/healthcare7020076
Melo P, Alves O. Community Empowerment and Community Partnerships in Nursing Decision-Making. Healthcare. 2019; 7(2):76. https://doi.org/10.3390/healthcare7020076
Chicago/Turabian StyleMelo, Pedro, and Odete Alves. 2019. "Community Empowerment and Community Partnerships in Nursing Decision-Making" Healthcare 7, no. 2: 76. https://doi.org/10.3390/healthcare7020076
APA StyleMelo, P., & Alves, O. (2019). Community Empowerment and Community Partnerships in Nursing Decision-Making. Healthcare, 7(2), 76. https://doi.org/10.3390/healthcare7020076