Abstract
Background: Diabetes mellitus is a complex chronic condition requiring continuous healthcare. Consequently, various organisations recommend therapeutic education to enhance treatment adherence. This is often facilitated by Advanced Practice Nurses, who provide a range of advanced interventions that impact clinical health outcomes and deliver healthcare services to these patients. Objective: To analyse the effectiveness of interventions performed by Advanced Practice Nurses in patients with diabetes. Method: A peer-reviewed systematic review was conducted and registered in PROSPERO. The databases consulted included PubMed, Scopus, Web of Science, and CINAHL. Inclusion criteria comprised studies published between 2014 and 2024 on the effectiveness of interventions by Advanced Practice Nurses in diabetic patients. The review included qualitative, quantitative, and mixed methods designs. Various screenings were carried out, including the assessment of methodological quality. Results: A total of 600 studies were identified, of which 17 were selected for final review. Among these, 12 studies focused on diabetic education. Interventions were predominantly delivered in person in primary care settings, private clinics, and hospitals. Reported outcomes included reductions in HbA1c levels, improved patient self-knowledge and self-efficacy, and decreased rates of readmission and mortality. Conclusions: The sample consisted predominantly of women over 60 years of age. Diabetic education emerged as the most common intervention, primarily delivered in person by Advanced Practice Nurses across diverse settings. Nearly all interventions proved effective in improving health outcomes for diabetic patients.
1. Introduction
Throughout time, Nursing has progressively evolved in the entire world, with the emergence of the Advanced Practice Nurse (APN) figure, which was defined by the International Nursing Council as a nurse who, through additional training, has acquired expert knowledge, complex decision-making skills, and clinical competences to expand their practice. All this exerts a direct influence on clinical health outcomes and on the provision of direct services to individuals, families, and communities. The characteristics of an APN can vary according to the context of the country where they develop their activities, as variations can be noticed in health systems, in the regulatory mechanisms for this figure, and in nursing training systems [1].
It is to be taken into account that the figure of APN was born in the United States at the beginning of the 20th century in the form of two roles: Clinical Nurse Specialists (CNSs) and Nurse Practitioners (NPs). Clinical Nurse Specialists usually concentrate in more indirect care, more linked to non-clinical activities such as supporting the system, education, leadership, and research, from a systemic approach more connected to in-hospital environments [1,2,3]. Nurse Practitioners concentrate more on direct care, more on clinical activities such as diagnosis, treatment, and prescriptions for the patients in different clinical environments; they are more autonomous professionals and are linked to Primary Health Care [1,2,4,5]. Nevertheless, there are other terms identified with APNs, such as expert nurses, midwifery nurses, nurse anaesthetists, outpatient care nurses, emergency nurses, and liaison nurses or case-management nurses, among others [5,6,7,8].
Following the United States, the figure of the APN was developed in Canada and in other countries such as the United Kingdom, Australia, New Zealand, Netherlands, Sweden, and Ireland. It did not reach Spain until the beginning of the 21st century, when there was a change in the organizational models to adapt health services to the population’s needs. This change was implemented in the form of different figures across different health services, mostly as Case-Management Nurse [9,10]. In fact, in Spain, this figure poses a major political, legislative, and educational challenge, with the mandatory requirement to devise laws that regulate it, define its profile, and regulate its process and integration into the Spanish health system, as well as to develop ruled university teaching strategies that favour sound development of clinical skills, knowledge, and vision to perform its duties [2].
With its varied denominations, the APN is an important figure in terms of support for generalist nurses due to the difficulties they face in their everyday practice, as the patients’ conditions are increasingly complex and demanding, which requires high care quality standards [9]. It is of utmost importance to highlight that the care provided to chronic patients constitutes one of the main challenges for most health systems [10].
In some cases, living with chronic disease can turn out to be difficult, even more so when the required and self-administered treatment and control are complex. In fact, therapeutic non-adherence is one of the main problems for chronicity care to be effective. In this regard, the APN plays a fundamental role in improving this care [11].
Several organizations speak about incorporating an APN profile for the diabetes approach, in order to promote complex case resolution and active education in the patients [11,12]. Diabetes Mellitus (DM) is a complex chronic disease that affects people of all ages and social statuses and requires continuing health care in charge of a multidisciplinary team, with multi-factorial strategies for risk reduction beyond glycaemic control. Various international consensuses recommend resorting to therapeutic education in DM by means of team comprising expert professionals with guaranteed knowledge; this is crucial for achieving good results in the patients, as it will help promote quality of life improvements, better treatment adherence, and reductions in the number of complications [11].
Based on the above, the objective proposed is to analyse the effectiveness of interventions carried out by Advanced Practice Nurses in patients with diabetes.
2. Materials and Methods
2.1. Study Design
A peer systematic review was carried out, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the Cochrane manual for intervention systematic reviews, which ensure the conduction of complete and rigorous reviews [13,14]. The study protocol was registered in PROSPERO (CRD42023407829) before selection and data extraction.
2.2. Search Strategies and Selection Criteria
The following databases were consulted to identify relevant studies: PubMed, Web of Science, Scopus, and CINAHL. Two reviewers conducted the searches independently from the keywords identified on the theme. The search strategy was: (“Nurse Practitioner” OR “Clinical Nurse Specialist” OR “APN” OR “Advanced Practice Nursing” OR “Practice Patterns, Nurses’”) AND “Diabetes Mellitus” NOT “Review”.
The study selection criteria were as follows: (1) published studies on the effectiveness of advanced practice nurse interventions in patients with diabetes; (2) studies employing qualitative, quantitative, and mixed methods designs published between 2014 and 2024. The studies (including protocols and projects) in which outcomes of interest were neither measured nor reported were not eligible.
2.3. Data Analysis and Assessment of Article Quality
Two reviewers selected the studies independently according to their titles and abstracts and, subsequently, as per the pre-established eligibility criteria. All disagreements regarding study selection were resolved by consensus with a third author. Subsequently, two reviewers separately extracted the data from the selected articles, and all authors participated in the discussion and synthesis of the results. A registration form was designed following the indications set forth in the Cochrane Manual [14], detailing (a) authorship and year; (b) study design, period, and country; (c) the ages and sexes of participants, as well as whether they belonged to a control group (CG) or an intervention group (IG), if specified in the study design. Additionally, the outcomes measured in each study, the instruments used for measurement (where applicable), the interventions performed by the APN, and their effectiveness were recorded.
The methodological quality of the included studies was assessed by the two independent reviewers using the following instruments (in case of disagreement, a third author was consulted):
- In qualitative studies, those scoring below 50% on the Standards for Reporting Qualitative Research (SRQR) were excluded. This instrument consists of 21 items divided into five dimensions, providing a framework and recommendations for reporting this type of research. The following categorization, based on the percentage of items meeting the evaluation criteria, was applied: Excellent (80–100%), Good (50–80%), Fair (30–50%), and Poor (<30%) [15];
- In observational studies, those scoring below 12 on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist were excluded. This instrument consists of 22 items, with a maximum possible score of 22. Studies with scores <12 were deemed to be of insufficient quality [16];
- In Randomised Controlled Trials (RCTs), studies scoring below 4 on the Physiotherapy Evidence Database (PEDro) scale were excluded. This instrument comprises 11 items, each with a binary response (“Yes” or “No”), where each affirmative response scores 1 point. The maximum score is 10, as the first item is not considered due to its relevance to the external validity of the studies. The methodological quality was categorized as follows: Excellent (9–10 points), Good (8–6 points), Acceptable (5–4 points), and Poor (<4 points). Studies scoring below 4 were of insufficient quality [17,18,19];
- In mixed-method studies, those scoring below 4 on the Good Reporting of a Mixed Methods Study (GRAMMS) scale were excluded. This instrument consists of six items, with a maximum possible score of 6. Studies scoring <4 were classified as being of insufficient quality [16,20];
- In quasi-experimental studies, those scoring below 12 on the Transparent Reporting of Evaluations with Nonrandomised Designs (TREND) checklist were excluded. This instrument comprises 22 items grouped into five domains: title and abstract, introduction, methodology, results, and discussion [21,22]. The same scoring criteria as the STROBE checklist were applied, given the identical number of items and the lack of evidence for a specific cut-off score. Accordingly, studies with scores <12 were of insufficient quality.
2.4. Risk of Bias Analysis
The Cochrane Risk of Bias (ROB-2) tool (V.2) was employed to assess the risk of bias in RCTs [23,24,25], while the JBI critical appraisal tool was utilised for quasi-experimental studies [26,27].
3. Results
3.1. Presentation of the Studies
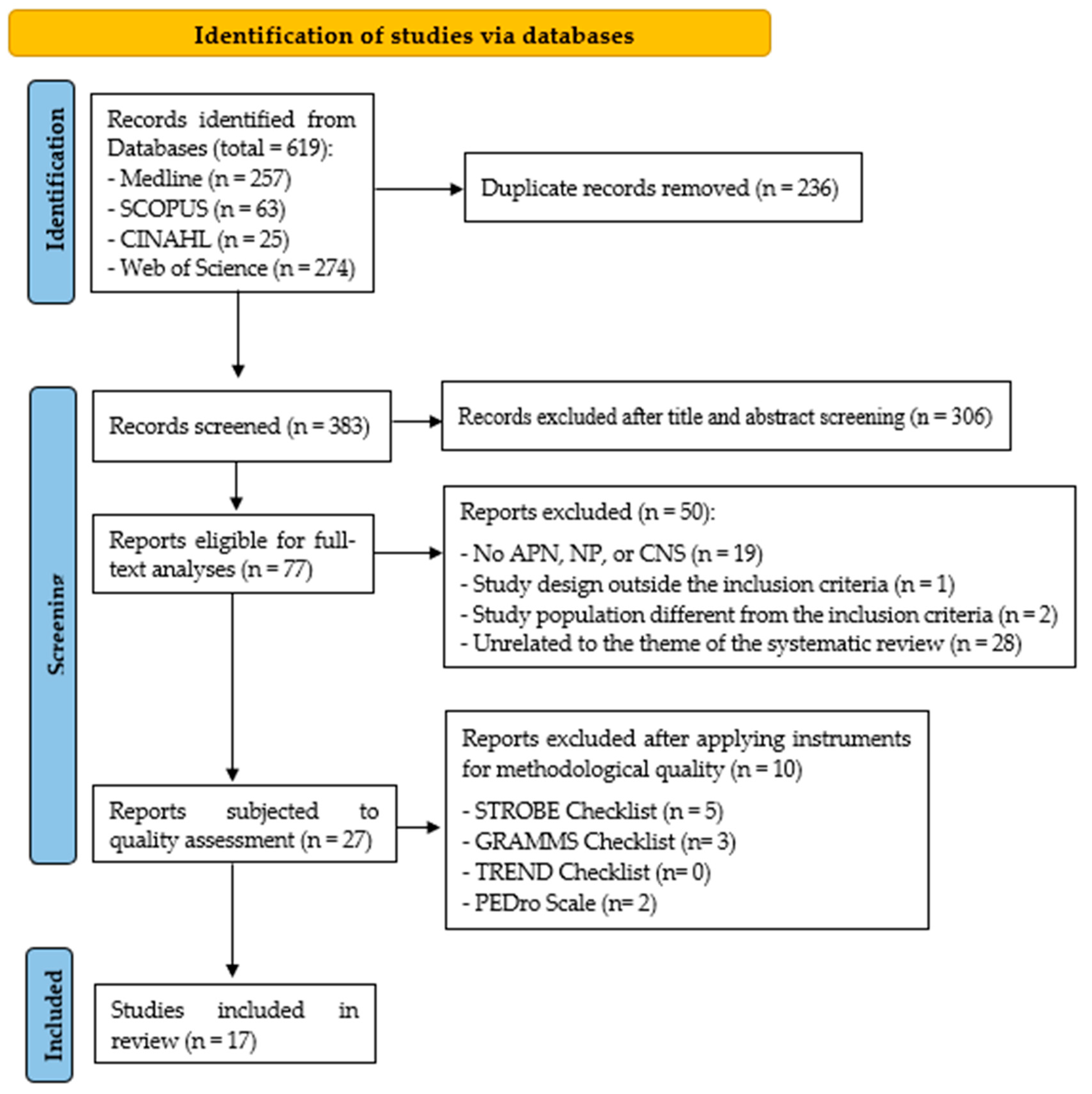
A total of seventeen studies met the inclusion criteria and were included (Figure 1). The characteristics of the studies are presented in Table S1.
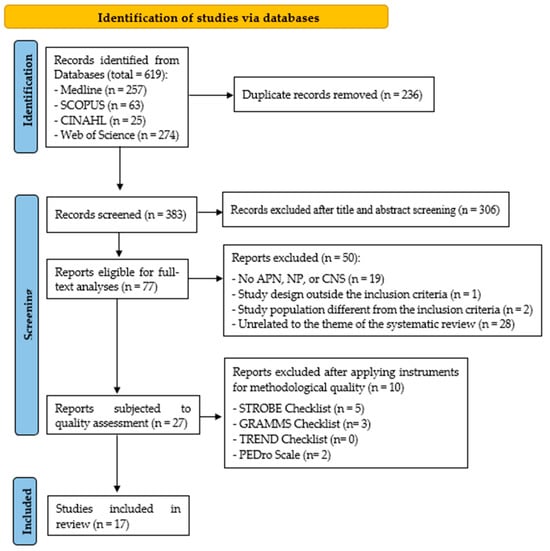
Figure 1.
PRISMA flow diagram of study.
3.2. Quality Assessment and Risk of Bias
Table S2 presents the results obtained in the third screening, following the application of various tools to assess the methodological quality of the 28 studies selected after the second screening. At the end of the third screening, 17 studies were finally selected, as depicted in the flow chart.
3.3. Thematic Analysis
3.3.1. Characteristics of the Diabetic Patients Subjected to APN Interventions
Table 1 shows the different characteristics of the sample comprising diabetic patients subjected to APN interventions. The samples of the studies consisted both of women and of men [28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43]. In 50% of them, there was a higher percentage of women in the sample [28,29,31,33,34,36,39,41]; 43.75% had a higher percentage of men [32,35,37,38,40,42,43]; and the percentage of men and women was the same in 6.25% [30]. In relation to gender, one study made no reference to this aspect [44].

Table 1.
Characteristics of the samples of diabetic patients with intervention by the APN.
As for the diabetic patients’ age, the overall mean found in the studies was 64.5 years old. It is to be noted that 23.53% of the studies had samples comprising people aged between 30 and 50 years old [28,30,34,44], whereas 76.5% included participants aged at least 60 years old [29,31,32,33,35,36,37,38,39,40,41,42,43].
Regarding the DM diagnosis in the samples from the studies, 35.3% of the patients had Type 2 DM (DM2) [32,33,36,39,40,42]. One study differentiated its sample between Type 1 DM (DM1) and DM2 [44]. Another one made a distinction between the patients with DM2 and those without [37]. Nevertheless, the type of diabetes presented by the patients was not specified in 41.18% [29,31,34,35,38,41,43]. In addition, the patients had DM (without specifying its type) along with other chronic diseases in two studies [28,30].
3.3.2. APN Interventions in Diabetic Patients and Their Effectiveness
Table 2 presents the variables and/or instruments used in the studies, as well as the APN interventions carried out and their effectiveness.
Table 2.
Variables and/or instruments, interventions carried out by APNs, and their effectiveness.
As for the interventions, 70.59% of the studies focused on diabetic education [28,29,32,33,34,35,36,37,38,39,43,44]. In 35.29% of them, the interventions were targeted at lifestyle changes, treatment adherence, prevention of complications, and drug prescription [28,33,36,37,39,43]. Diabetic education was implemented in combination with insulin therapy training in two studies [29,32]. Finally, in other cases, diabetic education was combined with telemonitoring support [38] or with insulin self-injection simulations, in turn promoting fewer fears, concerns, and myths [34]. One study combined education with support and motivation-improving measures [35]. Another one included supervision by means of a device called the Abbott FreeStyle Precision Pro and changing the treatment [44]. Two studies make reference to the need to train, supervise, and work as a team with other professionals when it comes to implementing and promoting interventions carried out by APNs [40,41].
Resuming the topic of the interventions themselves, the following findings were observed as for their in-person or remote modality: (1) exclusive in-person modality in 76.47% of the studies [28,29,30,31,32,34,35,36,37,39,40,42,44]; (2) exclusive remote modality in two cases, via videoconferences [43] or phone calls [33]; (3) in-person/remote combined modality in another two studies [38,41]. In the cases with in-person modality, they were carried out in hospital centres in six studies [29,32,35,37,40,44], in Primary Health Care centres in five cases [28,30,34,36,42], and in two in private clinics [31,39].
In relation to the professional figure that was in charge of the interventions, they were carried out independently by APNs in 64.7% of the cases [30,31,32,34,36,37,38,39,42,43,44]; in the other cases (35.3%), the interventions were jointly implemented by an APN along with other health professionals such as physicians, endocrinologists, educators specialized in diabetes, or community health workers [28,29,33,35,40,41].
As for the effectiveness of the APN interventions in diabetic patients, we should make it clear that they were focused on clinical results (HbA1c, LDL, or BP) in 76.47% of the studies [28,29,30,32,33,34,35,36,37,38,39,40,42]. Two of them were RCTs, which allowed comparing the IG results against those obtained in the CG [28,33], finding significant improvements in the IG clinical outcomes in only one of the studies [28]. In the case of the observational studies [29,30,35,36,40,42], it was possible to reduce the patients’ HbA1c levels at the end of the intervention; however, in two studies [29,36], the results were only attained when the intervention was carried out by an APN against the one implemented by another professional. This reduction in the HbA1c levels after the intervention was also described in the quasi-experimental studies [32,34,38,39,41].
In 41.18% of the studies, the interventions were focused on the self-knowledge and self-efficacy attained by the patients after the APN intervention [30,31,34,38,39,41,43]. The patients’ self-knowledge and self-efficacy in managing their pathology were improved in all of them at the end of the intervention, which helped improve treatment adherence and self-care, thus increasing empowerment in diabetes management [30,34,38,39,41,43]. In one of these studies, it is also stated that it is fundamental to establish an adequate patient–APN relationship, as it helps improve the clinical outcomes and reduce the emotional distress sometimes related to diabetes [38]. Despite these findings, a reduction in treatment adherence between the patients cared for by an APN and those served by another professional was observed in another of the studies selected. Nevertheless, the patients cared for by an APN presented fewer comorbidities, complications, and hospitalizations when compared to those served by another professional [31].
In 29.41% of the cases, the hospital admission and mortality rates stood out among their variables, in addition to hospitalization time or costs [28,31,32,37,44]. Two of these studies reported that an intervention led by an APN reduced hospital readmission rates among the treated patients [32,44]. It was also possible to reduce the mortality rate and mean hospitalization time among the patients at the end of the intervention in two of the studies selected [37,44]. Three studies addressed the costs [28,31,37]. In this sense, one of these studies stated that the cost of an intervention in charge of an APN was similar to that of one carried out by another professional [31]. However, another study indicated that the intervention carried by the APN had a higher cost when compared to the other control intervention [28].
3.3.3. Improvement Strategies in Relation to APNs
Improvement strategies were described in 12 studies [28,29,30,31,32,34,36,39,41,42,43,44]; they are presented in Table 3.
Table 3.
Improvement strategies in relation to APNs.
4. Discussion
4.1. Characteristics of the Diabetic Patients Subjected to APN Interventions
In the studies selected, some differences regarding the characteristics of the samples can be noticed. In relation to the diabetic patients’ age, the samples in most of the studies presented mean ages over 60 years old [29,31,32,33,35,36,37,38,39,40,41,42,44]. This finding is in line with other authors, whose studies show mean ages that are similar to the ones described by the studies included in the current review [45,46]. It is to be noted that DM2 is linked to aging in many cases, with its prevalence increasing with age, which can intensify many of the geriatric symptoms [47,48].
As for gender, most the studies had a predominance of women in their samples [28,29,31,33,34,36,39,41]. Various authors have incorporated higher percentages of women in their samples [46]. Nevertheless, other studies with samples comprising the same number of men and women have been conducted [45]. It is also important to consider that diabetes affects each gender in a different way, both in terms of its clinical repercussion and of its impact [49,50]. It is for this reason that it is important to consider the existing biases in health care between men and women, as many of the current social determinants cause late diabetes recognition and delays in care and treatment initiation among women, which leads to deficient control of the pathology [49].
4.2. APN Interventions in Diabetic Patients and Their Effectiveness
Various studies have highlighted the challenges that may arise in diabetes management, such as recurrent hypoglycaemia or persistent hyperglycaemia. In this regard, APN-led interventions focused on diabetes education are key to improving diabetes management and preventing complications. In fact, it was the intervention most commonly led by APNs and cited in the majority of the reviewed studies [28,29,32,33,34,35,36,37,38,39,43,44]. Various studies have also incorporated this intervention, both to enhance patients’ knowledge and self-efficacy [51] and to improve their biochemical parameters [52]. Other authors support this intervention by promoting the inclusion of complementary group dynamics that improve the interaction among individuals with the same pathology. This, in turn, fosters experience sharing, clarifies doubts, facilitates the acquisition of new knowledge, and reduces the impact of the pathology on a person’s quality of life [53].
Another of the interventions proposed is especially linked to working as a multidisciplinary team, where APNs should foster their training and supervision [40,41]. In fact, some authors stress the importance for APNs to work in an interdisciplinary way, following structured coordination of the care provided in order to improve and ensure the patients’ quality of life [54]. This aspect is also crucial to improve comprehensive care [31,55].
As for the modality of the interventions (in-person, remote, or mixed), it was in-person in most of the studies selected [28,29,30,31,32,34,35,36,37,39,40,42,44]. This coincides with various studies already conducted on the theme [39,45,52,56]. Other studies included the remote modality by resorting to videoconferences or phone calls. Some authors have put forward the suitability of incorporating interventions through mobile apps or other remote devices [57]. The mixed modality has also been described in studies from the current review [38,41], which finds a number of authors who mention the usefulness of incorporating the in-person modality of intervention along with remote ones, such as phone calls [57].
In relation to the professional figure that was in charge of the interventions, they were carried out independently by APNs in most of the studies [30,31,32,34,36,37,38,39,42,43,44], as already described in other studies alien to this review [45,55]. In other studies included, the APNs worked along with other professionals in implementing the interventions [28,29,33,35,40,41]. These findings are in line with other authors who stress interdisciplinary work coordinated with other professionals to improve the care provided and ensure patient care quality [54].
Regarding the effectiveness of interventions led by APNs, it should be considered that nearly all studies have designed their interventions to subsequently analyse changes in patients’ clinical outcomes, especially those focused on the HbA1c levels. In general, it was possible to reduce these levels in almost all the studies [28,29,30,32,34,35,36,38,39,40,41,42], approaching the recommended values. This coincides with the postulates set forth by various authors who, when developing APN therapeutic education programs with patients on insulin, observed a reduction in the HbA1c levels [45].
Another of the aspects assessed in the studies selected was determining how the interventions influenced the self-knowledge and self-efficacy levels attained by the patients. In this case, they were improved and increased in a large part of the studies [30,34,38,39,41,43]. This is consistent with other authors, who indicate that these aspects also lead to an improvement in treatment adherence and, in many cases, to insulin injections, if necessary [45].
The readmission rates, hospitalisation time, mortality rate, and costs were equally addressed in some of the studies selected, showing reductions in general [28,31,32,37,44]. In this sense, other authors have stated how APN interventions in a hospital emergency service have allowed reducing the readmission rates, as well as the patients’ hospitalisation times [55]. In the study conducted by Ordoñez-Piedra et al. [58], it was possible to reduce the readmission and mortality rates, as well as the costs. In relation to the costs, various authors indicate that coordination between APNs and case-management nurses not only improves the care provided to the patients and eases their access to these health services but also helps reduces the economic impact on the consumption of hospital supplies and the costs associated with non-efficiencies. APNs manage to reduce healthcare costs by being well prepared to address the challenges of care focused on health promotion and prevention actions, while also standardising health education [59]. Regarding cost-effectiveness, some authors indicate that APNs are generally cost-efficient providers. However, as their role, scope of practice, and payment mechanisms vary by country, further research with clearly defined cost measures is needed to better understand the potential of APNs to reduce the high cost of healthcare services [60].
4.3. Improvement Strategies in Relation to APNs
Some of the studies selected indicate the need to increase the number of APN professionals as an improvement strategy regarding the care provided to diabetic patients, as these professionals help improve the health outcomes [28,31,32,36]. This finding coincides with the postulates set forth by other authors, who highlight this professional figure because it has specialised knowledge and skills that help provide effective and good quality care [61]. To increase the number of APNs and achieve greater integration in diabetes management, it is necessary to convince key decision-makers of their value, promote educational programmes for their training, and improve regulatory frameworks and policies [62,63].
The following have also been described as improvement strategies: APNs incorporating innovative methods to improve the results, such as performing self-injection simulations, glucose continuous monitoring, or incorporating new technologies like videoconference sessions [30,34,42,43]. Various authors have also made reference to the suitability of introducing new methods, including resorting to telehealth options for health care, which helped improve diabetes self-control [64]. Nevertheless, when referring to telehealth as an alternative care method during the COVID-19 pandemic, worsened diabetes quality measures were observed in another study already carried out [65].
Another of the improvement strategies proposed in the studies was to foster diabetic education during hospitalisation, not limiting it exclusively to primary care services. This will foster better treatment adherence after the patients’ discharge [39,44]. In another study, it is described how the care provided by APNs during hospitalisation improved treatment adherence and increased the knowledge levels. This helped reduce the HbA1c levels, the hospitalization times, and the number of readmissions after discharge [66].
The following is also proposed among the improvement strategies: training and qualifying other professionals in diabetes management to support the specialised team and increase profitability [29,41]. This coincides with other authors alien to the review, who mention how training and qualification of other professionals by APNs (such as health support workers) helps reduce APNs’ workload and improve the results obtained [67].
4.4. Limitations
The present study has certain limitations, which are as follows: 1. Heterogeneity in the design and methodology of the selected studies. However, several authors consider this aspect a source of valuable information for research when conducted methodically [14]. 2. Regarding the quality and validity of the studies, it should be noted that the majority were either observational or quasi-experimental in design, which entails a higher risk of bias compared to the RCTs included in the review. In this regard, it should also be considered that for quasi-experimental studies, due to the lack of evidence to establish a cut-off point for distinguishing between good or poor quality, the same reference threshold was applied as for purely observational studies, using the STROBE checklist. 3. Restricting the search strategy to the last 10 years.
5. Conclusions
Regarding the characteristics of the sample, most of the studies included patients diagnosed with DM2, over the age of 60, and with a higher percentage of women.
As for the interventions carried out by APNs, significant diversity was observed in terms of intervention type, as well as in their number, length in time, modality, and the professional figure in charge of the sessions conducted. The intervention most frequently described was diabetic education, exclusively implemented by APNs in most of the cases, and in the in-person modality, both in primary care environments and in in-hospital ones. Referring to effectiveness, the most effective interventions are those focused on therapeutic education, in which APNs coordinate with the rest of the healthcare team and families. This requires a high level of training to address the challenges of diabetes management. The APN interventions were able to improve the clinical outcomes in general, especially those related to the HbA1c levels. Likewise, the patients’ self-knowledge and self-efficacy in diabetes management are improved, which favours treatment adherence and reducing possible future complications. In addition, it has been described how APN interventions in these patients helps reduce readmission and mortality rates, hospitalisation times, and costs.
In relation to the improvement strategies, it becomes necessary to increase the number of APNs in the different health scopes to enhance care quality and the patients’ quality of life. Likewise, promoting diabetic education (both in primary care and in in-hospital settings), fostering the introduction of new care methods, and encouraging training and qualification of other professionals in diabetes management as support for APNs.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/healthcare13070738/s1, Table S1: Study Characteristics; Table S2: Results obtained from assessing the methodological quality of the studies; Table S3: Results of applying the Cochrane Risk of Bias (ROB-2) tool for RCTs; Table S4: Results of using the JBI critical appraisal tool for quasi-experimental studies; Figure S1: Results of applying the Cochrane Risk of Bias (ROB-2) tool for RCTs.
Author Contributions
Conceptualization, M.D.G.-M. and A.R.-G.; methodology, M.D.G.-M., A.R.-G., Á.B.-R. and E.M.; formal analysis, M.D.G.-M., A.R.-G. and E.M.; investigation, M.D.G.-M., A.R.-G., Á.B.-R. and E.M.; data curation, M.D.G.-M., A.R.-G. and E.M.; writing—original draft preparation, M.D.G.-M. and Á.B.-R.; writing—review and editing, M.D.G.-M. and Á.B.-R.; supervision, M.D.G.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No additional data are available.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Consejo Internacional de Enfermería (CIE). Directrices de Enfermería de Práctica Avanzada. 2020. Available online: https://www.icn.ch/sites/default/files/2023-04/ICN_APN%20Report_ES_WEB.pdf (accessed on 7 February 2024).
- Canga-Armayor, N. La formación académica de las enfermeras que desarrollan roles de práctica avanzada. Enferm. Intensiva. 2024, 35, e41–e48. [Google Scholar] [CrossRef]
- Del Barrio-Linares, M. Competencias y perfil profesional de la enfermera de práctica avanzada. Enferm. Intensiv. 2014, 25, 52–57. [Google Scholar] [CrossRef]
- Palma, R.B. Enfermería de Práctica Avanzada: Situación Actual y Perspectiva a Futuro. 2019. Available online: https://docs.bvsalud.org/biblioref/2019/08/1008589/vea_47-49-54.pdf (accessed on 14 March 2024).
- Ramírez, P.; Hernández, O.; Sáenz De Ormijana, A.; Reguera, A.I.; Meneses, M.T. Enfermería de práctica avanzada: Historia y definición. Enfermería Clín. 2002, 12, 286–289. [Google Scholar]
- Giménez, A.M. La Enfermería y la Práctica Avanzada: Su Desarrollo en España. Ph.D. Thesis, Universidad Complutense de Madrid, Madrid, Spain, 2013. [Google Scholar]
- Miguélez-Chamorro, A.; Casado-Mora, M.I.; Company-Sancho, M.C.; Balboa-Blanco, E.; Font-Oliver, M.A.; Román-Medina, I.I. Enfermería de Práctica Avanzada y gestión de casos: Elementos imprescindibles en el nuevo modelo de atención a la cronicidad compleja en España. Enferm. Clin. 2019, 29, 99–106. [Google Scholar] [CrossRef]
- Sevilla, S.; Miranda, J.; Zabalegui, A. Profile of advanced nursing practice in Spain: A cross-sectional study: Advanced Practice Nursing in Spain. Nurs. Health Sci. 2018, 20, 99–106. [Google Scholar] [CrossRef]
- San Martín-Rodríguez, L. Práctica avanzada en Enfermería y nuevos modelos de organización sanitaria. Enferm. Clin. 2016, 26, 155–157. [Google Scholar] [CrossRef]
- Sánchez-Martín, C.I. Cronicidad y complejidad: Nuevos roles en Enfermería. Enfermeras de Práctica Avanzada y paciente crónico. Enferm. Clin. 2014, 24, 79–89. [Google Scholar] [CrossRef]
- Consejo General de Enfermería (CGE). Marco de Competencias de la Enfermera/o Experta en Cuidados y Educación Terapéutica de las Personas con Diabetes, Familiares o Cuidadores. Instituto Español de Investigación Enfermera y Consejo General de Enfermería de España. 2020. Available online: https://uesce.com/wp-content/uploads/2024/07/Marco-competencias-enfermeria-diabetes.pdf (accessed on 8 February 2024).
- Servicio Andaluz de Salud. Enfermera de Práctica Avanzada en la Atención de Personas con Tratamiento Complejos para Diabetes (EPA-TCD). Consejería de Salud de la Junta de Andalucía. 2018. Available online: https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/sites/default/files/sincfiles/wsas-media-mediafile_sasdocumento/2019/epa_diabetes_definitiva_1.pdf (accessed on 15 February 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Li, T.; Higgins, J.; Deeks, J.; Higgins, J.; Thomas, J.; Chnadler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane. 2021. Available online: https://training.cochrane.org/handbook (accessed on 4 February 2024).
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Lozano-Muñoz, N.; Borrallo-Riego, Á.; Guerra-Martín, M.D. Impact of social network use on anorexia and bulimia in female adolescents: A systematic review. An. Sist. Sanit. Navar. 2022, 45, e1009. [Google Scholar] [CrossRef]
- Foley, N.C.; Teasell, R.W.; Bhogal, S.K.; Speechley, M.R. Stroke Rehabilitation Evidence-Based Review: Methodology. Top. Stroke Rehabil. 2003, 10, 1–7. [Google Scholar] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; Sainz De Baranda, P. Calidad metodológica de los programas de estiramiento: Revisión sistemática. Rev. Int. Med. Cienc. Act. Física Deporte 2013, 13, 163–181. [Google Scholar]
- O’cathain, A.; Murphy, E.; Nicholl, J. The quality of mixed methods studies in health services research. J. Health Serv. Res. Policy 2008, 13, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Moraga, J.; Cartes-Velasquez, R. Pautas de chequeo, parte I: CONSORT y TREND. Rev. Chil. Cirugía 2015, 67, 225–232. [Google Scholar]
- Vallvé, C.; Artés, M.; Cobo, E. Estudios de intervención no aleatorizados (TREND). Med. Clin. 2005, 125, 38–42. [Google Scholar]
- Higgins, J.P.T.; Savoviç, J.; Page, M.J.; Sterne, J.A.C. Revised Cochrane Risk-of-Bias Tool for Randomized Trials (RoB-2). 2019. Available online: https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/current-version-of-rob-2?authuser=0 (accessed on 2 April 2024).
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Cochrane. Review Manager (RevMan). 2024. Available online: https://training.cochrane.org/online-learning/core-software (accessed on 8 April 2024).
- Barker, T.H.; Habibi, N.; Aromataris, E.; Stone, J.C.; Leonardi-Bee, J.; Sears, K.; Hasanoff, S.; Klugar, M.; Tufanaru, C.; Moola, S.; et al. The revised JBI critical appraisal tool for the assessment of risk of bias for quasi-experimental studies. JBI Evid. Synth. 2024, 22, 378–388. [Google Scholar] [CrossRef]
- National Heart Lung and Blood Institute (NIHLBI). Quality Assessment Tool for Before-After (Pre-Post) Studies with No Control Group. 2014. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 2 April 2024).
- Allen, J.K.; Dennison, C.R.; Szanton, S.L.; Frick, K.D. Cost-effectiveness of nurse practitioner/community health worker care to reduce cardiovascular health disparities. J. Cardiovasc. Nurs. 2014, 29, 308–314. [Google Scholar] [CrossRef]
- Mackey, P.A. Care directed by speciality-trained nurse practitioner or physician assistant can overcome clinical inertia in management of inpatient diabetes. Endocr. Pract. 2014, 20, 112–119. [Google Scholar]
- Richardson, G.C.; Derouin, A.L.; Vorderstrasse, A.A.; Hipkens, J.; Thompson, J.A. Nurse practitioner management of type 2 diabetes. Perm. J. 2014, 18, e134–e140. [Google Scholar] [CrossRef] [PubMed]
- Kuo, Y.F.; Goodwin, J.S.; Chen, N.W.; Lwin, K.K.; Baillargeon, J.; Raji, M.A. Diabetes mellitus care provided by nurse practitioners vs primary care physicians. J. Am. Geriatr. Soc. 2015, 63, 1980–1988. [Google Scholar] [CrossRef] [PubMed]
- Brumm, S.; Theisen, K.; Falciglia, M. Diabetes transition care from an inpatient to outpatient setting in a veteran population: Quality improvement pilot study: Quality improvement pilot study. Diabetes Educ. 2016, 42, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Hurwitz, S.; Rein, R.; Schuman, B.; Underwood, P.; Bhandari, S. Effect of follow-up by a hospital diabetes care team on diabetes control at one year after discharge from the hospital. Diabetes Res. Clin. Pract. 2017, 133, 78–84. [Google Scholar] [CrossRef]
- Kuo, C.R.; Quan, J.; Kim, S.; Tang, A.Y.; Heuerman, D.P.; Murphy, E.J. Group visits to encourage insulin initiation: Targeting patient barriers. J. Clin. Nurs. 2017, 26, 1705–1713. [Google Scholar] [CrossRef]
- Gardiner, F.W.; Nwose, E.U.; Bwititi, P.T.; Crockett, J.; Wang, L. Does a hospital diabetes inpatient service reduce blood glucose and HbA1c levels? A prospective cohort study. Ann. Med. Surg. 2018, 26, 15–18. [Google Scholar] [CrossRef]
- Marin, P.A.; Bena, J.F.; Albert, N.M. Real-world comparison of HbA 1c reduction at 6-, 12- and 24-months by primary care provider type. Prim. Care Diabetes 2018, 12, 319–324. [Google Scholar] [CrossRef]
- Akiboye, F.; Adderley, N.J.; Martin, J.; Gokhale, K.; Rudge, G.M.; Marshall, T.P.; Rajendran, R.; Nirantharakumar, K.; Rayman, G.; DICE team. Impact of the Diabetes Inpatient Care and Education (DICE) project on length of stay and mortality. Diabet. Med. A J. Br. Diabet. Assoc. 2019, 37, 277–285. [Google Scholar]
- McGloin, H.; O’Connell, D.; Glacken, M.; Mc Sharry, P.; Healy, D.; Winters-O’Donnell, L.; Crerand, K.; Gavaghan, A.; Doherty, L. Patient empowerment using electronic telemonitoring with telephone support in the transition to insulin therapy in adults with type 2 diabetes: Observational, pre-post, mixed methods study. J. Med. Internet Res. 2020, 22, e16161. [Google Scholar]
- Kulsick, C.; Votta, J.; Wright, W.L.; White, P.; Strowman, S. Enhancing medication adherence in older adults at two nurse practitioner-owned clinics. J. Am. Assoc. Nurse Pract. 2020, 33, 553–562. [Google Scholar] [CrossRef]
- Yago-Esteban, G.; Venturas, M.; Blanco, J.; Pérez, I.; Falces, C.; Roqué, M.; Yugueros, X.; Cardete, L.; Renu, A.; Caellas, D.; et al. Blood glucose monitoring during hospitalisation: Advanced practice nurse and semi-automated insulin prescription tools. Endocrinol. Diabetes Nutr. 2022, 69, 500–508. [Google Scholar] [CrossRef]
- Marsh, Z.; Teegala, Y.; Cotter, V. Improving diabetes care of community-dwelling underserved older adults. J. Am. Assoc. Nurse Pract. 2022, 34, 1156–1166. [Google Scholar] [CrossRef] [PubMed]
- Dimond, K. Improving glucose control in patients with type 2 diabetes using retrospective continuous glucose monitoring. J. Am. Assoc. Nurse Pract. 2023, 35, 425–433. [Google Scholar]
- Ju, H.H.; Momin, R.; Cron, S.; Jularbal, J.; Alford, J.; Johnson, C. A nurse-led telehealth program for diabetes foot care: Feasibility and usability study. JMIR Nurs. 2023, 6, e40000. [Google Scholar]
- Knee, M.; Hussain, Z.; Alkharaiji, M.; Sugunendran, S.; Idris, I. Diabetes specialist nurse point-of-care review service: Improving clinical outcomes for people with diabetes on emergency wards. Pract. Diabetes 2020, 37, 50–54. [Google Scholar] [CrossRef]
- Cabré, C.; Colungo, C.; Vinagre, I.; Jansà Morató, M.; Conget, I. Resultados del programa de educación terapéutica de optimización dirigido a pacientes insulinizados con diabetes tipo 2 desarrollado por enfermería de práctica avanzada en diabetes en el ámbito de atención primaria. Endocrinol. Diabetes Nutr. 2021, 68, 628–635. [Google Scholar] [CrossRef]
- Russo, M.P.; Grande-Ratti, M.F.; Burgos, M.A.; Molaro, A.A.; Bonella, M.B. Prevalencia de diabetes, características epidemiológicas y complicaciones vasculares. Arch. Cardiol. Mex. 2023, 93, 30–36. [Google Scholar] [CrossRef]
- Franch, J.; Artola, S.; Diez, J.; Mata, M. Evolución de los indicadores de calidad asistencial al diabético tipo 2 en atención primaria (1996–2007). Programa de mejora continua de calidad de la Red de Grupos de Estudio de la Diabetes en Atención Primaria de la Salud. Med. Clin. 2010, 135, 600–607. [Google Scholar] [CrossRef]
- Lewandowicz, A.; Skowronek, P.; Maksymiuk-Kłos, A.; Piątkiewicz, P. The giant geriatric syndromes are intensified by diabetic complications. Gerontol. Geriatr. Med. 2018, 4, 233372141881739. [Google Scholar] [CrossRef]
- Simarro, L.; Unanua, F. Diferencias y similitudes de la DM2 en hombres y mujeres: Lo que nos hace diferentes en diabetes. Rev. Diabetes 2024, 86, 1–6. [Google Scholar]
- Puig, P.; Ciria, M.T. Diabetes desde la perspectiva de género. Diabetes Práct. 2021, 12, 35–76. [Google Scholar] [CrossRef]
- Chapman, M.; García, R.; Caballero, G.; Paneque, Y.; Sablón, A. Efectividad de intervención educativa en el conocimiento del paciente diabético sobre autocuidados. Rev. Cuba Enfermería 2016, 32, 49–59. [Google Scholar]
- Guzmán-Priego, C.G.; Baeza-Flores, G.; Atilano-Jiménez, D.; Torres-León, J.A.; de Jesús León-Mondragón, O. Efecto de una intervención educativa sobre los parámetros bioquímicos de pacientes diabéticos de un servicio médico institucional. Aten. Fam. 2017, 24, 82–86. [Google Scholar] [CrossRef]
- De Carvalho, H.; Rodrigues, F.; Rodrigues, L. Avaliação das ações educativas na promoção do autogerenciamento dos cuidados em diabetes mellitus tipo 2. Rev. Esc. Enferm. USP 2011, 45, 1077–1082. [Google Scholar] [CrossRef]
- Tellier, H.; Colson, S.; Gentile, S. Améliorer la prise en charge de l’enfant atteint de diabète de type 1 et celle de sa famille: Quel rôle pour l’infirmière de pratique avancée, coordinatrice de parcours complexe de soins? Une étude qualitative et exploratoire. Rech. En. Soins Infirm. 2019, 136, 80–89. [Google Scholar]
- Galiana-Camacho, T.; Gómez-Salgado, J.; García-Iglesias, J.J.; Fernández-García, D. Enfermería de Práctica Avanzada en la atención urgente, una propuesta de cambio: Revisión sistemática. Rev. Española Salud Pública 2018, 92, e201809065. [Google Scholar]
- Martínez, A.; González, A.M.; Roldán, M.T.; Cervantes, C.; Conesa, A.M.; Riquelme Hurtado, M.J. Intervenciones de enfermería psicoeducativas presenciales y on-line, para el manejo de la ansiedad: Revisión integradora de la literatura. Enferm. Glob. 2022, 21, 531–561. [Google Scholar] [CrossRef]
- Tinoco, J.M.; Hidalgo, M.A.; Daifuku, N.; Lluch, M.T.; Raigal, L.; Puig, M. Intervenciones enfermeras para disminuir la sobrecarga de cuidadores informales. Revisión sistemática de ensayos clínicos. Enferm. Glob. 2022, 21, 562–586. [Google Scholar] [CrossRef]
- Ordóñez-Piedra, J.; Ponce-Blandón, J.A.; Robles-Romero, J.M.; Gómez-Salgado, J.; Jiménez-Picón, N.; Romero-Martín, M. Effectiveness of the Advanced Practice Nursing interventions in the patient with heart failure: A systematic review. Nurs. Open 2021, 8, 1879–1891. [Google Scholar] [CrossRef]
- Huaraca, C.G.; Ordoya, S.M.; Rivera, I.C.; Melgarejo, N.M.; Li, I.L. Enfermería de práctica avanzada (EPA) en un contexto internacional. Rev. Climatol. 2023, 23, 3106–3123. [Google Scholar] [CrossRef]
- Abraham, C.M.; Norful, A.A.; Stone, P.W.; Poghosyan, L. Cost-Effectiveness of Advance Practice Nurses compared to Physician-Led care for Chronic Diseases: A systematic review. Nurs. Econ. 2019, 36, 293–305. [Google Scholar]
- Molina-Gil, M.J.; Guerra-Martín, M.D.; De Diego-Cordero, R. Primary healthcare Case Management Nurses and assistance provided to chronic patients: A narrative review. Healthcare 2024, 12, 1054. [Google Scholar] [CrossRef] [PubMed]
- Schober, M. Desarrollo de la Enfermería de Práctica Avanzada: Contexto internacional. Enfermería Clín. 2019, 29, 63–66. [Google Scholar] [CrossRef] [PubMed]
- San Martín Rodríguez, L.; Soto Ruiz, N.; Escalada Hernández, P. Formación de las enfermeras de práctica avanzada: Perspectiva internacional. Enfermería Clín. 2019, 29, 125–130. [Google Scholar] [CrossRef]
- Momin, R.P.; Kobeissi, M.M.; Casarez, R.L.; Khawaja, M. A nurse practitioner–led telehealth protocol to improve diabetes outcomes in primary care. J. Am. Assoc. Nurse Pract. 2022, 34, 1167–1173. [Google Scholar] [CrossRef]
- Wright, W.L.; White, P.A.; Welsh, M.; Cutting, K. Evaluating the effect of COVID-19 on quality measures of patients with type 2 diabetes in two family nurse practitioner–owned clinics. J. Am. Assoc. Nurse Pract. 2022, 34, 1090–1097. [Google Scholar] [CrossRef]
- Akiboye, F.; Sihre, H.K.; Al Mulhem, M.; Rayman, G.; Nirantharakumar, K.; Adderley, N.J. Impact of diabetes specialist nurses on inpatient care: A systematic review. Diabet. Med. 2021, 38, e14573. [Google Scholar] [CrossRef]
- Dutton, J.; McCaskill, K.; Alton, S.; Levesley, M.; Hemingway, C.; Farndon, L. Changing roles in community health care: Delegation of insulin injections to health care support workers. Br. J. Community Nurs. 2018, 23, 14–19. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).