
Singing for the Rehabilitation of Acquired Neurogenic Communication Disorders: Continuing the Evidence Dialogue with a Survey of Current Practices in Speech-Language Pathology


Abstract
:1. Introduction
2. Materials and Methods
2.1. Conception of the Study
2.2. Target Population
2.3. Type and Size of the Sample
2.4. Questionnaire
2.5. Procedure
2.6. Data Analysis
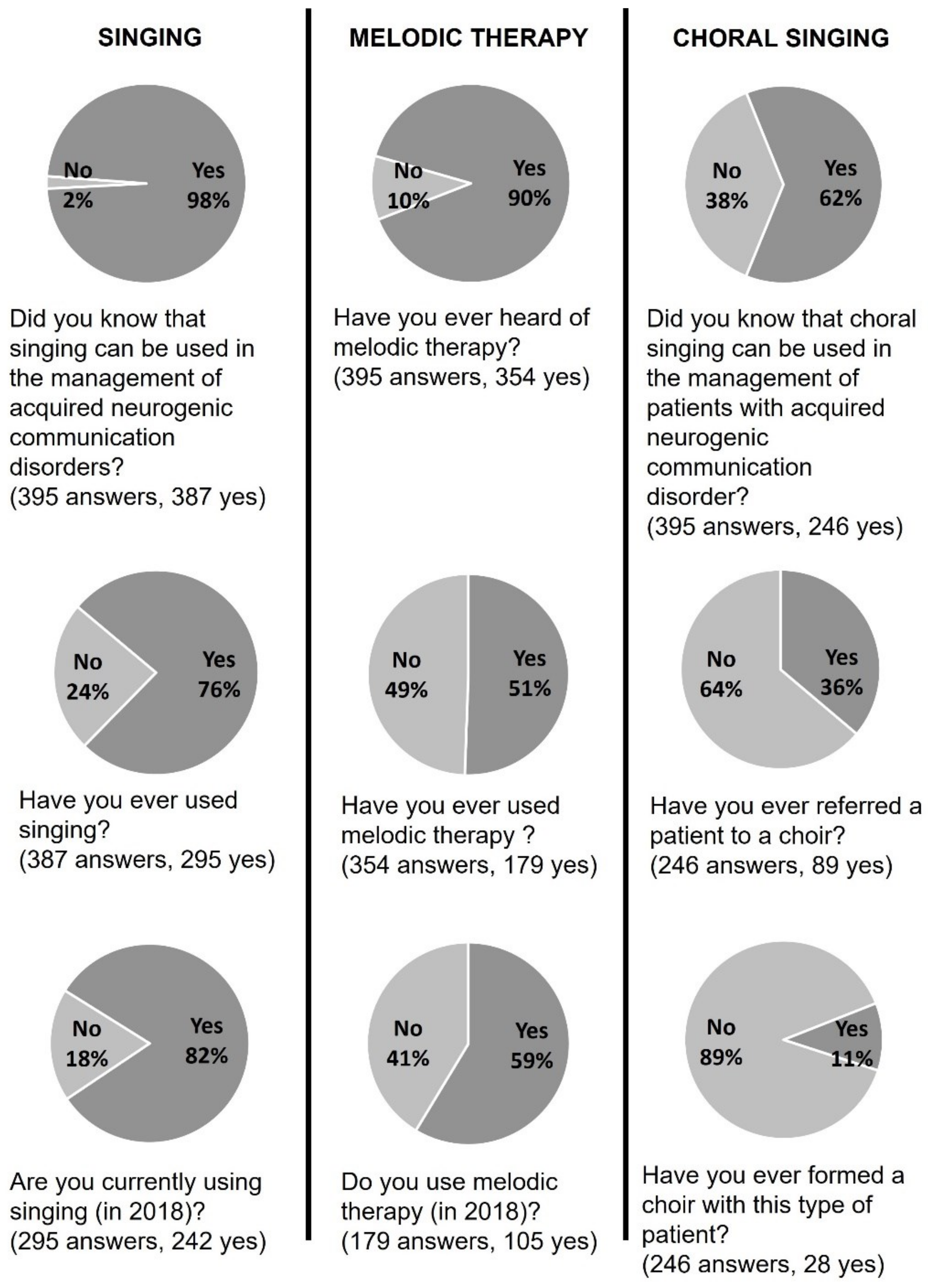
3. Results
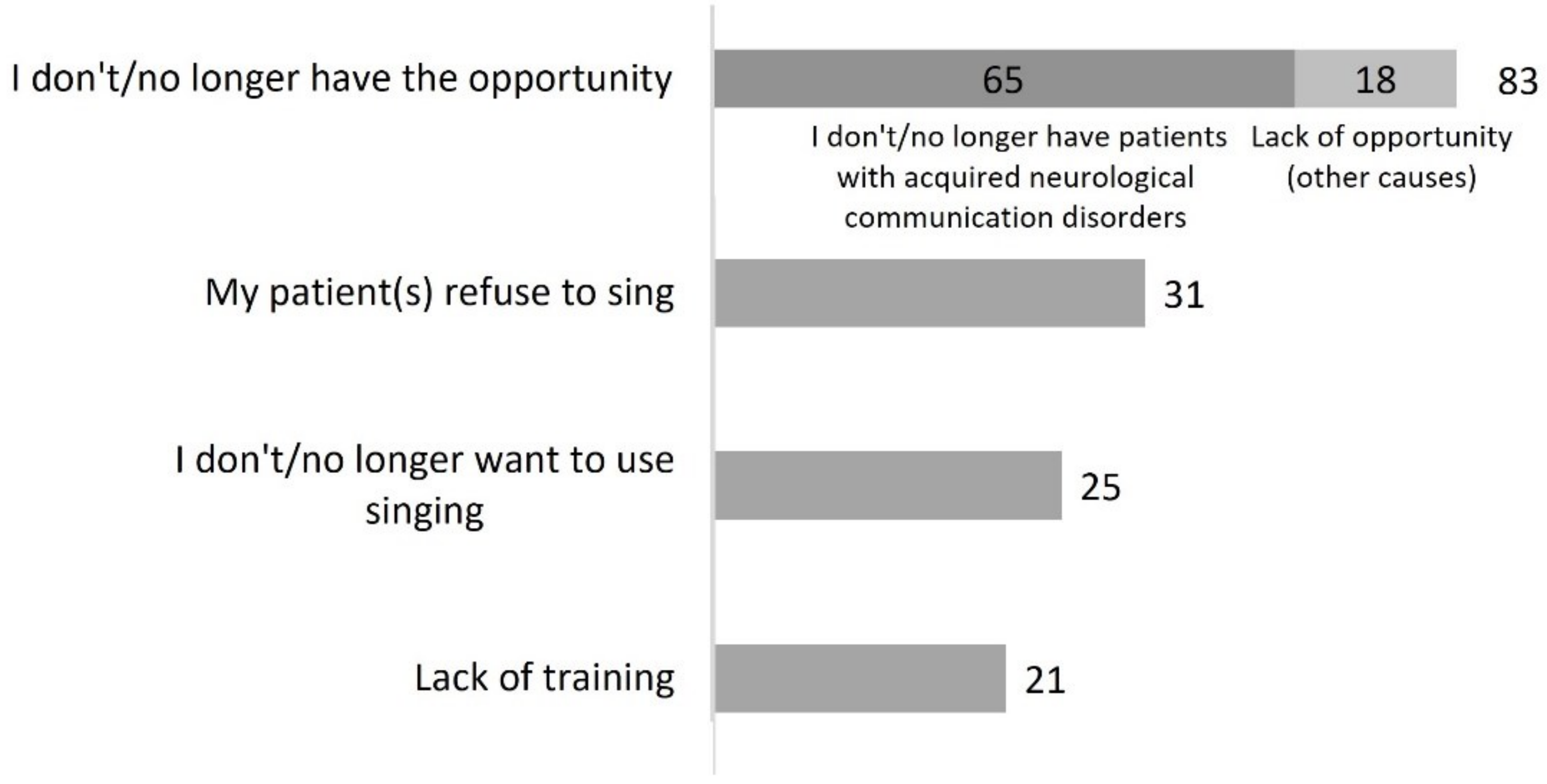
3.1. Singing
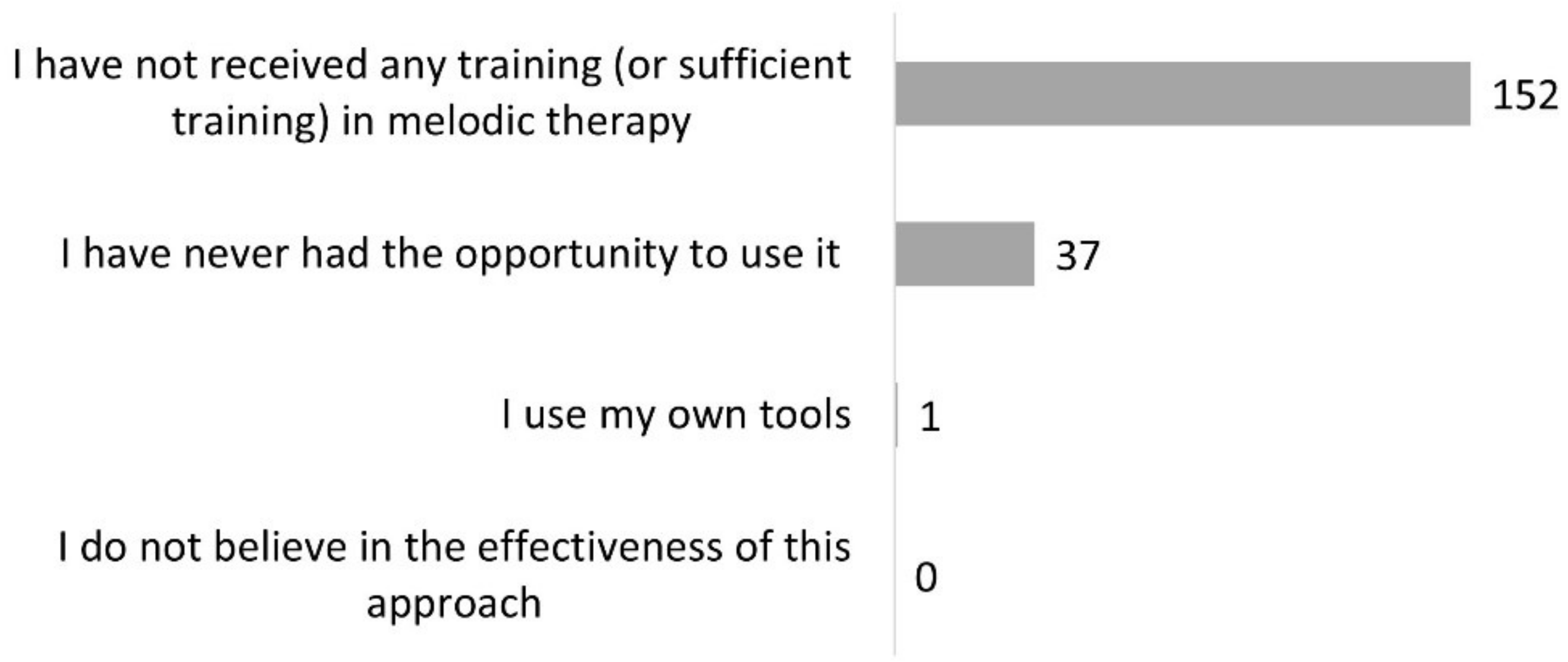
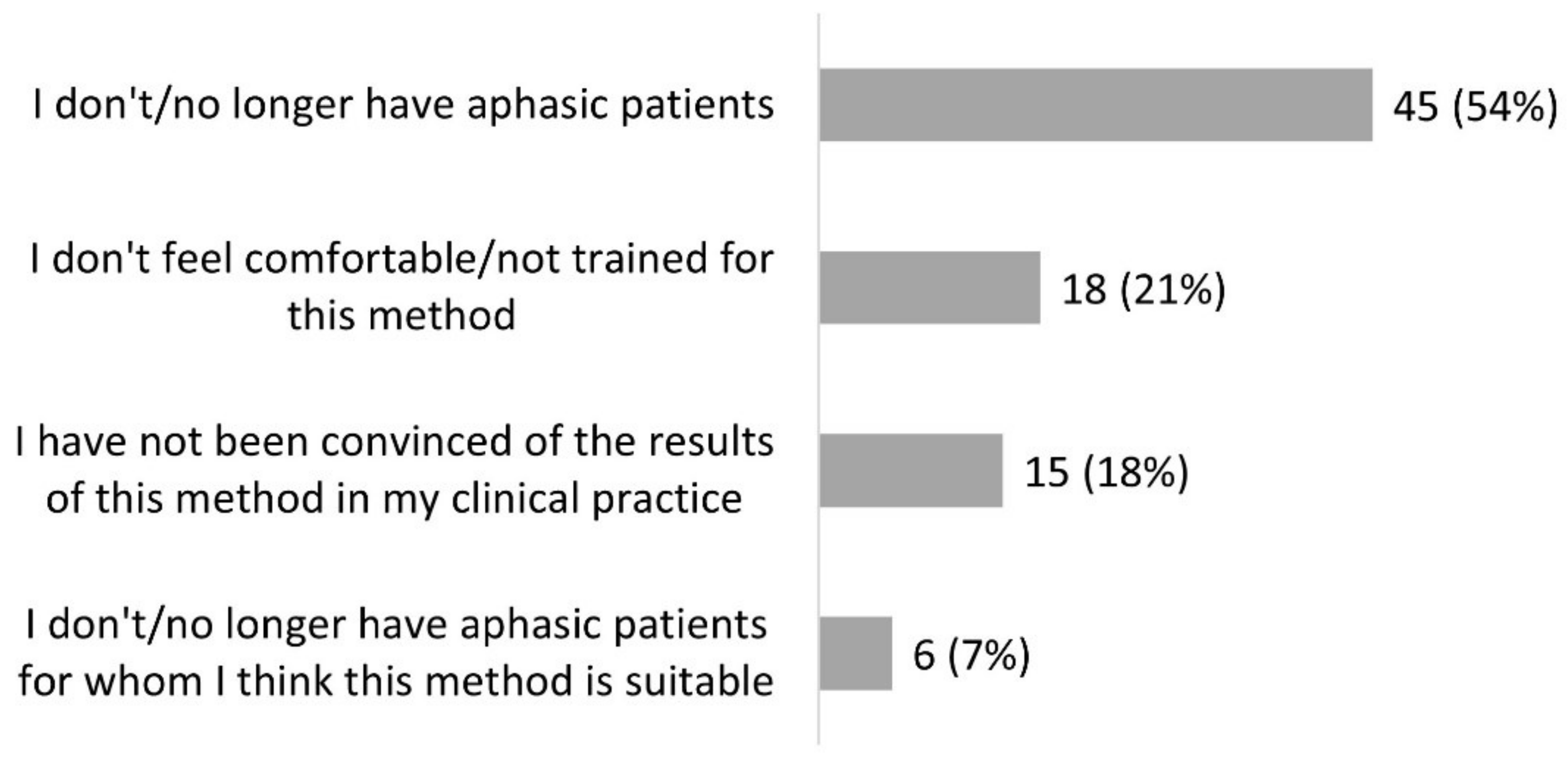
3.2. Melodic Therapy
3.3. Choral Singing
4. Discussion
4.1. Singing
4.2. Melodic Therapy
4.3. Choral Singing
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magee, W.L.; Clark, I.; Tamplin, J.; Bradt, J. Music Interventions for Acquired Brain Injury. Cochrane Database Syst. Rev. 2017, 1, CD006787. [Google Scholar] [CrossRef] [PubMed]
- Monroe, P.; Halaki, M.; Kumfor, F.; Ballard, K.J. The Effects of Choral Singing on Communication Impairments in Acquired Brain Injury: A Systematic Review. Int. J. Lang. Commun. Disord. 2020, 55, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Sihvonen, A.J.; Särkämö, T.; Leo, V.; Tervaniemi, M.; Altenmüller, E.; Soinila, S. Music-Based Interventions in Neurological Rehabilitation. Lancet Neurol. 2017, 16, 648–660. [Google Scholar] [CrossRef] [Green Version]
- Van der Meulen, I.; Van de Sandt-Koenderman, W.M.E.; Heijenbrok-Kal, M.H.; Visch-Brink, E.G.; Ribbers, G.M. The Efficacy and Timing of Melodic Intonation Therapy in Subacute Aphasia. Neurorehabilit. Neural Repair 2014, 28, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Zumbansen, A.; Peretz, I.; Hébert, S. The Combination of Rhythm and Pitch Can Account for the Beneficial Effect of Melodic Intonation Therapy on Connected Speech Improvements in Broca’s Aphasia. Front. Hum. Neurosci. 2014, 8, 592. [Google Scholar] [CrossRef] [Green Version]
- Tamplin, J.; Morris, M.E.; Marigliani, C.; Baker, F.A.; Noffs, G.; Vogel, A.P. ParkinSong: Outcomes of a 12-Month Controlled Trial of Therapeutic Singing Groups in Parkinson’s Disease. J. Parkinson’s Dis. 2020, 10, 1217–1230. [Google Scholar] [CrossRef]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Numminen, A.; Kurki, M.; Johnson, J.K.; Rantanen, P. Cognitive, Emotional, and Social Benefits of Regular Musical Activities in Early Dementia: Randomized Controlled Study. Gerontologist 2014, 54, 634–650. [Google Scholar] [CrossRef] [Green Version]
- Thaut, M.H.; McIntosh, G.C.; Hoemberg, V. Neurologic Music Therapy: From Social Science to Neuroscience. In Oxford Handbook of Neurologic Music Therapy; Oxford University Press: Oxford, UK, 2014; pp. 1–6. [Google Scholar]
- Clements-Cortes, A.; Bartel, L. Are We Doing More Than We Know? Possible Mechanisms of Response to Music Therapy. Front. Med. 2018, 5, 255. [Google Scholar] [CrossRef]
- Baroncelli, L.; Braschi, C.; Spolidoro, M.; Begenisic, T.; Sale, A.; Maffei, L. Nurturing Brain Plasticity: Impact of Environmental Enrichment. Cell Death Differ. 2010, 17, 1092–1103. [Google Scholar] [CrossRef]
- Merrett, D.L.; Peretz, I.; Wilson, S.J. Neurobiological, Cognitive, and Emotional Mechanisms in Melodic Intonation Therapy. Front. Hum. Neurosci. 2014, 8, 401. [Google Scholar] [CrossRef] [Green Version]
- Yamadori, A.; Osumi, Y.; Masuhara, S.; Okubo, M. Preservation of Singing in Broca’s Aphasia. J. Neurol. Neurosurg. Psychiatry 1977, 40, 221–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jungblut, M.; Aldridge, D. Musik Als Brücke Zur Sprache—Die Musiktherapeutische Behandlungsmethode “SIPARI®” Bei Langzeitaphasikern [Music as a Bridge to Speech—the Music-Therapeutic Treatment Method SIPARI® with Long-Term Aphasia Patient]. Neurol. Rehabil. 2004, 10, 69–78. [Google Scholar]
- Yinger, O.S.; Lapointe, L.L. The Effects of Participation in a Croup Music Therapy Voice Protocol (G-MTVP) on the Speech of Individuals with Parkinson’s Disease. Music Ther. Perspect. 2012, 30, 25–31. [Google Scholar] [CrossRef]
- Di Benedetto, P.; Cavazzon, M.; Mondolo, F.; Rugiu, G.; Peratoner, A.; Biasutti, E. Voice and Choral Singing Treatment: A New Approach for Speech and Voice Disorders in Parkinson’s Disease. Eur. J. Phys. Rehabil. Med. 2009, 45, 13–19. [Google Scholar]
- Albert, M.L.; Sparks, R.W.; Helm, N.A. Melodic Intonation Therapy for Aphasia. Arch. Neurol. 1973, 29, 130–131. [Google Scholar] [CrossRef]
- Zumbansen, A.; Peretz, I.; Hébert, S. Melodic Intonation Therapy: Back to Basics for Future Research. Front. Neurol. 2014, 5, 7. [Google Scholar] [CrossRef] [Green Version]
- Sparks, R.; Helm, N.; Albert, M. Aphasia Rehabilitation Resulting from Melodic Intonation Therapy. Cortex 1974, 10, 303–316. [Google Scholar] [CrossRef]
- Baker, F.A. Modifying the Melodic Intonation Therapy Program for Adults With Severe Non-Fluent Aphasia. Music Ther. Perspect. 2000, 18, 110–114. [Google Scholar] [CrossRef]
- Conklyn, D.; Novak, E.; Boissy, A.; Bethoux, F.; Chemali, K. The Effects of Modified Melodic Intonation Therapy on Nonfluent Aphasia: A Pilot Study. J. Speech Lang. Hear. Res. JSLHR 2012, 55, 1463–1471. [Google Scholar] [CrossRef]
- Stahl, B.; Henseler, I.; Turner, R.; Geyer, S.; Kotz, S.A. How to Engage the Right Brain Hemisphere in Aphasics without Even Singing: Evidence for Two Paths of Speech Recovery. Front. Hum. Neurosci. 2013, 7, 35. [Google Scholar] [CrossRef] [Green Version]
- Van Eeckhout, P.; Bhatt, P. Rythme, Intonation, Accentuation: La Rééducation Des Aphasies Non-Fluentes Sévères. Rééduc. Orthophonique 1984, 22, 311–327. [Google Scholar]
- Cortese, M.D.; Riganello, F.; Arcuri, F.; Pignataro, L.M.; Buglione, I. Rehabilitation of Aphasia: Application of Melodic-Rhythmic Therapy to Italian Language. Front. Hum. Neurosci. 2015, 9, 520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.A.; Haynes, R.B.; Richardson, W.S. Evidence Based Medicine: What It Is and What It Isn’t. Br. Med. J. 1996, 312, 71–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Direction de la Recherche, des Études, de L’évaluation et des Statistiques (DREES) [National Division of Research, Studies, Evaluation and Statistics]. Effectif Des Orthophonistes Par Mode D’exercice Global, Zone D’activité Principale, Sexe et Tranche d’âge [Number of Speech-Language Pathologists by Overall Practice Pattern, Primary Practice Area, Gender and Age Group]. Available online: http://www.data.drees.sante.gouv.fr/TableViewer/tableView.aspx?ReportId=3719 (accessed on 9 March 2021).
- Raglio, A.; Oasi, O.; Gianotti, M.; Rossi, A.; Goulene, K.; Stramba-Badiale, M. Improvement of Spontaneous Language in Stroke Patients with Chronic Aphasia Treated with Music Therapy: A Randomized Controlled Trial. Int. J. Neurosci. 2016, 126, 235–242. [Google Scholar] [CrossRef]
- Särkämö, T.; Tervaniemi, M.; Laitinen, S.; Forsblom, A.; Soinila, S.; Mikkonen, M.; Autti, T.; Silvennoinen, H.M.; Erkkilä, J.; Laine, M.; et al. Music Listening Enhances Cognitive Recovery and Mood after Middle Cerebral Artery Stroke. Brain 2008, 131, 866–876. [Google Scholar] [CrossRef] [Green Version]
- Chu, H.; Yang, C.-Y.; Lin, Y.; Ou, K.-L.; Lee, T.-Y.; O’Brien, A.P.; Chou, K.-R. The Impact of Group Music Therapy on Depression and Cognition in Elderly Persons with Dementia: A Randomized Controlled Study. Biol. Res. Nurs. 2014, 16, 209–217. [Google Scholar] [CrossRef]
- Pohl, P.; Wressle, E.; Lundin, F.; Enthoven, P.; Dizdar, N. Group-Based Music Intervention in Parkinson’s Disease—Findings from a Mixed-Methods Study. Clin. Rehabil. 2020, 34, 533–544. [Google Scholar] [CrossRef] [Green Version]
- Fogg-Rogers, L.; Buetow, S.; Talmage, A.; McCann, C.M.; Leão, S.H.S.; Tippett, L.; Leung, J.; McPherson, K.M.; Purdy, S.C. Choral Singing Therapy Following Stroke or Parkinson’s Disease: An Exploration of Participants’ Experiences. Disabil. Rehabil. 2016, 38, 952–962. [Google Scholar] [CrossRef]
- Talmage, A.; Ludlam, S.; Leao, S.H.; Fogg-Rogers, L.; Purdy, S.C. Leading the CeleBRation Choir: The Choral Singing Therapy Protocol and the Role of the Music Therapist in a Social Singing Group for Adults with Neurological Conditions. N. Z. J. Music Ther. 2013, 11, 7–50. [Google Scholar]
- Tamplin, J.; Baker, F.A.; Jones, B.; Way, A.; Lee, S. “Stroke a Chord”: The Effect of Singing in a Community Choir on Mood and Social Engagement for People Living with Aphasia Following a Stroke. NeuroRehabilitation 2013, 32, 929–941. [Google Scholar] [CrossRef]
- Hurkmans, J.; de Bruijn, M.; Boonstra, A.M.; Jonkers, R.; Bastiaanse, R.; Arendzen, H.; Reinders-Messelink, H.A. Music in the Treatment of Neurological Language and Speech Disorders: A Systematic Review. Aphasiology 2012, 26, 1–19. [Google Scholar] [CrossRef]
- Racette, A.; Bard, C.; Peretz, I. Making Non-Fluent Aphasics Speak: Sing Along! Brain 2006, 129, 2571–2584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Kelly, J.; Magee, W.L. The Complementary Role of Music Therapy in the Detection of Awareness in Disorders of Consciousness: An Audit of Concurrent SMART and MATADOC Assessments. Neuropsychol. Rehabil. 2013, 23, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, A.S.F.; Ramos, A.; Bermejo, E.; Casero, M.; Corrales, J.M.; Grantham, S. Effects of Different Musical Stimuli in Vital Signs and Facial Expressions in Patients with Cerebral Damage: A Pilot Study. J. Am. Assoc. Neurosci. Nurses 2014, 46, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Maggiori, M. Music Therapy in France. Available online: https://wfmt.info/resource-centers/publication-center/regional-information/ (accessed on 14 May 2022).
- Schulkind, M.D.; Hennis, L.K.; Rubin, D.C. Music, Emotion, and Autobiographical Memory: They’re Playing Your Song. Mem. Cogn. 1999, 27, 948–955. [Google Scholar] [CrossRef] [PubMed]
- Kasdan, A.; Kiran, S. Please Don’t Stop the Music: Song Completion in Patients with Aphasia. J. Commun. Disord. 2018, 75, 72–86. [Google Scholar] [CrossRef]
- Ferguson, J.H.; Altrocchi, P.H.; Brin, M.F.; Goldstein, M.L.; Gorelick, P.B.; Hanley, D.F.; Vandennoort, S. American Academy of Neurology Assessment: Melodic Intonation Therapy. Neurology 1994, 44, 566–568. [Google Scholar]
- Cohen, N.S. The Effect of Singing Instruction on the Speech Production of Neurologically Impaired Persons. J. Music Ther. 1992, 29, 87–102. [Google Scholar] [CrossRef]
- Mantie-Kozlowski, A.; Mantie, R.; Keller, C.H. Enjoyment in a Recreational Sing-along Group for People with Aphasia and Their Caregivers. Aphasiology 2018, 32, 518–537. [Google Scholar] [CrossRef]
- Bickerdike, L.; Booth, A.; Wilson, P.M.; Farley, K.; Wright, K. Social Prescribing: Less Rhetoric and More Reality. A Systematic Review of the Evidence. BMJ Open 2017, 7, e013384. [Google Scholar] [CrossRef]
- Leguédé, F. Les Facilitateurs et les Obstacles dans la Participation à une Activité Chorale Chez le Sujet Porteur D’un Trouble Acquis de la Communication D’origine Neurologique [Facilitators and Barriers to Participation in Choral Activity in Individuals with Neurological Acquired Communication Disorders]. Master’s Thesis, Université de Franche-Comté, Besançon, France, 2018. [Google Scholar]
- European Choral Association. Singing Europe; European Choral Association: Bonn, Germany, 2015. [Google Scholar]
- Higgins, A.N.; Richardson, K.C. The Effects of a Choral Singing Intervention on Speech Characteristics in Individuals With Parkinson’s Disease: An Exploratory Study. Commun. Disord. Q. 2019, 40, 195–205. [Google Scholar] [CrossRef]
- Mittelman, M.S.; Papayannopoulou, P.M.; Vernooij-Dassen, M.; Moniz-Cook, E.; Jeon, Y.-H. The Unforgettables: A Chorus for People with Dementia with Their Family Members and Friends. Int. Psychogeriatr. 2018, 30, 779–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zumbansen, A.; Peretz, I.; Anglade, C.; Bilodeau, J.; Généreux, S.; Hubert, M.; Hébert, S. Effect of Choir Activity in the Rehabilitation of Aphasia: A Blind, Randomised, Controlled Pilot Study. Aphasiology 2017, 31, 879–900. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Theme | Occurrences | Quote (Example of a Participant) | |||
|---|---|---|---|---|---|
| Disorders | |||||
| Neurodegenerative diseases (total) | 109 | ||||
| Alzheimer’s type dementia | 50 | “with patients with Alzheimer’s disease, we sing familiar songs together.” (P293) | |||
| Parkinson’s disease | 44 | “voice therapy with Parkinson’s patients” (P111) | |||
| Neurodegenerative diseases | 11 | “as part of the rehabilitation in neurodegenerative diseases” (P62) | |||
| Huntington’s disease | 2 | “targeting articulation and rhythm ((...) Huntington’s chorea...)” (P153) | |||
| Multiple sclerosis | 1 | “I sometimes make people sing or hum (...) with MS” (P354) | |||
| Progressive supranuclear palsy | 1 | “I recently received a patient with PSP and singing became my working tool with her” (P81) | |||
| Aphasia (total) | 84 | ||||
| Aphasia | 81 | “with an aphasic patient, I try to sing songs with her” (P168) | |||
| Anomia | 3 | “using intonation in anomia therapies” (P46) | |||
| Dysarthria | 22 | “In the context of dysarthria it works with the rhythm and the melody.” (P345) | |||
| Voice disorder | 5 | “Vocalizations for voice rehabilitation.” (P346) | |||
| Dysphagia | 2 | “Individual and collective for (...) dysphagia” (P34) | |||
| Apraxia | 2 | “work of buccofacial apraxia” (P106) | |||
| Neurological diseases | 2 | “I sing with my ‘neuro’ patients” (P231) | |||
| Stuttering | 1 | “Use of nursery rhymes/songs for patients who stutter” (P373) | |||
| Oral language disorders | 1 | “I have always used singing in all my rehabilitations (oral or written language)” (P13) | |||
| Written language disorders | 1 | “I have always used singing in all my rehabilitations (oral or written language)” (P13) | |||
| Deafness | 1 | “Constitution of a choir (with small orchestra) for people with cochlear implants” (P373) | |||
| Ataxia | 1 | “Rhythm (in the context of ataxia)...” (P372) | |||
| Therapy formats | |||||
| Individual | 278 | “Use of singing in one-on-one session” (P332) | |||
| Group | 46 | “choral for people with aphasia” (P122) | |||
| Homework | 2 | “at home as complementary work” (P72) | |||
| Targeted domains | |||||
| Language | 200 | “Using automatic abilities to access language” (P47) | |||
| Memory (total) | 143 | ||||
| Semantic memory | 79 | “I hide the text and ask them to find the last word of each sentence” (P287) | |||
| Memory | 40 | “Stimulating memory” (P90) | |||
| Procedural memory | 26 | “ song lyrics used for the automatic ending of sentences” (P256) | |||
| Autobiographical memory | 19 | “We also listen to music to bring out emotions and even memories” (P206) | |||
| Episodic memory | 10 | “ to train episodic memory “ (P370) | |||
| Speech and voice | 101 | “(...) with people who have lost in fluidity of speech” (P224) | |||
| Executive functions | 40 | “I often propose songs to stimulate language, memory, attention, respect of rhythm” (P376) | |||
| Speech restoration | 37 | “to restore speech in patients” (P120) | |||
| Pleasure | 34 | “Sometimes also just for the pleasure of listening to an artist they liked” (P324) | |||
| Rhythm | 28 | “by proposing (...) melodies to work on articulation and rhythm” (P153) | |||
| Communication | 18 | “non-verbal communication intensifies” “working on turn taking “ (P232) | |||
| Emotions | 14 | “expression of emotion through singing in someone who is disoriented” (P367) | |||
| Awakening | 9 | “We would choose a song with the patient and (...) I would sing and the patient would follow or wake up to the words “ (P243) | |||
| Sense of identity | 7 | “We sing together because this memory is preserved so it is gratifying” (P178) | |||
| Cognitive stimulation | 6 | “The lyrics of the songs are the starting point for many cognitive stimulation exercises” (P88) | |||
| Therapeutic bond | 5 | “I use singing (...) with the idea of being connected to the patient” (P264) | |||
| Swallowing | 3 | “Rehabilitation of swallowing” (P94) | |||
| Social ties | 3 | “A patient with Alzheimer’s disease participates in a choir, which is very valuable for him because it (...) gives him the opportunity to socialize” (P303) | |||
| Modalities | |||||
| Production | 241 | “Singing duet with patient or music found on the internet and the patient sings the lyrics” (P74) | |||
| Reception | 241 | “Listening to songs and working on emotions and memories” (P271) | |||
| Activities | |||||
| Completion of sung phrases | 50 | “by playing musical excerpts to patients and (...) asking them to sing the rest. “ (P4) | |||
| Melodic therapy | 49 | “use of the principles of Melodic Intonation Therapy or Thérapie Mélodique et Rythmée” (P234) | |||
| Singing in unison | 40 | “ singing in duet with the patient” (P74) | |||
| Song games (total) | 30 | ||||
| Melody quizzes (total) | 16 | ||||
| Melody quizzes | 8 | “finding the singer, or the title of a hummed song”, “blindtest” (P304) | |||
| Melody/performer association | 3 | “humming a melody and the patient must find the title or performer” (P150) | |||
| Melody/lyrics association | 3 | “beginning of melodic phrase… it’s up to her to put the lyrics to it” (P65) | |||
| Melody/title association | 2 | “humming a melody and the patient must find the title or performer” (P150) | |||
| Lyrics/song association | 6 | “search for songs from a word” (P174) | |||
| Title/singer association | 5 | “association of a song title and its singer for example” (P239) | |||
| Song games | 3 | “we make singing games” (P231) | |||
| Vocal exercises | 26 | “warm-up vocalization (…) that will help to work on prosody” (P153) | |||
| Listening | 21 | “Listening to songs” (P271) | |||
| Choir | 19 | “singing group as part of a long-term care service in the hospital” (P339) | |||
| Evocation | 19 | “pleasure to sing at the end of the session and remember the memories it evokes” (P150) | |||
| Reading | 15 | “reading aloud the lyrics” (P365) | |||
| Repetition | 11 | “singing phrases to facilitate their repetition”(P229) | |||
| Karaoke | 10 | “when possible, I do karaoke” (P306) | |||
| Rhythmic exercises | 8 | “we also work on purely rhythmic exercises” (P99) | |||
| Body exercises | 7 | “I combine body and vocal exercises” (P9) | |||
| Psychophony approach | 3 | “I use the tools and the approach of the psychophony method” (P391) | |||
| Automatic series | 3 | “I use singing to initiate, recite, remember automatic series” (P224) | |||
| Associated with the Lee Silverman Voice Treatment program | 3 | “As a complement to the LSVT” (P249) | |||
| Beatboxing | 1 | “use of human beatboxing techniques” (P275) | |||
| Mimes | 1 | “I sing mime rhymes (I sing and mime)” (P319) | |||
| Types of music | |||||
| Personalized music | 80 | “use of songs known to the patient” (P232) | |||
| Popular songs | 62 | “traditional French songs, La Marseillaise” (P131) | |||
| Rhymes | 17 | “mainly in known nursery rhymes” (P291) | |||
| Prayers | 2 | “ canticle heard many times in his childhood” (P263) | |||
| Theme | Occurrences | Quote (Example of a Participant) | |||
|---|---|---|---|---|---|
| Sources of information | |||||
| Training (total) | 12 | ||||
| Continuous education | 6 | “I trained with Dominique Benichou last year.” (P78) | |||
| Initial training | 3 | “I had some knowledge of this practice during my initial training” (P155) | |||
| Training | 3 | “systematic protocol after training” (P69) | |||
| Personal readings (total) | 12 | ||||
| Manual | 6 | “In one-on-one session, with the help of the manual” (P34) | |||
| Articles (total) | 3 | ||||
| Van Eeckhout writings | 2 | “with texts by Philippe Van Eeckhout” (P177) | |||
| Article | 1 | “I relied on a book or article describing this work” (P63) | |||
| Software | 2 | “I have a software and I follow it” (P317) | |||
| Personal reading | 1 | “I read a lot on the subject to deepen my understanding and practice” (P379) | |||
| Colleagues | 8 | “I worked with a colleague who was trained; she introduced me to it a little” (P9) | |||
| No training | 2 | “Unfortunately, I haven’t undergone the training yet” (P60) | |||
| Disorders | |||||
| Aphasia | 80 | ||||
| Aphasia | 39 | “with aphasic patients” (P217) | |||
| Non-fluent aphasia | 32 | “early therapy in patients with non-fluent aphasia” (P167) | |||
| Anomia | 5 | “in anomia therapies” (P46) | |||
| Fluent aphasia | 1 | “sometimes in fluent aphasia” (P202) | |||
| Mixed aphasia | 1 | “Mixed aphasia profile” (P349) | |||
| Motor aphasia | 1 | “mainly in the context of motor aphasia “ (P355) | |||
| Agrammatism | 1 | “With aphasic (…) agrammatic patients “ (P374) | |||
| Parkinson’s disease | 5 | “with patients with (…) Parkinson’s disease to work on prosody” (P275) | |||
| Dysarthria | 2 | “for dysarthric patients (…) with speech rate and prosody disorders “ (P6) | |||
| Neurological diseases | 1 | “with aphasic or ‘neuro’ patients” (P98) | |||
| Alzheimer’s type dementia | 1 | “with Alzheimer’s patients (…)” (P275) | |||
| Developmental disorders | 1 | “ Whether it’s for (…) children with disabilities or aphasia, it’s always a good help” (P104) | |||
| Language delays/disorders | 1 | “Whether it’s for big language delays (…), it’s always a good help” (P104) | |||
| Impairment severity | |||||
| Severe | 6 | “I have used TMR with some patients with severe aphasia” (P38) | |||
| Moderate | 1 | “For lexical production deficits in moderate aphasia” (P338) | |||
| Targeted domains | |||||
| Language | 165 | ||||
| Language | 102 | “In the context of massive aphasia, where automatic language can be spared” (P136) | |||
| Language production | 63 | “For lexical production deficits in moderate aphasia” (P338) | |||
| Speech restoration | 22 | “speech restoration in the beginning of care” (P7) | |||
| Speech | 12 | “support for the articulation of a word” (P162) | |||
| Rhythm | 3 | “I work on rhythm reproduction” (P119) | |||
| Communication | 2 | “especially for all polite forms, communication openings, simple requests. “ (P251) | |||
| Speech perception | 1 | “to work on auditory discrimination” (P188) | |||
| Sense of identity | 1 | “It allows them to hear themselves, be proud” (P374) | |||
| Observance of the method | |||||
| Isolated facilitation technique | 45 | “I chant the syllables following the melodic pattern” (P25) | |||
| Entire program | 22 | “following the systematic protocol after training” (P69) | |||
| Part of the program | 12 | “I have never been able to get past the rhythmic stage of the program because my patients are struggling with it” (P30) | |||
| Departures from conventional programs | |||||
| Combination with more regular singing | 2 | “working on speech and communication disorders in association with pure singing” (P35) | |||
| Reading | 2 | “Sentence repetition, sentence generation, reading in patients with dysarthria and aphasia “ (P345) | |||
| Telling about one’s day | 1 | “We tell the patient’s day in this way: the lunch menu, the weekend activities...” (P40) | |||
| Naming | 1 | “during naming exercises, with the support of syntactic constructions” (P70) | |||
| Homework | 1 | “Modeling phrases to be trained at home” (P344) | |||
| Time of use | |||||
| Beginning of care | 22 | “in the initial phase of aphasic patient’s care for speech restoration “ (P68) | |||
| Each session | 12 | “I use it every session with patients with severe expression deficits” (P40) | |||
| At the beginning of sessions | 1 | “at the beginning of each session and sometimes throughout the session in cases of very severe aphasia “ (P215) | |||
| At the end of a session | 1 | “Quite often at the end of a session when fatigue sets” (P30) | |||
| Importance within therapy options | |||||
| Important | 18 | “She is at the center of four of my interventions” (P31) | |||
| Rare | 15 | “I use it too little to talk about it” (P99) | |||
| Used among other approaches | 11 | “with people with aphasia (combined with other approaches) “ (P220) | |||
| Second choice | 2 | “I have used TMR with some patients with severe aphasia after working with more traditional approaches” (P38) | |||
| Theme | Occurrences | Quote (Example of a Participant) | |
|---|---|---|---|
| Targeted domains | |||
| Speech and voice | 34 | “To free his voice, (…) stimulate rhythm and voice projection” (P393) | |
| Social ties | 33 | “to regain a social link” (P297) | |
| Pleasure | 15 | “because I thought it was very important for the patient to rediscover the pleasure of singing in a group” (P167) | |
| Language | 14 | “Because his language is more fluent in singing” (P25) | |
| Well-being | 11 | “Continuity of the work done in speech-language therapy with the addition of a social, playful and well-being dimension” (P312) | |
| Memory | 8 | “Patient in the early stage of Alzheimer’s disease seeking to maintain memory” (P304) | |
| Communication | 5 | “It depends, it can be for a rather functional or rather communicational purpose, or mixed more often!” (P220) | |
| Sense of identity | 4 | “Young patient (stroke) formerly a singer, with experience in choral singing, needing to restore her self-image and skills (…)” (P388) | |
| Cognitive functions | 2 | “(…) Cognitive and language stimulation” (P5) | |
| Favorable conditions for the success of this referral | |||
| Former choir singer | 9 | “these were patients who had already practiced choral singing before and who had stopped because of their disorders” (P177) | |
| Singing benefits noticed | 5 | “Patient (…) showing clear signs of progress when using singing during sessions” (P12) | |
| Available adapted choir | 5 | “Towards a choir set up by the clinic where I worked, in collaboration with France Parkinson (…)” (P43) | |
| Likes to sing | 3 | “The patient already had an interest in singing, and liked to sing, so we thought that this would be a good activity” (P239) | |
| Patient’s request | 3 | “Because patients were asking for more singing and had trouble doing it alone (…)” (P33) | |
| Facilitated inclusion | 2 | “because I am part of this choir and it was easy for me to include them and enjoy the benefits of socialization” (P99) | |
| Easy to set up | 1 | “Because easily set up” (P127) | |
| Sufficient recovery | 1 | “It was a patient (…) who had progressed enough to feel comfortable again in a small country choir” (P229) | |
| Complementary role to conventional speech-language therapy | 16 | “(…)to complete/enrich the care” (P73) | |
| Disorders | |||
| Parkinson’s disease | 11 | “in a patient with Parkinson’s disease, to maintain skills acquired in rehabilitation” (P76) | |
| Alzheimer’s disease | 2 | “For a young patient with Alzheimer’s disease in the early stage, the goal is to stimulate memory (…)” (P75) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behaghel, E.; Zumbansen, A. Singing for the Rehabilitation of Acquired Neurogenic Communication Disorders: Continuing the Evidence Dialogue with a Survey of Current Practices in Speech-Language Pathology. Healthcare 2022, 10, 1010. https://doi.org/10.3390/healthcare10061010
Behaghel E, Zumbansen A. Singing for the Rehabilitation of Acquired Neurogenic Communication Disorders: Continuing the Evidence Dialogue with a Survey of Current Practices in Speech-Language Pathology. Healthcare. 2022; 10(6):1010. https://doi.org/10.3390/healthcare10061010
Chicago/Turabian StyleBehaghel, Estelle, and Anna Zumbansen. 2022. "Singing for the Rehabilitation of Acquired Neurogenic Communication Disorders: Continuing the Evidence Dialogue with a Survey of Current Practices in Speech-Language Pathology" Healthcare 10, no. 6: 1010. https://doi.org/10.3390/healthcare10061010
APA StyleBehaghel, E., & Zumbansen, A. (2022). Singing for the Rehabilitation of Acquired Neurogenic Communication Disorders: Continuing the Evidence Dialogue with a Survey of Current Practices in Speech-Language Pathology. Healthcare, 10(6), 1010. https://doi.org/10.3390/healthcare10061010