
Use of the Nursing Interventions Classification and Nurses’ Workloads: A Scoping Review

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
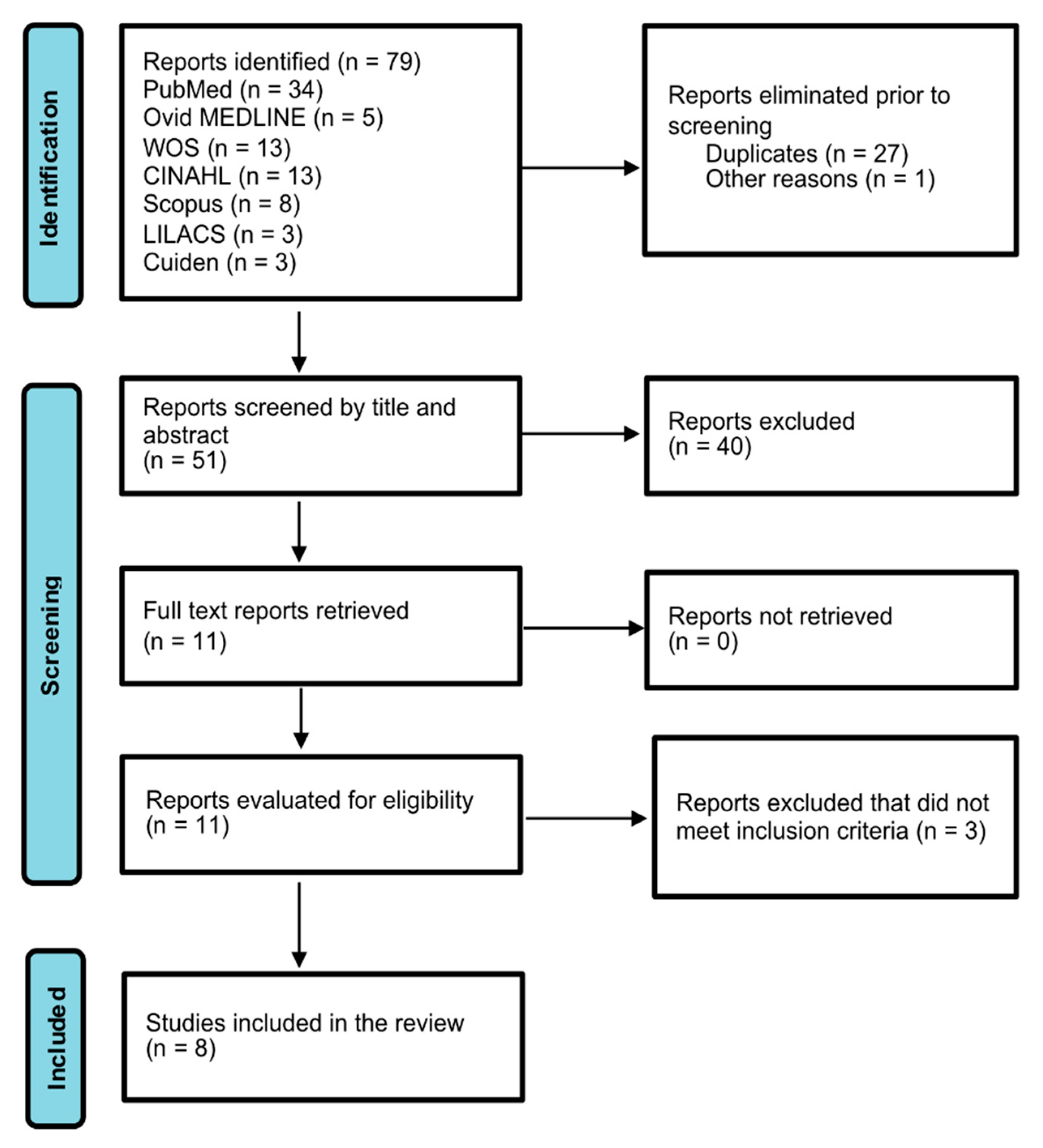
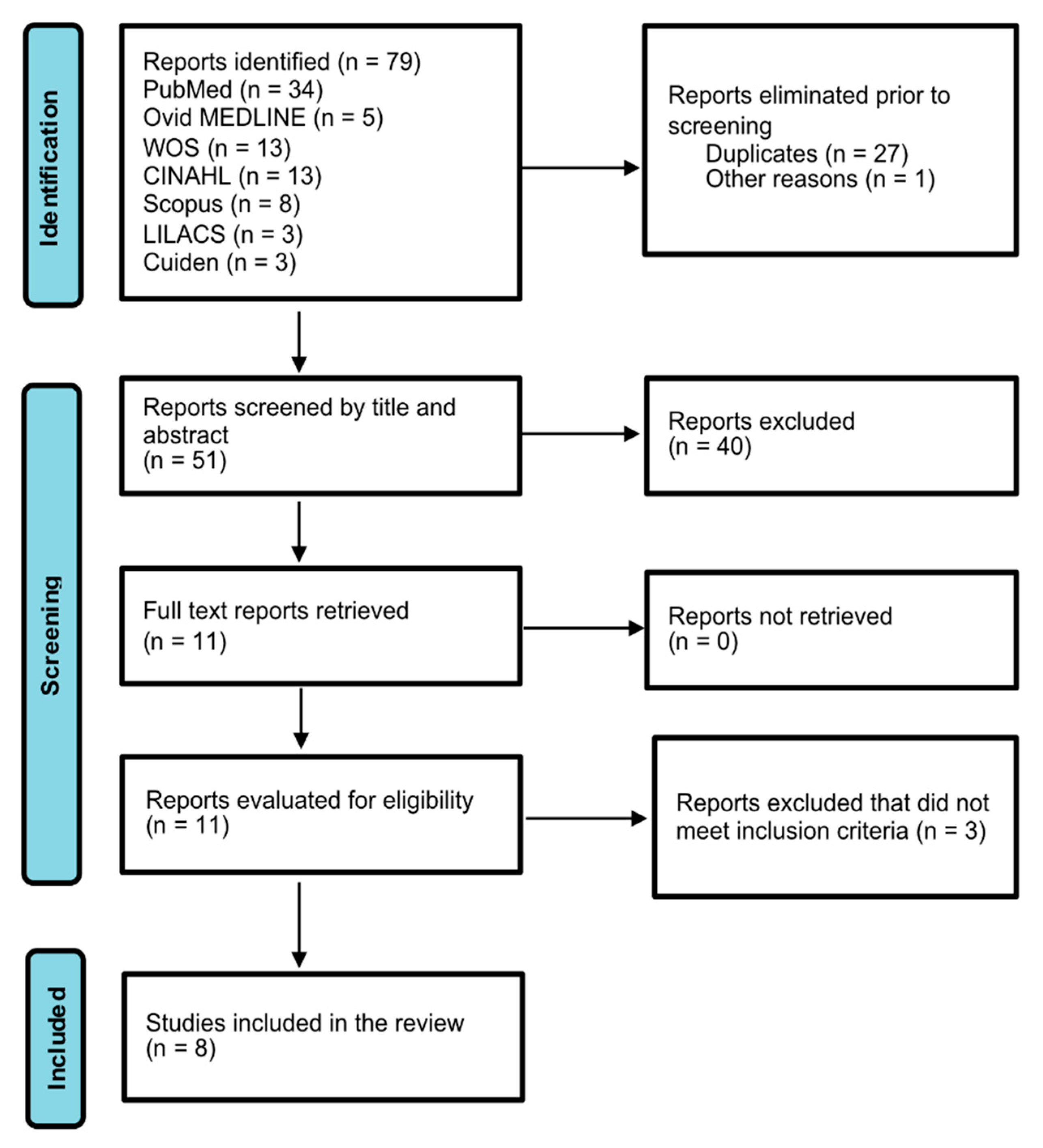
2. Materials and Methods
3. Results
3.1. Identification of Specific Interventions
3.2. Distribution of Interventions by Types of Activities
3.3. Prevalence of Interventions
3.4. Estimated Time to Carry out Interventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Butcher, H.K.; Bulechek, G.M.; Dochterman, J.M.; Wagner, C.M. Clasificación de Intervenciones de Enfermería (NIC), 7th ed.; Elsevier España, S.L.U.: Barcelona, España, 2019; ISBN 978-84-9113-404-6. [Google Scholar]
- da Cruz, C.W.M.; Bonfim, D.; Gaidzinski, R.R.; Fugulin, F.M.T.; Laus, A.M. The Use of Nursing Interventions Classification (NIC) in Identifying the Workload of Nursing: An Integrative Review. Int. J. Nurs. Knowl. 2014, 25, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Cordova, P.B.; Lucero, R.J.; Hyun, S.; Quinlan, P.; Price, K.; Stone, P.W. Using the Nursing Interventions Classification as a Potential Measure of Nurse Workload. J. Nurs. Care Qual. 2010, 25, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Somensi, R.M.; Caregnato, R.C.A.; Cervi, G.H.; Flores, C.D. Workload: A comparison between the online and observational methods. Rev. Bras. Enferm. 2018, 71, 1850–1857. [Google Scholar] [CrossRef] [PubMed]
- Trovó, S.A.; Cucolo, D.F.; Perroca, M.G. Transfer of patients in hospital units: Impacts on nursing workload. Rev. Esc. Enferm. USP 2021, 55, e0327. [Google Scholar] [CrossRef]
- Martin, L.G.R.; Gaidzinski, R.R. Creating and validating an instrument to identify the workload at an oncology and hematology outpatient service. Einstein 2014, 12, 323–329. [Google Scholar] [CrossRef] [PubMed]
- de Assis, M.N.; de Andrade, A.C.R.; Rogenski, K.E.; Castilho, V.; Fugulin, F.M.T. Intervenções de enfermagem em pediatria: Contribuição para a mensuração da carga de trabalho. Rev. Esc. Enferm. USP 2015, 49, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, Y.; Shen, N. The Use of the Nursing Interventions Classification in Identifying the Workload of a Nursing Team in a Pediatric Oncology Center. In Studies in Health Technology and Informatics; IOS Press: Clifton, VA, USA, 2021; Volume 284, pp. 83–84. [Google Scholar] [CrossRef]
- de Souza, C.A.; de Jericó, M.C.; Perroca, M.G. Nursing intervention/activity mapping at a Chemotherapy Center: An instrument for workload assessment. Rev. Lat.-Am. Enferm. 2013, 21, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Possari, J.F.; Gaidzinski, R.R.; Lima, A.F.C.; Fugulin, F.M.T.; Herdman, T.H. Use of the nursing intervention classification for identifying the workload of a nursing team in a surgical center. Rev. Lat. Am. Enferm. 2015, 232260m, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Chambergo-Michilot, D.; Diaz-Barrera, M.E.; Benites-Zapata, V.A. Revisiones de alcance, revisiones paraguas y síntesis enfocada en revisión de mapas: Aspectos metodológicos y aplicaciones. Rev. Peru. Med. Exp. Salud Publica 2021, 38, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Watson, M. Guidance on Conducting a Systematic Literature Review. J. Plan. Educ. Res. 2019, 39, 93–112. [Google Scholar] [CrossRef]
- Bertolazzi, L.G.; Perroca, M.G. Impact of interruptions on the duration of nursing interventions: A study in a chemotherapy unit. Rev. Esc. Enferm. USP 2020, 54, e03551. [Google Scholar] [CrossRef] [PubMed]
- Souza, P.; Cucolo, D.F.; Perroca, M.G. Nursing workload: Influence of indirect care interventions. Rev. Esc. Enferm. 2019, 53, e03440. [Google Scholar] [CrossRef]
- De Groot, K.; De Veer, A.J.E.; Munster, A.M.; Francke, A.L.; Paans, W. Nursing documentation and its relationship with perceived nursing workload: A mixed-methods study among community nurses. BMC Nurs. 2022, 21, 34. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author (Year) | Journal | Setting (Country) | Methodology | Aim |
|---|---|---|---|---|
| Cordova et al. (2010) [3] | Journal of Nursing Care Quality | Orthopedic surgery (U.S.) | Qualitative | Determine the utility of NIC 1 terminology in classifying nursing care interventions as a measure of nursing workloads |
| Souza, Jericó & Perroca (2013) [9] | Revista Latino Americana de Enfermagem | Oncology (Brazil) | Descriptive | Identify the interventions and activities carried out in a chemotherapy centre, using standardised language, and validate its contents |
| Martin & Gaidzinski (2014) [6] | Einstein | Pediatric oncology (Brazil) | Descriptive | Create and validate an instrument to measure the time dedicated by nurses to interventions and activities in a Pediatric Hematology and Oncology Service Outpatient Centre |
| Assis et al. (2015) [7] | Revista da Escola de Enfermagem da USP | Pediatrics (Brazil) | Descriptive | Identify and validate the interventions and activities carried out by a nursing team in a pediatric unit in Brazil |
| Possari et al. (2015) [10] | Revista Latino Americana de Enfermagem | Oncology surgery (Brazil) | Descriptive | Analyse the distribution of nursing professionals’ workloads related to interventions and activities during the trans-operative period in a surgical centre specializing in oncology based on the NIC |
| Somensi et al. (2018) [4] | Revista Brasileira de Enfermagem | Hospital ward (Brazil) | Observational descriptive | Measure the workloads of nurses working on Hospital Wards, as recommended by the NIC, comparing observational and online methods to propose supervision strategies for professionals and academics |
| Sun, Li & Shen (2021) [8] | Studies in health technology and informatics | Pediatric oncology (China) | Descriptive | Identify and analyse the workloads of nursing professionals, according to the NIC, in a pediatric oncology centre |
| Trovó, Cucolo & Perroca (2021) [5] | Revista da Escola de Enfermagem da USP | Hospital ward (Brazil) | Observational descriptive | Measure the average time taken by nurses to transfer patients; compare the activities observed during this intervention with those described in the NIC and explore the intensity of their influence on workloads |
| Author (Year) | Activities Identified | Activities Validated | NIC 1 Identified | NIC Validated |
|---|---|---|---|---|
| Cordova et al. (2010) [3] | - | - | 224 | 42 |
| Souza, Jericó & Perroca (2013) [9] | 48 | 48 | 35 | 35 |
| Martin & Gaidzinski (2014) [6] | - | - | 32 | 25 |
| Assis et al. (2015) [7] | 275 | 205 | 63 | 53 |
| Possari et al. (2015) [10] | 266 | 266 | 49 | 49 |
| Somensi et al. (2018) [4] | - | - | 30 | - |
| Sun, Li & Shen (2021) [8] | 13,021 | - | 89 | - |
| Trovó, Cucolo & Perroca (2021) [5] | - | - | - | - |
| Author (Year) | Scheduled | Unscheduled | Direct (Included in NIC 1) | Indirect (Included in NIC) | Associated | Personal |
|---|---|---|---|---|---|---|
| Cordova et al. (2010) [3] | 25 NIC (59.53%) | 17 NIC (40.47%) | - | - | - | - |
| Assis et al. (2015) [7] | - | - | 238 (86.54%) | 24 (8.73%) | 13 (4.73%) | |
| Possari et al. (2015) [10] | - | - | 380 (42.79%) | 373 (42%) | 71 (8%) | 64 (7.21%) |
| Somensi et al. (2018) [4] | - | - | 16 NIC (face-to-face: 402 activities; telematic: 334 activities) | 14 NIC (face-to-face: 1499 activities; telematic: 1175 activities) | - | - |
| Sun, Li & Shen (2021) [8] | - | - | 63 NIC (35.84% activities) | 26 NIC (43.66% activities) | - | - |
| Interventions | Type of Activity | Possari et al. (2015) [10] n (%) | Somensi et al. (2018) [4] (In-Person Observation) n (%) | Somensi et al. (2018) [4] (Telematic Observation) n (%) |
|---|---|---|---|---|
| 0580 Bladder catheter | Direct | 18 (2.03) | 4 (1.0) | 3 (0.90) |
| 0582 Intermittent bladder catheterization | Direct | - | 1 (0.25) | 11 (3.29) |
| 0842 Change of position: intraoperative | Direct | 14 (1.58) | - | - |
| 1080 Nasogastric tube | Direct | - | 5 (1.24) | 3 (0.90) |
| 1630 Emotional support | Direct | 2 (0.10) | - | - |
| 1806 Help with self-care: transfer | Direct | 17 (1.91) | - | - |
| 1872 Thoracic drain care | Direct | - | 28 (6.97) | 16 (4.79) |
| 2000 Electrolyte management | Direct | 9 (1.01) | - | - |
| 2300 Administration of medication | Direct | - | 10 (2.49) | 15 (4.49) |
| 2870 Post-anesthesia care | Direct | 6 (0.69) | - | - |
| 2900 Surgical assistance | Direct | 49 (5.52) | - | - |
| 2920 Surgical precautions | Direct | 41 (4.62) | - | - |
| 3160 Airway suction | Direct | - | 2 (0.50) | 2 (0.60) |
| 3660 Wound care | Direct | 1 (0.11) | - | - |
| 3902 Temperature regulation: intraoperative | Direct | 12 (1.35) | - | - |
| 4030 Administration of blood products | Direct | 2 (0.22) | - | - |
| 4054 Central venous access device management | Direct | - | 19 (4.73) | 13 (3.89) |
| 4130 Liquid monitoring | Direct | 1 (0.11) | 2 (0.50) | - |
| 4232 Phlebotomy: arterial blood extraction | Direct | - | 15 (3.73) | 8 (2.40) |
| 4238 Phlebotomy: venous blood extraction | Direct | - | 6 (1.49) | 4 (1.20) |
| 4820 Orientation in the health system | Direct | - | 230 (57.21) | 150 (44.91) |
| 5340 Presence | Direct | 31 (3.49) | - | - |
| 5460 Contact | Indirect | - | 29 (1.93) | 40 (3.40) |
| 6200 Emergency care | Direct | - | 27 (6.72) | 26 (7.78) |
| 6320 Reanimation | Direct | - | - | 2 (0.60) |
| 6482 Environmental management: comfort | Direct | 4 (0.45) | - | - |
| 6486 Environmental management: safety | Direct | 2 (0.22) | - | - |
| 6545 Infection control: intraoperative | Direct | 19 (2.14) | - | - |
| 6650 Vigilance | Direct | 76 (8.56) | - | - |
| 6680 Monitoring vital signs | Direct | 1 (0.11) | - | - |
| 7140 Family support | Direct | 28 (3.15) | - | - |
| 7640 Development of clinical pathways | Indirect | 1 (0.11) | - | - |
| 7650 Delegation | Indirect | 76 (8.56) | - | - |
| 7680 Help in exploration | Direct | - | 29 (7.21) | 53 (15.87) |
| 7710 Cooperation with the doctor | Indirect | 11 (1.24) | - | - |
| 7760 Product assessment | Indirect | 2 (0.22) | - | - |
| 7820 Sample management | Indirect | 3 (0.35) | - | - |
| 7830 Supervision of personnel | Indirect | - | 78 (5.20) | 119 (10.13) |
| 7840 Supply change management | Indirect | 32 (3.60) | - | - |
| 7850 Personnel development | Indirect | 18 (2.03) | 27 (1.80) | 27 (2.30) |
| 7880 Management of technology | Indirect | 1 (0.11) | - | - |
| 7892 Transport: within the facility | Direct | 49 (5.52) | - | - |
| 7920 Documentation | Indirect | 166 (18.69) | - | - |
| 7960 Exchange of health care information | Indirect | - | 370 (24.68) | 120 (10.21) |
| 8140 Transfer of patient care | Indirect | 63 (7.09) | - | - |
| Billing review * | Indirect | - | 10 (0.67) | 9 (0.77) |
| Contact with medical staff * | Indirect | - | 185 (12.34) | 45 (3.83) |
| Control of psychotropic medication stock * | Indirect | - | 18 (1.20) | 32 (2.72) |
| Filling in protocols * | Indirect | - | 27 (1.80) | 13 (1.11) |
| Medical record review * | Indirect | - | 114 (7.61) | 35 (2.98) |
| Peripheral vein catheterisation * | Direct | - | 16 (3.98) | 21 (6.29) |
| Prescription registration * | Indirect | - | 265 (17.68) | 384 (32.68) |
| Recording medical history * | Indirect | - | 25 (1.67) | 22 (1.87) |
| Recording patient course * | Indirect | - | 296 (19.75) | 302 (25.70) |
| Requesting material * | Indirect | - | 29 (1.93) | 14 (1.19) |
| Withdrawal of central vascular catheter * | Direct | - | 8 (1.99) | 7 (2.10) |
| Worksheet preparation * | Indirect | - | 26 (1.73) | 13 (1.11) |
| Interventions | Cordova et al. (2010) [3] n (CI 1) | Somensi et al. (2018) [4] (In-Person Observation) n (CI) | Somensi et al. (2018) [4] (Telematic Observation) n (CI) | Average NIC 2 |
|---|---|---|---|---|
| 0140 Encourage body mechanics | 15.08 (5–30) | - | - | 16–30 |
| 0450 Management of constipation/fecal impactation | 15.90 (15–45) | - | - | 16–30 |
| 0580 Bladder catheter | 17.61 (3.5–30) | 7.19 (7.19–7.19) | 16.92 (5.8–28.06) | <15 |
| 0582 Intermittent bladder catheter | - | 15.45 (15.5–15.5) | 10.77 (6.3–15.27) | <15 |
| 0740 Care of bedridden patient | 11.96 (3–30) | - | - | 16–30 |
| 0910 Inmobilisation 0940 Traction/immobilisation care | 15.67 (2.5–60) | - | - | <15 |
| 1080 Nasogastric tube | - | 23.59 (13.8–33.4) | 5.01 (0–12.26) | <15 |
| 1450 Management of nausea 1570 Management of vomiting | 14.25 (2–45) | - | - | 16–30 |
| 1806 Help with self-care: transfer | 18.98 (3.5–45) | - | - | <15 |
| 1872 Thoracic drain care | - | 4.97 (3.51–6.43) | 8.88 (4.8–13.02) | <15 |
| 2080 Management of liquids/electrolytes | 19.66 (1.5–60) | - | - | <15 |
| 2300 Administration of medication | 27.11 (2–120) | 6.11 (2.78–9.44) | 8.44 (5.2–11.77) | <15 |
| 2620 Neurological monitoring | 11 (1–30) | - | - | 16–30 |
| 2690 Seizure precautions | 14.62 (2–30) | - | - | 16–30 |
| 2930 Surgical preparation | 29.35 (7.5–75) | - | - | 46–60 |
| 3160 Airway suction | - | 0.38 (0.38–0.38) | 7 (0–52.74) | <15 |
| 3590 Skin exploration | 11.89 (2–30) | - | - | 16–30 |
| 3660 Wound care | 22.65 (4–60) | - | - | 31–45 |
| 4020 Bleeding reduction | 17.47 (1.5–60) | - | - | 46–60 |
| 4030 Administration of blood products | 31.08 (5–60) | - | - | >60 |
| 4054 Central venous access device management | - | 5.22 (1.17–9.28) | 19.21 (9.8–28.6) | 31–45 |
| 4110 Precautions in embolism | 13.47 (2–30) | - | - | 16–30 |
| 4130 Monitoring liquids | - | 5.05 (5.05–5.05) | - | 16–30 |
| 4210 Invasive hemodynamic monitoring | 22.71 (5–120) | - | - | 46–60 |
| 4232 Phlebotomy: arterial blood extraction | - | 8.87 (2.72–15.03) | 8.91 (4.8–13.02) | <15 |
| 4238 Phlebotomy: venous blood extraction | - | 7.36 (6.19–8.53) | 11.44 (0–24.58) | <15 |
| 4820 Orientation in the health system | - | 3.16 (3.01–3.31) | 4.44 (3.64–5.24) | 16–30 |
| 5240 Counselling | 22.04 (5–45) | - | - | 46–60 |
| 5460 Contact | - | 29.9 (11.9–47.91) | 28.17 (24.5–31.9) | <15 |
| 5606 Education: individual | 21.91 (4–60) | - | - | 31–45 |
| 6200 Emergency care | 40.52 (2–120) | 18.1 (0–52.2) | 9.09 (0–11.52) | 16–30 |
| 6320 Reanimation | - | - | 32.72 (0–233.7) | 16–30 |
| 6460 Dementia management | 35.50 (1.5–120) | - | - | >60 |
| 6486 Environmental management: safety | - | 16.74 (11.86) | 16.74 (11.86) | 31–45 |
| 6540 Infection control | 14.42 (1.5–30) | - | - | 31–45 |
| 7310 Nursing care on admission | 38.31 (5–75) | - | - | 16–30 |
| 7370 Planning for discharge | 31.70 (4–60) | - | - | 46–60 |
| 7680 Assistance in exploration | 14.85 (2–45) | 6.78 (5.7–7.86) | 4.27 (3.9–4.62) | 16–30 |
| 7830 Supervision of personnel | - | 2.07 (1.87–2.28) | 7.21 (2.99–11.4) | >60 |
| 7850 Personnel development | - | 14.5 (0–58.52) | 1.73 (1.6–1.87) | >60 |
| 7910 Consultation | 24.96 (4–62) | - | - | 46–60 |
| 7960 Health care information exchange | 22.34 (3–60) | - | - | <15 |
| Billing review * | - | 12.41 (1.6–23.22) | 13.2 (6.86–19.5) | 46–60 |
| Contact areas of support * | - | 1.36 (1.34–1.39) | 3.38 (2.86–3.89) | <15 |
| Contact with medical personnel * | - | 1.49 (1.28–1.69) | 3 (2.38–3.64) | 16–30 |
| Control of psychotropic medication * | - | 8.11 (0–18.78) | 12.06 (7.67–16.5) | 16–30 |
| Filling-in protocols * | - | 5.41 (3.18–7.65) | 7.59 (4.06–11.1) | 46–60 |
| Medical record review * | - | 5.51 (5.39–5.63) | 31.19 (20.3–42.1) | 46–60 |
| Peripheral vein catheterization * | - | 8.71 (0–57.9) | 11.72 (7.9–15.56) | 31–45 |
| Prescription registration * | - | 3.18 (2.97–3.38) | 3.03 (2.8–3.27) | 16–30 |
| Recording medical history * | - | 9.48 (9.17–9.78) | 10.19 (7.3–13.1) | 16–30 |
| Recording patient course * | - | 2.32 (2.06–2.59) | 3.43 (3.16–3.7) | 16–30 |
| Requesting material * | - | 5.39 (0–11.52) | 11.88 (9.41–14.3) | 16–30 |
| Withdrawal of central vascular catheter * | - | 9.06 (5.89–12.2) | 9.13 (6.9–11.39) | 31–45 |
| Worksheet preparation * | - | 18.81 (0–219.8) | 36.97 (25.9–48) | 46–60 |
| 1410 Pain management: acute ** | 13.39 (2–45) | - | - | 31–45 |
| 0960 Transport *** | 27.97 (4–75) | - | - | <15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Suárez, C.-A.; Rodríguez-Álvaro, M.; García-Hernández, A.-M.; Fernández-Gutiérrez, D.-Á.; Martínez-Alberto, C.-E.; Brito-Brito, P.-R. Use of the Nursing Interventions Classification and Nurses’ Workloads: A Scoping Review. Healthcare 2022, 10, 1141. https://doi.org/10.3390/healthcare10061141
Rodríguez-Suárez C-A, Rodríguez-Álvaro M, García-Hernández A-M, Fernández-Gutiérrez D-Á, Martínez-Alberto C-E, Brito-Brito P-R. Use of the Nursing Interventions Classification and Nurses’ Workloads: A Scoping Review. Healthcare. 2022; 10(6):1141. https://doi.org/10.3390/healthcare10061141
Chicago/Turabian StyleRodríguez-Suárez, Claudio-Alberto, Martín Rodríguez-Álvaro, Alfonso-Miguel García-Hernández, Domingo-Ángel Fernández-Gutiérrez, Carlos-Enrique Martínez-Alberto, and Pedro-Ruymán Brito-Brito. 2022. "Use of the Nursing Interventions Classification and Nurses’ Workloads: A Scoping Review" Healthcare 10, no. 6: 1141. https://doi.org/10.3390/healthcare10061141
APA StyleRodríguez-Suárez, C.-A., Rodríguez-Álvaro, M., García-Hernández, A.-M., Fernández-Gutiérrez, D.-Á., Martínez-Alberto, C.-E., & Brito-Brito, P.-R. (2022). Use of the Nursing Interventions Classification and Nurses’ Workloads: A Scoping Review. Healthcare, 10(6), 1141. https://doi.org/10.3390/healthcare10061141