
Use of the Therapy App Prescinde for Increasing Adherence to Smoking Cessation Treatment

 , ,
, ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Collection
2.3. Description of the Therapy App Prescinde
2.4. Participants
2.5. Measurements and Variables
2.5.1. Study Variables
- -
- Frequency of use (number of times the participant uses the app);
- -
- Time spent on the app (time), divided into 4 categories: (1) 1 week, (2) 1 month, (3) 3 months, and (4) more than 3 months;
- -
- Adherence1, understood as having been using the app for at least 1 month, categorized as 1 (adherence) and 0 (non-adherence);
- -
- Adherence3, understood as having been using the app for more than 3 months, categorized as 1 (adherence) and 0 (non-adherence).
2.5.2. Sociodemographic Variables
- -
- Gender, divided into two groups: (1) male, and (2) female;
- -
- Academic status (studying), divided into 2 categories: (1) no or (2) yes;
- -
- Employment status (working), divided into 2 categories: (1) no or (2) yes;
- -
- Tobacco use, divided into 2 categories: (1) no or (2) yes;
- -
- Cannabis use, divided into 2 categories: (1) no or (2) yes;
- -
- Age, divided into 3 groups: Group 1 (aged between 17 and 18 years), Group 2 (aged between 19 and 25 years), and Group 3 (aged between 26 and 62 years);
- -
- Main activity on the app, divided into 3 categories: (1) stop smoking tobacco (tobacco), (2) stop smoking cannabis (cannabis), and (3) physical exercise (physical exercise);
- -
- Level of education, divided into 3 categories: (1) high school; (2) bachelor degree, and (3) master/doctorate;
- -
- Occupation, divided into 8: (1) public administration, (2) agriculture/fishing, (3) trade, (4) private company manager, (5) hospitality/tourism, (6) technical professional, (7) transportation, and (8) unemployed.
3. Results
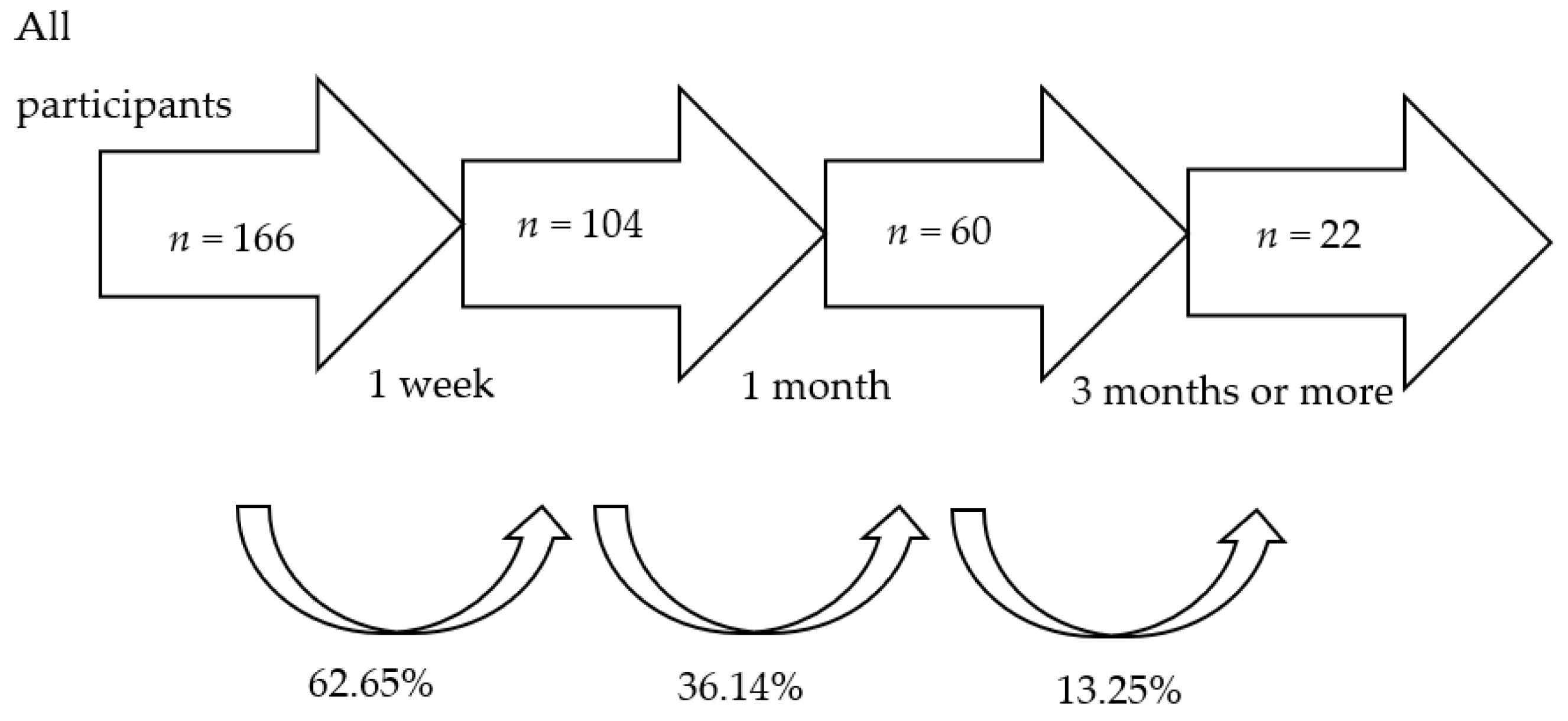
3.1. Time of Adherence
3.2. Frequency of Use
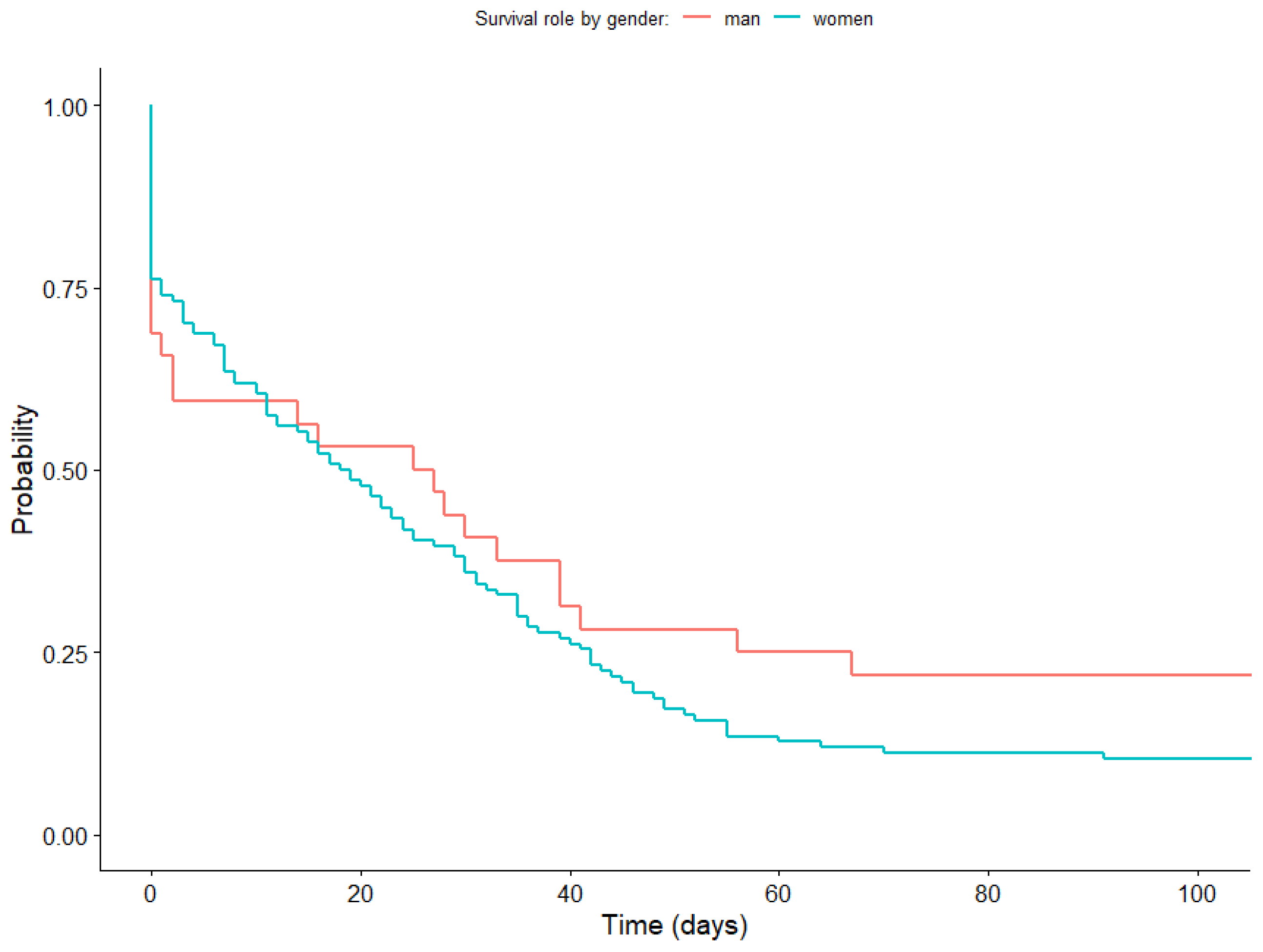
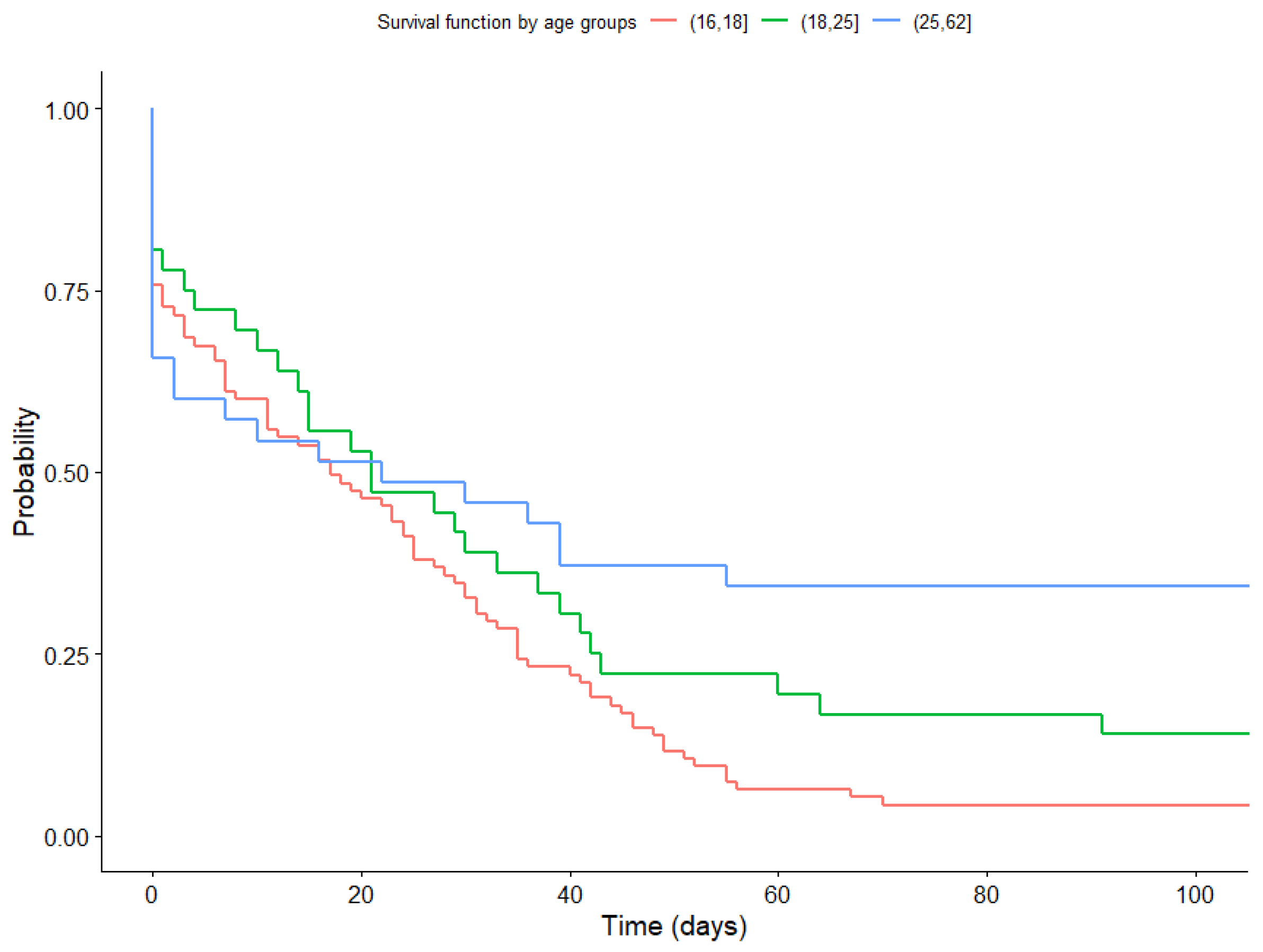
3.3. Probability of Total Adherence as a Function of Gender and Age: Survival Analysis
3.4. Probability of Adherence Based on the Main Activity: Survival Analysis
3.5. Nonparametric Analysis of Continuous Variables: Frequency of Usage and Time Elapsed from the First to the Last Usage of the Prescinde Therapy App and the Relationship with Sociodemographic Variables
3.6. Nonparametric Analysis of Qualitative Variables: Adherence and Its Relationship with Sociodemographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rey-Brandariz, J.; Pérez-Ríos, M.; Santiago-Pérez, M.I.; Varela-Lema, L.; Giraldo-Osorio, A.; Mourino, N.; Ruano-Ravina, A. Smoking-attributable mortality in Spain: A systematic review. Addictions 2023, 35, 1619. [Google Scholar] [CrossRef]
- Chu, A.; Chaiton, M.; Kaufman, P.; Goodwin, R.D.; Lin, J.; Hindocha, C.; Goodman, S.; Hammond, D. Co-Use, Simultaneous Use, and Mixing of Cannabis and Tobacco: A Cross-National Comparison of Canada and the US by Cannabis Administration Type. Int. J. Environ. Res. Public Health 2023, 20, 4206. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. World Health Organization. 2012. Available online: https://www3.paho.org/hq/index.php (accessed on 1 November 2023).
- Wallach, J.D.; Egilman, A.C.; Dhruva, S.S.; E McCarthy, M.; E Miller, J.; Woloshin, S.; Schwartz, L.M.; Ross, J.S. Postmarket studies required by the US Food and Drug Administration for new drugs and biologics approved between 2009 and 2012: Cross sectional analysis. BMJ 2018, 361, k2031. [Google Scholar] [CrossRef] [PubMed]
- Hammerich, A.; El-Awa, F.; Latif, N.A.; El-Gohary, S.; Borrero, M.D.L. Tobacco is a threat to the environment and human health. East Mediterr. Health J. 2022, 28, 319–320. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hecht, S.S. Carcinogenic components of tobacco and tobacco smoke: A 2022 update. Food Chem. Toxicol. 2022, 165, 113179. [Google Scholar] [CrossRef] [PubMed]
- Spanish Observatory on Drugs and Addictions. Ministry of Health, Social Services and Equality: Madrid, Spain. Report 2022. Available online: https://pnsd.sanidad.gob.es/profesionales/sistemasInformacion/sistemaInformacion/pdf/2022_Informe_Ejecutivo_EDADES_en.pdf (accessed on 8 January 2023).
- Cavalli, J.M.; Cservenka, A.; Kerr, D.C.R.; Tiberio, S.S.; Owen, L.D. Ratings of executive function as a risk factor for adolescents’ frequent cannabis use: A prospective longitudinal study. Psychol. Addict. Behav. 2023, 37, 616–625. [Google Scholar] [CrossRef]
- Rup, J.; Freeman, T.P.; Perlman, C.; Hammond, D. Cannabis and mental health: Prevalence of use and modes of cannabis administration by mental health status. Addict. Behav. 2021, 121, 106991. [Google Scholar] [CrossRef]
- González-Ortega, I.; Echeburúa, E.; Alberich, S.; Bernardo, M.; Vieta, E.; de Pablo, G.S.; González-Pinto, A. Cognitive Behavioral Therapy Program for Cannabis Use Cessation in First-Episode Psychosis Patients: A 1-Year Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 7325. [Google Scholar] [CrossRef]
- Martínez-Vispo, C.; Rodríguez-Cano, R.; López-Durán, A.; Senra, C.; Fernández Del Río, E.; Becoña, E. Cognitive-behavioral treatment with behavioral activation for smoking cessation: Randomized controlled trial. PLoS ONE 2019, 14, e0214252. [Google Scholar] [CrossRef]
- Ouellette, M.J.; Rowa, K.; Cameron, D.H.; Elcock, A.; Soreni, N.; Pawluk, E.J.; McCabe, R.E. Does cannabis use impact cognitive behavioural therapy outcomes for anxiety and related disorders? A preliminary examination. J. Psychiatr. Res. 2022, 156, 690–697. [Google Scholar] [CrossRef]
- Rajani, N.B.; Mastellos, N.; Filippidis, F.T. Self-Efficacy and Motivation to Quit of Smokers Seeking to Quit: Quantitative Assessment of Smoking Cessation Mobile Apps. JMIR mHealth uHealth 2021, 9, e25030. [Google Scholar] [CrossRef] [PubMed]
- Dono, J.; Martin, K.; Bowden, J.; Miller, C. A population-level analysis of changes in Australian smokers’ preferences for smoking cessation support over two decades—From 1998 to 2017. Lancet Reg. Health West. Pac. 2021, 19, 100342. [Google Scholar] [CrossRef] [PubMed]
- Schnall, R.; Liu, J.; Alvarez, G.; Porras, T.; Ganzhorn, S.; Boerner, S.; Huang, M.-C.; Trujillo, P.; Cioe, P. A Smoking Cessation Mobile App for Persons Living with HIV: Preliminary Efficacy and Feasibility Study. JMIR Form. Res. 2022, 6, e28626. [Google Scholar] [CrossRef] [PubMed]
- Soulakova, J.N.; Crockett, L.J. Unassisted Quitting and Smoking Cessation Methods Used in the United States: Analyses of 2010–2011 Tobacco Use Supplement to the Current Population Survey Data. Nicotine Tob. Res. 2017, 20, 30–39. [Google Scholar] [CrossRef]
- Alarcó-Rosales, R.; Sánchez-SanSegundo, M.; Ferrer-Cascales, R.; Albaladejo-Blazquez, N.; Lordan, O.; Zaragoza-Martí, A. Effects of a School-Based Intervention for Preventing Substance Use among Adolescents at Risk of Academic Failure: A Pilot Study of the Reasoning and Rehabilitation V2 Program. Healthcare 2021, 9, 1488. [Google Scholar] [CrossRef] [PubMed]
- Mersha, A.G.; Eftekhari, P.; Bovill, M.; Tollosa, D.N.; Gould, G.S. Evaluating level of adherence to nicotine replacement therapy and its impact on smoking cessation: A systematic review and meta-analysis. Arch. Public Health 2021, 79, 26. [Google Scholar] [CrossRef] [PubMed]
- Klemperer, E.M.; Streck, J.M.; Lindson, N.; West, J.C.; Su, A.; Hughes, J.R.; Carpenter, M.J. A systematic review and meta-analysis of interventions to induce attempts to quit tobacco among adults not ready to quit. Exp. Clin. Psychopharmacol. 2023, 31, 541–559. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, N.A.; Kruse, G.R.; Livingstone-Banks, J.; Hartmann-Boyce, J. Treatment of Tobacco Smoking: A Review. JAMA 2022, 327, 566–577. [Google Scholar] [CrossRef]
- Lappan, S.N.; Brown, A.W.; Hendricks, P.S. Dropout rates of in-person psychosocial substance use disorder treatments: A systematic review and meta-analysis. Addiction 2020, 115, 201–217. [Google Scholar] [CrossRef]
- Leal, I.M.; Taing, M.; Correa-Fernández, V.; Obasi, E.M.; Kyburz, B.; Le, K.; Koshy, L.; Chen, T.A.; Williams, T.; Casey, K.; et al. Addressing Smoking Cessation among Women in Substance Use Treatment: A Qualitative Approach to Guiding Tailored Interventions. Int. J. Environ. Res. Public Health 2021, 18, 5764. [Google Scholar] [CrossRef]
- Martínez, A.M.; Pérez-Ríos, M.; Ortiz, C.; See, G.; Labaca, I.G. Changes in smoking cessation in Spain, 1987–2020. Med. Clin. (Engl. Ed.) 2023, 160, 237–244. [Google Scholar] [CrossRef]
- Niedzin, M.; Gaszyńska, E.; Krakowiak, J.; Saran, T.; Szatko, F.; Kaleta, D. Gender, age, social disadvantage and quitting smoking in Argentina and Uruguay. Ann. Agric. Environ. Med. 2018, 25, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Bessette, A.J.; Weinberger, A.H.; Sheffer, C.E.; McKee, S.A. Sex/gender differences in smoking cessation: A review. Prev. Med. 2016, 92, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Ding, Q.; Shen, J.; Qu, H.; Meng, X. A 28-day challenge to help quit smoking using telephone follow-ups combined with the WeChat app: The impact of the humanistic approach on smoking cessation. J. Addict. Nurs. 2021, 32, 211–215. [Google Scholar] [CrossRef]
- Avşar, T.S.; Jackson, L.; Barton, P.; Jones, M.; McLeod, H. Supporting pregnant women not ready to quit smoking: An economic evaluation. BMC Pregnancy Childbirth. 2022, 22, 865. [Google Scholar] [CrossRef]
- Beard, E.; Brown, J.; E Jackson, S.; West, R.; Kock, L.; Boniface, S.; Shahab, L. Independent Associations between Different Measures of Socioeconomic Position and Smoking Status: A Cross-Sectional Study of Adults in England. Nicotine Tob. Res. 2021, 23, 107–114. [Google Scholar] [CrossRef]
- Meijer, E.; Korst, J.S.; Oosting, K.G.; Heemskerk, E.; Hermsen, S.; Willemsen, M.C.; Putte, B.V.D.; Chavannes, N.H.; Brown, J. At least someone thinks I’m doing well: A real-world evaluation of the quit-smoking app StopCoach for lower socio-economic status smokers. Addict. Sci. Clin. Pract. 2021, 16, 48. [Google Scholar] [CrossRef]
- Roberts, V.; Maddison, R.; Simpson, C.; Bullen, C.; Prapavessis, H. The acute effects of exercise on cigarette cravings, withdrawal symptoms, affect, and smoking behaviour: Systematic review update and meta-analysis. Psychopharmacology 2012, 222, 1–15. [Google Scholar] [CrossRef]
- Underner, M.; Perriot, J.; Peiffer, G.; Meurice, J.C. The efficacy of physical activity as an aid to smoking cessation. Rev. Mal. Respir. 2015, 32, 1016–1033. [Google Scholar] [CrossRef]
- Alphonse, A.; Stewart, K.; Brown, J.; Perski, O. Exploring Users’ Experiences with a Quick-Response Chatbot within a Popular Smoking Cessation Smartphone App: Semistructured Interview Study. JMIR Form. Res. 2022, 6, e36869. [Google Scholar] [CrossRef]
- Dubad, M.; Winsper, C.; Meyer, C.; Livanou, M.; Marwaha, S. A systematic review of the psychometric properties, usability and clinical impacts of mobile mood-monitoring applications in young people. Psychol. Med. 2018, 48, 208–228. [Google Scholar] [CrossRef] [PubMed]
- Mclaughlin, M.; Delaney, T.; Hall, A.; Byaruhanga, J.; Mackie, P.; Grady, A.; Reilly, K.; Campbell, E.; Sutherland, R.; Wiggers, J.; et al. Associations between Digital Health Intervention Engagement, Physical Activity, and Sedentary Behavior: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e23180. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.G.; Steinberg, D.; Askew, S.; Levine, E.; Foley, P.; Batch, B.C.; Svetkey, L.P.; Bosworth, H.B.; Puleo, E.M.; Brewer, A.; et al. Effectiveness of an App and Provider Counseling for Obesity Treatment in Primary Care. Am. J. Prev. Med. 2018, 55, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Haskins, B.L.; Lesperance, D.; Gibbons, P.; Boudreaux, E.D. A systematic review of smartphone applications for smoking cessation. Transl. Behav. Med. 2017, 7, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Vederhus, J.K.; Rørendal, M.; Bjelland, C.; Skar, A.K.S.; Kristensen, Ø. Can a Smartphone App for Cannabis Cessation Gain a Broader User Group than Traditional Treatment Services? Subst. Abuse 2020, 14, 1178221820902237. [Google Scholar] [CrossRef] [PubMed]
- Bricker, J.B.; Mull, K.E.; Santiago-Torres, M.; Miao, Z.; Perski, O.; Di, C. Smoking Cessation Smartphone App Use Over Time: Predicting 12-Month Cessation Outcomes in a 2-Arm Randomized Trial. J. Med. Internet Res. 2022, 24, e39208. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Rogers, E.S.; Cupertino, P.; Zhao, X.; Cartujano-Barrera, F.; Lyu, J.C.; Hu, L.; Sherman, S.E. Development of a WeChat-based Mobile Messaging Smoking Cessation Intervention for Chinese Immigrant Smokers: Qualitative Interview Study. JMIR Form. Res. 2022, 6, e36091. [Google Scholar] [CrossRef]
- Hoepper, B.B.; Siegel, K.R.; A Carlon, H.; Kahler, C.W.; Park, E.R.; Taylor, S.T.; Simpson, H.V.; Hoeppner, S.S. Feature-Level Analysis of a Smoking Cessation Smartphone App Based on a Positive Psychology Approach: Prospective Observational Study. JMIR Form. Res. 2022, 6, e38234. [Google Scholar] [CrossRef]
- Jardine, J.; Bowman, R.; Doherty, G. Digital Interventions to Enhance Readiness for Psychological Therapy: Scoping Review. J. Med. Internet Res. 2022, 24, e37851. [Google Scholar] [CrossRef]
- López-Durán, A.; Becoña, E.; Senra, C.; Suárez-Castro, D.; Barroso-Hurtado, M.; Martínez-Vispo, C.A. Randomized Clinical Trial to Assess the Efficacy of a Psychological Treatment to Quit Smoking Assisted with an App: Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 9770. [Google Scholar] [CrossRef]
- Regmi, D.; Tobutt, C.; Shaban, S. Quality and use of free smoking cessation app for smartphones. Int. J. Technol. Assess. Health Care 2018, 34, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Heckathorn, D.D. Respondent-driven sampling: A new approach to the study of hidden populations. Soc. Probl. 1997, 44, 174–199. [Google Scholar] [CrossRef]
- Sánchez-Borrego, I.; Rueda, M.D.M.; Mullo, H. Estimation of Non-Linear Parameters with Data Collected Using Respondent-Driven Sampling. Mathematics 2020, 8, 1315. [Google Scholar] [CrossRef]
- Ferri-García, R.; Rueda, M.M. Efficiency of propensity score adjustment and calibration on the estimation from non-probabilistic online surveys. SORT Stat. Oper. Res. Trans. 2018, 42, 0159–0182. [Google Scholar]
- Ferri-García, R.; Rueda, M.M. Propensity score adjustment using machine learning classification algorithms to control selection bias in online surveys. PLoS ONE 2020, 15, e0231500. [Google Scholar] [CrossRef] [PubMed]
- Ferri-García, R.; Rueda, M.M.; Cabrera-León, A. Self-Perceived Health, Life Satisfaction and Related Factors among Healthcare Professionals and the General Population: Analysis of an Online Survey, with Propensity Score Adjustment. Mathematics 2021, 9, 791. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Treat. Rep. 1966, 50, 163–170. [Google Scholar]
- Kolmogorov, A. Sulla Determinazione Empirica di Una Legge di Distribuzione. Giorn. Dell’inst. Ital. Degli. Att. 1933, 4, 83–91. [Google Scholar]
- Smirnov, N. Table for Estimating the Goodness of Fit of Empirical Distributions. Ann. Math. Stat. 1948, 19, 279–281. [Google Scholar] [CrossRef]
- Mann, H.B.; Whitney, D.R. On a test of whether one of two random variables is stochastically lagers than the other. Ann. Math. Stat. 1947, 18, 50–60. [Google Scholar] [CrossRef]
- Wilcoxon, F. Individual Comparisons by Ranking Methods. Bibliometr. Bul. 1945, 1, 80–83. [Google Scholar] [CrossRef]
- Kruskal, W.H.; Wallis, W.A. Use of Ranks in One-Criterion Variance Analysis. J. Am. Stat. Assoc. 1952, 47, 583–621. [Google Scholar] [CrossRef]
- Pearson, K. Contributions to the mathematical theory of evolution. Philos. Trans. R. Soc. Lond. A 1894, 185, 71–110. [Google Scholar]
- Hawn, S.E.; Cusack, S.E.; Amstadter, A.B. A Systematic Review of the Self-Medication Hypothesis in the Context of Posttraumatic Stress Disorder and Comorbid Problematic Alcohol Use. J. Trauma Stress 2020, 33, 699–708. [Google Scholar] [CrossRef]
- Bauer, A.G.; Ruglass, L.M.; Shevorykin, A.; Saraiya, T.C.; Robinson, G.; Cadet, K.; Julien, L.; Chao, T.; Hien, D. Predictors of therapeutic alliance, treatment feedback, and clinical outcomes among African American women in treatment for co-occurring PTSD and SUD. J. Subst. Abuse Treat. 2022, 1, 39. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age | Main Activity | ||||||
|---|---|---|---|---|---|---|---|---|
| Male | Female | (17–18) | (19–25) | (26–62) | Physical Exercise | Cannabis | Tobacco | |
| Education level | ||||||||
| High School | 12 | 70 | 58 | 16 | 8 | 62 | 4 | 16 |
| Bachelor degree | 13 | 49 | 37 | 10 | 15 | 38 | 1 | 23 |
| Master/Doctorate | 7 | 15 | 10 | 12 | 13 | 1 | 8 | |
| Currently studying | ||||||||
| No | 9 | 13 | 4 | 18 | 11 | 3 | 8 | |
| Yes | 23 | 121 | 95 | 32 | 17 | 102 | 3 | 39 |
| Profession | ||||||||
| Public Administration | 7 | 8 | 2 | 13 | 7 | 8 | ||
| Agriculture/Fishing | 1 | 1 | 1 | |||||
| Trade | 2 | 1 | 1 | 1 | 1 | |||
| Private Company Manager | 2 | 1 | 1 | 1 | 1 | |||
| Hospitality/tourism | 1 | 4 | 3 | 2 | 2 | 1 | 2 | |
| Technical professional | 5 | 12 | 2 | 7 | 8 | 10 | 1 | 6 |
| Transportation | 1 | 1 | 2 | 2 | ||||
| Unemployed | 16 | 106 | 90 | 25 | 7 | 92 | 3 | 27 |
| Time | ||||||||
| 1 week | 13 | 49 | 37 | 10 | 15 | 38 | 4 | 20 |
| 1 month | 6 | 37 | 27 | 12 | 4 | 29 | 14 | |
| 3 months | 6 | 33 | 27 | 8 | 4 | 25 | 2 | 12 |
| More than 3 months | 7 | 15 | 4 | 6 | 12 | 21 | 1 | |
| Adherence1 (1 month) | ||||||||
| Yes | 13 | 48 | 31 | 14 | 16 | 46 | 2 | 13 |
| No | 19 | 86 | 64 | 22 | 19 | 67 | 4 | 34 |
| Adherence3 (more than 3 months) | ||||||||
| Yes | 7 | 15 | 4 | 6 | 12 | 21 | 0 | 1 |
| No | 25 | 119 | 91 | 30 | 23 | 92 | 6 | 46 |
| Gender | Age | Main Activity | ||||||
|---|---|---|---|---|---|---|---|---|
| Time | Male | Female | (17–18) | (19–25) | (26–62) | Physical Exercise | Cannabis | Tobacco |
| 1 week | 4.385 | 2.612 | 2.405 | 1.600 | 5.333 | 2.263 | 5.500 | 3.850 |
| 1 month | 14.333 | 9.621 | 9.519 | 10.833 | 13.750 | 8.897 | 13.143 | |
| 3 months | 96.333 | 22.091 | 20.889 | 44.375 | 97.000 | 15.640 | 25.000 | 72.166 |
| More than 3 months | 153.000 | 118.067 | 118.750 | 132.167 | 131.167 | 134.476 | 18.000 | |
| Frequency of Use | Time | |
|---|---|---|
| Gender | 0.133 | 0.726 |
| Studying | 0.665 | 0.297 |
| Working | 0.828 | 0.245 |
| Tobacco Consumption | 0.015 * | 0.337 |
| Cannabis Consumption | 0.012 * | 0.197 |
| Age | 0.048 * | 0.416 |
| Main activity | 0.856 | 0.059 |
| Education level | 0.017 * | 0.021 * |
| Profession | 0.196 | 0.216 |
| Adherence1 | Adherence3 | |
|---|---|---|
| Gender | 0.764 | 0.190 |
| Studying | 1.000 | 0.081 |
| Working | 0.713 | 0.160 |
| Tobacco Consumption | 0.338 | 0.010 ** |
| Cannabis Consumption | 0.388 | 0.010 * |
| Age | 0.373 | 0.010 ** |
| Main activity | 0.292 | 0.012 * |
| Education level | 0.148 | 0.010 ** |
| Profession | 0.648 | 0.034 * |
| Variables | Comparative Groups | p-Value | |
|---|---|---|---|
| Age | Adherence3 | (17–18)–(19–25) | 0.043 * |
| (17–18)–(26–62) | 0.010 ** | ||
| (19–25)–(26–62) | 0.152 | ||
| Main activity | Adherence3 | Cannabis–Physical exercise | 0.539 |
| Cannabis–Tobacco | 0.010 ** | ||
| Physical exercise–Tobacco | 0.012 * | ||
| Education level | Frequency of use | High School–Bachelor degree | 0.112 |
| High School–Master/Doctorate | 0.466 | ||
| Bachelor degree–Master/Doctorate | 0.039 * | ||
| Education level | Adherence3 | High School–Bachelor degree | 0.045 * |
| High School–Master/Doctorate | 0.046 * | ||
| Bachelor degree–Master/Doctorate | 0.010 ** | ||
| Profession | Adherence3 | Public administration–Unemployed | 0.012 |
| Technical Professional–Unemployed | 0.026 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Torrecillas, F.; Ramírez-Uclés, I.; Rueda, M.d.M.; Cobo-Rodríguez, B.; Castro-Martín, L.; Urrea-Castaño, S.A.; Muñoz-López, L. Use of the Therapy App Prescinde for Increasing Adherence to Smoking Cessation Treatment. Healthcare 2023, 11, 3121. https://doi.org/10.3390/healthcare11243121
López-Torrecillas F, Ramírez-Uclés I, Rueda MdM, Cobo-Rodríguez B, Castro-Martín L, Urrea-Castaño SA, Muñoz-López L. Use of the Therapy App Prescinde for Increasing Adherence to Smoking Cessation Treatment. Healthcare. 2023; 11(24):3121. https://doi.org/10.3390/healthcare11243121
Chicago/Turabian StyleLópez-Torrecillas, Francisca, Isabel Ramírez-Uclés, María del Mar Rueda, Beatriz Cobo-Rodríguez, Luis Castro-Martín, Sabina Arantxa Urrea-Castaño, and Lucas Muñoz-López. 2023. "Use of the Therapy App Prescinde for Increasing Adherence to Smoking Cessation Treatment" Healthcare 11, no. 24: 3121. https://doi.org/10.3390/healthcare11243121
APA StyleLópez-Torrecillas, F., Ramírez-Uclés, I., Rueda, M. d. M., Cobo-Rodríguez, B., Castro-Martín, L., Urrea-Castaño, S. A., & Muñoz-López, L. (2023). Use of the Therapy App Prescinde for Increasing Adherence to Smoking Cessation Treatment. Healthcare, 11(24), 3121. https://doi.org/10.3390/healthcare11243121