
Validation and Clinical Application of a Developed Pedal Coordination Assessment Device for Older Drivers


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
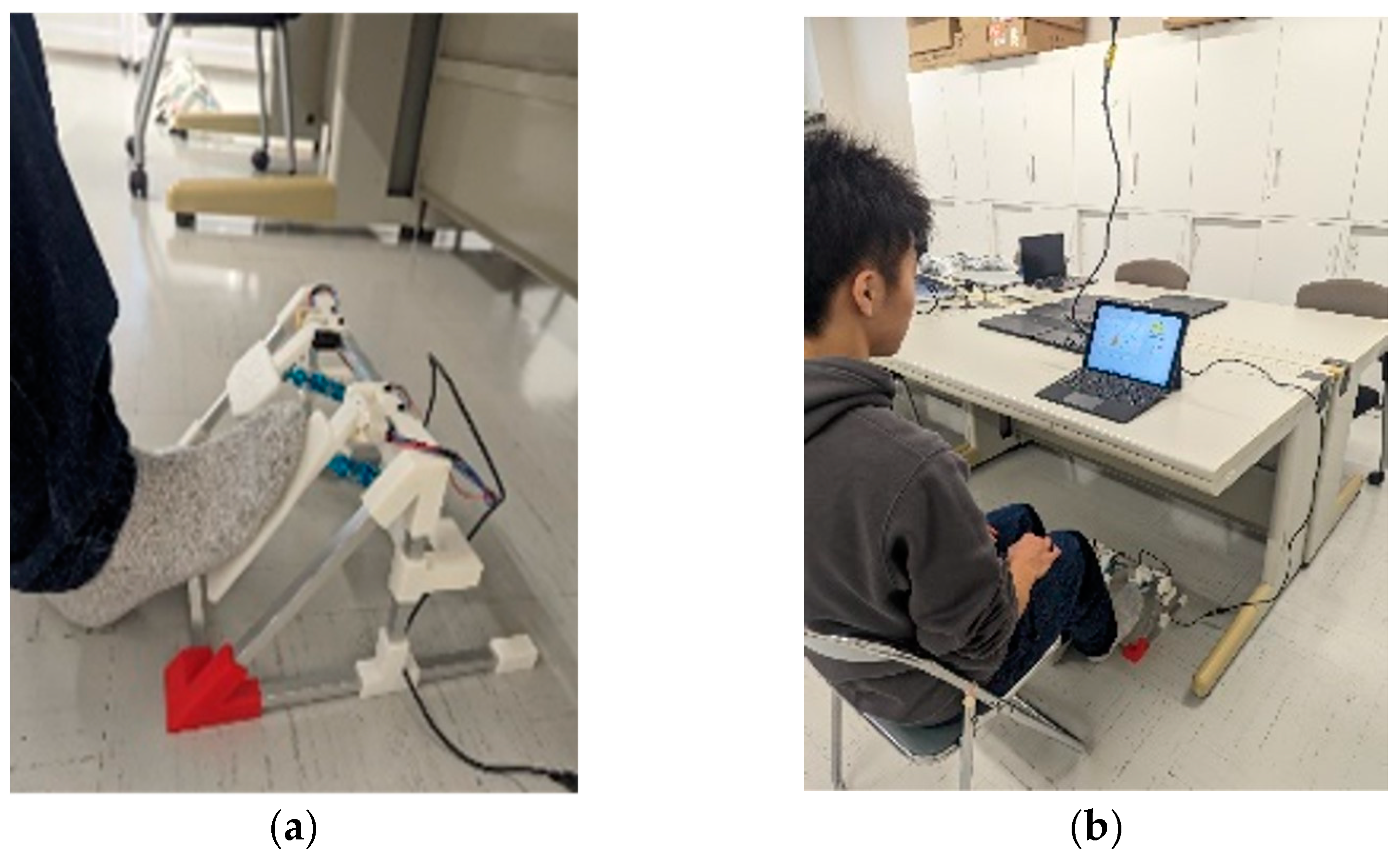
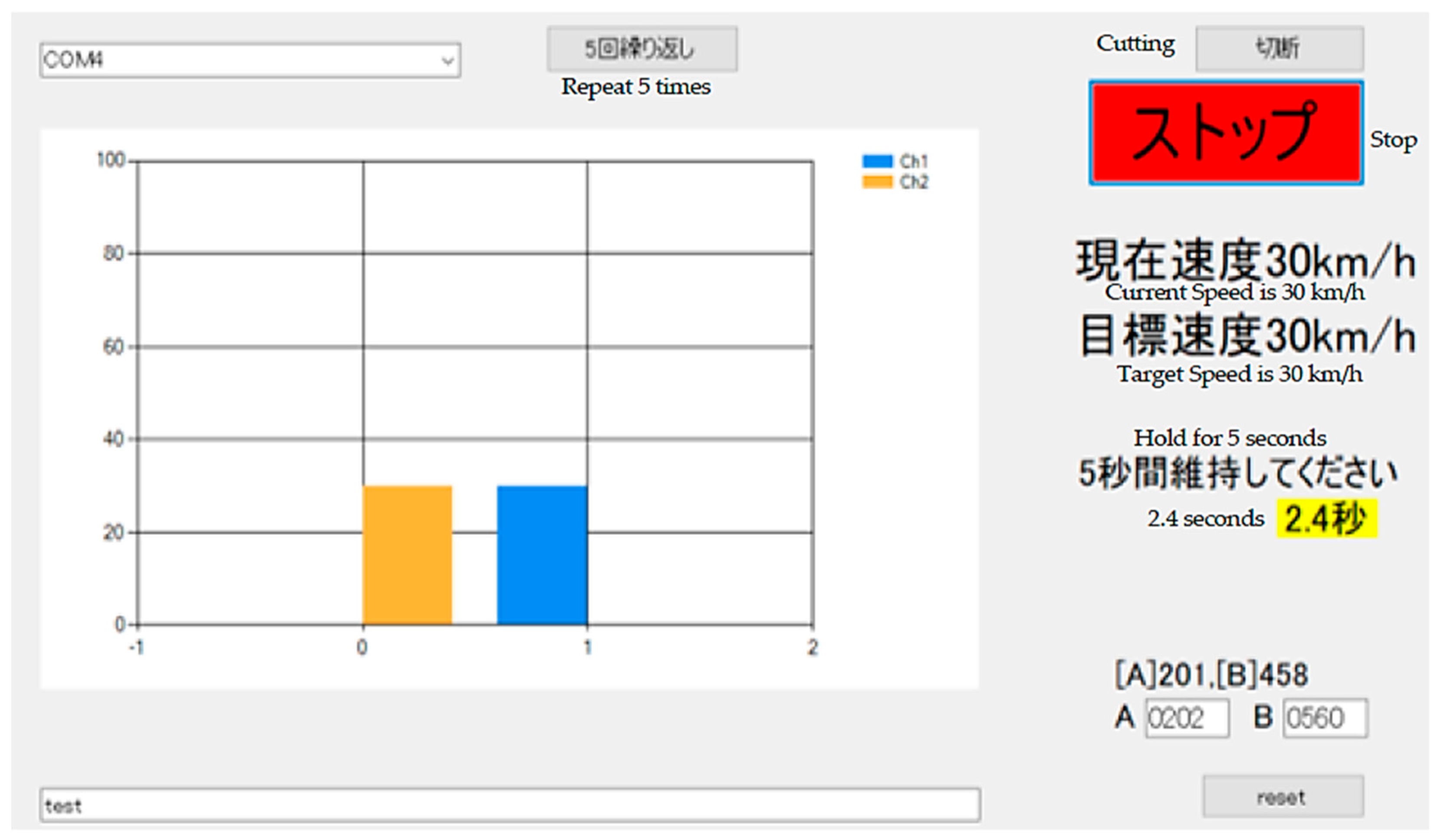
2.2. Pedal Coordination Assessment Device
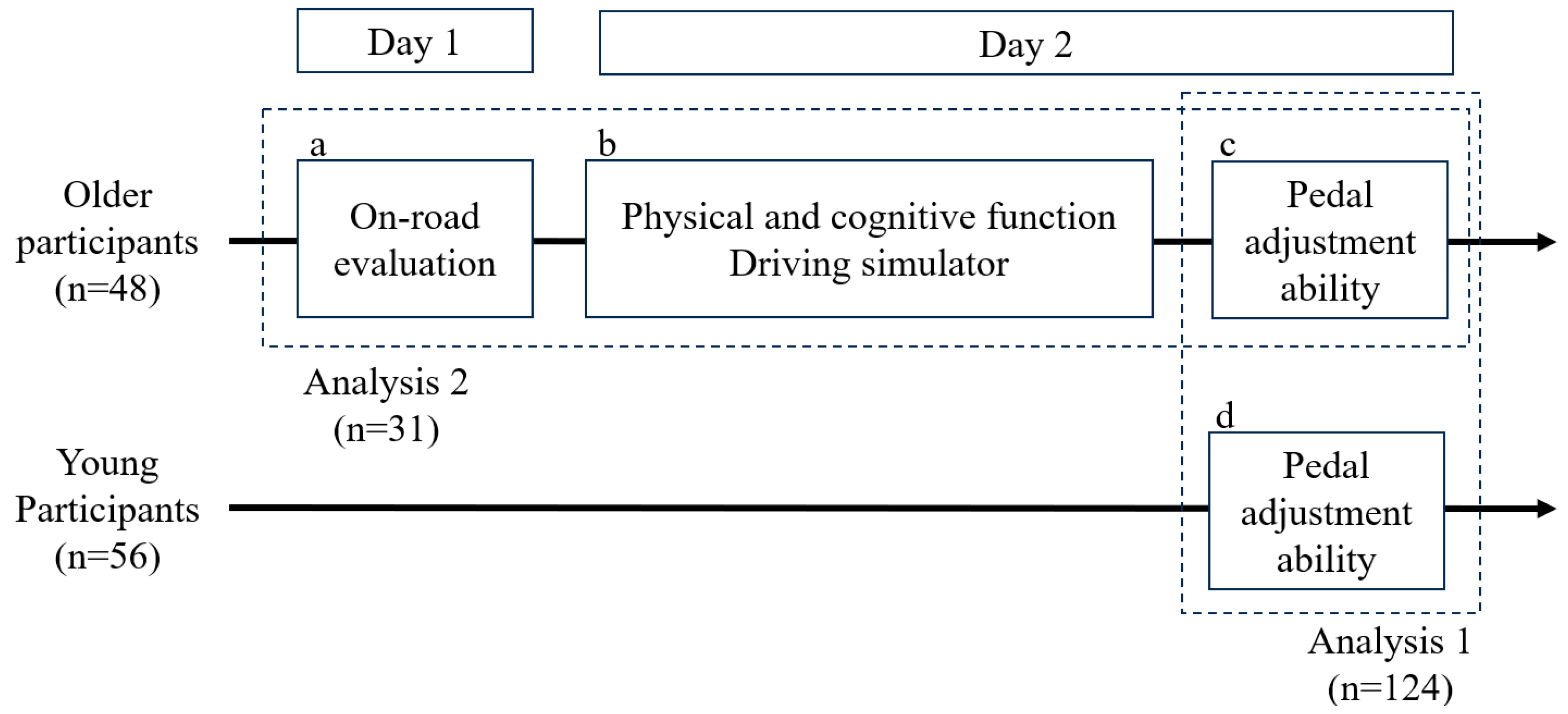
2.3. Procedure
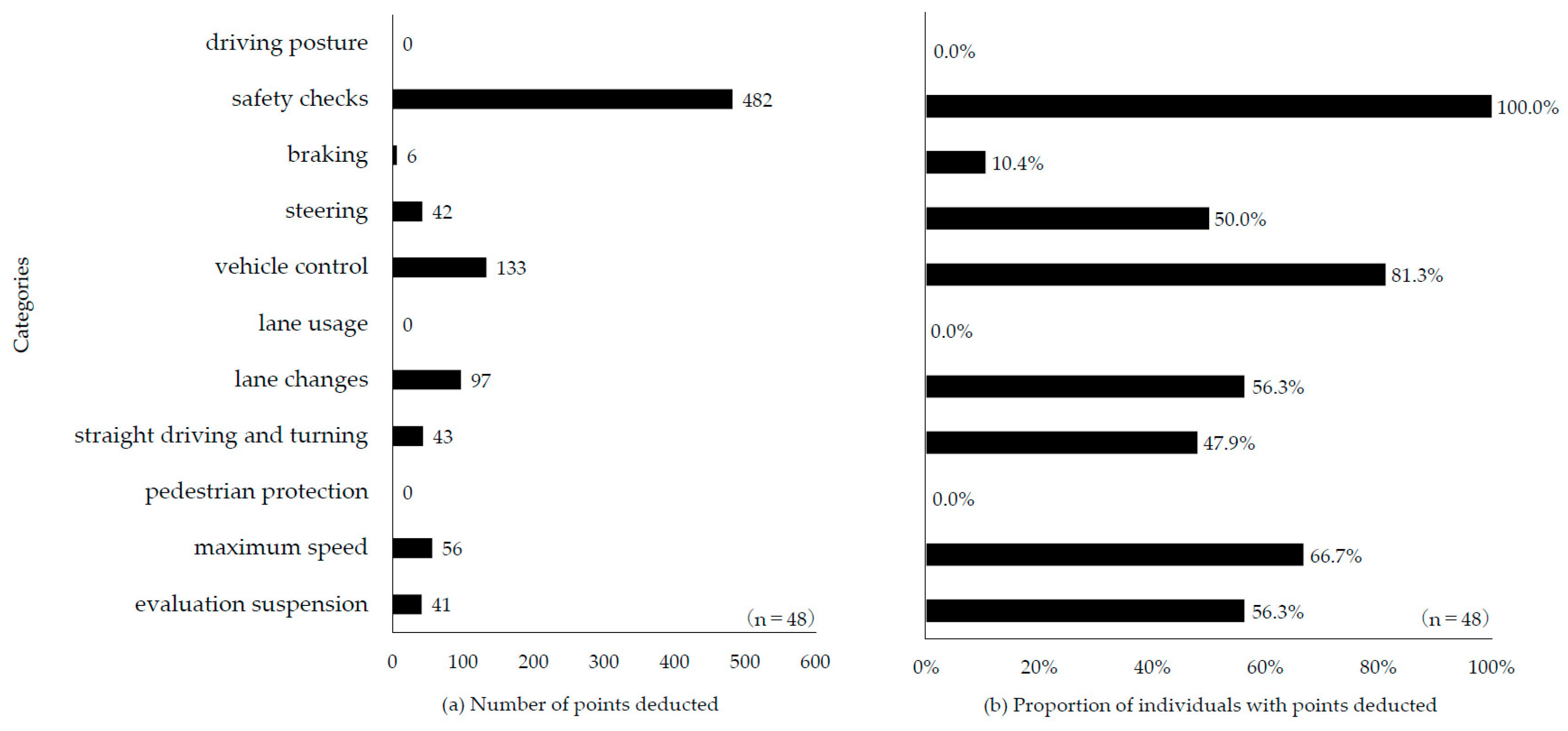
- Driving posture—e.g., the driver’s body is not facing forward in alignment with the steering wheel.
- Safety checks—e.g., failure to directly check surroundings when starting or changing lanes or failure to signal when turning.
- Braking—e.g., not moving the foot to the brake pedal despite road conditions requiring deceleration.
- Steering—e.g., noticeable wavering while driving.
- Vehicle control—e.g., inability to position the vehicle appropriately to avoid potential collisions with bicycles or motorcycles approaching from behind when making a left turn.
- Lane usage—e.g., driving in prohibited areas.
- Lane changes—e.g., failing to move the vehicle toward the left side of the lane several meters before making a left turn.
- Straight driving and turning—e.g., failing to decelerate appropriately when making right or left turns.
- Pedestrian protection—e.g., obstructing pedestrians attempting to cross the road.
- Maximum speed—e.g., exceeding the posted speed limit.
- Evaluation suspension—e.g., failing to comply with a stop sign.
2.4. Analysis
3. Results
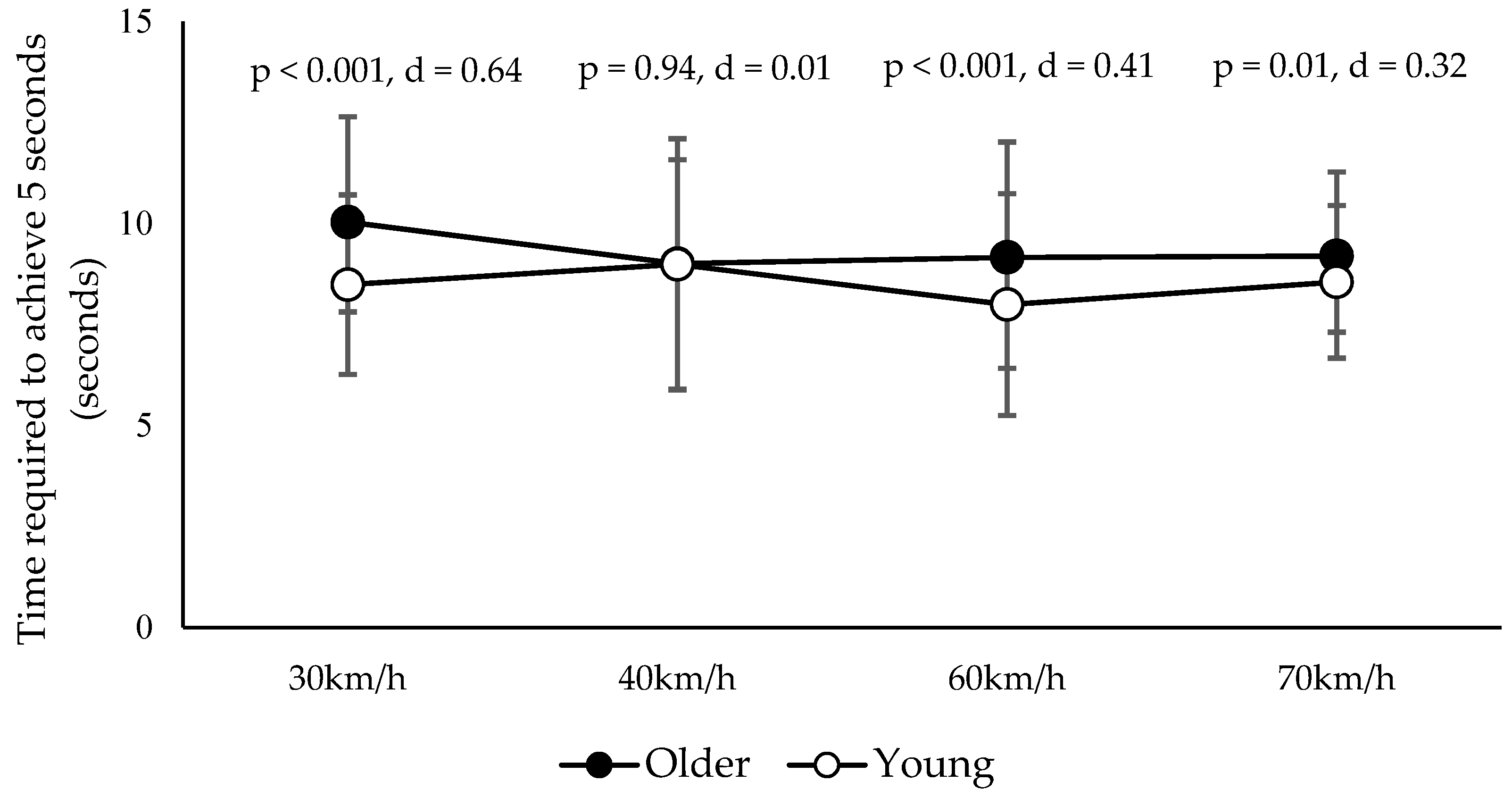
3.1. Pedal Adjustment Ability
3.2. Correlation Between Pedal Adjustment Ability and Physical, Cognitive, and Driving Ability
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- World Health Organization (WHO). Global Status Report on Road Safety 2023. Available online: https://www.who.int/teams/social-determinants-of-health/safety-and-mobility/global-status-report-on-road-safety-2023 (accessed on 20 February 2025).
- Bucsuhazy, K.; Matuchova, E.; Zuvala, R.; Moravcova, P.; Kostikova, M.; Mikulec, R. Human factors contributing to the road traffic accident occurrence. Transp. Res. Procedia 2020, 45, 555–561. [Google Scholar] [CrossRef]
- Lombardi, M.; Mauro, F.; Berardi, D.; Galuppi, M. Occupational road safety management: A preliminary insight for a landfill remediation site. Buildings 2023, 13, 1238. [Google Scholar] [CrossRef]
- Klinjun, N.; Kelly, M.; Praditsathaporn, C.; Petsirasan, R. Identification of factors affecting road traffic injuries incidence and severity in South Thailand based on accident investigation reports. Sustainability 2021, 13, 12467. [Google Scholar] [CrossRef]
- World Health Organization (WHO). New Political Declaration to Halve Road Traffic Deaths and Injuries by 2030 Is a Milestone Achievement. 2022. Available online: https://www.who.int/news/item/30-06-2022-new-political-declaration-to-halve-road-traffic-deaths-and-injuries-by-2030-is-a-milestone-achievement (accessed on 20 February 2025).
- Marottoli, R.A.; Allore, H.; Araujo, K.L.; Iannone, L.P.; Acampora, D.; Gottschalk, M.; Charpentier, P.; Kasl, S.; Peduzzi, P. A randomized trial of a physical conditioning program to enhance the driving performance of older persons. J. Gen. Intern. Med. 2007, 22, 590–597. [Google Scholar] [CrossRef]
- Cuenen, A.; Jongen, E.M.; Brijs, T.; Brijs, K.; Houben, K.; Wets, G. Effect of a working memory training on aspects of cognitive ability and driving ability of older drivers: Merits of an adaptive training over a non-adaptive training. Transp. Res. Part F Traffic Psychol. Behav. 2016, 42, 15–27. [Google Scholar] [CrossRef]
- Roge, J.; Ndiaye, D.; Vienne, F. Useful visual field training: A way to improve elderly car drivers’ ability to detect vulnerable road users. Transp. Res. Part F Traffic Psychol. Behav. 2014, 26, 246–257. [Google Scholar] [CrossRef]
- Owsley, C.; Stalvey, B.T.; Phillips, J.M. The efficacy of an educational intervention in promoting self-regulation among high-risk older drivers. Accid. Anal. Prev. 2003, 35, 393–400. [Google Scholar] [CrossRef]
- Anstey, K.J.; Eramudugolla, R.; Kiely, K.M.; Price, J. Effect of tailored on-road driving lessons on driving safety in older adults: A randomised controlled trial. Accid. Anal. Prev. 2018, 115, 1–10. [Google Scholar] [CrossRef]
- Fausto, B.A.; Maldonado, P.F.A.; Ross, L.A.; Lavalliere, M.; Edwards, J.D. A systematic review and meta-analysis of older driver interventions. Accid. Anal. Prev. 2021, 149, 105852. [Google Scholar] [CrossRef]
- Lee, J.; Itoh, M. Effects of driver compensatory behaviour on risks of critical pedestrian collisions under simulated visual field defects. PLoS ONE 2020, 15, e0231130. [Google Scholar] [CrossRef]
- Ichikawa, M.; Inada, H.; Nakahara, S. Revisiting older drivers’ risks of at-fault motor vehicle collisions in Japan. J. Epidemiol. 2024, 34, 295–300. [Google Scholar] [CrossRef]
- Arora, C.; Frantz, C.; Toglia, J. Awareness of performance on a functional cognitive performance-based assessment across the adult life span. Front. Psychol. 2021, 12, 753016. [Google Scholar] [CrossRef]
- Davis, R.; Owens, M. Self-regulation of driving behaviors in persons with early-stage Alzheimer’s disease. J. Gerontol. Nurs. 2021, 47, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Meng, A.; Siren, A. Cognitive problems, self-rated changes in driving skills, driving-related discomfort and self-regulation of driving in older drivers. Accid. Anal. Prev. 2012, 49, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Hird, M.A.; Vetivelu, A.; Saposnik, G.; Schweizer, T.A. Cognitive, on-road, and simulator-based driving assessment after stroke. J. Stroke Cerebrovasc. Dis. 2014, 23, 2654–2670. [Google Scholar] [CrossRef] [PubMed]
- Meguro, K.; Kumai, K. Lower extremities task of pressing an “accelerator” or a “brake”: Association with traffic accidents in older drivers—A preliminary study. Dement. Neuropsychol. 2022, 16, 475–480. [Google Scholar] [CrossRef]
- Moran, C.; Bennett, J.M.; Prabhakharan, P. Road user hazard perception tests: A systematic review of current methodologies. Accid. Anal. Prev. 2019, 129, 309–333. [Google Scholar] [CrossRef]
- Willstrand, T.D.; Broberg, T.; Selander, H. Driving characteristics of older drivers and their relationship to the useful field of view test. Gerontology 2016, 32, 180–188. [Google Scholar] [CrossRef]
- Vaucher, P.; Herzig, D.; Cardoso, I.; Herzog, M.H.; Mangin, P.; Favrat, B. The trail making test as a screening instrument for driving performance in older drivers: A translational research. BMC Geriatr. 2014, 14, 123. [Google Scholar] [CrossRef]
- Gaines, J.M.; Burke, K.L.; Marx, K.A.; Wagner, M.; Parrish, J.M. Enhancing older driver safety: A driving survey and evaluation of the Carfit program. J. Safety Res. 2011, 42, 351–358. [Google Scholar] [CrossRef]
- Liddle, J.; Haynes, M.; Pachana, N.A.; Mitchell, G.; McKenna, K.; Gustafsson, L. Effect of a group intervention to promote older adults’ adjustment to driving cessation on community mobility: A randomized controlled trial. Gerontologist 2013, 54, 409–422. [Google Scholar] [CrossRef]
- Lodha, N.; Moon, H.; Kim, C.; Onushko, T.; Christou, E.A. Motor output variability impairs driving ability in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1676–1681. [Google Scholar] [CrossRef] [PubMed]
- Yuda, E.; Yoshida, Y.; Ueda, N.; Kaneko, I.; Miura, Y.; Hayano, J. Effects of aging on foot pedal responses to visual stimuli. J. Physiol. Anthropol. 2020, 39, 3. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Weaver, B.; Ruberte, L.; Khan, F.; Arndt, S. Normal pedal activation in real-world situations. SAE Int. J. Passeng. Cars Mech. Syst. 2011, 4, 364–369. [Google Scholar] [CrossRef]
- Shimada, H.; Hotta, R.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Makino, K. Effects of driving skill training on safe driving in older adults with mild cognitive impairment. Gerontology 2019, 65, 90–97. [Google Scholar] [CrossRef]
- Welch, S.A.; Ward, R.E.; Beauchamp, M.K.; Leveille, S.G.; Travison, T.; Bean, J.F. The short physical performance battery (SPPB): A quick and useful tool for fall risk stratification among older primary care patients. J. Am. Med. Dir. Assoc. 2021, 22, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, Y.; Park, K.; Ueda, H.; Ono, H.; Miyake, H. Being watched over by a conversation robot may enhance safety in simulated driving. J. Saf. Res. 2019, 71, 207–218. [Google Scholar] [CrossRef]
- Brydges, C.R. Effect size guidelines, sample size calculations, and statistical power in gerontology. Innov. Aging 2019, 3, 1–8. [Google Scholar] [CrossRef]
- Cohen, J. Quantitative methods in psychology: A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Jones, S.; Schultz, M.G.; Tillin, T.; Park, C.; Williams, S.; Chaturvedi, N.; Hughes, A.D. Sex differences in the contribution of different physiological systems to physical function in older adults. Geroscience 2021, 43, 443–455. [Google Scholar] [CrossRef] [PubMed]
- McCarrey, A.C.; An, Y.; Kitner-Triolo, M.H.; Ferrucci, L.; Resnick, S.M. Sex differences in cognitive trajectories in clinically normal older adults. Psychol. Aging 2016, 31, 166–175. [Google Scholar] [CrossRef]
- Bauer, M.J.; Adler, G.; Kuskowski, M.A.; Rottunda, S. The influence of age and gender on the driving patterns of older adults. J. Women Aging 2003, 15, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Perret, E.; Regli, F. Age and the perceptual threshold for vibratory stimuli. Eur. Neurol. 1970, 4, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Fujita, K.; Kobayashi, Y.; Sato, M.; Hori, H.; Sakai, R.; Ogawa, T.; Sugano, T.; Kawabata, K.; Hitosugi, M. Kinematic and electrophysiological characteristics of pedal operation by elderly drivers during emergency braking. Healthcare 2021, 9, 852. [Google Scholar] [CrossRef]
- Gomez-Granados, A.; Barany, D.A.; Schrayer, M.; Kurtzer, I.L.; Bonnet, C.T.; Singh, T. Age-related deficits in rapid visuomotor decision-making. J. Neurophysiol. 2021, 126, 1592–1603. [Google Scholar] [CrossRef]
- Vachon, C.M.; Modchalingam, S.; ‘t Hart, B.M.; Henriques, D.Y.P. The effect of age on visuomotor learning processes. PLoS ONE 2020, 15, e0239032. [Google Scholar] [CrossRef]
- Boucher, J.L.; Denis, S.; Landriault, J.A. Sex differences and effects of aging on visuomotor coordination. Percept. Mot. Skills 1991, 72, 507–512. [Google Scholar] [CrossRef]
- Ribeiro, B.; Bengtsson, L.; Benneworth, P.; Buhrer, S.; Castro-Martinez, E.; Hansen, M.; Jarmai, K.; Lindner, R.; Olmos-Penuela, J.; Ott, C.; et al. Introducing the dilemma of societal alignment for inclusive and responsible research and innovation. J. Respons. Innov. 2019, 5, 316–331. [Google Scholar] [CrossRef]
- Wynne, R.A.; Beanland, V.; Salmon, P.M. Systematic review of driving simulator validation studies. Safe Sci. 2019, 117, 138–151. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Health Technology Assessment. 2011. Available online: https://www.who.int/health-topics/health-technology-assessment#tab=tab_1 (accessed on 20 February 2025).
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://sdgs.un.org/2030agenda?utm_source=chatgpt.com (accessed on 20 February 2025).
- United Nations, General Assembly Economic and Social Council. Progress Towards the Sustainable Development Goals. Report of the Secretary-General. 2024. Available online: https://unstats.un.org/sdgs/files/report/2024/secretary-general-sdg-report-2024--EN.pdf. (accessed on 20 February 2025).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Older (N = 48) | Young (N = 56) | |
|---|---|---|
| age (range, median) | 73.5 ± 4.9 (64–84, 73) | 21.1 ± 0.7 (20–23, 21) |
| sex (male/female) | 35/13 | 16/40 |
| driving frequency (high/low) | 47/1 | 11/45 |
| MMSE (range, median) | 28.3 ± 1.5 (25–30, 29) | - |
| Target Speed | ||||||||
|---|---|---|---|---|---|---|---|---|
| 30 km/h | 40 km/h | 60 km/h | 70 km/h | |||||
| r | [95%CI] | r | [95%CI] | r | [95%CI] | r | [95%CI] | |
| Age | 0.1 | [−0.26, 0.44] | −0.10 | [−0.44, 0.27] | 0.11 | [−0.26, 0.45] | 0.25 | [−0.12, 0.55] |
| [Physical, cognitive function] | ||||||||
| grip strength | −0.15 | [−0.48, 0.22] | −0.39 | [−0.66, −0.03] | −0.15 | [−0.49, 0.22] | −0.20 | [−0.52, 0.18] |
| SPPB | −0.15 | [−0.48, 0.21] | −0.09 | [−0.43, 0.28] | −0.17 | [−0.50, 0.19] | −0.09 | [−0.43, 0.27] |
| MMSE | −0.22 | [−0.54, 0.16] | 0.24 | [−0.14, 0.55] | 0.50 | [0.16, 0.73] | 0.26 | [−0.12, 0.57] |
| TMT-A | 0.21 | [−0.17, 0.53] | −0.04 | [−0.40, 0.33] | −0.21 | [−0.53, 0.17] | 0.30 | [−0.08, 0.60] |
| TMT-B | 0.17 | [−0.21, 0.50] | −0.07 | [−0.42, 0.31] | −0.07 | [−0.42, 0.31] | 0.28 | [−0.10, 0.59] |
| [DS driving reaction test] | ||||||||
| RT | 0.07 | [−0.30, 0.42] | −0.23 | [−0.54, 0.15] | −0.16 | [−0.49, 0.21] | 0.01 | [−0.36, 0.36] |
| miss | −0.02 | [−0.37, 0.35] | −0.14 | [−0.47, 0.24] | −0.21 | [−0.53, 0.17] | 0.10 | [−0.27, 0.44] |
| [DS course-driving task] | ||||||||
| accidents | 0.10 | [−0.34, 0.51] | 0.34 | [−0.11, 0.67] | 0.52 | [0.11, 0.78] | 0.58 | [0.20, 0.81] |
| rapid deceleration | 0.45 | [0.03, 0.74] | −0.14 | [−0.54, 0.31] | −0.33 | [−0.67, 0.12] | 0.10 | [−0.35, 0.51] |
| [On-road evaluation] | ||||||||
| total score | 0.02 | [−0.34, 0.37] | −0.12 | [−0.46, 0.24] | −0.12 | [−0.45, 0.25] | −0.16 | [−0.49, 0.20] |
| safety checks | 0.16 | [−0.21, 0.48] | 0.35 | [−0.01, 0.63] | 0.15 | [−0.22, 0.47] | 0.12 | [−0.25, 0.45] |
| braking | 0.07 | [−0.29, 0.42] | −0.13 | [−0.46, 0.24] | 0.08 | [−0.28, 0.43] | −0.12 | [−0.45, 0.25] |
| steering | −0.30 | [−0.59, 0.06] | −0.15 | [−0.48, 0.22] | 0.03 | [−0.33, 0.38] | 0.08 | [−0.29, 0.42] |
| vehicle control | −0.07 | [−0.41, 0.29] | 0.10 | [−0.27, 0.44] | 0.02 | [−0.34, 0.37] | 0.14 | [−0.23, 0.47] |
| lane changes | 0.12 | [−0.24, 0.46] | 0.04 | [−0.32, 0.39] | 0.09 | [−0.28, 0.43] | 0.35 | [0.0, 0.63] |
| straight driving and turning | −0.30 | [−0.59, 0.06] | −0.12 | [−0.45, 0.24] | −0.20 | [−0.52, 0.16] | −0.09 | [−0.43, 0.27] |
| maximum speed | 0.11 | [−0.26, 0.44] | 0.00 | [−0.36, 0.35] | 0.22 | [−0.15, 0.53] | 0.02 | [−0.34, 0.37] |
| [Undulation driving index] | ||||||||
| −40 km/h | −0.21 | [−0.58, 0.23] | 0.11 | [−0.32, 0.51] | −0.16 | [−0.55, 0.28] | 0.02 | [−0.40, 0.44] |
| 40–60 km/h | 0.09 | [−0.35, 0.49] | 0.05 | [−0.38, 0.46] | −0.07 | [−0.48, 0.36] | −0.12 | [−0.52, 0.32] |
| rapid acceleration | −0.59 | [−0.81, −0.22] | −0.20 | [−0.57, 0.25] | −0.22 | [−0.59, 0.22] | −0.28 | [−0.62, 0.17] |
| rapid deceleration | −0.01 | [−0.43, 0.41] | −0.10 | [−0.50, 0.33] | −0.12 | [−0.52, 0.32] | 0.08 | [−0.36, 0.48] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, T.; Yamada, K.; Tsuchiya, Y.; Takimoto, M. Validation and Clinical Application of a Developed Pedal Coordination Assessment Device for Older Drivers. Healthcare 2025, 13, 537. https://doi.org/10.3390/healthcare13050537
Sasaki T, Yamada K, Tsuchiya Y, Takimoto M. Validation and Clinical Application of a Developed Pedal Coordination Assessment Device for Older Drivers. Healthcare. 2025; 13(5):537. https://doi.org/10.3390/healthcare13050537
Chicago/Turabian StyleSasaki, Tsutomu, Kyohei Yamada, Yoshio Tsuchiya, and Moeka Takimoto. 2025. "Validation and Clinical Application of a Developed Pedal Coordination Assessment Device for Older Drivers" Healthcare 13, no. 5: 537. https://doi.org/10.3390/healthcare13050537
APA StyleSasaki, T., Yamada, K., Tsuchiya, Y., & Takimoto, M. (2025). Validation and Clinical Application of a Developed Pedal Coordination Assessment Device for Older Drivers. Healthcare, 13(5), 537. https://doi.org/10.3390/healthcare13050537