Abstract
Background/Objectives: Heart failure assistance is strictly correlated with the concept of palliative care. Supportive treatment should be part of the heart failure patient pathway from the beginning. Palliative care with interprofessional effective collaboration could be an important resource used to reduce heart failure distressing symptoms and improve quality of life. Nurses, as professionals with a holistic vision of care, play a crucial role in palliative care introduction and implementation. The aim was to explore nurses’ attitudes and perceptions of heart failure palliative care, updating and adding knowledge to the current evidence. Methods: A systematic mixed-method review following the Joanna Briggs Institute methodology was undertaken. The screening of articles, data extraction and quality appraisal were performed by more than one author. The search was undertaken in May 2024 and applied to PubMed, Cinahl, Embase, Web of science, PsycInfo, Cochrane library and Scopus. A convergent integrated approach allowed us to combine qualitative and quantitative data. The analysis and synthesis of results was guided by the Theoretical Domain Framework. Results: Of the 1048 records identified, 26 met the inclusion criteria. Twelve framework domains were completed with data extracted. A flow chart was elaborated to offer an overview of the main concepts included. Conclusions: Numerous behaviors and elements influenced heart failure palliative care implementations. Analysis has shown that each analyzed element was strictly correlated one with another. When implementation was possible, outcome improvement sustained palliative care benefits with the direct involvement of nurses as educators and coordinators.
1. Introduction
Palliative care is a comprehensive and supportive care program that is recommended for all people with distressing symptoms [1]. The belief that palliative care is delivered solely to patients who are about to die [2], and destined exclusively for patients dying or suffering from cancer, exists [3].
The prevalence of people living with chronic non-communicable diseases is increasing dramatically. There are numerous chronic diseases by which adults may be affected, and the correlated symptom burdens are very important [4].
The World Health Organization (WHO) underscores that 56.8 million people need palliative care, but less than 50% of people with non-communicable diseases are reached by their services [5].
Heart failure is a clinical syndrome consisting of cardinal symptoms such as breathlessness, ankle swelling and fatigue; it is accompanied by signs (e.g., elevated jugular venous pressure, pulmonary crackles, and peripheral edema) and correlated with elevated intracardiac pressures and/or inadequate cardiac output [6].
The Heart Failure Society of America 2024 states that the lifetime risk of heart failure has increased to 24%, and the prevalence is expected to rise to 8.7 million in 2030, 10.3 million in 2040, and 11.4 million by 2050 [7]. The European Society of Cardiology (ESC) 2021 reported a prevalence of 1–2% in adults. This prevalence is probably higher since studies reported only recognized/diagnosed heart failure cases.
Patients with heart failure have the same distressing symptoms and correlated symptom burdens as those with cancers. In the most advanced stages, the number of symptoms exceeds those associated with advanced cancer [3,8]. The disease trajectory of each heart failure patient is unique but characterized by a gradual decline, which leads to team-based approach palliative care evaluations [6].
As studies have evidenced, heart failure palliative care is correlated with multiple difficulties due to the unpredictable course of the disease, the lack of specific education and communication, and misconceptions [3,9].
The literature in primary and secondary studies on heart failure palliative care is increasing.
Different types of reviews—narrative, systematic and integrative review—have been conducted. However, they explore different palliative care aspects such as cost effectiveness [10], tools [11], carer needs [12], interventions [9], and nurse opportunities to overcome barriers [13], with different methodological aspects.
Bagheri et al. (2022) [1] analyzed palliative care heart failure guidelines’ quality, and they evidence a low score of these guidelines’ applicability due to a lack of discussion about facilitators, barriers, potential sources of recommendations, and monitoring and/or audit criteria.
The WHO recognizes the importance of nurses as part of the multidisciplinary teams involved in palliative care [5].
Nurses play a crucial role in palliative care delivery. Nurses often recognize changes in patient health status, providing an understanding of the right moment to consider palliative care [14]. Indeed, they are holistic providers whose role is crucial in delivering palliative care, which is also influenced by their attitudes [15,16]. Research has demonstrated a positive impact of palliative care led by nurse involvement when barriers are overcome [14]. Across palliative care settings, nurses have a unique position, with a broad range of abilities and activities [17].
As part of the interprofessional approach on which palliative care is based [1], understanding the point of view of each specific team member may help improve palliative care’s effective implementation with correlated benefits for the patients and carers involved.
The purpose of this systematic review was to elaborate an overview of nurses’ attitudes, experiences and perceptions about heart failure palliative care using a methodology that allows integrated results derived from qualitative and quantitative studies. Deepening knowledge of these topics may help to identify facilitators and barriers to effective palliative care implementation. Clear identification may allow interventions and improvement in clinical practice. The published articles mostly analyze heart failure palliative care without focusing merely on the nurses’ point of view.
Aims
The primary aim of this systematic mixed method review is to explore nurses’ attitudes and perceptions regarding heart failure palliative care.
The main questions that the systematic revision intends to answer are as follows:
1—What are nurses’ attitudes and experiences of heart failure palliative care implementation?
2—What are nurses’ perceptions of effective heart failure palliative care applicability?
The secondary aim was to distinguish nursing interventions according to the caring phase—onset of heart failure, decompensation, end of life care and advanced care planning.
2. Materials and Methods
2.1. Design
A systematic mixed method review was conducted following the Joanna Briggs Institute (JBI) guidelines [18]. This method was chosen to evidence all the potential eligible information about nursing attitudes, experiences and perceptions. A first review of the literature, in fact, showed that the potentially pertinent studies conducted differ in methodological aspects.
This systematic mixed method review is reported using the preferred reporting items for systematic review and meta-analysis (PRISMA) statement criteria [19].
The review protocol has been registered in Prospero https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024573570 (accessed on 29 December 2024).
2.2. Search Method
The search strategies were developed with the support and the guidance of an expert informatician and academic librarian. In order to find all the available evidence, a specific research strategy was adapted for each interrogated database, using keywords as indexed terms. It was applied to many sources—Cinahl, Psycinfo, Embase, Scopus, Cochrane Library, PubMed and Web of Science. Every article, either in English or in Italian, corresponding to inclusion criteria was selected. The search was undertaken in May 2024 with no limitation applied to publication date.
After performing the searches (Table 1), duplicate records were eliminated and screened by title and abstract by two independent reviewers. Any disagreement was actively discussed with the collaboration of a third researcher in case of discordance. To minimize the risk of bias, the Rayyan software (https://help.rayyan.ai/hc/en-us/articles/4406419348369-What-is-the-version-of-Rayyan, accessed on 15 February 2025) was used to ensure the blindness of the process [20,21]. With the same procedure, the full texts of the potentially eligible studies were analyzed. Reference lists of screened eligible articles were reviewed to find other eligible articles.

Table 1.
Search strategy, focus of interest and exclusion motivations.
Studies were considered for inclusion when the eligibility criteria were met. The inclusion criteria were applied to all studies in which the utilized method was clearly defined, and the full text of the article was available. Primary qualitative, quantitative and mixed-methods studies were included. Mixed-method studies were only considered if data from quantitative or qualitative components could be clearly extracted.
Secondary literature studies (e.g., reviews, meta-analyses, study synopsis), descriptive articles that did not report data collected on a sample of subjects, case reports, case series, and expert opinions were not included. Articles of secondary literature studies were evaluated for inclusion, while review articles were excluded. Our aim was in fact to extract data from primary studies and to elaborate a mixed method systematic review.
Studies involving children or patients aged less than 18 were excluded, given the particular needs of this segment of population.
The PICO of the included studies summarizes the two aim questions described above. The acronym includes “P” as heart failure patients for whom nurses’ palliative aspects of care were implemented or considered; “I” is nurses’ attitudes and perceptions of palliative care implementation; “C” is usual practice and any kind of different intervention, if present; “O” is outcomes related to nursing palliative care attitudes, perceptions, and interventions in palliative heart failure care.
The expression “nurses’ attitudes and perceptions” refers to all the aspects of evidence-based practice implementation considered as triggering issues or opportunities.
The main outcomes that the systematic mixed method review intended to study in depth were nursing palliative care aspects for heart failure patients.
Other outcomes that the systematic review aimed to explore were the specific interventions with nursing involvement in heart failure palliative care.
The critical assessment of included studies was conducted by two researchers using the JBI Critical Appraisal Tools—Checklist for Randomized Controlled Trials [22], Checklist for quasi-experimental study [23], Checklist for Prevalence study [24], Checklist for analytical cross-sectional study [25], Checklist for cohort studies [25] and Checklist for qualitative studies [26]. Quantitative and qualitative aspects of mixed-method studies were evaluated using the corresponding JBI checklist. After independent evaluations, any disagreement was discussed by the two members of the team. In case of discordance, a third one was involved. Quality appraisal was evidenced and considered in the interpretation and discussion of results.
Data of eligible studies were extracted by first and second authors following the Joanna Briggs Institute indications. Aspects included in the data extraction format were the type of study, country, setting, aim, characteristics of participants, age and sex of participants, training, heart failure population type, type of palliative care, outcomes defined, data collection, period of data collection, data analysis, key findings and limitations.
To have a greater depth of understanding of the phenomena, the convergent integrated approach of the JBI mixed-methods systematic review guidelines was implemented. Data were synthesized by two researchers with continuous comparison and discussion. Convergent synthesis refers to the process of combining data extracted from quantitative research and qualitative research. Quantitative data were “qualitized” as textual descriptions through narrative interpretation. Qualitative data were firstly extracted, identifying findings, categories and synthetized findings.
Hence, nursing attitudes and perceptions towards palliative care practice were categorized using the Theoretical Domains Framework (TDF) revised by Cane et al. (2012) [27]. TDF identifies 14 domains in which categorized behavior influences the implementation of the evidence base.
Summarizing nursing attitudes and perceptions in the specific setting of heart failure palliative care enabled us to identify all variables that have to be considered to undertake palliative care in heart failure patients.
In order to synthesize the existing knowledge, tables have been used to present the key concepts identified through the analysis in which the synthetized findings were reported.
3. Results
3.1. Selection of Sources
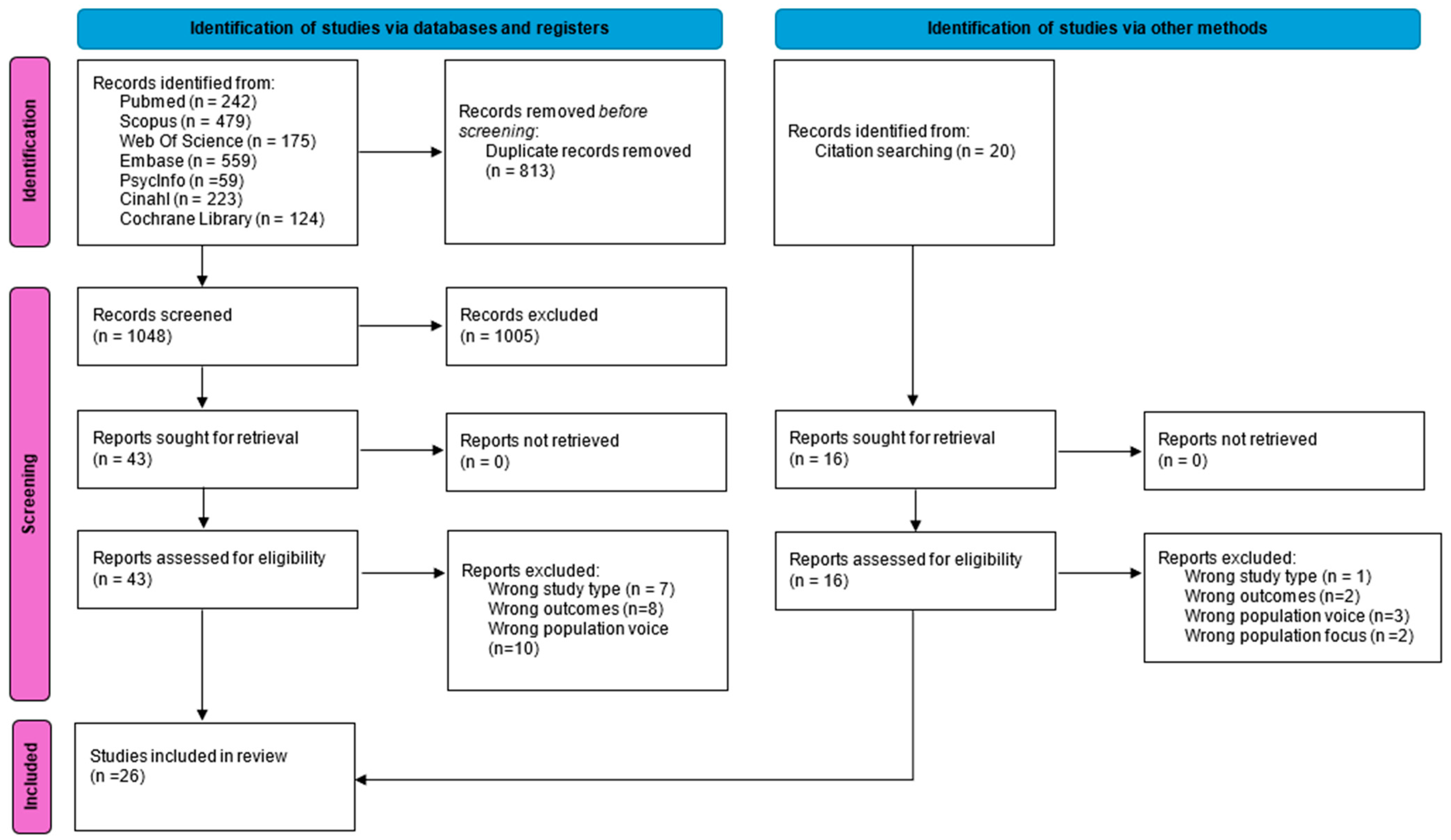
Database searching identified 1861 articles; after removing duplicates, 1048 articles were screened for title and abstract. Among these, 43 articles were included for full-text review. Following a full text review, 18 articles were included. Another 16 articles that were potentially eligible were identified from full-text reference analyses, from which 8 were excluded. A total of 26 articles are included in this review. An outline of the study screening and selection process is presented in the PRISMA flowchart shown in Figure 1 [19].
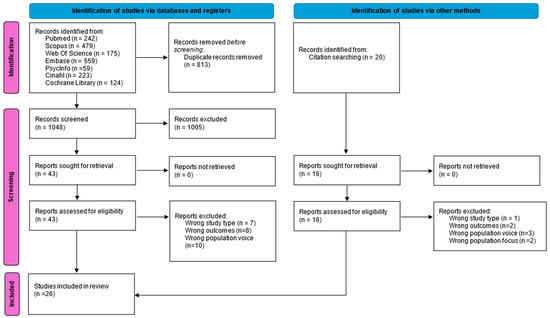
Figure 1.
Flow diagram for selection of studies (PRISMA FLOW DIAGRAM).
3.2. Critical Appraisal of Sources of Evidence
Seven randomized controlled trials were appraised using the JBI Critical Appraisal Tools: Checklist for Randomized Controlled Trials. For all studies, patient and assessor blindness was not applied [28,29,30,31,32,33,34]. Therefore, four assessors were not blind to treatment assignment, or the report was unclear about the item [28,30,33,34]. Thirteen studies were evaluated through the qualitative checklist [35,36,37,38,39,40,41,42,43,44,45,46,47]. Most of them demonstrated a lack of information or an absence of researcher influence on the study evaluation.
The critical aspect of the cohort study analyzed was the absence of confounding factors considered [48]. A cross-sectional study was conducted for almost all checklist items [43]. Patient characteristics were not described in detail by all [43,49,50,51], and three [49,50,51] of them did not clearly describe inclusion criteria.
Prevalence studies demonstrated some critical aspects related to the detail of the sample and coverage and response rates [42,52].
No study was excluded based on quality evaluation. Critical appraisal was fundamental to the discussion and interpretation of the results, and to deriving an understanding of the studies’ characteristics.
3.3. Characteristics of Source of Evidence
Table 2 outlines the included studies. Most employed a qualitative design (n = 11) [35,36,37,38,39,40,41,44,45,46,47]. Ten employed the interview format for data collection. Four studies were conducted in the United Kingdom [38,39,41,45], two in Iran [35,40], three in Australia [36,44,46], one in Sweden [37] and one in Germany [47]. Quantitative studies were mostly randomized controlled studies (n = 7) [28,29,30,31,32,33,34], with one pilot pre- and post-test study [53], one pragmatic nonrandomized study [51], one descriptive study [48] with a cohort method, and three cross-sectional studies [43,49,50]. Two mixed-method studies [42,52] with qualitative data and a survey were included.
Table 2.
Characteristics and main results of the studies considered in this review.
Qualitative interviews or questionnaire were directed only towards nurses in four studies [35,36,37,42]. Other samples consisted of an interprofessional team, with carer involvement in two cases [38,40]. Randomized controlled studies evaluated the efficacy of the intervention analyzed for samples of patients [28,29,30,31,32,33,34]. The observational cohort and cross-sectional studies observed nurses working in heart failure palliative care [43,48,49,50]. The pilot quasi experimental study focused on nurses’ outcomes improvement after educational intervention [53]. The survey was submitted to nurses, physicians and other healthcare professionals. Mixed studies evaluated only nurses’ positions.
3.4. Nurses’ Attitudes and Perceptions
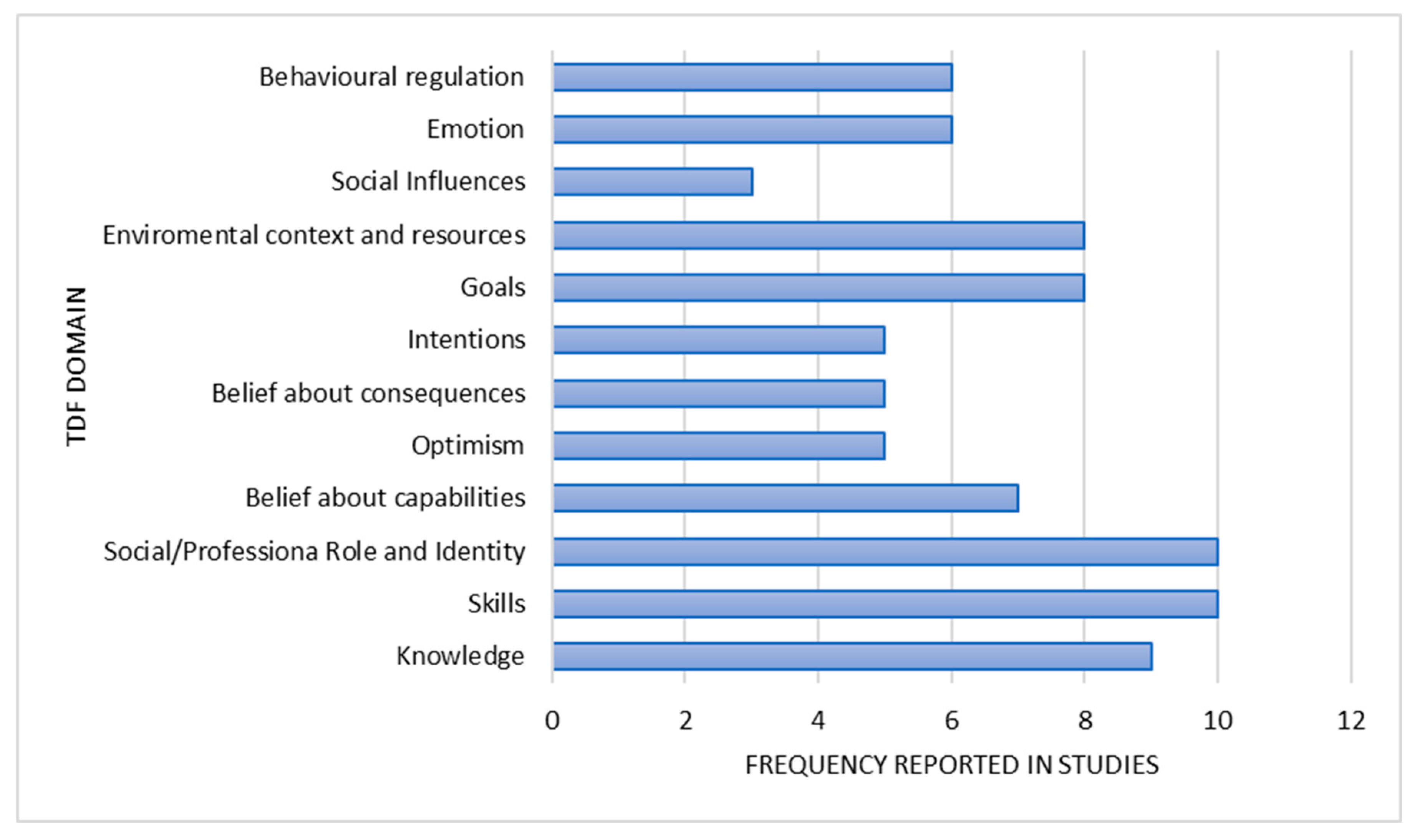
Qualitative and qualitative data about nurses’ attitudes and perceptions were allocated to twelve of the fourteen TDF domains (Figure 2, Table 3).
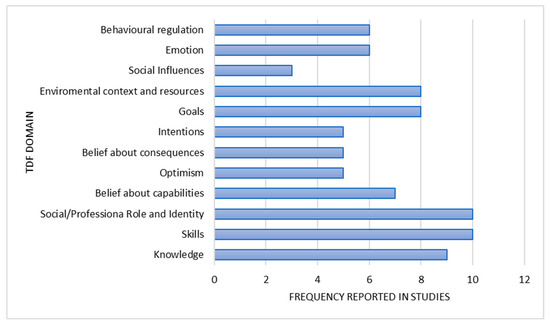
Figure 2.
TDF domains frequency.
Table 3.
Findings for each TDF domain.
3.4.1. Knowledge
Knowledge was a theme discussed by nurses. Patients and carers were described to have unrealistic expectations regarding diagnosis and trajectory. Education and information were not always given by doctors when it was perceived that patients had to have all treatment options. Professionals and nurses knew that each patient was unique and that knowledge improved attitudes. Knowledge about palliative care and chronic illness is important. Clinicians were lacking in palliative care for heart failure management and did not know how to delay all symptoms. Knowledge also implies knowing who is responsible for providing palliative care. Nurses knew and understood the concept of working in a team.
3.4.2. Skills
Recognition of when to start palliative care was considered difficult, and it often happened too late. Relapses offer indicators for considering palliative care. Nurses were better than clinicians at talking about palliative care and at considering constructing a good relationship and related communication with the patient from the beginning. Nurse specialists who could provide end-of-life palliative care were lacking due to a lack of master’s degrees in the sector.
3.4.3. Social/Professional Role and Identity
Palliative care team involvement and consultation was desirable. Interprofessional involvement, cooperation and communication are needed. It could be painful or helpful, but it is important. Multiple ideas and poor communication could become an obstacle to palliative care implementation. Defining roles and duties was perceived as fundamental. Communicating, asking for advice and reflecting on difficult situations were outlined elements, and discussion across team members helped the learning process.
3.4.4. Beliefs About Capabilities
Communication abilities between members of an interdisciplinary team were described as fundamental to help patients achieve good death. Sometimes, communication abilities were also reported as weak and fragmented. Nurses understood the importance of discussing prognosis, but they hesitated if clinicians had not already done so. They did not feel comfortable when perceiving a lack of education in discussing prognosis, which was considered a physician’s responsibility.
3.4.5. Optimism
Patients’ false hopes were described. They were optimistic when included on the transplant list because they did not have cancer, without recognizing the chronic life-limiting condition. Patients’ and families’ thoughts were unrealistic and they did not accept limited further interventions. Younger nurses did not always understand mortality. Professionals perceived patients’ limited awareness of the gravity of the situation.
3.4.6. Beliefs About Consequences
Patients and families identified palliative care as giving up. Nurses were afraid to frighten people or take away their hope by talking about the end of life. Specific palliative care education was considered beneficial in allowing the integration of palliative care and relative signs’ recognition.
3.4.7. Intentions
Prognosis was a difficult topic to address in heart failure assistance. It is described as important. Clinicians desired to talk about prognosis, but it was not always possible. Some people appreciated discussing the prognosis others did not want.
Transition to palliative care was considered by physicians as a failure, and team spirit was lacking.
3.4.8. Goals
Nurses described heart failure as an illness with an unpredictable trajectory correlated with a difficulty in understanding when to start palliative care. It was difficult to understand when to begin focusing on symptoms or medical treatment. Patients were not aware of the chronic long-term progressive illness. Death acceptance and discussions about death were important. Professionals would have preferred to be honest with patients when nurses and clinicians perceived the need to initiate palliative care and correlated goals in different moments. Cardiologists fixated on heart failure mechanisms without thinking about well-being or death.
3.4.9. Environmental Context and Resources
Limited resources, financial constraints, and little time to build relationships were some of the obstacles described by nurses. Professional education was a huge need when there was a shortage of specialist medical professionals and services in the field of palliative care. The homecare setting was considered easier for people to be themselves.
3.4.10. Social Influences
Health system support in providing palliative care services was not always perceived, and societies might not want to introduce, speak about or plan for death. In some contexts, no-resuscitation laws were present. A gap in identifying who is responsible to provide palliative care is sometimes described.
3.4.11. Emotions
Nurses felt nervous, constantly anxious, and tired when taking care of end-of-life heart failure patients, drowning in their suffering. They felt angry and frustrated about resuscitating people when they identified it as not appropriate. Frustration emerged when nobody made decisions about palliative care, or when it was difficult to talk about death in a homecare setting. Positive feelings arose instead when patients relied on them in communicating their feelings. The family and patients did not always desire to talk about death. Some welcomed it, while others denied that patients’ conditions were getting worse.
3.4.12. Behavioral Regulation
Nurse involvement as case managers in disease and symptoms management has a positive impact on multiple dimensions: severity of symptoms, physical and mental functioning, satisfaction, admission, and quality of life. The leadership or nurse coordination of a team is correlated with positive outcomes. Psychoeducational interventions and virtual programs are some of the methods used to improve patient outcomes.
3.5. Nurses’ Interventions
Quantitative studies’ interventions and their correlated outcomes are synthesized in Table 4. Ten different types of interventions were identified. None of the studies evidenced a negative impact of the intervention analyzed. Regarding outcomes explored, only in a limited number of situations was there no difference in the intervention implementation found [28,31].
Table 4.
Quantitative studies’ interventions and outcomes explored.
4. Discussion
This systematic review evaluates nurses’ attitudes and perceptions about heart failure palliative care. A mixed-method methodology allowed us to integrate experiences and effectiveness so as to derive a deeper understanding of the topic [18].
We classified nursing attitudes, experiences and perceptions using TDF domains developed by Cane et al. (2012) [27]. This framework was developed to explain implementation problems, inform implementation interventions, and bring about behavioral change. It could be applied to either qualitative or quantitative data [27]. A summary of the findings is presented with Table 5. Knowledge was a theme that affected all care participants. Nurses highlighted that patients and carers have unrealistic expectations regarding diagnosis and trajectory. A lack of information regarding heart failure severity and prognosis is an important barrier to palliative care implementation, described also by Schallmo et al. (2019) [54]. Clinicians and nurses were aware of the importance of knowledge to improving attitudes. However, information was not always given, and clinicians were lacking in training about symptom management. Nevertheless, symptom burden associated with heart failure is comparable to, or exceeds, that of cancer patients [9].
Table 5.
Summary of findings.
Knowledge should be improved considering not only health professionals’ training and educations, but also enhancing patient’s awareness and disease knowledge. Although cardiologists should be able to assess and treat heart failure symptoms, it is also important to consider specific palliative care specialists’ involvement [55]. Poorly delivered information is strictly correlated with communication. Communication and education about treatment options are fundamental to increase healthcare professionals’ knowledge, attitudes and preparedness to practice [54]. A lack of knowledge about who was responsible for providing palliative care emerged. Oishi et al. (2014) [56] evidenced this problem in 2014, describing how each professional involved expects other specialists to take more responsibility in patients’ palliative care. They underlined the importance of coordinated care, recognizing the presence of many barriers correlated with a lack of resources and time to maintain the shared vision, mutual respect and inclusive decision-making. These are the same barriers that were identified by our systematic review. Responsibility also emerged through the prognosis concept. Nurses described the topic as difficult. It is not clear who is responsible for talking about prognosis and patients do not always appreciate talking about it. Prognosis represents an obstacle related to the concept of intentions. Prognosis is in fact correlated with the concept of shared decision-making. Timing and communication in relation to prognosis are also difficult in the case of cancer patients [57]. In noncommunicable non-cancer diseases, such as heart failure, understanding prognosis is more difficult because of the unpredictable nature of the illness characterized by episodic, acute exacerbations, frequent hospitalization, stabilization and steady decline. Predicting and talking about prognosis is, however, important to estimate healthcare utilization and to identify groups that may benefit from specific intervention [58,59]. However, tools and scores available to estimate prognosis were prevalent in relation to cancer disease [58]. There are wide variations in access to palliative care in people with heart failure compared to those with cancer [59]. We believe that it is possible to state that communication should not be overlooked in clinical practice. It is in fact an important theme strictly correlated with healthcare professionals’ effective communication within their team, but also with patients and families. If adequately implemented, it could contribute many barrier reductions.
Moreover, our results show that patients were not always aware about the illness’s gravity, and did not recognize the chronic life-limiting conditions. As the study of Shropshire et al. (2023) [60] shows, heart failure awareness is still lacking, and it is influenced by multiple factors, such as numbers of opportunities to meet healthcare providers, the lack of symptoms or nonspecific symptoms, and an identifiable heart failure cause as the consequence of myocardial infarction. Lack of awareness is a problem that starts in the general population, who have insufficient knowledge of the symptoms, causes and treatment methods of this disease [61]. Awareness, poor understanding of the disease and a lack of belief in treatment are some of the factors influencing a patient’s adherence to treatment [62].
Starting palliative care for heart failure patients and carers was perceived as giving up. Consequently, nurses were afraid to talk about prognosis, end of life and death. Understanding when to start palliative care or focusing on symptoms rather than medical treatment is limited by the unpredictable illness trajectory and patient awareness of illness. The literature contains evidence that it should be necessary to consider palliative care as part of the overall treatment due to the unpredictable course of the disease [3]. Clinicians sometimes are more able to predict death or end-of-life care due to the severe and refractory symptoms that are present [2]. Tools and scores are prevalent in relation to cancer disease, and now some have also been developed for heart failure patients, such as the “needs assessment tools progressive disease: heart failure” (NAT: PD-HF) [11,58,63].
Nurses identified the importance of education for the implementation and integration of palliative care services. Education is a huge need. The literature has already evidenced that structured nursing student education may improve and encourage attitudes regarding providing care to patient who are dying [64]. However, limited resources and financial constraints have been described as obstacles to palliative care. The lack of specialists and services is a problem that has already been described. The WHO, in an article published in 2021, underlined that the provision of palliative care in most countries lags far behind the need for these essential services. Further elements on which to focus attention include the fact that health system support in providing palliative care was not always perceived, and societies might not want to introduce, speak about or plan for death, or set specific laws on some aspects of palliative care. Healthcare systems should take into consideration the importance of palliative care, differentiating intervention based also on cultural beliefs. As such, it may be possible to avoid unnecessary expenses or later interventions. The lack of palliative care treatments is a problem described across the world, in which cultural aspects should be considered, particularly in multicultural societies in which the dominant culture affects life opportunities at both group and individual levels in lower social strata [65]. In many countries, there is a progressive and growing acceptance of legal support as a key component of holistic palliative care to defend and respect human rights. Ezer et al. (2018) [66] and Osei et al. (2022) [67] described the progress made by countries such as Romania, Hungary, Georgia, Malawi, Kenya and East Asian countries. As these studies have demonstrated, legislation about palliative care is increasing, but differences already exist across the countries, and many developments still have to be encouraged.
A theme that permeates, and which is the consequence of all the topics analyzed, regards the emotions felt by nurses, patients and carers. Nurses described themselves as anxious, tired, frustrated and angry due to the patients’ suffering, and thus encountered difficulty in palliative care implementation.
Experimental studies demonstrated positive results, supporting the importance of building good-quality palliative care programs.
Interdisciplinary collaboration was mostly implemented [28,30,33,34,51]. People receiving the palliative program experienced positive effects on symptoms frequency and severity, health status, and quality of life. Clear evidence of hospital admission reductions did not emerge, possibly related to the type of intervention delivered.
These interventions were focused on the introduction of a nurse with palliative competence who evaluated patients’ symptoms and supported them throughout educational interventions or the coordinated interventions of the interdisciplinary team. The activities aligned with the needs that emerged from the qualitative aspects.
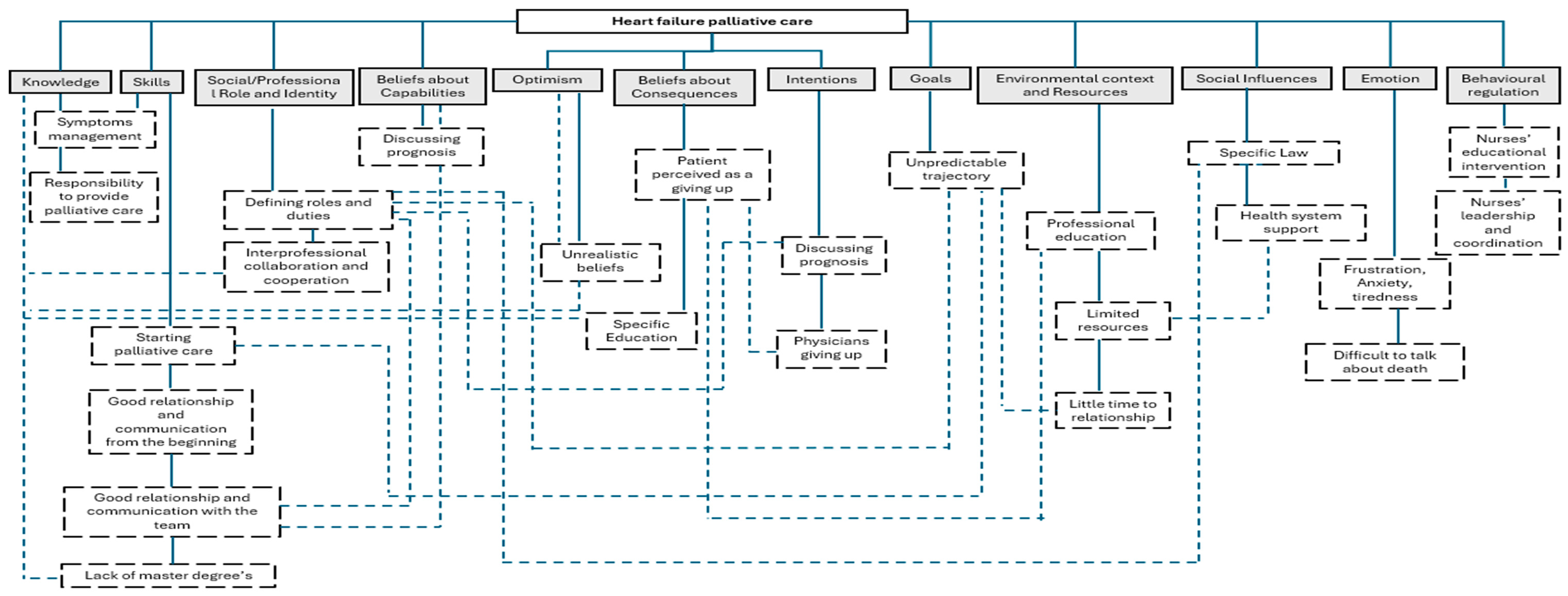
Finally, due to the importance of palliative care intervention implementation to reduce barriers, avoid negative feelings and foster good practice, we have elaborated a flowchart based on the results (Figure 3). This flowchart attempts to summarize TDF elements, showing strict internal correlations.
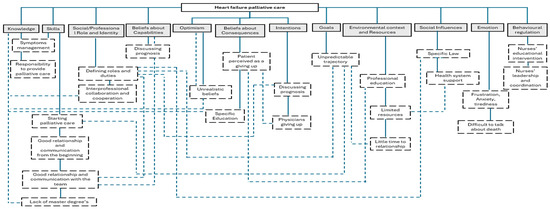
Figure 3.
Summary flowchart of main topics. Legend: solid lines TDF identified, dashed lines findings and correlations between TDF domains.
The flowchart helps us to understand that acting on an element may have a positive impact on the correlated ones. Some main themes and recurrent issues emerged from our results. Knowledge, education and communication concern all TDF domains addressed by nurses’ attitudes and perceptions. They may be considered associated with the capability, opportunity and motivation components of the target ideal behavior [27]. The TDF framework enables us to have a clear view of nurses’ attitudes and perceptions, allowing us to categorize and closely analyze the results. Behavioral change in clinical practice should, in fact, begin with an analysis of which elements could influence them to explain implementation problems and construct implementation interventions. Improvements in knowledge, communication and education could have a positive impact on other potential barriers, such as the unpredictable course of the disease and differences in patients’ symptom burdens in progressive heart failure stages.
As described by WHO (2021) [68], palliative care is a human right and a moral imperative that should not be neglected. Implementation helps improve the quality of life of people who are dealing with the challenges posed by life-threatening illnesses.
Strenghs and Limitations
It is fundamental to underline that it was not possible in our analysis to distinguish interventions and attitudes according to the heart failure stage, since the studies did not clearly specify it. Transplant and left ventricular assistance device (LVAD) patients were not considered due to the specific interventions needed. Other specific reviews may be useful in enriching the results obtained.
We acknowledge heterogeneity in study design and intervention type. Consequently, we adopted a convergent-integrated design. This method allows us to generate a deeper understanding of the topic from multiple points of view. Regarding this aspect, it is important to think about it as a limitation, but also as a strength. Nevertheless, it is important to be careful in forming the results and generalizations due to the different study methodologies and quality appraisal levels.
Language restrictions (English or Italian) should also be considered, as the vast majority of articles are now published in the English language.
5. Conclusions
Nurses’ attitudes and perceptions towards heart failure palliative care are characterized by many influences and behaviors that are strictly correlated with one another. Communication, knowledge and education emerged as important topics that influence palliative care implemantation. Palliative care among the heart failure population is recognized as important, but misconceptions and a lack of knowledge primarily on the part of patients and clinicians may exist. As such, the risk of hindering the real impact of palliative care is present. Evidence has indicated that nurses’ contributions, with educational interventions and leadership, improve patients’ outcomes and palliative care implementation. As researchers and practitioners, we must consider the complexity of such types of care, illnesses and elements involved. Understanding the correlation between factors that can influence palliative care implementation, as we have tried to underline, may help us to understand the starting point for improving heart failure palliative care implementation.
Author Contributions
Conceptualisation, D.C. (Dalia Caleffi) and P.F.; Data Curation, D.C. (Dalia Caleffi), P.F., S.A., S.R., M.C.B., H.H., I.S. and D.C. (Domenico Cannizzaro); Methodology, D.C. (Dalia Caleffi), P.F., S.A., S.R. and M.C.B.; Formal Analysis, D.C. (Dalia Caleffi), P.F., H.H., I.S. and D.C. (Domenico Cannizzaro); Investigation, D.C. (Dalia Caleffi), Resources D.C. (Dalia Caleffi), P.F., S.A. and M.C.B.; Writing—Original Draft Preparation, D.C. (Dalia Caleffi) and P.F.; Writing—Review and Editing, D.C. (Dalia Caleffi), P.F., S.A., S.R., M.C.B., H.H., I.S. and D.C. (Domenico Cannizzaro); Visualisation, D.C. (Dalia Caleffi), P.F., S.A., S.R., M.C.B., H.H., I.S. and D.C. (Domenico Cannizzaro); Validation D.C. (Dalia Caleffi), P.F., S.A., S.R. and M.C.B.; Supervision, D.C. (Dalia Caleffi), P.F., S.A., S.R. and M.C.B.; Project Administration, D.C. (Dalia Caleffi), P.F. and M.C.B. All authors approved the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review was not required for this systematic review of previously published works.
Informed Consent Statement
Patient consent was not required for this systematic review of previously published works.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Acknowledgments
We would like to thank Orianna Raggioli and Irene Caleffi for the English revision.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ESC | European Society of Cardiology |
| LVAD | Left ventricular assistance device |
| JBI | Joanna Briggs Institute |
| PRISMA | Preferred Reported Items for Systematic review and Meta-analysis |
| QL | Qualitative |
| QT | Quantitative |
| TDF | Theoretical domains framework |
| WHO | World Health Organization |
References
- Bagheri, I.; Yousefi, H.; Bahrami, M.; Shafie, D. Quality of Palliative Care Guidelines in Patients with Heart Failure: A Systematic Review of Quality Appraisal using AGREE II Instrument. Indian J. Palliat. Care 2022, 29, 7–14. [Google Scholar] [CrossRef]
- Singh, G.K.; Davidson, P.M.; Macdonald, P.S.; Newton, P.J. The Perspectives of Health Care Professionals on Providing End of Life Care and Palliative Care for Patients With Chronic Heart Failure: An Integrative Review. Heart Lung Circ. 2019, 28, 539–552. [Google Scholar] [CrossRef]
- Romanò, M. Barriers to Early Utilization of Palliative Care in Heart Failure: A Narrative Review. Healthcare 2020, 8, 36. [Google Scholar] [CrossRef] [PubMed]
- ALHosni, F.; Al Qadire, M.; Omari, O.A.; Al Raqaishi, H.; Khalaf, A. Symptom prevalence, severity, distress and management among patients with chronic diseases. BMC Nurs. 2023, 22, 155. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Palliative Care: Key Fact. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/palliative-care (accessed on 29 December 2024).
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Ahmad, T.; Alexander, K.M.; Baker, W.L.; Bosak, K.; Breathett, K.; Fonarow, G.C.; Heidenreich, P.; Ho, J.E.; Hsich, E.; et al. Heart Failure Epidemiology and Outcomes Statistics: A Report of the Heart Failure Society of America. J. Card. Fail. 2023, 29, 1412–1451. [Google Scholar] [CrossRef]
- Alnajar, M.; Darawad, M.; Khater, W.; Alshahwan, R.; Mosleh, S.; Nofal, B.; Abdalrahim, M. Exploring Palliative Care Needs Among Patients With Cancer and Non-Cancer Serious Chronic Diseases: A Comparison Study. Am. J. Hosp. Palliat. Med. 2025, 42, 20–31. [Google Scholar] [CrossRef]
- Diop, M.S.; Rudolph, J.L.; Zimmerman, K.M.; Richter, M.A.; Skarf, L.M. Palliative Care Interventions for Patients with Heart Failure: A Systematic Review and Meta-Analysis. J. Palliat. Med. 2017, 20, 84–92. [Google Scholar] [CrossRef]
- Hicks, S.; Davidson, M.; Efstathiou, N.; Guo, P. Effectiveness and cost effectiveness of palliative care interventions in people with chronic heart failure and their caregivers: A systematic review. BMC Palliat. Care 2022, 21, 205. [Google Scholar] [CrossRef]
- Ament, S.M.; Couwenberg, I.M.; Boyne, J.J.; Kleijnen, J.; Stoffers, H.E.; Van Den Beuken, M.H.; Engels, Y.; Bellersen, L.; Janssen, D.J. Tools to help healthcare professionals recognize palliative care needs in patients with advanced heart failure: A systematic review. Palliat. Med. 2021, 35, 45–58. [Google Scholar] [CrossRef]
- Doherty, L.C.; Fitzsimons, D.; McIlfatrick, S.J. Carers’ needs in advanced heart failure: A systematic narrative review. Eur. J. Cardiovasc. Nurs. 2016, 15, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Joberns, L. Nurse opportunities to overcome barriers to palliative care provision for patients with heart failure: An integrative review. Br. J. Card. Nurs. 2021, 16, 1–15. [Google Scholar] [CrossRef]
- Hagan, T.L.; Xu, J.; Lopez, R.P.; Bressler, T. Nursing’s role in leading palliative care: A call to action. Nurse Educ. Today 2018, 61, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Getie, A.; Ayalneh, M.; Aytenew, T.M.; Bimerew, M.; Wondmieneh, A. Attitude of nurses towards palliative care and its associated factors in Ethiopia, systematic review and meta-analysis. BMC Palliat. Care 2024, 23, 67. [Google Scholar] [CrossRef] [PubMed]
- Harden, K.; Price, D.; Duffy, E.; Galunas, L.; Rodgers, C. Palliative Care: Improving Nursing Knowledge, Attitudes, and Behaviors. Clin. J. Oncol. Nurs. 2017, 21, E232–E238. [Google Scholar] [CrossRef]
- Sekse, R.J.T.; Hunskår, I.; Ellingsen, S. The nurse’s role in palliative care: A qualitative meta-synthesis. J. Clin. Nurs. 2018, 27, e21–e38. Available online: https://onlinelibrary.wiley.com/doi/10.1111/jocn.13912 (accessed on 29 December 2024). [CrossRef]
- Lizarondo, L.; Stern, C.; Carrier, J.; Godfrey, C.; Rieger, K.; Salmond, S.; Apostolo, J.; Kirkpatrick, P.; Loveday, H. Chapter 8: Mixed methods systematic reviews (2020). In JBI Manual for Evidence Synthesis; Aromataris, E., Lockwood, C., Porritt, K., Pilla, B., Jordan, Z., Eds.; JBI: Adelaide, Australia, 2024; Available online: https://synthesismanual.jbi.global (accessed on 29 December 2024).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLOS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Johnson, N.; Phillips, M. Rayyan for systematic reviews. J. Electron. Resour. Librariansh. 2018, 30, 46–48. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Tufanaru, C.; Leonardi-Bee, J.; Aromataris, E.; Munn, Z. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evid. Synth. 2023, 21, 494–506. Available online: https://journals.lww.com/10.11124/JBIES-22-00430 (accessed on 29 December 2024). [CrossRef]
- Aromataris, E.; Munn, Z. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Munn, Z.; Moola, S.; Lisy, K.; Riitano, D.; Tufanaru, C. Chapter 5: Systematic reviews of prevalence and incidence. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 29 December 2024).
- Lockwood, C.; Munn, Z.; Porritt, Z. Qualitative research synthesis: Methodological guidance for systematic reviewers utilizing meta-aggregation. Int. J. Evid. Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef]
- Aiken, L.S.; Butner, J.; Lockhart, C.A.; Volk-Craft, B.E.; Hamilton, G.; Williams, F.G. Outcome Evaluation of a Randomized Trial of the PhoenixCare Intervention: Program of Case Management and Coordinated Care for the Seriously Chronically Ill. J. Palliat. Med. 2006, 9, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Bakitas, M.A.; Dionne-Odom, J.N.; Ejem, D.B.; Wells, R.; Azuero, A.; Stockdill, M.L.; Keebler, K.; Sockwell, E.; Tims, S.; Engler, S.; et al. Effect of an Early Palliative Care Telehealth Intervention vs Usual Care on Patients With Heart Failure: The ENABLE CHF-PC Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1203–1213. [Google Scholar] [CrossRef]
- Bekelman, D.B.; Feser, W.; Morgan, B.; Welsh, C.H.; Parsons, E.C.; Paden, G.; Baron, A.; Hattler, B.; McBryde, C.; Cheng, A.; et al. Nurse and Social Worker Palliative Telecare Team and Quality of Life in Patients With COPD, Heart Failure, or Interstitial Lung Disease: The ADAPT Randomized Clinical Trial. JAMA 2024, 331, 212. [Google Scholar] [CrossRef] [PubMed]
- Mirshahi, A.; Bakitas, M.; Khoshavi, M.; Khanipour-Kencha, A.; Riahi, S.M.; Wells, R.; Odom, J.N.; Ghiyasvandian, S.; Zakerimoghadam, M. The impact of an integrated early palliative care telehealth intervention on the quality of life of heart failure patients: A randomized controlled feasibility study. BMC Palliat. Care 2024, 23, 22. [Google Scholar] [CrossRef]
- Ng, A.Y.M.; Wong, F.K.Y. Effects of a Home-Based Palliative Heart Failure Program on Quality of Life, Symptom Burden, Satisfaction and Caregiver Burden: A Randomized Controlled Trial. J. Pain Symptom Manag. 2018, 55, 1–11. [Google Scholar] [CrossRef]
- Rogers, J.G.; Patel, C.B.; Mentz, R.J.; Granger, B.B.; Steinhauser, K.E.; Fiuzat, M.; Adams, P.A.; Speck, A.; Johnson, K.S.; Krishnamoorthy, A.; et al. Palliative Care in Heart Failure. J. Am. Coll. Cardiol. 2017, 70, 331–341. [Google Scholar] [CrossRef]
- Wong, F.K.Y.; Ng, A.Y.M.; Lee, P.H.; Lam, P.; Ng, J.S.C.; Ng, N.H.Y.; Sham, M.M.K. Effects of a transitional palliative care model on patients with end-stage heart failure: A randomised controlled trial. Heart 2016, 102, 1100–1108. [Google Scholar] [CrossRef]
- Akbarian-Rokni, M.; Mardani-Hamooleh, M.; Abbasi, M.; Seyedfatemi, N.; Pezaro, S. Nurses’ perceptions of the challenges involved in providing of end-of-life care to people with heart failure: A context-based study. BMC Palliat. Care 2023, 22, 180. [Google Scholar] [CrossRef]
- Borbasi, S.; Wotton, K.; Redden, M.; Champan, Y. Letting go: A qualitative study of acute care and community nurses’ perceptions of a ‘good’ versus a ‘bad’ death. Aust. Crit. Care 2005, 18, 104–113. [Google Scholar] [CrossRef]
- Brännström, M.; Brulin, C.; Norberg, A.; Boman, K.; Strandberg, G. Being a Palliative Nurse for Persons with Severe Congestive Heart Failure in Advanced Homecare. Eur. J. Cardiovasc. Nurs. 2005, 4, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Browne, S.; Macdonald, S.; May, C.R.; Macleod, U.; Mair, F.S. Patient, Carer and Professional Perspectives on Barriers and Facilitators to Quality Care in Advanced Heart Failure. Harris F, curatore. PLoS ONE 2014, 9, e93288. [Google Scholar] [CrossRef]
- Fairlamb, H.J.; Murtagh, F.E.M. Health professionals’ perceptions of palliative care for end-stage cardiac and respiratory conditions: A qualitative interview study. BMC Palliat. Care 2021, 20, 103. [Google Scholar] [CrossRef] [PubMed]
- Gholami Motlagh, F.; Nobahar, M.; Bahrami, M. Barriers and Facilitators of Palliative Care in Older Adults With Heart Failure: A Qualitative Content Analysis. J. Palliat. Care 2024, 39, 271–281. [Google Scholar] [CrossRef]
- Glogowska, M.; Simmonds, R.; McLachlan, S.; Cramer, H.; Sanders, T.; Johnson, R.; Kadam, U.T.; Lasserson, D.S.; Purdy, S. “Sometimes we can’t fix things”: A qualitative study of health care professionals’ perceptions of end of life care for patients with heart failure. BMC Palliat. Care 2016, 15, 3. [Google Scholar] [CrossRef]
- Hjelmfors, L.; Strömberg, A.; Friedrichsen, M.; Mårtensson, J.; Jaarsma, T. Communicating prognosis and end-of-life care to heart failure patients: A survey of heart failure nurses’ perspectives. Eur. J. Cardiovasc. Nurs. 2014, 13, 152–161. [Google Scholar] [CrossRef]
- O’Hanlon, D.; Harding, R. Are specialist heart failure nurses currently able to provide palliative care to their patients? Prog. Palliat. Care 2011, 19, 165–171. [Google Scholar] [CrossRef]
- Singh, G.K.; Ramjan, L.; Ferguson, C.; Davidson, P.M.; Newton, P.J. Access and referral to palliative care for patients with chronic heart failure: A qualitative study of healthcare professionals. J. Clin. Nurs. 2020, 29, 1576–1589. [Google Scholar] [CrossRef]
- Stocker, R.; Close, H.; Hancock, H.; Hungin, A.P.S. Should heart failure be regarded as a terminal illness requiring palliative care? A study of heart failure patients’, carers’ and clinicians’ understanding of heart failure prognosis and its management. BMJ Support. Palliat. Care 2017, 7, 464–469. [Google Scholar] [CrossRef]
- Wotton, K.; Borbasi, S.; Redden, M. When All Else Has Failed: Nurses’ Perception of Factors Influencing Palliative Care for Patients With End-Stage Heart Failure. J. Cardiovasc. Nurs. 2005, 20, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Ziehm, J.; Farin, E.; Seibel, K.; Becker, G.; Köberich, S. Health care professionals’ attitudes regarding palliative care for patients with chronic heart failure: An interview study. BMC Palliat. Care 2016, 15, 76. [Google Scholar] [CrossRef]
- Bharani, A.; Mehta, A.; Hiensch, K.; Zeng, L.; Lala, A.; Pinney, S.; Goldstein, N.; Chai, E.; Gelfman, L.P. Referral Versus Embedded Palliative Care Consultation Among People Hospitalized With Heart Failure: A Report From a Single Center Pilot Program. J. Pain Symptom Manag. 2024, 67, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Barrett, M.; Connaire, K. A palliative care approach in heart failure: Knowledge and attitudes of cardiac nurses. Br. J. Card. Nurs. 2016, 11, 136–142. [Google Scholar] [CrossRef]
- Kim, S.; Lee, K.; Kim, S. Knowledge, attitude, confidence, and educational needs of palliative care in nurses caring for non-cancer patients: A cross-sectional, descriptive study. BMC Palliat. Care 2020, 19, 105. [Google Scholar] [CrossRef]
- Pattenden, J.F.; Mason, A.R.; Lewin, R.J.P. Collaborative palliative care for advanced heart failure: Outcomes and costs from the ‘Better Together’ pilot study. BMJ Support. Palliat. Care 2013, 3, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Ferguson, C.; Davidson, P.M.; Newton, P.J. Attitudes and practices towards palliative care in chronic heart failure: A survey of cardiovascular nurses and physicians. Contemp. Nurse 2021, 57, 113–127. [Google Scholar] [CrossRef]
- Turrise, S.; Jenkins, C.A.; Arms, T.; Jones, A.L. Palliative Care Conversations for Heart Failure Nurses: A Pilot Education Intervention. SAGE Open Nurs. 2021, 7, 23779608211044592. [Google Scholar] [CrossRef]
- Schallmo, M.K.; Dudley-Brown, S.; Davidson, P.M. Healthcare Providers’ Perceived Communication Barriers to Offering Palliative Care to Patients With Heart Failure: An Integrative Review. J. Cardiovasc. Nurs. 2019, 34, E9–E18. [Google Scholar] [CrossRef]
- Alpert, C.M.; Smith, M.A.; Hummel, S.L.; Hummel, E.K. Symptom burden in heart failure: Assessment, impact on outcomes, and management. Heart Fail. Rev. 2017, 22, 25–39. [Google Scholar] [CrossRef]
- Oishi, A.; Murtagh, F.E. The challenges of uncertainty and interprofessional collaboration in palliative care for non-cancer patients in the community: A systematic review of views from patients, carers and health-care professionals. Palliat. Med. 2014, 28, 1081–1098. [Google Scholar] [CrossRef]
- LeBlanc, T.W.; Temel, J.S.; Helft, P.R. “How Much Time Do I Have?”: Communicating Prognosis in the Era of Exceptional Responders. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 787–794. [Google Scholar] [CrossRef]
- Gebresillassie, B.M.; Attia, J.R.; Mersha, A.G.; Harris, M.L. Prognostic models and factors identifying end-of-life in non-cancer chronic diseases: A systematic review. BMJ Support. Palliat. Care 2024, 14, e2316–e2329. [Google Scholar] [CrossRef] [PubMed]
- NHS. Addressing Palliative and End of Life Care Needs for People Living with Heart Failure: A Revised Framework for Integrated Care Systems. NHS England. 2023. Available online: https://www.england.nhs.uk/long-read/addressing-palliative-and-end-of-life-care-needs-for-people-living-with-heart-failure/ (accessed on 29 December 2024).
- Shropshire, S.J.; Fabbri, M.; Manemann, S.M.; Roger, V.L.; Killian, J.M.; Weston, S.A.; Chamberlain, A.M. Patient Awareness of Heart Failure Diagnosis: A Community Study. J. Am. Heart Assoc. 2023, 12, e029284. [Google Scholar] [CrossRef]
- Kałużna-Oleksy, M.; Wawrzyniak, M.; Klimkowska, M.; Dudek, M.; Migaj, J.; Straburzyńska-Migaj, E. Awareness of heart failure and perception of the problem in the general population. Cardiovasc. J. Afr. 2022, 33, 18–23. [Google Scholar] [CrossRef]
- Burnier, M. The role of adherence in patients with chronic diseases. Eur. J. Intern. Med. 2024, 119, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Waller, A.; Girgis, A.; Davidson, P.M.; Newton, P.J.; Lecathelinais, C.; Macdonald, P.S.; Hayward, C.S.; Currow, D.C. Facilitating Needs-Based Support and Palliative Care for People With Chronic Heart Failure: Preliminary Evidence for the Acceptability, Inter-Rater Reliability, and Validity of a Needs Assessment Tool. J. Pain Symptom Manag. 2013, 45, 912–925. [Google Scholar] [CrossRef] [PubMed]
- Ferri, P.; Alberti, S.; Di Lorenzo, R.; Caleffi, D.; Rubbi, I.; Artioli, G.; Rovesti, S.; Saguatti, I. Improving quality of end-of-life education: Results of a composite educational intervention on nursing students’ attitudes toward care of dying patients. Acta Biomed. Atenei Parm. 2024, 95, e2024163. [Google Scholar] [CrossRef]
- Cain, C.L.; Surbone, A.; Elk, R.; Kagawa-Singer, M. Culture and Palliative Care: Preferences, Communication, Meaning, and Mutual Decision Making. J. Pain Symptom Manag. 2018, 55, 1408–1419. [Google Scholar] [CrossRef]
- Ezer, T.; Burke-Shyne, N.; Hepford, K. Legal Support for Palliative Care Patients. J. Pain Symptom Manag. 2018, 55, S157–S162. [Google Scholar] [CrossRef]
- Osei, E.; Lee, D.H.; Kim, S.Y. Comparison of legislation, regulations, and national health policies for palliative care in three East Asian countries: A review of the literature. J. Glob. Health Sci. 2022, 4, e3. [Google Scholar] [CrossRef]
- World Health Organization. WHO Takes Steps to Address Glaring Shortage of Quality Palliative Care Services. 2021. Available online: https://www.who.int/news/item/05-10-2021-who-takes-steps-to-address-glaring-shortage-of-quality-palliative-care-services (accessed on 29 December 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).