
Dietary Intake of Capsaicin and Its Association with Markers of Body Adiposity and Fatty Liver in a Mexican Adult Population of Tijuana


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Anthropometric Measurements and Blood Pressure
2.3. Dietary Intake and Appetite
2.4. Blood Tests
2.5. Statistical Analyses
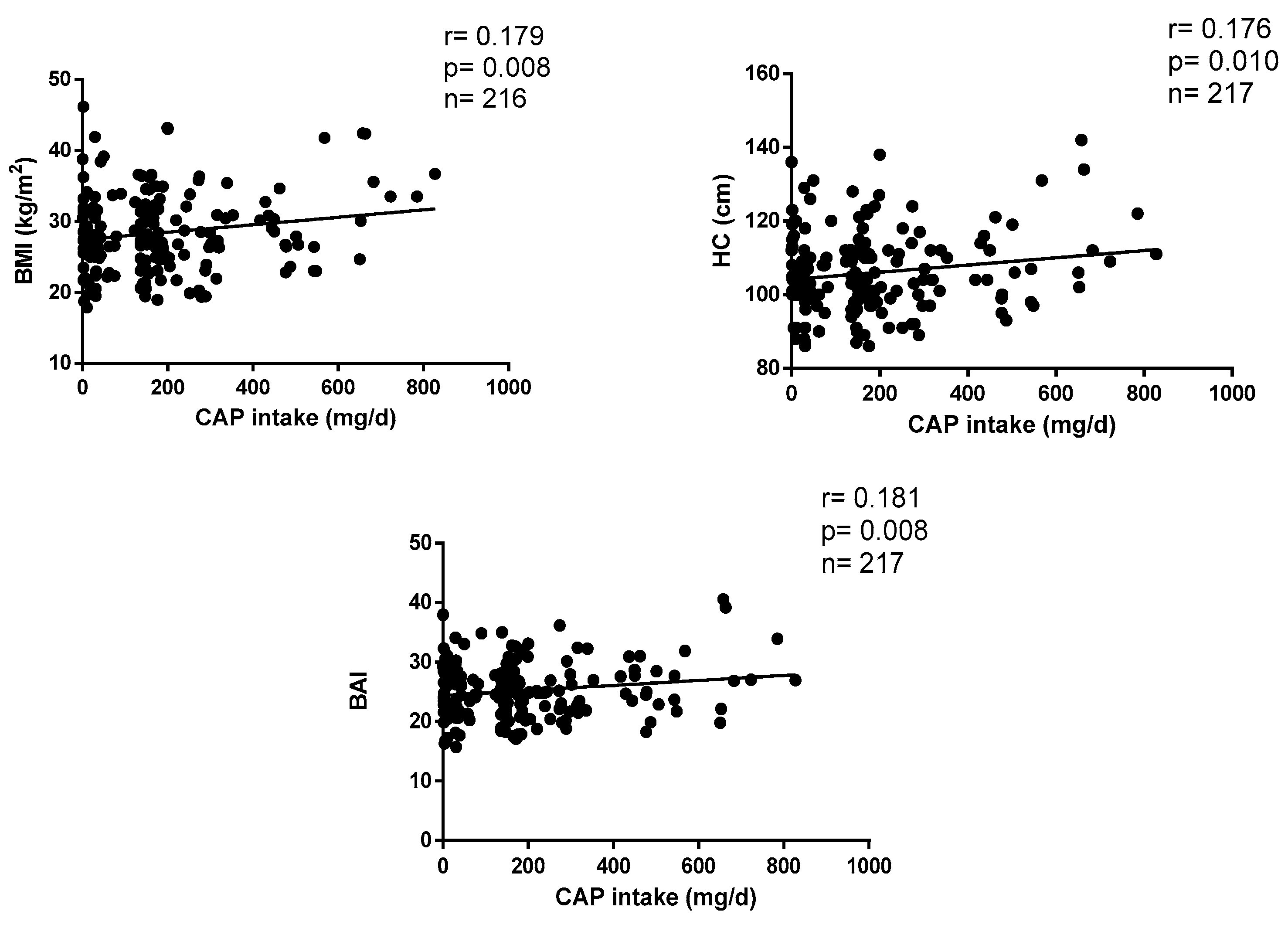
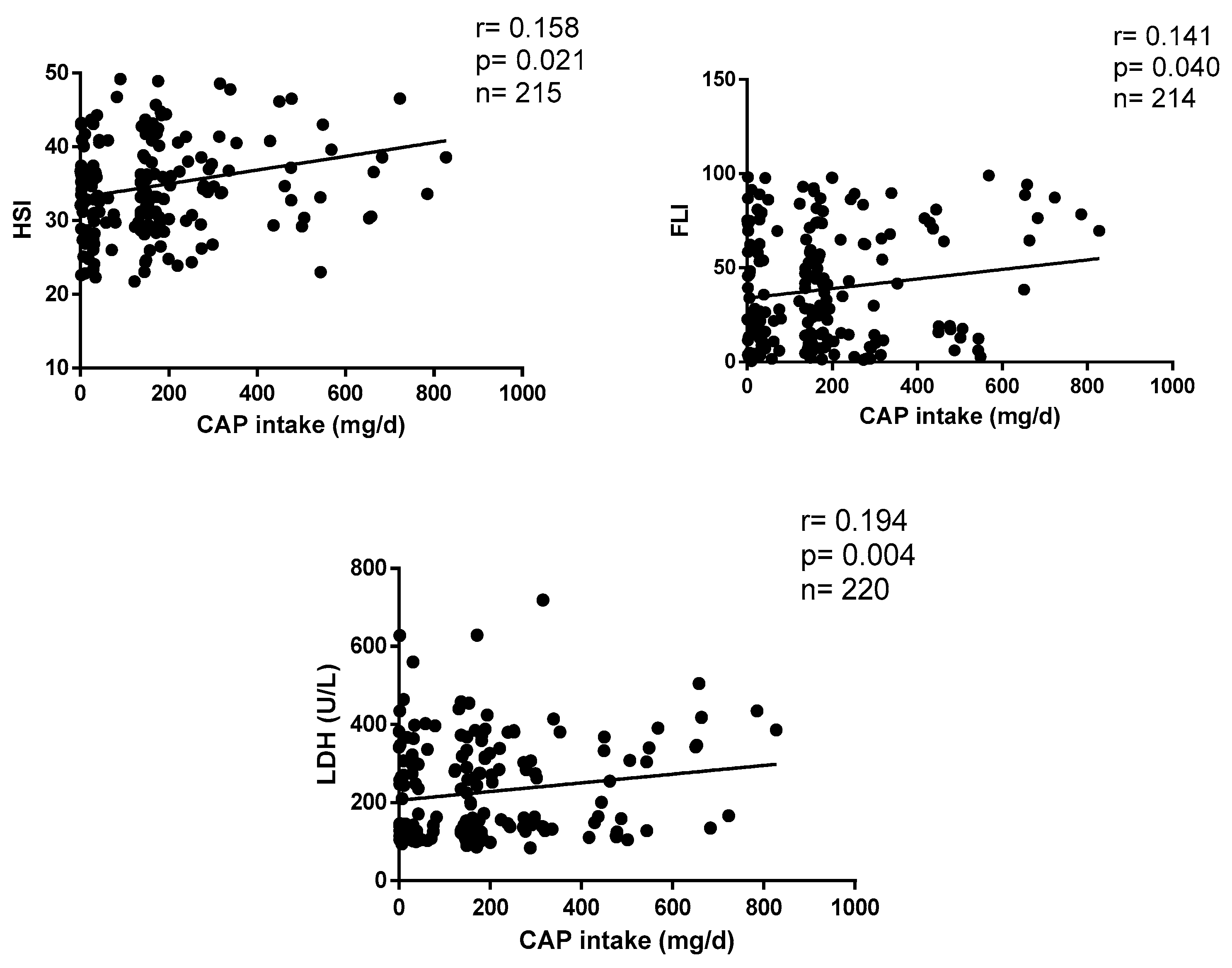
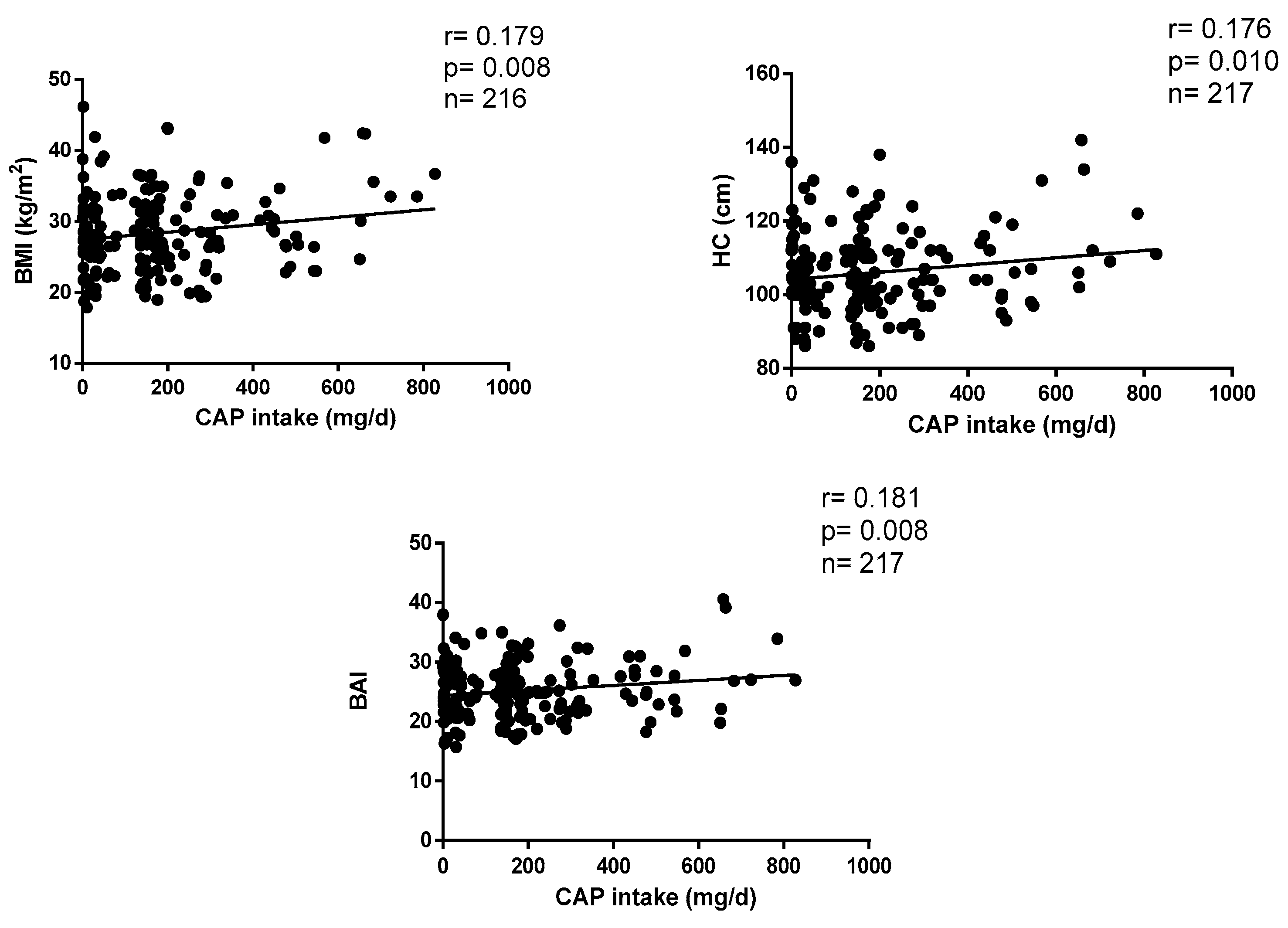
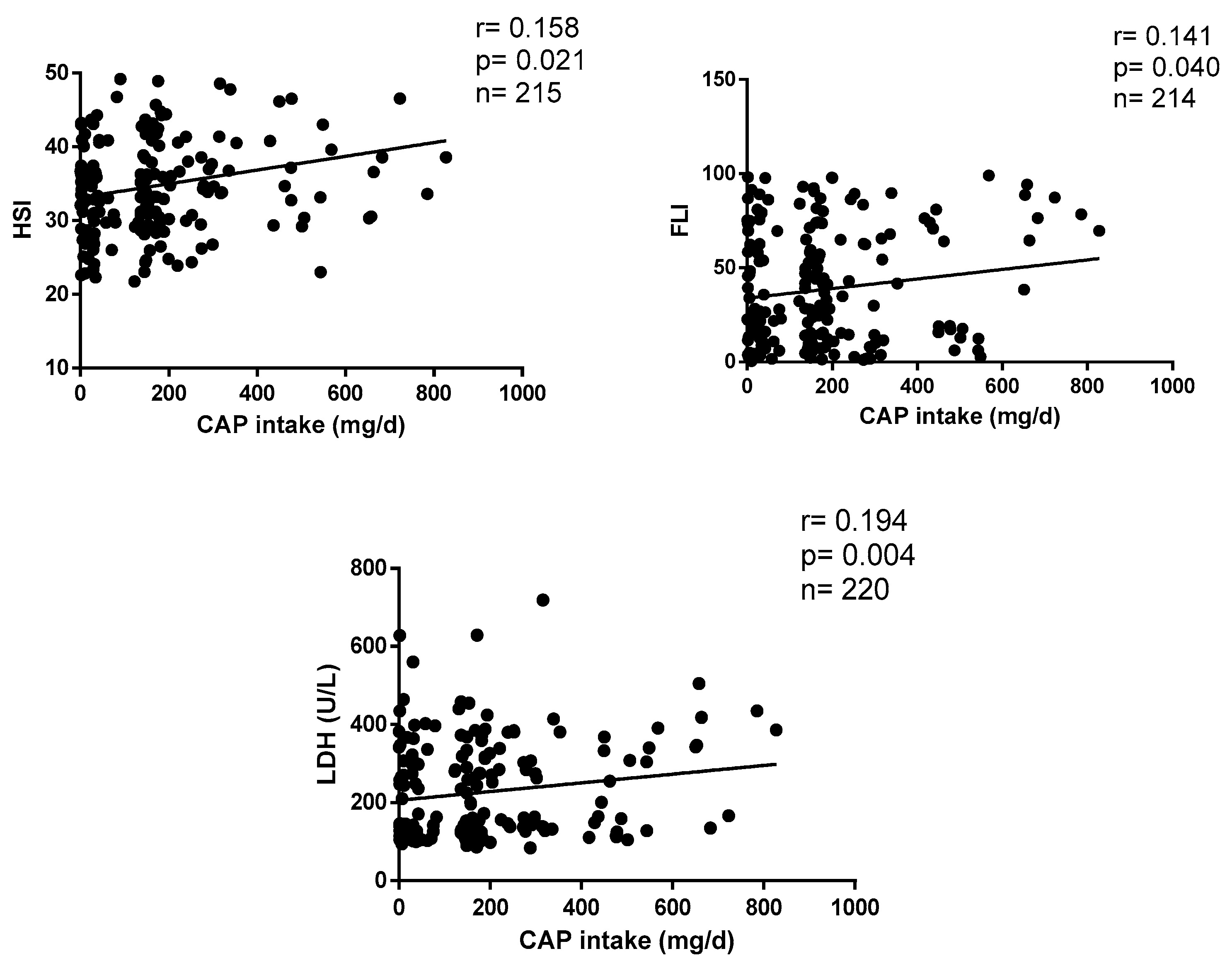
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aguilar-Meléndez, A.; Vásquez-Dávila, M.A.; Manzanero-Medina, G.I.; Katz, E. Chile (Capsicum Spp.) as Food-Medicine Continuum in Multiethnic Mexico. Foods 2021, 10, 2502. [Google Scholar] [CrossRef]
- Román, S.; Ojeda-Granados, C.; Panduro, A. Genética y evolución de la alimentación de la población en México. Rev. Endocrinol. Nutr. 2013, 21, 42–51. [Google Scholar]
- McCoy, J.; Martínez-Ainsworth, N.; Bernau, V.; Scheppler, H.; Hedblom, G.; Adhikari, A.; McCormick, A.; Kantar, M.; McHale, L.; Jardón-Barbolla, L.; et al. Population Structure in Diverse Pepper (Capsicum Spp.) Accessions. BMC Res. Notes 2023, 16, 20. [Google Scholar] [CrossRef] [PubMed]
- López-Carrillo, L.; López-Cervantes, M.; Robles-Díaz, G.; Ramírez-Espitia, A.; Mohar-Betancourt, A.; Meneses-García, A.; López-Vidal, Y.; Blair, A. Capsaicin Consumption, Helicobacter Pylori Positivity and Gastric Cancer in Mexico. Int. J. Cancer 2003, 106, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Vij, A.S.; Sharma, M. Mechanisms and Clinical Uses of Capsaicin. Eur. J. Pharmacol. 2013, 720, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.-S.; Alqahtani, A.; Ojo, O.A.; Shaheen, H.M.; Wasef, L.; Elzeiny, M.; Ismail, M.; Shalaby, M.; Murata, T.; Zaragoza-Bastida, A.; et al. Biological Properties, Bioactive Constituents, and Pharmacokinetics of Some Capsicum Spp. and Capsaicinoids. Int. J. Mol. Sci. 2020, 21, 5179. [Google Scholar] [CrossRef]
- García-Rosales, M.E.; Ortega Martínez, J.; García-Galindo, H.S.; Martínez Martínez, C.; Beristain Guevara, C.I. La Capsaicina, El Principio Pungente Del Chile; Su Naturaleza, Absorción, Metabolismo y Efectos Farmacológicos. Ciencia 1995, 46, 82–102. [Google Scholar]
- Ferdowsi, P.V.; Ahuja, K.D.K.; Beckett, J.M.; Myers, S. Capsaicin and Zinc Signalling Pathways as Promising Targets for Managing Insulin Resistance and Type 2 Diabetes. Molecules 2023, 28, 2861. [Google Scholar] [CrossRef]
- Panchal, S.K.; Bliss, E.; Brown, L. Capsaicin in Metabolic Syndrome. Nutrients 2018, 10, 630. [Google Scholar] [CrossRef]
- Weng, G.; Duan, Y.; Zhong, Y.; Song, B.; Zheng, J.; Zhang, S.; Yin, Y.; Deng, J. Plant Extracts in Obesity: A Role of Gut Microbiota. Front. Nutr. 2021, 8, 727951. [Google Scholar] [CrossRef]
- Fischer, M.J.M.; Ciotu, C.I.; Szallasi, A. The Mysteries of Capsaicin-Sensitive Afferents. Front. Physiol. 2020, 11, 554195. [Google Scholar] [CrossRef]
- Shi, Z.; Riley, M.; Taylor, A.W.; Page, A. Chilli Consumption and the Incidence of Overweight and Obesity in a Chinese Adult Population. Int. J. Obes. 2017, 41, 1074–1079. [Google Scholar] [CrossRef]
- Whiting, S.; Derbyshire, E.; Tiwari, B.K. Capsaicinoids and capsinoids. A potential role for weight management? A systematic review of the evidence. Appetite 2012, 59, 341–348. [Google Scholar] [CrossRef]
- Rigamonti, A.E.; Casnici, C.; Marelli, O.; De Col, A.; Tamini, S.; Lucchetti, E.; Tringali, G.; De Micheli, R.; Abbruzzese, L.; Bortolotti, M.; et al. Acute administration of capsaicin increases resting energy expenditure in young obese subjects without affecting energy intake, appetite, and circulating levels of orexigenic/anorexigenic peptides. Nutr. Res. 2018, 52, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Janssens, P.L.; Hursel, R.; Martens, E.A.; Westerterp-Plantenga, M.S. Acute effects of capsaicin on energy expenditure and fat oxidation in negative energy balance. PLoS ONE 2013, 8, e67786. [Google Scholar] [CrossRef] [PubMed]
- van Avesaat, M.; Troost, F.J.; Westerterp-Plantenga, M.S.; Helyes, Z.; Le Roux, C.W.; Dekker, J.; Masclee, A.A.; Keszthelyi, D. Capsaicin-induced satiety is associated with gastrointestinal distress but not with the release of satiety hormones. Am. J. Clin. Nutr. 2016, 103, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Whiting, S.; Derbyshire, E.J.; Tiwari, B. Could capsaicinoids help to support weight management? A systematic review and meta-analysis of energy intake data. Appetite 2014, 73, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhang, Q.; Wang, L.; Zhou, Q.; Wang, P.; Qing, Y.; Sun, C. The effects of capsaicin intake on weight loss among overweight and obese subjects: A systematic review and meta-analysis of randomised controlled trials. Br. J. Nutr. 2023, 130, 1645–1656. [Google Scholar] [CrossRef]
- Sun, D.; Lv, J.; Chen, W.; Li, S.; Guo, Y.; Bian, Z.; Yu, C.; Zhou, H.; Tan, Y.; Chen, J.; et al. Spicy Food Consumption Is Associated with Adiposity Measures among Half a Million Chinese People: The China Kadoorie Biobank Study. BMC Public. Health 2014, 14, 1293. [Google Scholar] [CrossRef]
- Xu, Q.; Yan, S.; Wang, C.; Yu, B.; Zhou, X.; Luan, Q.; Na, L. Spicy food intake increases the risk of overweight and obesity. Wei Sheng Yan Jiu 2019, 48, 374–379. [Google Scholar]
- Yang, K.; Li, Y.; Mao, Z.; Liu, X.; Zhang, H.; Liu, R.; Xue, Y.; Tu, R.; Liu, X.; Zhang, X.; et al. Relationship between Spicy Flavor, Spicy Food Intake Frequency, and General Obesity in a Rural Adult Chinese Population: The RuralDiab Study. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 252–261. [Google Scholar] [CrossRef]
- Yang, X.; Tang, W.; Mao, D.; Liu, X.; Qian, W.; Dai, Y.; Chen, L.; Ding, X. Spicy Food Consumption Is Associated with Abdominal Obesity among Chinese Han Population Aged 30–79 Years in the Sichuan Basin: A Population-Based Cross-Sectional Study. BMC Public. Health 2022, 22, 1881. [Google Scholar] [CrossRef]
- Yang, K.; Li, Y.; Xue, Y.; Wang, L.; Liu, X.; Tu, R.; Dong, X.; Mao, Z.; Li, W.; Wang, C. Association of the Frequency of Spicy Food Intake and the Risk of Abdominal Obesity in Rural Chinese Adults: A Cross-Sectional Study. BMJ Open 2019, 9, e028736. [Google Scholar] [CrossRef]
- Wang, M.; Huang, W.; Xu, Y. Effects of spicy food consumption on overweight/obesity, hypertension and blood lipids in China: A meta-analysis of cross-sectional studies. Nutr. J. 2023, 22, 29. [Google Scholar] [CrossRef]
- Dávila-Torres, J.; González-Izquierdo, J.J.; Barrera-Cruz, A. Panorama de la obesidad en México [Obesity in Mexico]. Rev. Med. Inst. Mex. Seguro Soc. 2015, 53, 240–249. [Google Scholar]
- Ramos-Lopez, O.; Martinez-Lopez, E.; Roman, S.; Fierro, N.A.; Panduro, A. Genetic, metabolic and environmental factors involved in the development of liver cirrhosis in Mexico. World J. Gastroenterol. 2015, 21, 11552–11566. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [CrossRef]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A Better Index of Body Adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Vega-Cárdenas, M.; Teran-Garcia, M.; Vargas-Morales, J.M.; Padrón-Salas, A.; Aradillas-García, C. Visceral adiposity index is a better predictor to discriminate metabolic syndrome than other classical adiposity indices among young adults. Am. J. Hum. Biol. 2023, 35, e23818. [Google Scholar] [CrossRef]
- Whitworth, J.A.; Chalmers, J. World Health Organisation-International Society of Hypertension (WHO/ISH) Hypertension Guidelines. Clin. Exp. Hypertens. 2004, 26, 747–752. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Panduro, A.; Martinez-Lopez, E.; Roman, S. Sweet Taste Receptor TAS1R2 Polymorphism (Val191Val) Is Associated with a Higher Carbohydrate Intake and Hypertriglyceridemia among the Population of West Mexico. Nutrients 2016, 8, 101. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Panduro, A.; Rivera-Iñiguez, I.; Roman, S. Dopamine D2 Receptor Polymorphism (C957T) Is Associated with Sugar Consumption and Triglyceride Levels in West Mexicans. Physiol. Behav. 2018, 194, 532–537. [Google Scholar] [CrossRef] [PubMed]
- López-Carrillo, L.; Camargo, M.C.; Schneider, B.G.; Sicinschi, L.A.; Hernández-Ramírez, R.U.; Correa, P.; Cebrian, M.E. Capsaicin Consumption, Helicobacter Pylori CagA Status and IL1B-31C > T Genotypes: A Host and Environment Interaction in Gastric Cancer. Food Chem. Toxicol. 2012, 50, 2118–2122. [Google Scholar] [CrossRef]
- Lau, S.; Pek, K.; Chew, J.; Lim, J.P.; Ismail, N.H.; Ding, Y.Y.; Cesari, M.; Lim, W.S. The Simplified Nutritional Appetite Questionnaire (SNAQ) as a Screening Tool for Risk of Malnutrition: Optimal Cutoff, Factor Structure, and Validation in Healthy Community-Dwelling Older Adults. Nutrients 2020, 12, 2885. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Han, A.L. Validation of Fatty Liver Index as a Marker for Metabolic Dysfunction-Associated Fatty Liver Disease. Diabetol. Metab. Syndr. 2022, 14, 44. [Google Scholar] [CrossRef]
- Wang, C.; Cai, Z.; Deng, X.; Li, H.; Zhao, Z.; Guo, C.; Zhang, P.; Li, L.; Gu, T.; Yang, L.; et al. Association of Hepatic Steatosis Index and Fatty Liver Index with Carotid Atherosclerosis in Type 2 Diabetes. Int. J. Med. Sci. 2021, 18, 3280–3289. [Google Scholar] [CrossRef]
- Araújo, S.P.; Juvanhol, L.L.; Bressan, J.; Hermsdorff, H.H.M. Triglyceride Glucose Index: A New Biomarker in Predicting Cardiovascular Risk. Prev. Med. Rep. 2022, 29, 101941. [Google Scholar] [CrossRef]
- Man, M.A.; Rajnoveanu, R.M.; Motoc, N.S.; Bondor, C.I.; Chis, A.F.; Lesan, A.; Puiu, R.; Lucaciu, S.R.; Dantes, E.; Gergely-Domokos, B.; et al. Neutrophil-to-lymphocyte ratio, platelets-to-lymphocyte ratio, and eosinophils correlation with high-resolution computer tomography severity score in COVID-19 patients. PLoS ONE 2021, 16, e0252599. [Google Scholar] [CrossRef]
- Gawiński, C.; Michalski, W.; Mróz, A.; Wyrwicz, L. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Tumor-Infiltrating Lymphocytes (TILs) in Left-Sided Colorectal Cancer Patients. Biology 2022, 11, 385. [Google Scholar] [CrossRef]
- Mosqueda-Solís, A.; Lafuente-Ibáñez de Mendoza, I.; Aguirre-Urizar, J.M.; Mosqueda-Taylor, A. Capsaicin Intake and Oral Carcinogenesis: A Systematic Review. Med. Oral. Patol. Oral. Cir. Bucal 2021, 26, e261–e268. [Google Scholar] [CrossRef]
- Siebert, E.; Lee, S.-Y.; Prescott, M.P. Chili Pepper Preference Development and Its Impact on Dietary Intake: A Narrative Review. Front. Nutr. 2022, 9, 1039207. [Google Scholar] [CrossRef]
- Kwon, Y. Estimation of Dietary Capsaicinoid Exposure in Korea and Assessment of Its Health Effects. Nutrients 2021, 13, 2461. [Google Scholar] [CrossRef]
- Ludy, M.J.; Moore, G.E.; Mattes, R.D. The effects of capsaicin and capsiate on energy balance: Critical review and meta-analyses of studies in humans. Chem. Senses 2012, 37, 103–121. [Google Scholar] [CrossRef]
- Baskaran, P.; Krishnan, V.; Ren, J.; Thyagarajan, B. Capsaicin induces browning of white adipose tissue and counters obesity by activating TRPV1 channel-dependent mechanisms. Br. J. Pharmacol. 2016, 173, 2369–2389. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Tang, C.; Tang, Y.; Yin, H.; Liu, X. Capsaicin has an anti-obesity effect through alterations in gut microbiota populations and short-chain fatty acid concentrations. Food Nutr. Res. 2020, 64, 3615. [Google Scholar] [CrossRef]
- Shen, W.; Shen, M.; Zhao, X.; Zhu, H.; Yang, Y.; Lu, S.; Tan, Y.; Li, G.; Li, M.; Wang, J.; et al. Anti-obesity Effect of Capsaicin in Mice Fed with High-Fat Diet Is Associated with an Increase in Population of the Gut Bacterium Akkermansia muciniphila. Front. Microbiol. 2017, 8, 272. [Google Scholar] [CrossRef]
- Lee, G.R.; Shin, M.K.; Yoon, D.J.; Kim, A.R.; Yu, R.; Park, N.H.; Han, I.S. Topical application of capsaicin reduces visceral adipose fat by affecting adipokine levels in high-fat diet-induced obese mice. Obesity 2013, 21, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.L.; Yan Liu, D.; Ma, L.Q.; Luo, Z.D.; Cao, T.B.; Zhong, J.; Yan, Z.C.; Wang, L.J.; Zhao, Z.G.; Zhu, S.J.; et al. Activation of transient receptor potential vanilloid type-1 channel prevents adipogenesis and obesity. Circ. Res. 2007, 100, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zheng, S.; Feng, Q.; Zhang, Q.; Xiao, X. Dietary capsaicin and its anti-obesity potency: From mechanism to clinical implications. Biosci. Rep. 2017, 37, BSR20170286. [Google Scholar] [CrossRef]
- Li, Q.; Li, L.; Wang, F.; Chen, J.; Zhao, Y.; Wang, P.; Nilius, B.; Liu, D.; Zhu, Z. Dietary capsaicin prevents nonalcoholic fatty liver disease through transient receptor potential vanilloid 1-mediated peroxisome proliferator-activated receptor δ activation. Pflug. Arch. 2013, 465, 1303–1316. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.K.; Yang, S.M.; Han, I.S. Capsaicin suppresses liver fat accumulation in high-fat diet-induced NAFLD mice. Anim. Cells Syst. 2020, 24, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Sales, E.; Mohaddes, G.; Alipour, M.R. Hepatoprotection of capsaicin in alcoholic and non-alcoholic fatty liver diseases. Arch. Physiol. Biochem. 2021, 16, 1–11. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Xu, M.; Chen, Y.; Peng, K.; Huang, Y.; Wang, P.; Ding, L.; Lin, L.; Xu, Y.; Chen, Y.; et al. Validation of the Fatty Liver Index for Nonalcoholic Fatty Liver Disease in Middle-Aged and Elderly Chinese. Medicine 2015, 94, e1682. [Google Scholar] [CrossRef]
- Rietman, A.; Sluik, D.; Feskens, E.J.M.; Kok, F.J.; Mensink, M. Associations between dietary factors and markers of NAFLD in a general Dutch adult population. Eur. J. Clin. Nutr. 2018, 72, 117–123. [Google Scholar] [CrossRef]
- Martínez-Urbistondo, D.; San Cristóbal, R.; Villares, P.; Martínez-González, M.Á.; Babio, N.; Corella, D.; Del Val, J.L.; Ordovás, J.M.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Role of NAFLD on the Health Related QoL Response to Lifestyle in Patients With Metabolic Syndrome: The PREDIMED Plus Cohort. Front. Endocrinol. 2022, 13, 868795. [Google Scholar] [CrossRef]
- Pérez Rodrigo, C.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Food frequency questionnaires. Nutr. Hosp. 2015, 31 (Suppl. S3), 49–56. [Google Scholar] [CrossRef]
- Okamoto, N.; Okumura, M.; Tadokoro, O.; Sogawa, N.; Tomida, M.; Kondo, E. Effect of Single-Nucleotide Polymorphisms in TRPV1 on Burning Pain and Capsaicin Sensitivity in Japanese Adults. Mol. Pain. 2018, 14, 1744806918804439. [Google Scholar] [CrossRef]
- Liviero, F.; Campisi, M.; Scarpa, M.C.; Mason, P.; Guarnieri, G.; Maestrelli, P.; Pavanello, S. Multiple Single Nucleotide Polymorphisms of the Transient Receptor Potential Vanilloid 1 (TRPV1) Genes Associate with Cough Sensitivity to Capsaicin in Healthy Subjects. Pulm. Pharmacol. Ther. 2020, 61, 101889. [Google Scholar] [CrossRef] [PubMed]
- Nolden, A.A.; McGeary, J.E.; Hayes, J.E. Differential bitterness in capsaicin, piperine, and ethanol associates with polymorphisms in multiple bitter taste receptor genes. Physiol. Behav. 2016, 156, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Báez, S.; Tsuchiya, Y.; Calvo, A.; Pruyas, M.; Nakamura, K.; Kiyohara, C.; Oyama, M.; Yamamoto, M. Genetic variants involved in gallstone formation and capsaicin metabolism, and the risk of gallbladder cancer in Chilean women. World J. Gastroenterol. 2010, 16, 372–378. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Occasional CAP Consumers (n = 37) | Daily CAP Consumers, 0–100 mg (n = 66) | Daily CAP Consumers, 100–400 mg (n = 93) | Daily CAP Consumers, 400–900 mg (n = 25) | p-Value |
|---|---|---|---|---|---|
| Age (years) | 39.0 ± 13.72 | 38.8 ± 12.18 | 36.8 ± 12.18 | 35.2 ± 12.26 | 0.499 |
| Sex (F/M) | 19/15 | 115/69 | 115/69 | 115/69 | 0.891 |
| BMI (kg/m2) | 27.4 ± 5.18 | 27.9 ± 5.70 | 28.1 ± 5.13 | 30.5 ± 5.92 | 0.147 |
| Body fat (%) | 33.8 ± 8.55 | 33.9 ± 10.3 | 34.5 ± 8.25 | 39.3 ± 8.74 | 0.260 |
| WC (cm) | 89.2 ± 16.2 | 89.5 ± 13.6 | 89.3 ± 14.1 | 95.3 ± 15.5 | 0.299 |
| HC (cm) | 103 ± 9.87 | 105 ± 10.6 | 104 ± 9.87 | 110 ± 12.3 | 0.074 |
| WHR | 0.85 ± 0.10 | 0.84 ± 0.08 | 0.85 ± 0.09 | 0.86 ± 0.10 | 0.875 |
| SBP (mmHg) | 121 ± 17.4 | 118 ± 21.5 | 121 ± 16.0 | 120 ± 15.5 | 0.817 |
| DBP (mmHg) | 80.1 ± 10.1 | 78.1 ± 10.3 | 78.6 ± 9.95 | 78.0 ± 9.93 | 0.779 |
| BAI | 22.9 ± 7.59 | 24.9 ± 4.62 | 24.8 ± 4.20 | 26.9 ± 5.51 | 0.033 * |
| VAI | 3.99 ± 2.90 | 4.17 ± 2.87 | 4.73 ± 5.47 | 4.09 ± 2.77 | 0.741 |
| Variable | Occasional CAP Consumers (n = 37) | Daily CAP Consumers, 0–100 mg (n = 66) | Daily CAP Consumers, 100–400 mg (n = 93) | Daily CAP Consumers, 400–900 mg (n = 25) | p-Value |
|---|---|---|---|---|---|
| Appetite | 10.1 ± 4.20 | 11.5 ± 2.22 | 11.5 ± 2.35 | 12.0 ± 2.29 | 0.029 * |
| Total calories | 1898 ± 831 | 2205 ± 772 | 1975 ± 693 | 1995 ± 755 | 0.196 |
| Proteins (%) | 19.6 ± 9.89 | 18.3 ± 4.16 | 18.6 ± 4.06 | 20.8 ± 5.17 | 0.250 |
| Fat (%) | 38.4 ± 8.51 | 38.8 ± 8.36 | 37.0 ± 8.10 | 36.9 ± 6.9 | 0.533 |
| Carbohydrates (%) | 41.7 ± 12.4 | 41.8 ± 9.12 | 43.4 ± 9.30 | 41.8 ± 8.01 | 0.720 |
| Variable | Occasional CAP Consumers (n = 37) | Daily CAP Consumers, 0–100 mg (n = 66) | Daily CAP Consumers, 100–400 mg (n = 93) | Daily CAP Consumers, 400–900 mg (n = 25) | p-Value |
|---|---|---|---|---|---|
| Blood glucose (mg/dL) | 95.6 ± 21.4 | 94.9 ± 12.5 | 95.0 ± 11.6 | 94.4 ± 11.4 | 0.989 |
| Total cholesterol (mg/dL) | 191 ± 39 | 191 ± 36 | 190 ± 37 | 195 ± 46 | 0.947 |
| HDL-c (mg/dL) | 43.6 ± 11.1 | 47.2 ± 13.1 | 45.0 ± 14.0 | 46.6 ± 12.9 | 0.548 |
| LDL-c (mg/dL) | 128 ± 36 | 123 ± 29 | 123 ± 36 | 127 ± 38 | 0.832 |
| Triglycerides (mg/dL) | 102 ± 55 | 105 ± 60 | 108 ± 64 | 109 ± 61 | 0.954 |
| Urea (mg/dL) | 23.5 ± 14.4 | 24.7 ± 11.9 | 24.2 ± 13.1 | 24.7 ± 12.7 | 0.971 |
| Total proteins (g/dL) | 7.38 ± 0.49 | 7.37 ± 0.44 | 7.52 ± 0.46 | 7.49 ± 0.46 | 0.155 |
| Albumin (g/dL) | 4.04 ± 0.19 | 4.00 ± 0.17 | 4.03 ± 0.19 | 4.01 ± 0.20 | 0.725 |
| Globulins | 3.33 ± 0.048 | 3.37 ± 0.46 | 3.49 ± 0.47 | 3.45 ± 0.45 | 0.232 |
| Creatinine (mg/dL) | 0.64 ± 0.18 | 0.70 ± 0.18 | 0.68 ± 0.20 | 0.65 ± 0.20 | 0.188 |
| LDH (U/L) | 179 ± 91 | 217 ± 125 | 225 ± 125 | 256 ± 124 | 0.087 |
| AST (U/L) | 44.0 ± 41.0 | 37.3 ± 15.5 | 36.2 ± 8.83 | 37.3 ± 10.1 | 0.241 |
| ALT (U/L) | 36.7 ± 59.7 | 28.0 ± 21.1 | 27.3 ± 17.2 | 31.4 ± 22.3 | 0.416 |
| GGT (U/L) | 19.3 ± 15.5 | 19.0 ± 15.3 | 1817 ± 11.1 | 20.1 ± 18.3 | 0.921 |
| TB (µmol/L) | 1.01 ± 0.33 | 1.22 ± 0.56 | 1.15 ± 0.62 | 1.20 ± 0.44 | 0.320 |
| DB (µmol/L) | 0.14 ± 0.06 | 0.17 ± 0.09 | 0.16 ± 0.07 | 0.18 ± 0.05 | 0.289 |
| ALP (U/L) | 150 ± 67 | 154 ± 57 | 163 ± 63 | 154 ± 64 | 0.692 |
| Uric acid (mg/dL) | 5.41 ± 1.89 | 5.27 ± 1.85 | 5.61 ± 1.99 | 5.45 ± 1.74 | 0.745 |
| Total calcium (mg/dL) | 9.28 ± 1.42 | 9.51 ± 0.50 | 9.65 ± 0.40 | 9.58 ± 0.42 | 0.064 |
| Total phosphorus (mg/dL) | 2.88 ± 0.41 | 2.98 ± 0.53 | 3.02 ± 0.57 | 2.76 ± 0.38 | 0.117 |
| Total iron (µmol/L) | 90.6 ± 33.6 | 84.6 ± 31.3 | 84.8 ± 36.4 | 94.3 ± 32.7 | 0.518 |
| Creatine kinase (U/L) | 245 ± 240 | 377 ± 696 | 236 ± 263 | 202 ± 198 | 0.156 |
| Sodium (mmol/L) | 141 ± 1.28 | 141 ± 1.22 | 141 ± 1.17 | 141 ± 1.03 | 0.931 |
| Potassium (mmol/L) | 4.04 ± 0.30 | 4.04 ± 0.24 | 4.04 ± 0.28 | 3.99 ± 0.24 | 0.708 |
| Chlorine (mmol/L) | 103 ± 1.05 | 103 ± 1.17 | 103 ± 3.99 | 103 ± 1.11 | 0.725 |
| FLI | 35.4 ± 31.2 | 36.3 ± 30.3 | 37.5 ± 29.4 | 48.1 ± 33.7 | 0.344 |
| HSI | 34.2 ± 7.39 | 33.9 ± 8.26 | 34.7 ± 6.89 | 37.6 ± 7.55 | 0.214 |
| TyG | 4.52 ± 0.28 | 4.52 ± 0.29 | 4.54 ± 0.28 | 4.55 ± 0.26 | 0.941 |
| Variable | CAP Non-Consumers (n = 37) | CAP Consumption 0–100 (n = 66) | CAP Consumption 100–400 (n = 93) | CAP Consumption 400–900 (n = 25) | p-Value |
|---|---|---|---|---|---|
| NLR | 1.96 ± 0.85 | 1.84 ± 0.95 | 1.97 ± 1.02 | 2.44 ± 1.72 | 0.140 |
| PLR | 135 ± 44.8 | 132 ± 63.8 | 147 ± 64.8 | 137 ± 42.4 | 0.459 |
| EBR | 3.29 ± 5.19 | 4.80 ± 8.79 | 4.75 ± 8.04 | 7.90 ± 17.1 | 0.305 |
| ELR | 0.07 ± 0.07 | 0.08 ± 0.05 | 0.10 ± 0.09 | 0.08 ± 0.06 | 0.335 |
| LMR | 5.86 ± 2.05 | 5.97 ± 2.24 | 6.04 ± 2.29 | 6.32 ± 3.45 | 0.898 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Aceviz, Y.; Sobrevilla-Navarro, A.A.; Ramos-Lopez, O. Dietary Intake of Capsaicin and Its Association with Markers of Body Adiposity and Fatty Liver in a Mexican Adult Population of Tijuana. Healthcare 2023, 11, 3001. https://doi.org/10.3390/healthcare11223001
Martínez-Aceviz Y, Sobrevilla-Navarro AA, Ramos-Lopez O. Dietary Intake of Capsaicin and Its Association with Markers of Body Adiposity and Fatty Liver in a Mexican Adult Population of Tijuana. Healthcare. 2023; 11(22):3001. https://doi.org/10.3390/healthcare11223001
Chicago/Turabian StyleMartínez-Aceviz, Yesenia, Ana Alondra Sobrevilla-Navarro, and Omar Ramos-Lopez. 2023. "Dietary Intake of Capsaicin and Its Association with Markers of Body Adiposity and Fatty Liver in a Mexican Adult Population of Tijuana" Healthcare 11, no. 22: 3001. https://doi.org/10.3390/healthcare11223001
APA StyleMartínez-Aceviz, Y., Sobrevilla-Navarro, A. A., & Ramos-Lopez, O. (2023). Dietary Intake of Capsaicin and Its Association with Markers of Body Adiposity and Fatty Liver in a Mexican Adult Population of Tijuana. Healthcare, 11(22), 3001. https://doi.org/10.3390/healthcare11223001