

Identifying the Bundle/Care Development Process in Clinical Risk Management: A Systematic Review

 ,
,  , and
, and
Abstract
1. Introduction
2. Methods
2.1. Study Protocol
2.2. Literature Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction and Study Quality
2.5. Data Synthesis
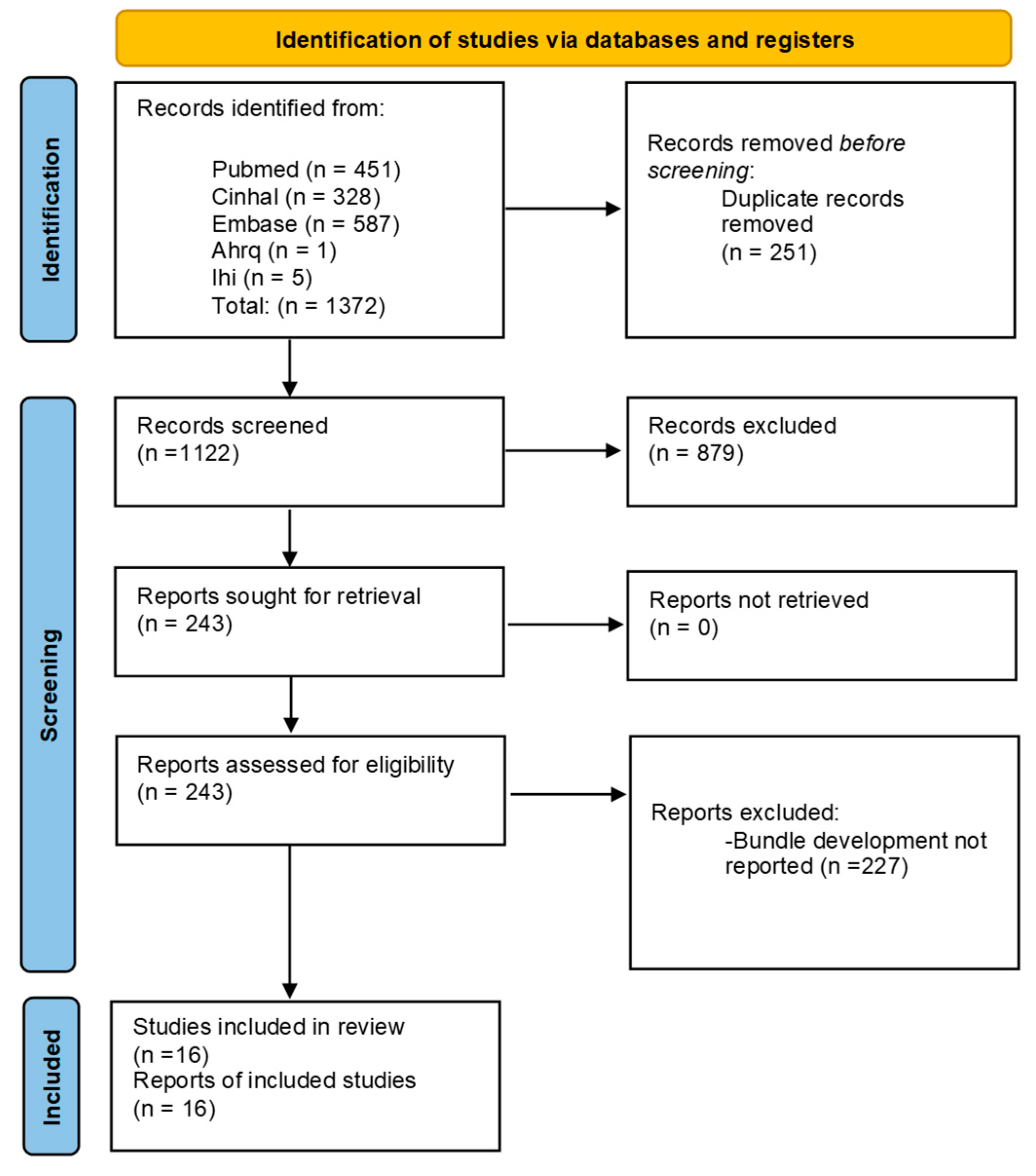
3. Results
Overview
4. Discussion
4.1. Principal Findings
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Resar, R.; Griffin, F.A.; Haraden, C.; Nolan, T.W. Using Care Bundles to Improve Health Care Quality; IHI Innovation Series White Paper; Institute for Healthcare Improvement: Cambridge, MA, USA, 2012; Available online: https://www.ihi.org/ (accessed on 1 September 2023).
- Ruscitti, L.E.; Puro, V. L‘utilizzo dei bundle nella pratica clinica. Infez Med. 2008, 16, 121–129. (In Italian) [Google Scholar] [PubMed]
- Nguyen, H.B.; Jaehne, A.K.; Jayaprakash, N.; Semler, M.W.; Hegab, S.; Yataco, A.C.; Tatem, G.; Salem, D.; Moore, S.; Boka, K.; et al. Early goal-directed therapy in severe sepsis and septic shock: Insights and comparisons to ProCESS, ProMISe, and ARISE. Crit. Care 2016, 20, 160. [Google Scholar] [CrossRef] [PubMed]
- Buongiorno, L.; Mele, F.; Solarino, B.; Ferorelli, D.; Zotti, F.; Dell’erba, A.; Carabellese, F.F.; Catanesi, R.; Ferracuti, S.; Mandarelli, G. Falls in the hospital: An Italian clinical risk management perspective. J. Patient Saf. Risk Manag. 2024, 29, 165–172. [Google Scholar] [CrossRef]
- Wachter, R.M.; Pronovost, P.J. The 100,000 lives campaign: A scientific and policy review. Jt. Comm. J. Qual. Patient Saf. 2006, 32, 621–627. [Google Scholar] [CrossRef]
- Arroliga, A.C.; Pollard, C.L.; Wilde, C.D.; Pellizzari, S.J.; Chebbo, A.; Song, J.; Ordner, J.; Cormier, S.; Meyer, T. Reduction in the incidence of ventilator-associated pneumonia: A multidisciplinary approach. Respir. Care 2012, 57, 688–696. [Google Scholar] [CrossRef]
- Damiani, E.; Donati, A.; Serafini, G.; Rinaldi, L.; Adrario, E.; Pelaia, P.; Busani, S.; Girardis, M. Effetto dei programmi di miglioramento delle prestazioni sulla compliance con i bundle di sepsi e sulla mortalità: Una revisione sistematica e una meta-analisi di studi osservazionali. PLoS ONE 2015, 10, e0125827. [Google Scholar] [CrossRef]
- Levy, M.M.; Dellinger, R.P.; Townsend, S.R.; Linde-Zwirble, W.T.; Marshall, J.C.; Bion, J.; Schorr, C.; Artigas, A.; Ramsay, G.; Beale, R.; et al. The Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Crit. Care Med. 2010, 38, 367–374. [Google Scholar] [CrossRef]
- Moro, M.; Pan, A.; Parenti, M.; Marcelli, E. Prevention of Surgical Site Infections; Emilia-Romagna Regional Health and Social Agency: Bologna, Italy, 2017. [Google Scholar]
- Horner, D.L.; Bellamy, M.C. Care bundles in intensive care. Contin. Educ. Anaesth. Crit. Care Pain 2012, 12, 199–202. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Andiman, S.E.; Xu, X.; Boyce, J.M.; Ludwig, E.M.B.; Rillstone, H.R.W.; Desai, V.B.; Fan, L.L. Decreased Surgical Site Infection Rate in Hysterectomy: Effect of a Gynecology-Specific Bundle. Obstet. Gynecol. 2018, 131, 991–999. [Google Scholar] [CrossRef]
- Andreessen, L.D.; Wilde, M.H.P.; Herendeen, P.D. Preventing catheter-associated urinary tract infections in acute care: The bundle approach. J. Nurs. Care Qual. 2012, 27, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Anthony, T.; Murray, B.W.; Sum-Ping, J.T.; Lenkovsky, F.; Vornik, V.D.; Parker, B.J.; McFarlin, J.E.; Hartless, K.; Huerta, S. Evaluating an evidence-based bundle for preventing surgical site infection: A randomized trial. Arch. Surg. 2011, 146, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Bruce, H.R.; Maiden, J.; Fedullo, P.F.; Kim, S.C. Impact of nurse-initiated ED sepsis protocol on compliance with sepsis bundles, time to initial antibiotic administration, and in-hospital mortality. J. Emerg. Nurs. 2015, 41, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Bullock, M.W.; Brown, M.L.; Bracey, D.N.; Langfitt, M.K.; Shields, J.S.; Lang, J.E. A Bundle Protocol to Reduce the Incidence of Periprosthetic Joint Infections After Total Joint Arthroplasty: A Single-Center Experience. J. Arthroplast. 2017, 32, 1067–1073. [Google Scholar] [CrossRef]
- Davidson, C.; Enns, J.; Dempster, C.; Lundeen, S.; Eppes, C. Impact of a surgical site infection bundle on cesarean delivery infection rates. Am. J. Infect. Control 2020, 48, 555–559. [Google Scholar] [CrossRef]
- Davidson, C.; Enns, J.; Bennett, C.; Sangi-Haghpeykar, H.; Lundeen, S.; Eppes, C. Reducing abdominal hysterectomy surgical site infections: A multidisciplinary quality initiative. Am. J. Infect. Control 2020, 48, 1292–1297. [Google Scholar] [CrossRef]
- Muller, M.; Bryant, K.A.; Espinosa, C.; Jones, J.A.; Quach, C.; Rindels, J.R.; Stewart, D.L.; Zangwill, K.M.; Sánchez, P.J. SHEA Neonatal Intensive Care Unit (NICU) White Paper Series: Practical approaches for the prevention of central-line–associated bloodstream infections. Infect. Control Hosp. Epidemiol. 2023, 44, 550–564. [Google Scholar] [CrossRef]
- Rosgen, B.K.; Plotnikoff, K.M.; Krewulak, K.D.; Shahid, A.; Hernandez, L.; Sept, B.G.; Morrissey, J.; Robertson, K.; Fraser, N.; Niven, D.J.; et al. Co-development of a transitions in care bundle for patient transitions from the intensive care unit: A mixed-methods analysis of a stakeholder consensus meeting. BMC Health Serv. Res. 2022, 22, 10. [Google Scholar] [CrossRef]
- Speck, K.; Rawat, N.; Weiner, N.C.; Tujuba, H.G.; Farley, D.; Berenholtz, S. A systematic approach for developing a ventilator-associated pneumonia prevention bundle. Am. J. Infect. Control 2016, 44, 652–656. [Google Scholar] [CrossRef]
- Acun, A.; Şencan, I.; Sendağ, E.; Sevinç, G.; Tekin, A.; Callak Oku, F.; Çalışkan, N. Assessing the Efficacy of Ventilator-Associated Event Prevention Bundle in the Intensive Care Units: An Intervention Study. Int. J. Caring Sci. 2021, 14, 1619–1626. Available online: https://www.internationaljournalofcaringsciences.org/docs/8_aysun_original_14_3.pdf (accessed on 1 September 2023).
- Baldwin, L.N.; Smith, S.A.; Fender, V.; Gisby, S.; Fraser, J. An audit of compliance with the sepsis resuscitation care bundle in patients admitted to A&E with severe sepsis or septic shock. Int. Emerg. Nurs. 2008, 16, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Borgert, M.; Binnekade, J.; Paulus, F.; Goossens, A.; Dongelmans, D. A flowchart for building evidence-based care bundles in intensive care: Based on a systematic review. Int. J. Qual. Health Care 2017, 29, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Dieplinger, B.; Egger, M.; Jezek, C.; Heinisch-Finke, C.; Altendorfer, C.; Pernerstorfer, T.; Hefler, L.; Pateisky, N.; Mueller, T. Implementation of a comprehensive unit-based safety program to reduce surgical site infections in cesarean delivery. Am. J. Infect. Control 2020, 48, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Giles, M.; Watts, W.; O’brien, A.; Berenger, S.; Paul, M.; McNeil, K.; Bantawa, K. Does Our Bundle Stack up! Innovative Nurse-Led Changes for Preventing Catheter-Associated Urinary Tract Infection (CAUTI). Health Infect. 2015, 20, 62–71. [Google Scholar] [CrossRef]

{kind=link}
| First Author (Year of Publication) | Title | Country | Situation Risk | Method of Developing |
|---|---|---|---|---|
| Acun A (2022) [22]. | Assessing the Efficacy of Ventilator-Associated Event Prevention bundles in the Intensive Care Units: An Intervention Study | Turkey | VAP 1 |
|
| Andiman SE (2018) [12]. | Decreased Surgical Site Infection Rate in Hysterectomy: Effect of a Gynecology-Specific bundle | USA 3 | SSI 4 |
|
| Andreessen L (2012) [13]. | Preventing catheter-associated urinary tract infections in acute care: the bundle approach | USA | CAUTI 5 |
|
| Anthony T (2011) [14]. | Evaluating an evidence-based bundle for preventing surgical site infection: a randomized trial. | USA | SSI |
|
| Baldwin LN (2008) [23]. | An audit of compliance with the sepsis resuscitation care bundle in patients admitted to A&E with severe sepsis or septic shock | United Kingdom | SEPSIS 6 |
|
| Borgert M (2017) [24]. | A flowchart for building evidence-based care bundles in intensive care: based on a systematic review | Netherlands | VAP; CLABSI 7 |
|
| Bruce HR (2015) [15]. | Impact of nurse-initiated ed sepsis protocol on compliance with sepsis bundles, time to initial antibiotic administration, and in-hospital mortality | USA | SEPSIS |
|
| Bullock MW (2017) [16]. | A bundle Protocol to Reduce the Incidence of Periprosthetic Joint Infections After Total Joint Arthroplasty: A Single-Centre Experience | USA | INFECTIONS |
|
| Davidson C (2020) [17]. | Impact of a surgical site infection bundle on caesarean delivery infection rates | USA | SSI |
|
| Davidson C (2020) [18]. | Reducing abdominal hysterectomy surgical site infections: A multidisciplinary quality initiative | USA | SSI |
|
| Dieplinger B (2020) [25]. | Implementation of a comprehensive unit-based safety programme to reduce surgical site infections in caesarean delivery | Austria | SSI |
|
| Giles M (2015) [26]. | Does our bundle stack up! Innovative nurse-led changes for preventing catheter-associated urinary tract infection (CAUTI) | Australia | CAUTI |
|
| Muller M (2023) [19]. | Neonatal Intensive Care Unit (NICU) White Paper Series: Practical approaches for the prevention of central-line-associated bloodstream infections | USA | CLABSI |
|
| Resar R (2012) [1]. | Using Care Bundles to Improve Health Care Quality | USA | VAP; CLABSI |
|
| Rosgen BK (2022) [20]. | Co-development of a transitions in care bundle for patient transitions from the intensive care unit: a mixed-methods analysis of a stakeholder consensus meeting. | Canada | TRANSITIONS |
|
| Speck K. (2016) [21]. | A systematic approach for developing a ventilator-associated pneumonia prevention bundle | USA | VAP |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sebastiani, E.; Scacchetti, M.; Cesare, M.; Maurici, M.; Loiudice, M.T. Identifying the Bundle/Care Development Process in Clinical Risk Management: A Systematic Review. Healthcare 2024, 12, 2242. https://doi.org/10.3390/healthcare12222242
Sebastiani E, Scacchetti M, Cesare M, Maurici M, Loiudice MT. Identifying the Bundle/Care Development Process in Clinical Risk Management: A Systematic Review. Healthcare. 2024; 12(22):2242. https://doi.org/10.3390/healthcare12222242
Chicago/Turabian StyleSebastiani, Emanuele, Marina Scacchetti, Manuele Cesare, Massimo Maurici, and Michele Tancredi Loiudice. 2024. "Identifying the Bundle/Care Development Process in Clinical Risk Management: A Systematic Review" Healthcare 12, no. 22: 2242. https://doi.org/10.3390/healthcare12222242
APA StyleSebastiani, E., Scacchetti, M., Cesare, M., Maurici, M., & Loiudice, M. T. (2024). Identifying the Bundle/Care Development Process in Clinical Risk Management: A Systematic Review. Healthcare, 12(22), 2242. https://doi.org/10.3390/healthcare12222242