
Gender Risk Perception and Coping Mechanisms among Ghanaian University Students during the COVID-19 Pandemic

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context and Sample Characteristics
2.2. Study Measures
2.2.1. Risk Perception
2.2.2. Coping Mechanism
2.3. Procedure
2.4. Data Analyses
3. Results
3.1. Preliminary Analyses on Risk Perception, Coping Mechanisms, and Gender
3.2. Influence of COVID-19 Risk Perception on Coping Mechanism
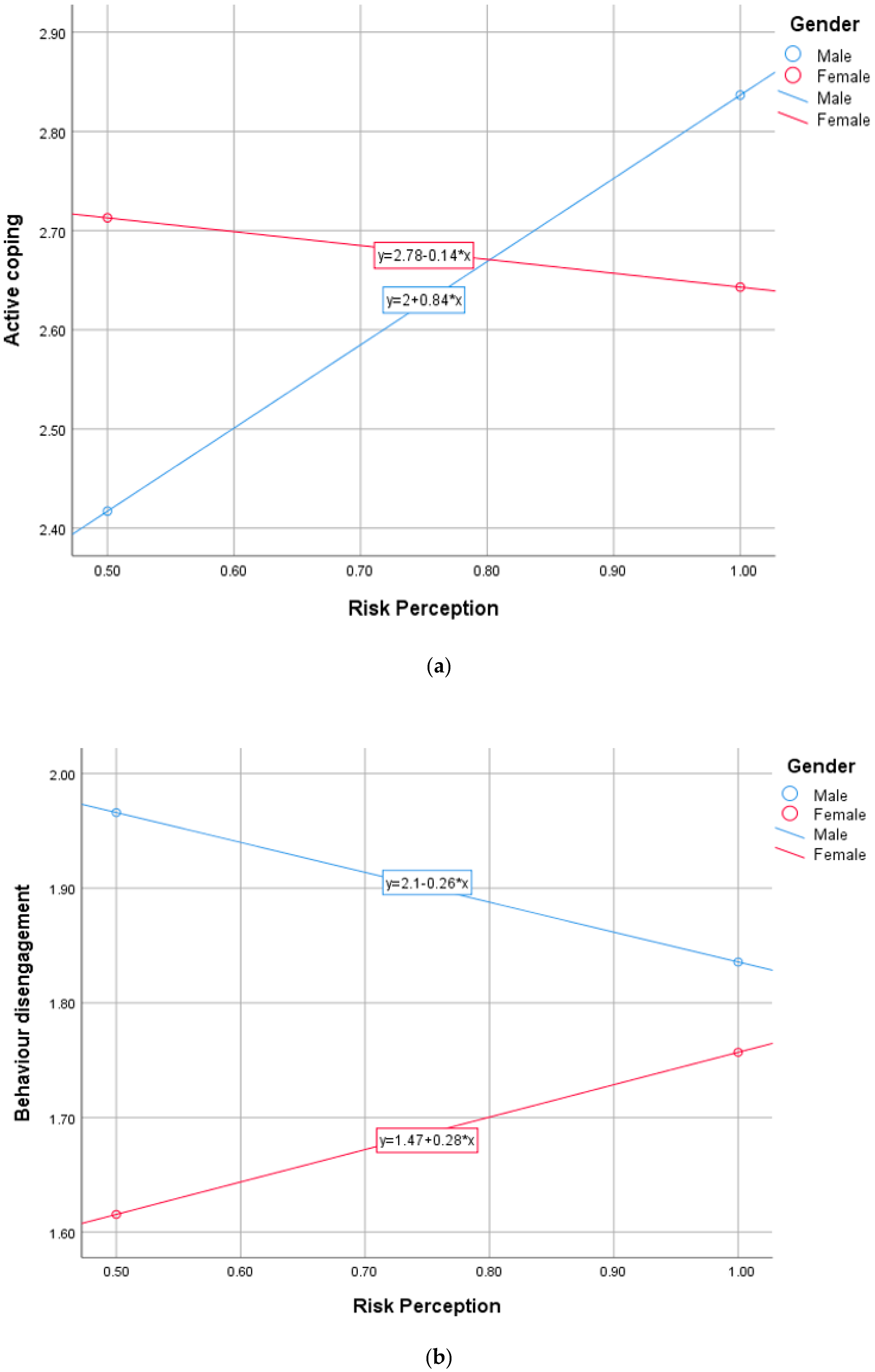
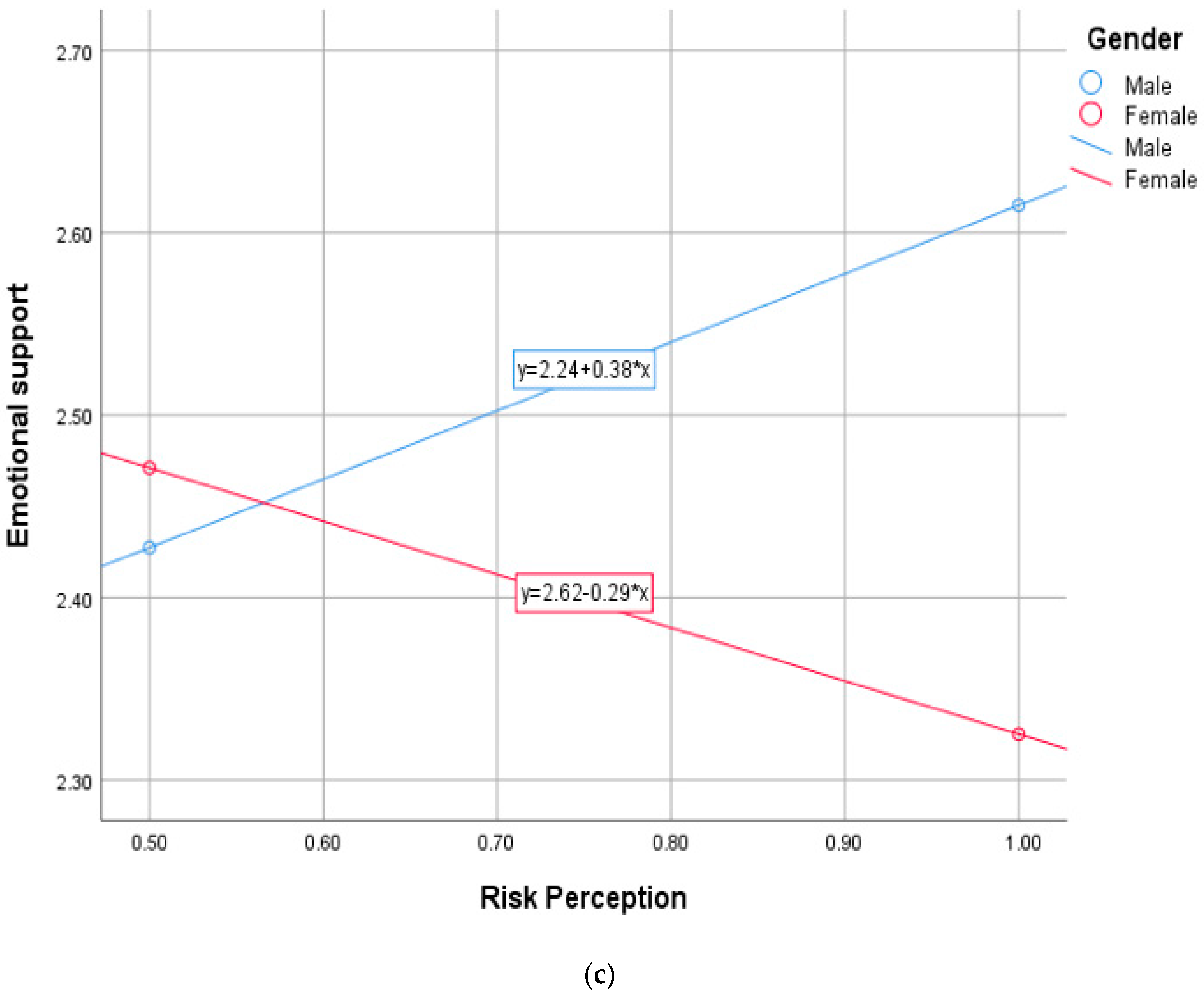
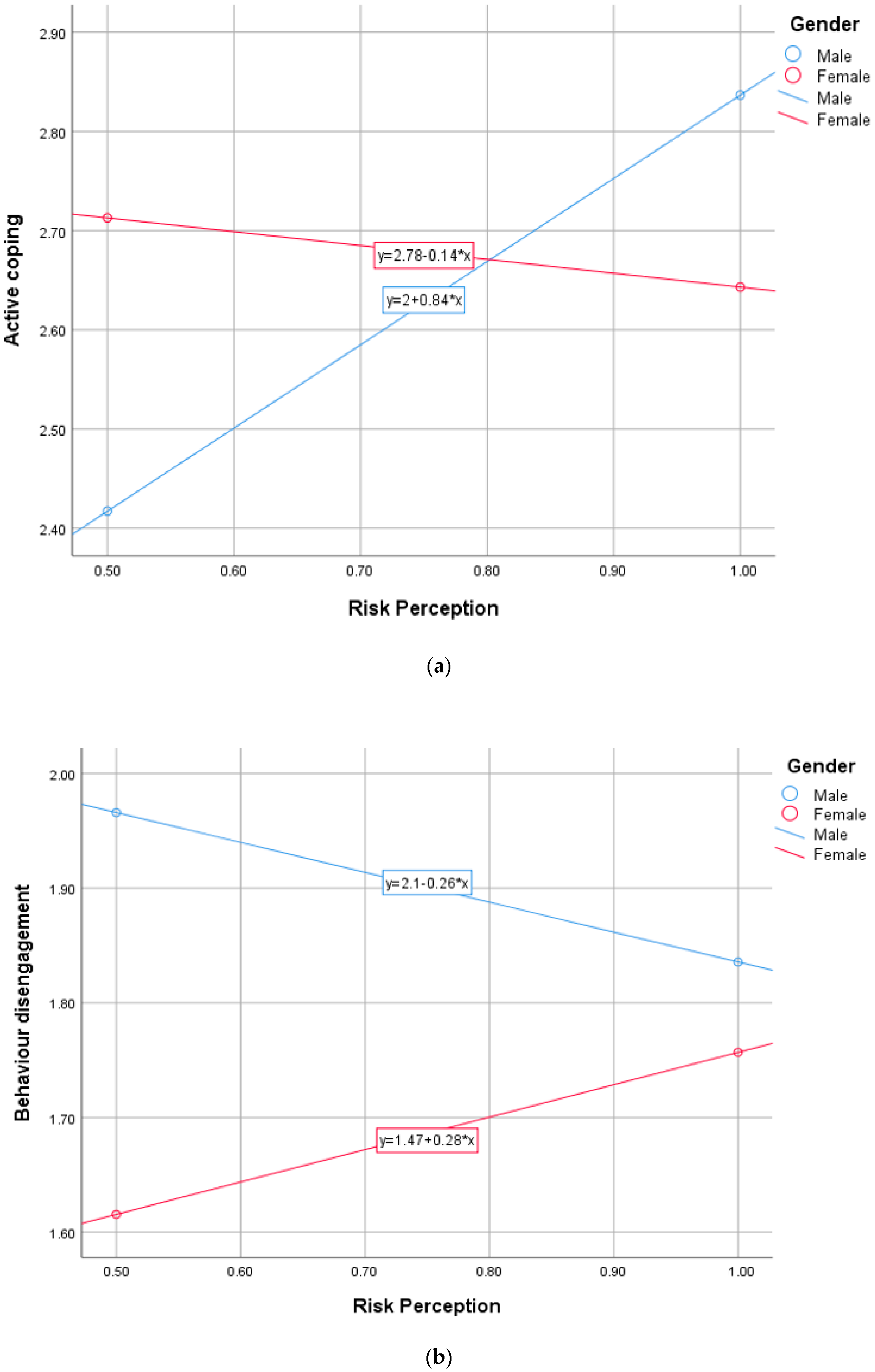
3.3. The Role of Gender in the Relationship between COVID-19 Risk Perception and Coping Mechanism
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 7 February 2022).
- World Health Organization. Ghana’s Situation of COVID-19. 2022. Available online: https://covid19.who.int/region/afro/country/gh (accessed on 7 February 2022).
- Yıldırım, M.; Arslan, G.; Wong, P.T. Meaningful living, resilience, affective balance, and psychological health problems among Turkish young adults during coronavirus pandemic. Curr. Psychol. 2021, 1–12. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Wang, Y.; Xue, J.; Zhao, N.; Zhu, T. The impact of COVID-19 epidemic declaration on psychological consequences: A study on active Weibo users. Int. J. Environ. Res. Public Health 2020, 17, 2032. [Google Scholar] [CrossRef] [Green Version]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2020, 368, m313. [Google Scholar] [CrossRef] [Green Version]
- Sjoberg, L. Factors in risk perception. Risk Anal. 2000, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Güler, A. Factor analysis of the COVID-19 Perceived Risk Scale: A preliminary study. Death Stud. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Geçer, E.; Akgül, Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol. Health Med. 2020, 26, 35–43. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; Chan, H.H.H.; Yi, Y.Y.; Tang, A.; Wei, W.I.; Wong, S.Y.S. Community Responses during Early Phase of COVID-19 Epidemic, Hong Kong. Emerg. Infect. Dis. 2020, 26, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, M.; Güler, A. Positivity explains how COVID-19 perceived risk increases death distress and reduces happiness. Personal. Individ. Differ. 2021, 168, 110347. [Google Scholar] [CrossRef]
- Yıldırım, M.; Arslan, G.; Özaslan, A. Perceived Risk and Mental Health Problems among Healthcare Professionals during COVID-19 Pandemic: Exploring the Mediating Effects of Resilience and Coronavirus Fear. Int. J. Ment. Health Addict. 2020, 20, 1035–1045. [Google Scholar] [CrossRef]
- Capone, V.; Caso, D.; Donizzetti, A.; Procentese, F. University Student Mental Well-Being during COVID-19 Outbreak: What Are the Relationships between Information Seeking, Perceived Risk and Personal Resources Related to the Academic Context? Sustainability 2020, 12, 7039. [Google Scholar] [CrossRef]
- Gerhold, L. COVID-19: Risk perception and coping strategies. PsyArXiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Quansah, F.; Hagan, J.E.; Sambah, F.; Frimpong, J.B.; Ankomah, F.; Srem-Sai, M.; Seibu, M.; Abieraba, R.S.K.; Schack, T. Perceived Safety of Learning Environment and Associated Anxiety Factors during COVID-19 in Ghana: Evidence from Physical Education Practical-Oriented Program. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Aktekin, M.; Karaman, T.; Senol, Y.Y.; Erdem, S.; Erengin, H.; Akaydin, M. Anxiety, depression and stressful life events among medical students: A prospective study in Antalya, Turkey. Med. Educ. 2001, 35, 12–17. [Google Scholar] [CrossRef]
- Zivin, K.; Eisenberg, D.; Gollust, S.E.; Golberstein, E. Persistence of mental health problems and needs in a college student population. J. Affect. Disord. 2009, 117, 180–185. [Google Scholar] [CrossRef]
- American College Health Association. American College Health Association National College Health Assessment II: Reference Group Executive Summary Fall 2017; American College Health Association: Hanover, MD, USA, 2018. [Google Scholar]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef] [PubMed]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef] [PubMed]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A Meta-Analysis of Research on Protection Motivation Theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Sutton, S. Fear-arousing communications: A critical examination of theory and research. In Social Psychology and Behavioral Medicine; Eiser, J., Ed.; John Wiley & Sons: Hoboken, NJ, USA, 1982; pp. 303–337. [Google Scholar]
- Wise, T.; Zbozinek, T.D.; Michelini, G.; Hagan, C.C.; Mobbs, D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R. Soc. Open Sci. 2020, 7, 200742. [Google Scholar] [CrossRef] [PubMed]
- Leppin, A.; Aro, A.R. Risk perceptions related to SARS and Avian Influenza: Theoretical foundations of current empirical research. Int. J. Behav. Med. 2009, 16, 7–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir. Med. 2020, 8, e20. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Caramelo, F.; Ferreira, N.; Oliveiros, B. Estimation of risk factors for COVID-19 mortality-preliminary results. MedRxiv 2020, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Rana, I.A.; Bhatti, S.S.; Aslam, A.B.; Jamshed, A.; Ahmad, J.; Shah, A.A. COVID-19 risk perception and coping mechanisms: Does gender make a difference? Int. J. Disaster Risk Reduct. 2021, 55, 102096. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Alsharawy, A.; Spoon, R.; Smith, A.; Ball, S. Gender Differences in Fear and Risk Perception During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 689467. [Google Scholar] [CrossRef] [PubMed]
- Burns, W.J.; Slovic, P. Risk Perception and Behaviors: Anticipating and Responding to Crises. Risk Anal. 2012, 32, 579–582. [Google Scholar] [CrossRef] [PubMed]
- Quansah, F.; Hagan, J.E.J.; Ankomah, F.; Srem-Sai, M.; Frimpong, J.B.; Sambah, F.; Schack, T. Relationship Between COVID-19 Related Knowledge and Anxiety Among University Students: Exploring the Moderating Roles of School Climate and Coping Strategies. Front. Psychol. 2022, 13, 820288. [Google Scholar] [CrossRef]
- Capone, V.; Donizzetti, A.R.; Park, M.S.-A. Validation and Psychometric Evaluation of the COVID-19 Risk Perception Scale (CoRP): A New Brief Scale to Measure Individuals’ Risk Perception. Int. J. Ment. Health Addict. 2021, 1–14. [Google Scholar] [CrossRef]
- Anselmi, P.; Colledani, D.; Robusto, E. A Comparison of Classical and Modern Measures of Internal Consistency. Front. Psychol. 2019, 10, 2714. [Google Scholar] [CrossRef] [PubMed]
- Quansah, F. The Use of Cronbach Alpha Reliability Estimate in Research Among Students in Public Universities in Ghana. Afr. J. Teach. Educ. 2017, 6, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Pallant, J. SPSS Survival Manual. A Step by Step Guide to Data Analysis Using IBM SPSS, 7th ed.; Routledge: London, UK, 2020. [Google Scholar]
- Quansah, F.; Ankomah, F.; Hagan, J.E.; Srem-Sai, M.; Frimpong, J.B.; Sambah, F.; Schack, T. Development and Validation of an Inventory for Stressful Situations in University Students Involving Coping Mechanisms: An Interesting Cultural Mix in Ghana. Psych 2022, 4, 173–186. [Google Scholar] [CrossRef]
- Hill, Y.; Hartigh, R.J.R.D.; Meijer, R.R.; De Jonge, P.; Van Yperen, N.W. Resilience in sports from a dynamical perspective. Sport Exerc. Perform. Psychol. 2018, 7, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Paredes, M.R.; Apaolaza, V.; Fernandez-Robin, C.; Hartmann, P.; Yañez-Martinez, D. The impact of the COVID-19 pandemic on subjective mental well-being: The interplay of perceived threat, future anxiety and resilience. Pers. Individ. Differ. 2020, 170, 110455. [Google Scholar] [CrossRef]
- Maiorano, T.; Vagni, M.; Giostra, V.; Pajardi, D. COVID-19: Risk Factors and Protective Role of Resilience and Coping Strategies for Emergency Stress and Secondary Trauma in Medical Staff and Emergency Workers—An Online-Based Inquiry. Sustainability 2020, 12, 9004. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| No. | Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| 1 | Risk perception | 1 | ||||
| 2 | Active coping | 0.173 ** | 1 | |||
| 3 | Religious coping | 0.053 | 0.406 ** | 1 | ||
| 4 | Behaviour disengagement | −0.021 | 0.143 ** | 0.204 ** | 1 | |
| 5 | Emotional support | 0.074 * | 0.410 ** | 0.339 ** | 0.325 ** | 1 |
| 6 | Gender *** | −0.125 ** | 0.035 | 0.078* | −0.138 ** | −0.063 |
| - | Mean | 0.733 | 2.641 | 2.790 | 1.843 | 2.50 |
| - | SD | 0.228 | 0.755 | 0.860 | 0.733 | 0.711 |
| Criterion Variable | Parameters | B | Std. Error | t | p | f2 |
|---|---|---|---|---|---|---|
| Active coping | Intercept | 2.222 | 0.086 | 25.970 | 0.000 | 0.031 |
| Risk perception | 0.573 | 0.111 | 5.138 | 0.000 * | ||
| Religious coping | Intercept | 2.645 | 0.099 | 26.763 | 0.000 | 0.003 |
| Risk perception | 0.198 | 0.129 | 1.541 | 0.124 | ||
| Behaviour disengagement | Intercept | 1.893 | 0.084 | 22.460 | 0.000 | 0 |
| Risk perception | −0.069 | 0.110 | −0.628 | 0.530 | ||
| Emotional support | Intercept | 2.326 | 0.082 | 28.491 | 0.000 | 0.005 |
| Risk perception | 0.231 | 0.106 | 2.174 | 0.030 |
| Models | B | SE | t | LLCI | ULCI | f2 | |
|---|---|---|---|---|---|---|---|
| 1 | Constant | 1.998 | 0.101 | 19.877 | 1.800 | 2.195 | 0.175 |
| Risk perception (RP) | 0.839 | 0.128 | 6.535 | 0.587 | 1.091 | ||
| W1 | 0.785 | 0.190 | 4.137 | 0.413 | 1.158 | ||
| RP*W1 | −0.979 | 0.258 | −3.795 | −1.485 | −0.473 | ||
| 2 | Constant | 2.489 | 0.117 | 21.333 | 2.260 | 2.718 | 0.013 |
| Risk perception (RP) | 0.350 | 0.149 | 2.351 | 0.058 | 0.643 | ||
| W1 | 0.486 | 0.220 | 2.203 | 0.053 | 0.918 | ||
| RP*W1 | −0.451 | 0.400 | −1.506 | −1.039 | 0.137 | ||
| 3 | constant | 2.096 | 0.099 | 21.235 | 1.903 | 2.290 | 0.144 |
| Risk perception (RP) | −0.261 | 0.126 | −2.069 | −0.509 | −0.013 | ||
| W1 | −0.623 | 0.187 | −3.338 | −0.989 | −0.256 | ||
| RP*W1 | 0.544 | 0.253 | 2.146 | 0.046 | 1.041 | ||
| 4 | Constant | 2.240 | 0.096 | 23.259 | 2.051 | 2.429 | 0.202 |
| Risk perception (RP) | 0.375 | 0.123 | 3.051 | 0.134 | 0.617 | ||
| W1 | 0.378 | 0.182 | 2.076 | 0.021 | 0.735 | ||
| RP*W1 | −0.668 | 0.247 | −2.701 | −1.153 | −0.182 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagan, J.E., Jr.; Quansah, F.; Frimpong, J.B.; Ankomah, F.; Srem-Sai, M.; Schack, T. Gender Risk Perception and Coping Mechanisms among Ghanaian University Students during the COVID-19 Pandemic. Healthcare 2022, 10, 687. https://doi.org/10.3390/healthcare10040687
Hagan JE Jr., Quansah F, Frimpong JB, Ankomah F, Srem-Sai M, Schack T. Gender Risk Perception and Coping Mechanisms among Ghanaian University Students during the COVID-19 Pandemic. Healthcare. 2022; 10(4):687. https://doi.org/10.3390/healthcare10040687
Chicago/Turabian StyleHagan, John Elvis, Jr., Frank Quansah, James Boadu Frimpong, Francis Ankomah, Medina Srem-Sai, and Thomas Schack. 2022. "Gender Risk Perception and Coping Mechanisms among Ghanaian University Students during the COVID-19 Pandemic" Healthcare 10, no. 4: 687. https://doi.org/10.3390/healthcare10040687
APA StyleHagan, J. E., Jr., Quansah, F., Frimpong, J. B., Ankomah, F., Srem-Sai, M., & Schack, T. (2022). Gender Risk Perception and Coping Mechanisms among Ghanaian University Students during the COVID-19 Pandemic. Healthcare, 10(4), 687. https://doi.org/10.3390/healthcare10040687