

Effect of Preventive Exercise Programs for Swimmer’s Shoulder Injury on Rotator Cuff Torque and Balance in Competitive Swimmers: A Randomized Controlled Trial



Abstract
1. Introduction
2. Materials and Methods
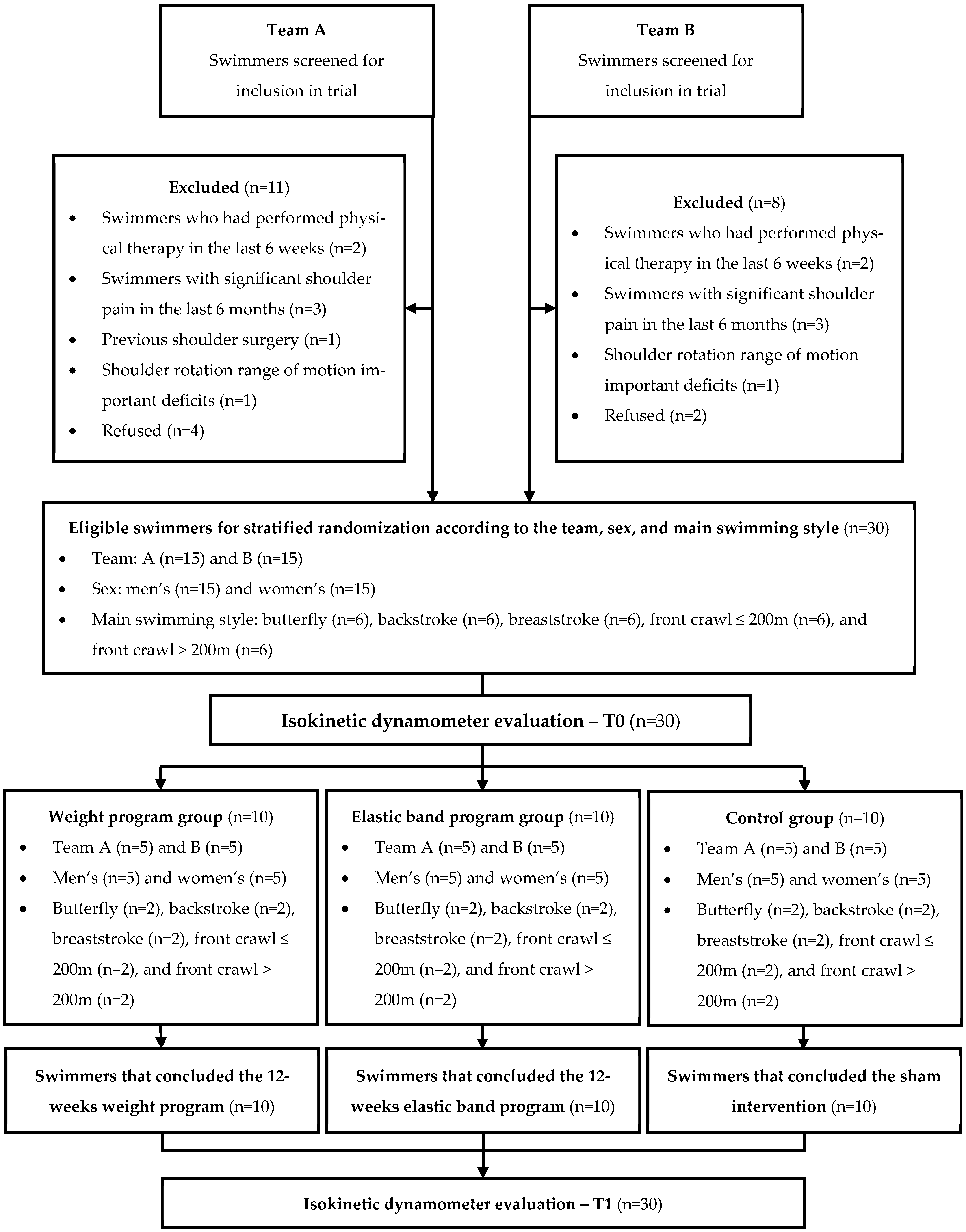
2.1. Trial Design
2.2. Participants
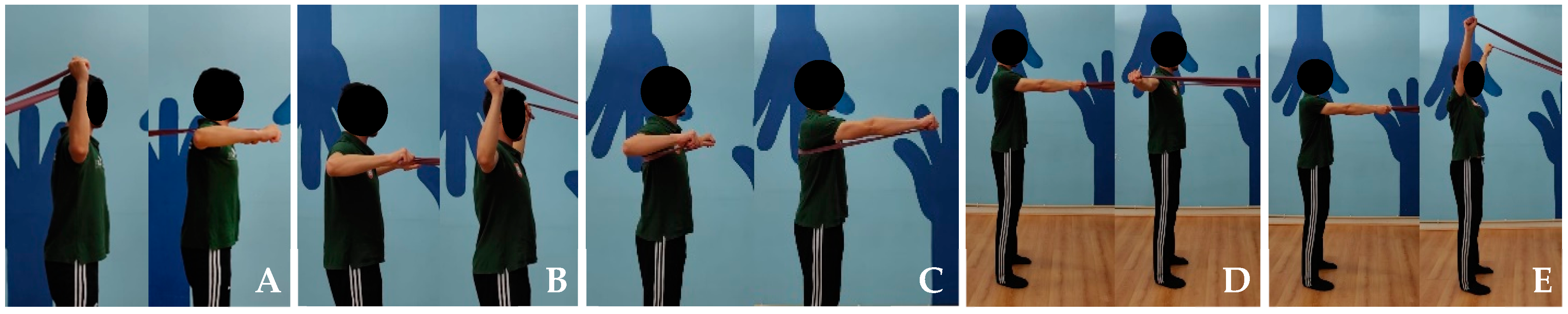
2.3. Intervention Programs
2.4. Control Group
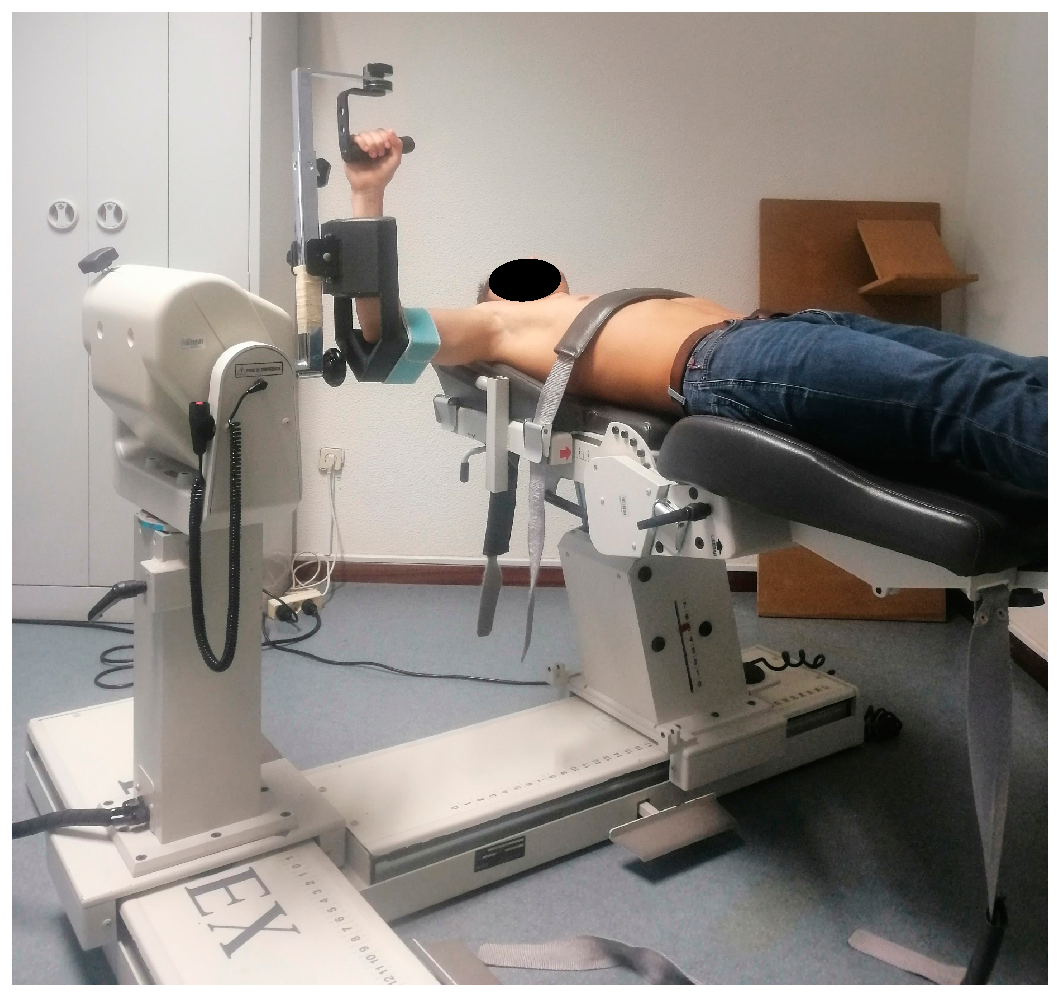
2.5. Outcomes and Testing Procedures
2.6. Sample Size
2.7. Randomization and Blinding
2.8. Data Analysis
3. Results
3.1. Peak Torque
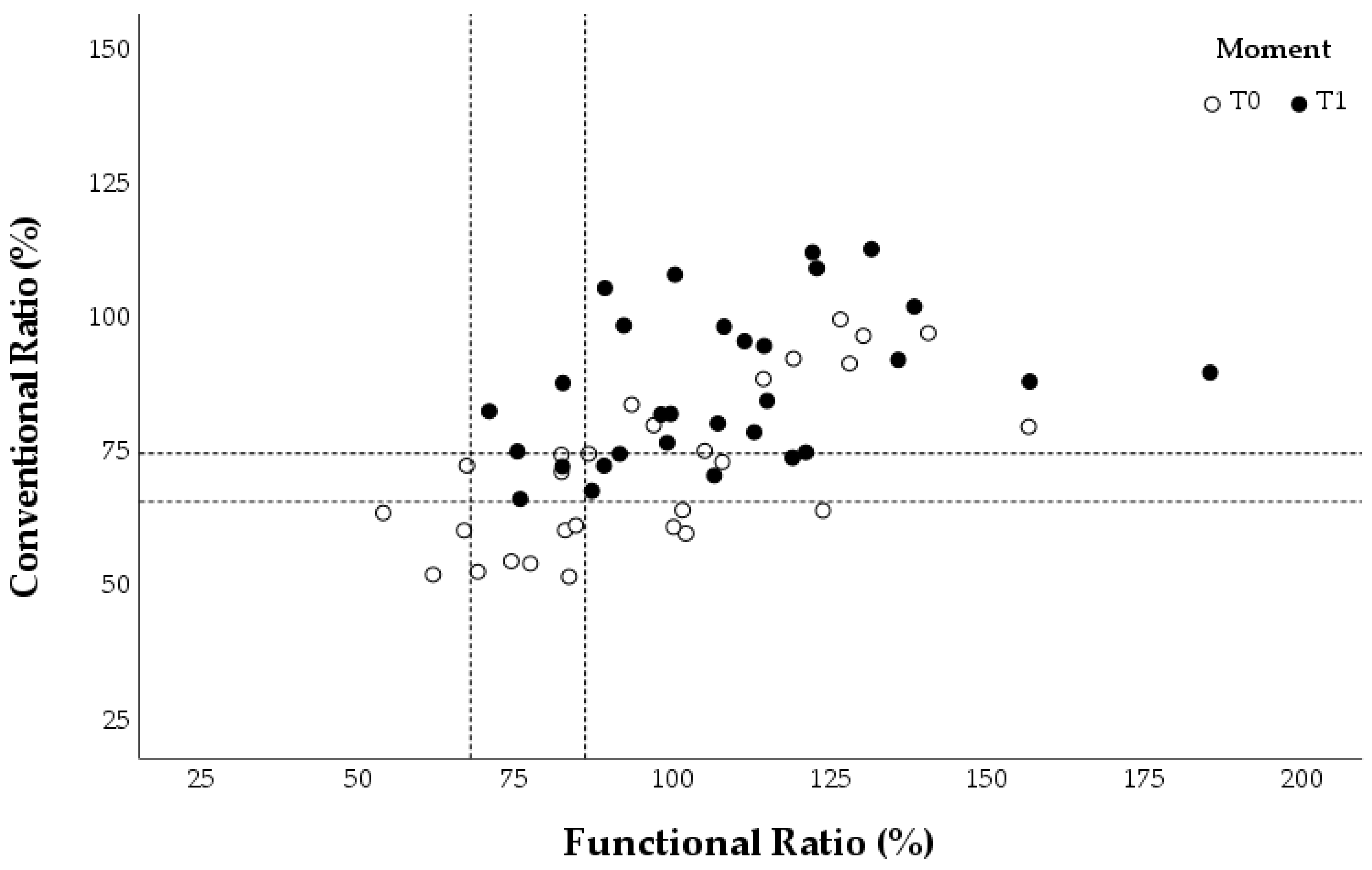
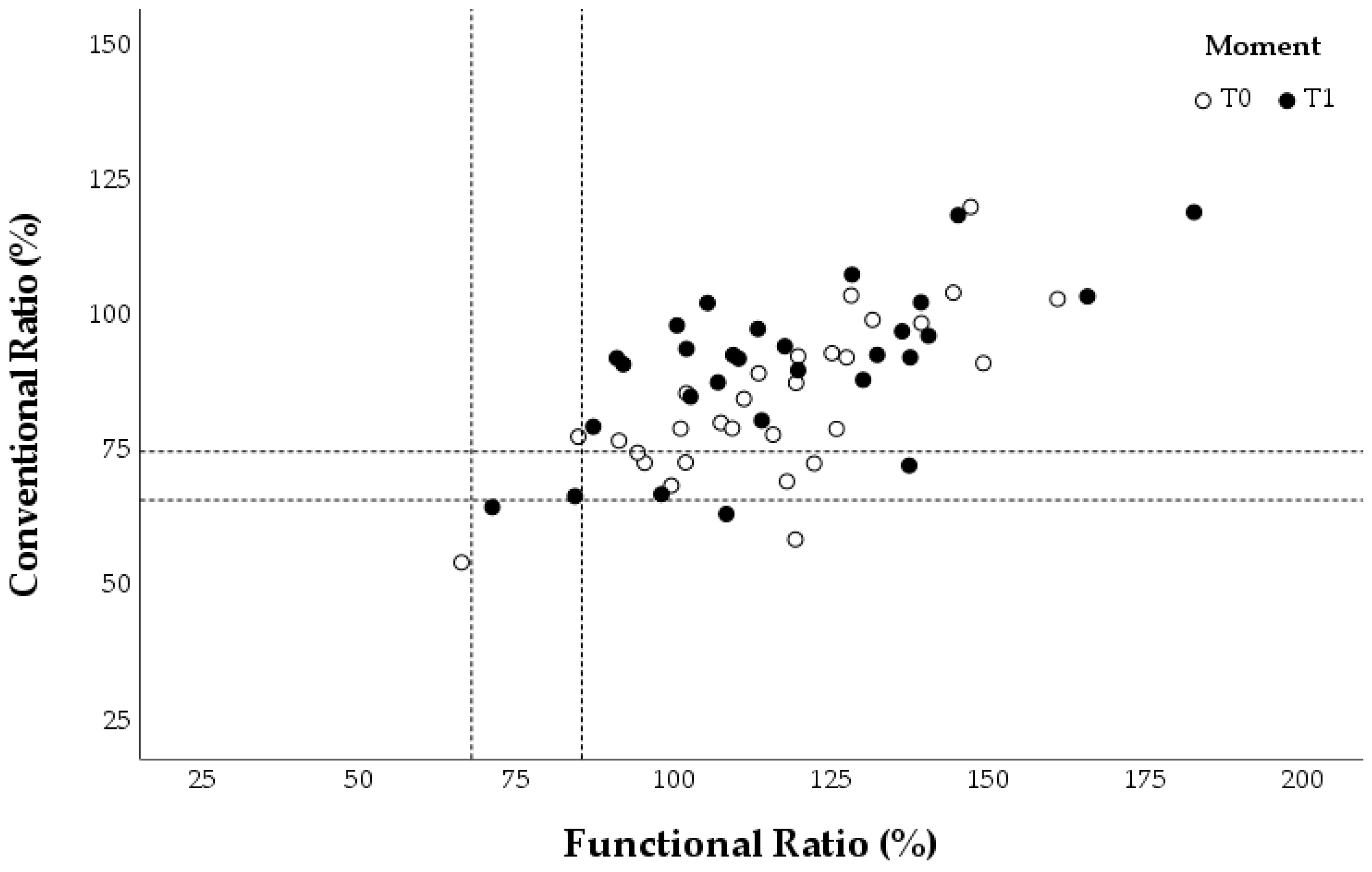
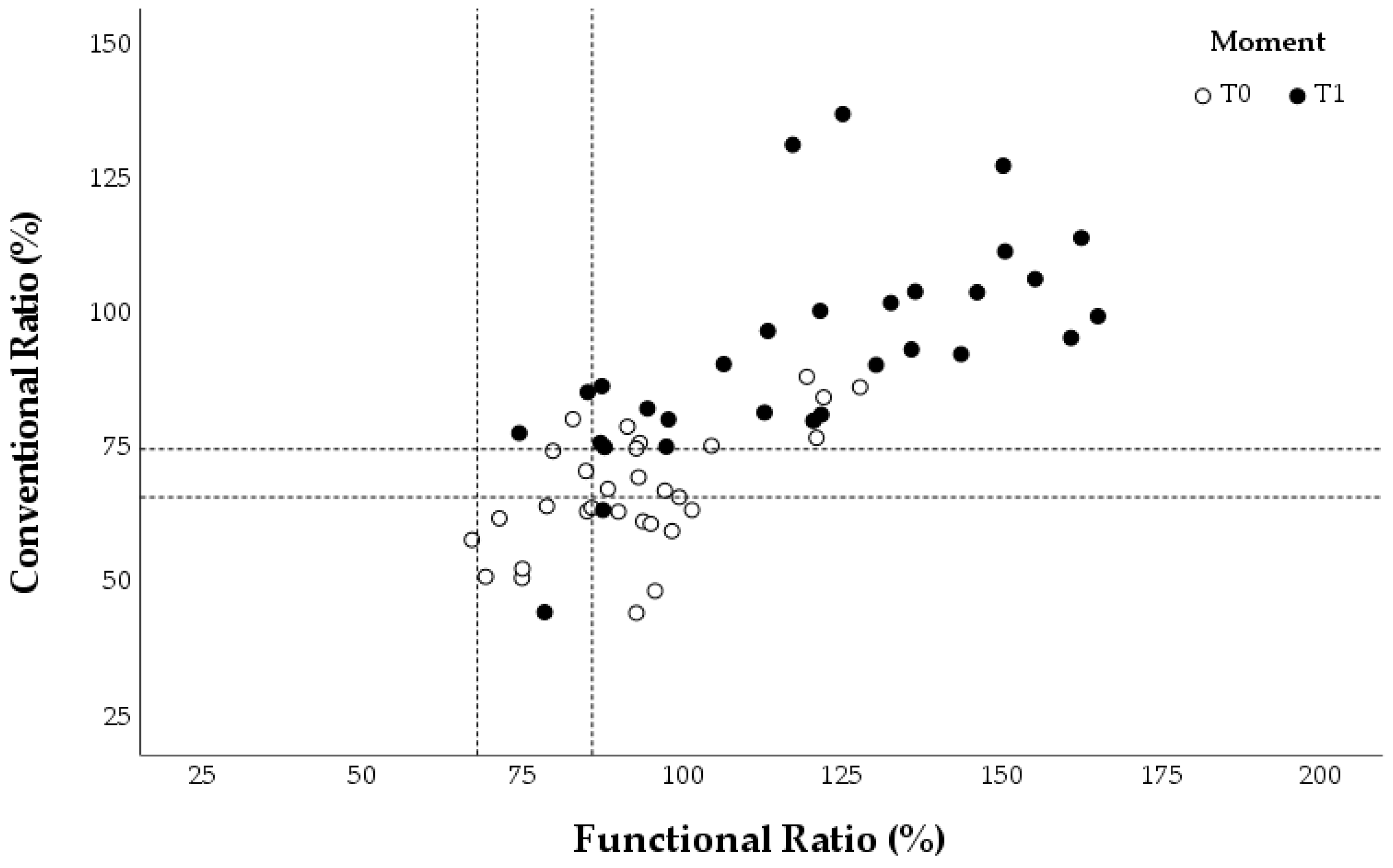
3.2. Conventional and Functional Ratios
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ER | External rotation |
| IR | Internal rotation |
| PT | Peak torque |
| con | Concentric |
| ecc | Eccentric |
| 1RM | One-repetition maximum |
| ROM | Range of motion |
References
- Feijen, S.; Tate, A.; Kuppens, K.; Claes, A.; Struyf, F. Swim-training volume and shoulder pain across the life span of the competitive swimmer: A systematic review. J. Athl. Train. 2020, 55, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Schlueter, K.R.; Pintar, J.A.; Wayman, K.J.; Hartel, L.J.; Briggs, M.S. Clinical evaluation techniques for injury risk assessment in elite swimmers: A systematic review. Sports Health 2021, 13, 57–64. [Google Scholar] [CrossRef]
- Struyf, F.; Tate, A.; Kuppens, K.; Feijen, S.; Michener, L.A. Musculoskeletal dysfunctions associated with swimmers’ shoulder. Br. J. Sports Med. 2017, 51, 775–780. [Google Scholar] [CrossRef]
- Walker, H.; Gabbe, B.; Wajswelner, H.; Blanch, P.; Bennell, K. Shoulder pain in swimmers: A 12-month prospective cohort study of incidence and risk factors. Phys. Ther. Sport 2012, 13, 243–249. [Google Scholar] [CrossRef]
- Yoma, M.; Herrington, L.; Mackenzie, T.A. The effect of exercise therapy interventions on shoulder pain and musculoskeletal risk factors for shoulder pain in competitive swimmers: A scoping review. J. Sport Rehabil. 2022, 31, 617–628. [Google Scholar] [CrossRef]
- Hill, L.; Mountjoy, M.; Miller, J. Non-shoulder injuries in swimming: A systematic review. Clin. J. Sport Med. 2022, 32, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Tavares, N.; Dias, G.; Carvalho, P.; Vilas-Boas, J.P.; Castro, M.A. Effectiveness of therapeutic exercise in musculoskeletal risk factors related to swimmer’s shoulder. Eur. J. Invest. Health Psychol. Educ. 2022, 12, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.; Collins, M.; Posthumus, M. Risk factors for shoulder pain and injury in swimmers: A critical systematic review. Physician Sportsmed. 2015, 43, 412–420. [Google Scholar] [CrossRef]
- Drigny, J.; Gauthier, A.; Reboursière, E.; Guermont, H.; Gremeaux, V.; Edouard, P. Shoulder muscle imbalance as a risk for shoulder injury in elite adolescent swimmers: A prospective study. J. Hum. Kinet. 2020, 75, 103–113. [Google Scholar] [CrossRef]
- Matzkin, E.; Suslavich, K.; Wes, D. Swimmer’s shoulder: Painful shoulder in the competitive swimmer. J. Am. Acad. Orthop. Surg. 2016, 24, 527–536. [Google Scholar] [CrossRef]
- Gaunt, T.; Maffulli, N. Soothing suffering swimmers: A systematic review of the epidemiology, diagnosis, treatment and rehabilitation of musculoskeletal injuries in competitive swimmers. Br. Med. Bull. 2012, 103, 45–88. [Google Scholar] [CrossRef] [PubMed]
- Yoma, M.; Herrington, L.; Mackenzie, T.A.; Almond, T.A. Training intensity and shoulder musculoskeletal physical quality responses in competitive swimmers. J. Athl. Train. 2021, 56, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Feijen, S.; Struyf, T.; Kuppens, K.; Tate, A.; Struyf, F. Prediction of shoulder pain in youth competitive swimmers: The development and internal validation of a prognostic prediction model. Am. J. Sports Med. 2021, 49, 154–161. [Google Scholar] [CrossRef]
- Buoite, S.A.; Cargnel, A.; Raffini, A.; Mazzari, L.; Martini, M.; Ajčević, M.; Accardo, A.; Deodato, M.; Murena, L. Shoulder tensiomyography and isometric strength in swimmers before and after a fatiguing protocol. J. Athl. Train. 2024, 59, 738–744. [Google Scholar] [CrossRef]
- Wanivenhaus, F.; Fox, A.J.; Chaudhury, S.; Rodeo, S.A. Epidemiology of injuries and prevention strategies in competitive swimmers. Sports Health 2012, 4, 246–251. [Google Scholar] [CrossRef]
- McKenzie, A.; Larequi, S.-A.; Hams, A.; Headrick, J.; Whiteley, R.; Duhig, S. Shoulder pain and injury risk factors in competitive swimmers: A systematic review. Scand. J. Med. Sci. Sports 2023, 33, 2396–2412. [Google Scholar] [CrossRef] [PubMed]
- Batalha, N.M.; Raimundo, A.M.; Tomas-Carus, P.; Barbosa, T.M.; Silva, A.J. Shoulder rotator cuff balance, strength, and endurance in young swimmers during a competitive season. J. Strength Cond. Res. 2013, 27, 2562–2568. [Google Scholar] [CrossRef] [PubMed]
- Collado-Mateo, D.; Dominguez-Muñoz, F.J.; Batalha, N.; Perraça, J.; Tomas-Carus, P.; Adsuar, J.C. Test-retest reliability of isokinetic arm strength measurements in competitive swimmers. J. Hum. Kinet. 2018, 65, 5–11. [Google Scholar] [CrossRef]
- Olivier, N.; Daussin, F.N. Relationships between isokinetic shoulder evaluation and fitness characteristics of elite french female water-polo players. J. Hum. Kinet. 2018, 64, 5–11. [Google Scholar] [CrossRef]
- So, B.C.L.; Lau, S.C.T.; Kwok, W.Y.; Tse, D.H.T.; Man, S.S. Investigating the association between supraspinatus tendon abnormality, shoulder pain and isokinetic strength in elite swimmers: A cross-sectional study. J. Sports Sci. Med. 2023, 22, 17–27. [Google Scholar] [CrossRef]
- Andrade, M.S.; Vancini, R.L.; Lira, C.A.B.; Mascarin, N.C.; Fachina, R.J.F.G.; Silva, A.C. Shoulder isokinetic profile of male handball players of the Brazilian national team. Braz. J. Phys. Ther. 2013, 17, 572–578. [Google Scholar] [CrossRef] [PubMed]
- Bak, K.; Magnusson, S.P. Shoulder strength and range of motion in symptomatic and pain-free elite swimmers. Am. J. Sports Med. 1997, 25, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Edouard, P.; Degache, F.; Oullion, R.; Plessis, J.Y.; Gleizes-Cervera, S.; Calmels, P. Shoulder strength imbalances as injury risk in handball. Int. J. Sports Med. 2013, 34, 654–660. [Google Scholar] [CrossRef]
- Ellenbecker, T.S.; Davies, G.J. The application of isokinetics in testing and rehabilitation of the shoulder complex. J. Athl. Train. 2000, 35, 338–350. [Google Scholar] [PubMed]
- Olivier, N.; Quintin, G.; Rogez, J. The high level swimmer articular shoulder complex. Ann. Readapt. Med. Phys. 2008, 51, 342–347. [Google Scholar] [CrossRef]
- Batalha, N.; Raimundo, A.; Tomas-Carus, P.; Paulo, J.; Simão, R.; Silva, A.J. Does a land-based compensatory strength-training programme influences the rotator cuff balance of young competitive swimmers? Eur. J. Sport Sci. 2015, 15, 764–772. [Google Scholar] [CrossRef]
- Chepeha, J.C.; Magee, D.J.; Bouliane, M.; Sheps, D.; Beaupre, L. Effectiveness of a posterior shoulder stretching program on university-level overhead athletes: Randomized controlled trial. Clin. J. Sport Med. 2018, 28, 146–152. [Google Scholar] [CrossRef]
- Kluemper, M.; Uhl, T.; Hazelrigg, H. Effect of stretching and strengthening shoulder muscles on forward shoulder posture in competitive swimmers. J. Sport Rehabil. 2006, 15, 58–70. [Google Scholar] [CrossRef]
- Lynch, S.S.; Thigpen, C.A.; Mihalik, J.P.; Prentice, W.E.; Padua, D. The effects of an exercise intervention on forward head and rounded shoulder postures in elite swimmers. Br. J. Sports Med. 2010, 44, 376–381. [Google Scholar] [CrossRef]
- Manske, R.C.; Lewis, S.; Wolff, S.; Smith, B. Effects of a dry-land strengthening program in competitive adolescent swimmers. Int. J. Sports Phys. Ther. 2015, 10, 858–867. [Google Scholar]
- Swanik, K.A.; Lephart, S.M.; Swanik, C.B.; Lephart, S.P.; Stone, D.A.; Fu, F.H. The effects of shoulder plyometric training on proprioception and selected muscle performance characteristics. J. Shoulder Elb. Surg. 2002, 11, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Hibberd, E.E.; Oyama, S.; Spang, J.T.; Prentice, W.; Myers, J.B. Effect of a 6-week strengthening program on shoulder and scapular-stabilizer strength and scapular kinematics in division I collegiate swimmers. J. Sport Rehabil. 2012, 21, 253–265. [Google Scholar] [CrossRef]
- Swanik, K.A.; Swanik, C.B.; Lephart, S.M.; Huxel, K. The effect of functional training on the incidence of shoulder pain and strength in intercollegiate swimmers. J. Sport Rehabil. 2002, 11, 140–154. [Google Scholar] [CrossRef]
- Fredriksen, H.; Cools, A.; Myklebust, G. No added benefit of 8 weeks of shoulder external rotation strength training for youth handball players over usual handball training alone: A randomized controlled trial. J. Orthop. Sports Phys. Ther. 2021, 51, 174–187. [Google Scholar] [CrossRef] [PubMed]
- Tavares, N.; Vilas-Boas, J.P.; Castro, M.A. Electromyographic activity of shoulder muscles on two preventive exercise programmes for swimmer’s shoulder: Elastic band versus weight. Sports Biomech. 2024, 1–13. [Google Scholar] [CrossRef]
- ACSM Wayne Westcott, W. ACSM strength training guidelines: Role in body composition and health enhancement. ACSMs Health Fit. J. 2009, 13, 14–22. [Google Scholar] [CrossRef]
- Shahpar, F.M.; Rahnama, N.; Salehi, S. The effect of 8 weeks open and closed kinetic chain strength training on the torque of the external and internal shoulder rotator muscles in elite swimmers. Asian J. Sports Med. 2019, 10, e82158. [Google Scholar] [CrossRef]
- Batalha, N.; Dias, S.; Marinho, D.A.; Parraca, J.A. The effectiveness of land and water based resistance training on shoulder rotator cuff strength and balance of youth swimmers. J. Hum. Kinet. 2018, 62, 91–102. [Google Scholar] [CrossRef]
- Van de Velde, A.; De Mey, K.; Maenhout, A.; Calders, P.; Cools, A.M. Scapular-muscle performance: Two training programs in adolescent swimmers. J. Athl. Train. 2011, 46, 160–167. [Google Scholar] [CrossRef]
- Ekstrom, R.A.; Donatelli, R.A.; Soderberg, G.L. Surface electromyographic analysis of exercises for trapezius and serratus anterior muscles. J. Orthop. Sports Phys. Ther. 2003, 33, 247–258. [Google Scholar] [CrossRef]
- Myers, J.B.; Pasquale, M.R.; Laudner, K.G.; Sell, T.C.; Bradley, J.P.; Lephart, S.M. On-the-field resistance-tubing exercises for throwers: An electromyographic analysis. J. Athl. Train. 2005, 40, 15–22. [Google Scholar] [PubMed]
- Oyama, S.; Myers, J.B.; Wassinger, C.A.; Lephart, S.M. Three-dimensional scapular and clavicular kinematics and scapular muscle activity during retraction exercises. J. Orthop. Sports Phys. Ther. 2010, 40, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Holt, G.R. Declaration of Helsinki—The world’s document of conscience and responsibility. South. Med. J. 2014, 107, 407. [Google Scholar] [CrossRef]
- Baechle, T.R.; Earle, R.W. Essentials Strength Training Conditioning, 3rd ed.; Human Kinetics: Champaign, IL, USA, 2008; pp. 381–412. [Google Scholar]
- Batalha, N.; Paixão, C.; Silva, A.J.; Costa, M.J.; Mullen, J.; Barbosa, T.M. The effectiveness of a dry-land shoulder rotators strength training program in injury prevention in competitive swimmers. J. Hum. Kinet. 2020, 71, 11–20. [Google Scholar] [CrossRef]
- Loureiro, R.L.; Oliveira, R.; Gonçalves, R.S. Comparação da Razão de Força Excêntrica-Concêntrica dos Rotadores do Ombro Entre Jogadores de Andebol e Futsal. Master’s Thesis, Coimbra Health School—Polytechnic Institute of Coimbra, Coimbra, Portugal, 2013. [Google Scholar]
- Noffal, G.J. Isokinetic eccentric-to-concentric strength ratios of the shoulder rotator muscles in throwers and nonthrowers. Am. J. Sports Med. 2003, 31, 537–541. [Google Scholar] [CrossRef]
- Forthomme, B.; Dvir, Z.; Crielaard, J.M.; Croisier, J.L. Isokinetic assessment of the shoulder rotators: A study of optimal test position. Clin. Physiol. Funct. Imaging 2011, 31, 227–232. [Google Scholar] [CrossRef]
- Ellenbecker, T.S.; Mattalino, A.J. Concentric isokinetic shoulder internal and external rotation strength in professional baseball pitchers. J. Orthop. Sports Phys. Ther. 1997, 25, 323–328. [Google Scholar] [CrossRef]
- Brown, L.E.; Whitehurst, M.; Gilbert, R.; Buchalter, D.N. The effect of velocity and gender on load range during knee extension and flexion exercise on an isokinetic device. J. Orthop. Sports Phys. Ther. 1995, 21, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Andrade, M.S.; Koffes, F.C.; Silva, A.A.B.; Silva, A.C.; Lira, C.A.B. Effect of fatigue caused by a simulated handball game on ball throwing velocity, shoulder muscle strength and balance ratio: A prospective study. BMC Sports Sci. Med. Rehabil. 2016, 8, 13. [Google Scholar] [CrossRef]
- Lopes, J.S.S.; Machado, A.F.; Micheletti, J.K.; Almeida, A.C.; Cavina, A.P.; Pastre, C.M. Effects of training with elastic resistance versus conventional resistance on muscular strength: A systematic review and meta-analysis. SAGE Open Med. 2019, 7, 2106903116. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise | Weight Program | Elastic Band Program |
|---|---|---|
| IR at 90° | Started in a supine position, 90° shoulder ABD, 90° ER, and 90° elbow FLX. Movement: 90° shoulder IR and return to the starting position (5 s). | Started in a SP, 90° shoulder ABD, 90° elbow FLX, and hands at the same height as shoulders. The elastic band should be fixed at shoulder height. Movement: 90° shoulder IR (5 s) and return to the starting position (5 s). |
| ER at 90° | Started in a SP, 90° shoulder ABD, 90° elbow FLX, and hands at the same height as shoulders. Movement: 90° shoulder ER (5 s) and return to the starting position (5 s). | Started in a SP, 90° shoulder ABD, 90 elbow FLX, and hands at the same height as shoulders. The elastic band should be fixed at shoulder height. Movement: 90° shoulder ER (5 s) and return to the starting position (5 s). |
| Scapular punches | Started in a SP, 90° shoulder ABD, 90° elbow FLX, and hands at the same height as shoulders. Movement: Elbow EXT (5 s) and return to the starting position (5 s). | Started in a SP, 90° shoulder ABD, 90° elbow FLX, and hands at the same height as shoulders. The elastic band should be fixed at shoulder height. Movement: Elbow EXT (5 s) and return to the starting position (5 s). |
| T’s | Started in a SP, 90° shoulder FLX, and maximum elbow EXT. Movement: 90° shoulder HABD (5 s) and return to the starting position (5 s). | Started in a SP, 90° shoulder FLX, and maximum elbow EXT. The elastic band should be fixed at shoulder height. Movement: 90° shoulder HABD (5 s) and return to the starting position (5 s). |
| Y’s | Started in a SP, 90° shoulder FLX, and maximum elbow EXT. Movement: 90° shoulder HABD and maximum shoulder FLX (5 s) and return to the starting position (5 s). | Started in a SP, 90° shoulder FLX, and maximum elbow EXT. The elastic band should be fixed at shoulder height. Movement: 90° shoulder HABD and maximum shoulder FLX (5 s) and return to the starting position (5 s). |
| Variables | WP Mean ± SD | EBP Mean ± SD | Control Mean ± SD | p-Value |
|---|---|---|---|---|
| Age (years) | 19.90 ± 2.92 | 19.60 ± 2.99 | 19.00 ± 3.62 | 0.506 |
| Body Mass (kg) | 68.86 ± 8.49 | 68.80 ± 14.76 | 65.57 ± 11.77 | 0.879 |
| Height (m) | 1.72 ± 0.08 | 1.70 ± 0.11 | 1.73 ± 0.09 | 0.774 |
| Body Mass Index (kg/m2) | 23.19 ± 2.24 | 23.64 ± 3.34 | 21.79 ± 1.91 | 0.262 |
| Fat mass (%) | 17.02 ± 10.30 | 17.37 ± 8.65 | 15.40 ± 7.19 | 0.700 |
| Lean mass (kg) | 55.23 ± 10.60 | 57.66 ± 12.83 | 52.04 ± 13.66 | 0.868 |
| Bone mass (kg) | 2.91 ± 0.51 | 3.03 ± 0.64 | 2.75 ± 0.69 | 0.706 |
| Swimming practice (years) | 12.10 ± 4.18 | 9.40 ± 4.81 | 12.30 ± 4.17 | 0.274 |
| Competitive swimming (years) | 8.90 ± 3.28 | 6.10 ± 3.73 | 7.90 ± 3.38 | 0.206 |
| Weekly swimming training (hours) | 16.80 ± 5.01 | 14.20 ± 6.29 | 16.60 ± 6.87 | 0.577 |
| WP PT (Nm/kg) | EBP PT (Nm/kg) | Control PT (Nm/kg) | p-Value | ||
|---|---|---|---|---|---|
| 60°/s | conIR | 36.06 ± 9.71 | 33.17 ± 9.25 | 37.99 ± 13.49 | 0.619 |
| eccIR | 37.30 ± 7.74 | 38.62 ± 14.47 | 41.67 ± 19.08 | 0.790 | |
| conER | 24.98 ± 6.63 | 27.62 ± 7.95 | 25.42 ± 10.25 | 0.756 | |
| eccER | 31.69 ± 7.11 | 36.14 ± 11.61 | 34.51 ± 13.58 | 0.667 | |
| 120°/s | conIR | 30.84 ± 9.22 | 32.13 ± 11.56 | 34.66 ± 13.53 | 0.756 |
| eccIR | 36.71 ± 8.05 | 36.43 ± 11.96 | 38.01 ± 17.24 | 0.959 | |
| conER | 23.95 ± 6.91 | 26.90 ± 8.88 | 23.63 ± 11.58 | 0.691 | |
| eccER | 29.74 ± 7.46 | 35.47 ± 11.95 | 30.79 ± 12.80 | 0.473 | |
| 180°/s | conIR | 28.63 ± 9.70 | 28.22 ± 10.73 | 32.07 ± 13.90 | 0.719 |
| eccIR | 38.11 ± 6.99 | 39.81 ± 12.95 | 39.53 ± 19.00 | 0.958 | |
| conER | 21.33 ± 5.07 | 24.26 ± 9.45 | 22.65 ± 11.64 | 0.774 | |
| eccER | 31.08 ± 7.74 | 37.28 ± 12.10 | 31.26 ± 14.64 | 0.464 |
| T0 PT (Nm/kg) | T1 PT (Nm/kg) | Difference PT (Nm/kg) | p-Value | ||
|---|---|---|---|---|---|
| Weight Program | conIR at 60°/s | 36.06 ± 9.71 | 30.41 ± 11.93 | −5.65 | 0.047 * |
| eccIR at 60°/s | 37.30 ± 7.74 | 37.16 ± 10.80 | −0.14 | 0.959 | |
| conER at 60°/s | 24.98 ± 6.63 | 25.96 ± 8.45 | 0.98 | 0.506 | |
| eccER at 60°/s | 31.69 ± 7.11 | 29.84 ± 7.78 | −1.85 | 0.315 | |
| conIR at 120°/s | 30.84 ± 9.22 | 29.57 ± 10.77 | −1.27 | 0.537 | |
| eccIR at 120°/s | 36.71 ± 8.05 | 36.91 ± 10.74 | 0.20 | 1.000 | |
| conER at 120°/s | 23.95 ± 6.91 | 24.41 ± 7.05 | 0.46 | 0.705 | |
| eccER at 120°/s | 29.74 ± 7.46 | 29.03 ± 7.54 | −0.71 | 0.704 | |
| conIR at 180°/s | 28.63 ± 9.70 | 26.21 ± 9.77 | −2.42 | 0.215 | |
| eccIR at 180°/s | 38.11 ± 6.99 | 37.49 ± 9.65 | −0.62 | 0.757 | |
| conER at 180°/s | 21.33 ± 5.07 | 22.74 ± 7.01 | 1.41 | 0.294 | |
| eccER at 180°/s | 31.08 ± 7.74 | 30.02 ± 8.83 | −1.06 | 0.642 | |
| Elastic Band Program | conIR at 60°/s | 33.17 ± 9.25 | 32.65 ± 13.57 | −0.52 | 0.445 |
| eccIR at 60°/s | 38.62 ± 14.47 | 38.08 ± 19.37 | −0.54 | 0.575 | |
| conER at 60°/s | 27.62 ± 7.95 | 28.42 ± 8.12 | 0.80 | 0.595 | |
| eccER at 60°/s | 36.14 ± 11.61 | 35.57 ± 13.38 | −0.57 | 0.818 | |
| conIR at 120°/s | 32.13 ± 11.56 | 30.95 ± 15.44 | −1.18 | 0.074 | |
| eccIR at 120°/s | 36.43 ± 11.96 | 36.63 ± 18.98 | 0.20 | 0.594 | |
| conER at 120°/s | 26.90 ± 8.88 | 26.84 ± 9.12 | −0.06 | 0.977 | |
| eccER at 120°/s | 35.47 ± 11.95 | 33.03 ± 11.15 | −2.44 | 0.386 | |
| conIR at 180°/s | 28.22 ± 10.73 | 27.37 ± 13.81 | −0.85 | 0.648 | |
| eccIR at 180°/s | 39.81 ± 12.95 | 37.48 ± 21.51 | −2.33 | 0.386 | |
| conER at 180°/s | 24.26 ± 9.45 | 24.74 ± 10.70 | 0.48 | 0.828 | |
| eccER at 180°/s | 37.28 ± 12.10 | 35.36 ± 13.47 | −1.92 | 0.301 | |
| Control | conIR at 60°/s | 37.99 ± 13.49 | 28.15 ± 10.65 | −9.84 | 0.002 * |
| eccIR at 60°/s | 41.67 ± 19.08 | 37.03 ± 16.37 | −4.64 | 0.036 * | |
| conER at 60°/s | 25.42 ± 10.25 | 25.85 ± 9.38 | 0.43 | 0.788 | |
| eccER at 60°/s | 34.51 ± 13.58 | 30.54 ± 12.50 | −3.97 | 0.048 * | |
| conIR at 120°/s | 34.66 ± 13.53 | 26.07 ± 10.35 | −8.59 | 0.005 * | |
| eccIR at 120°/s | 38.01 ± 17.24 | 37.08 ± 16.05 | −0.93 | 0.627 | |
| conER at 120°/s | 23.63 ± 11.58 | 24.02 ± 9.68 | 0.39 | 0.843 | |
| eccER at 120°/s | 30.79 ± 12.80 | 30.18 ± 12.88 | −0.61 | 0.675 | |
| conIR at 180°/s | 32.07 ± 13.90 | 24.53 ± 10.46 | −7.54 | 0.002 * | |
| eccIR at 180°/s | 39.53 ± 19.00 | 37.15 ± 16.10 | −2.38 | 0.264 | |
| conER at 180°/s | 22.65 ± 11.64 | 22.20 ± 9.70 | −0.45 | 0.771 | |
| eccER at 180°/s | 31.26 ± 14.64 | 31.61 ± 13.71 | 0.35 | 0.680 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavares, N.; Vilas-Boas, J.P.; Castro, M.A. Effect of Preventive Exercise Programs for Swimmer’s Shoulder Injury on Rotator Cuff Torque and Balance in Competitive Swimmers: A Randomized Controlled Trial. Healthcare 2025, 13, 538. https://doi.org/10.3390/healthcare13050538
Tavares N, Vilas-Boas JP, Castro MA. Effect of Preventive Exercise Programs for Swimmer’s Shoulder Injury on Rotator Cuff Torque and Balance in Competitive Swimmers: A Randomized Controlled Trial. Healthcare. 2025; 13(5):538. https://doi.org/10.3390/healthcare13050538
Chicago/Turabian StyleTavares, Nuno, João Paulo Vilas-Boas, and Maria António Castro. 2025. "Effect of Preventive Exercise Programs for Swimmer’s Shoulder Injury on Rotator Cuff Torque and Balance in Competitive Swimmers: A Randomized Controlled Trial" Healthcare 13, no. 5: 538. https://doi.org/10.3390/healthcare13050538
APA StyleTavares, N., Vilas-Boas, J. P., & Castro, M. A. (2025). Effect of Preventive Exercise Programs for Swimmer’s Shoulder Injury on Rotator Cuff Torque and Balance in Competitive Swimmers: A Randomized Controlled Trial. Healthcare, 13(5), 538. https://doi.org/10.3390/healthcare13050538