
Same Pandemic Yet Different COVID-19 Vaccination Roll-Out Rates in Two Small European Islands: A Comparison between Cyprus and Malta

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
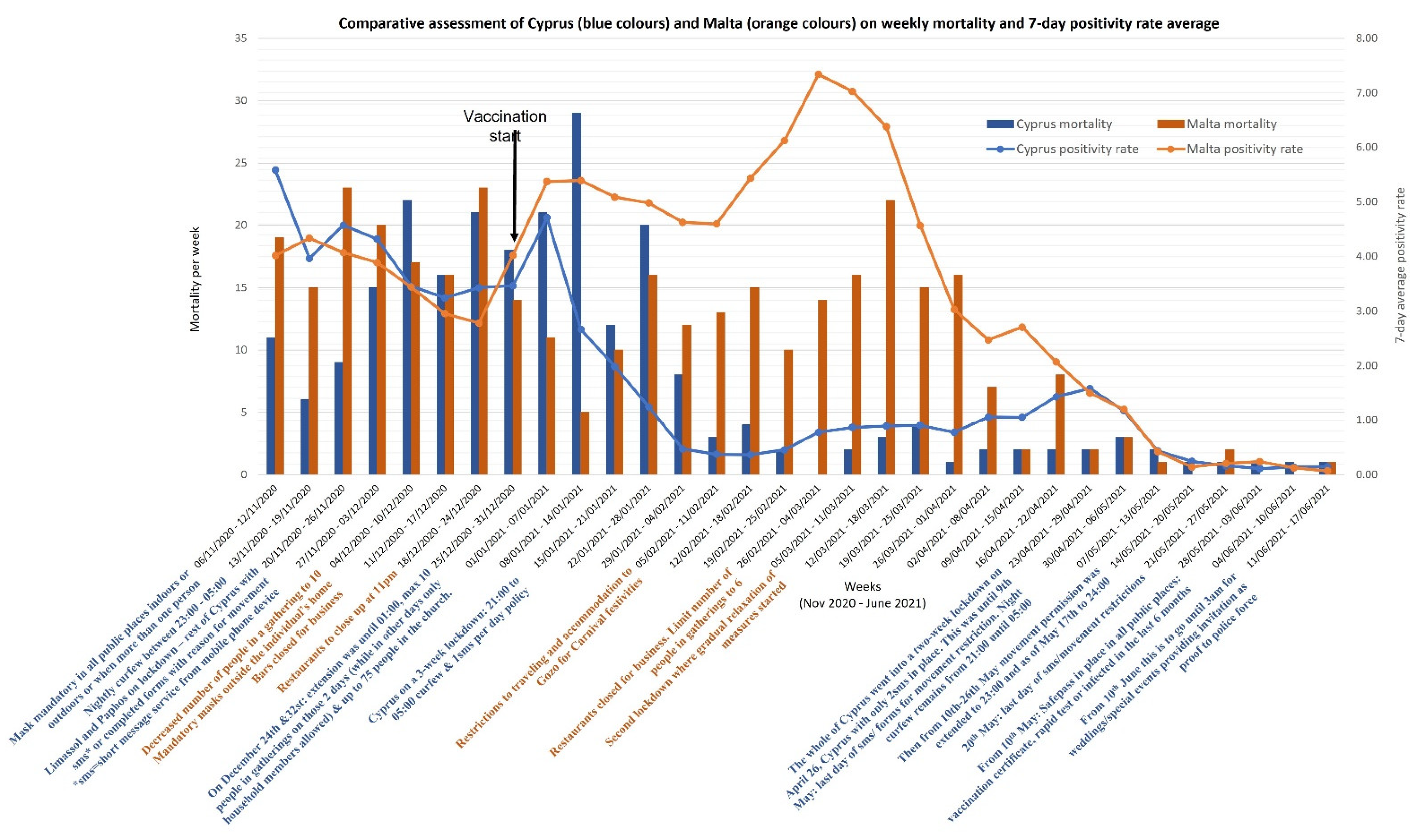
3.1. The COVID-19 Situation
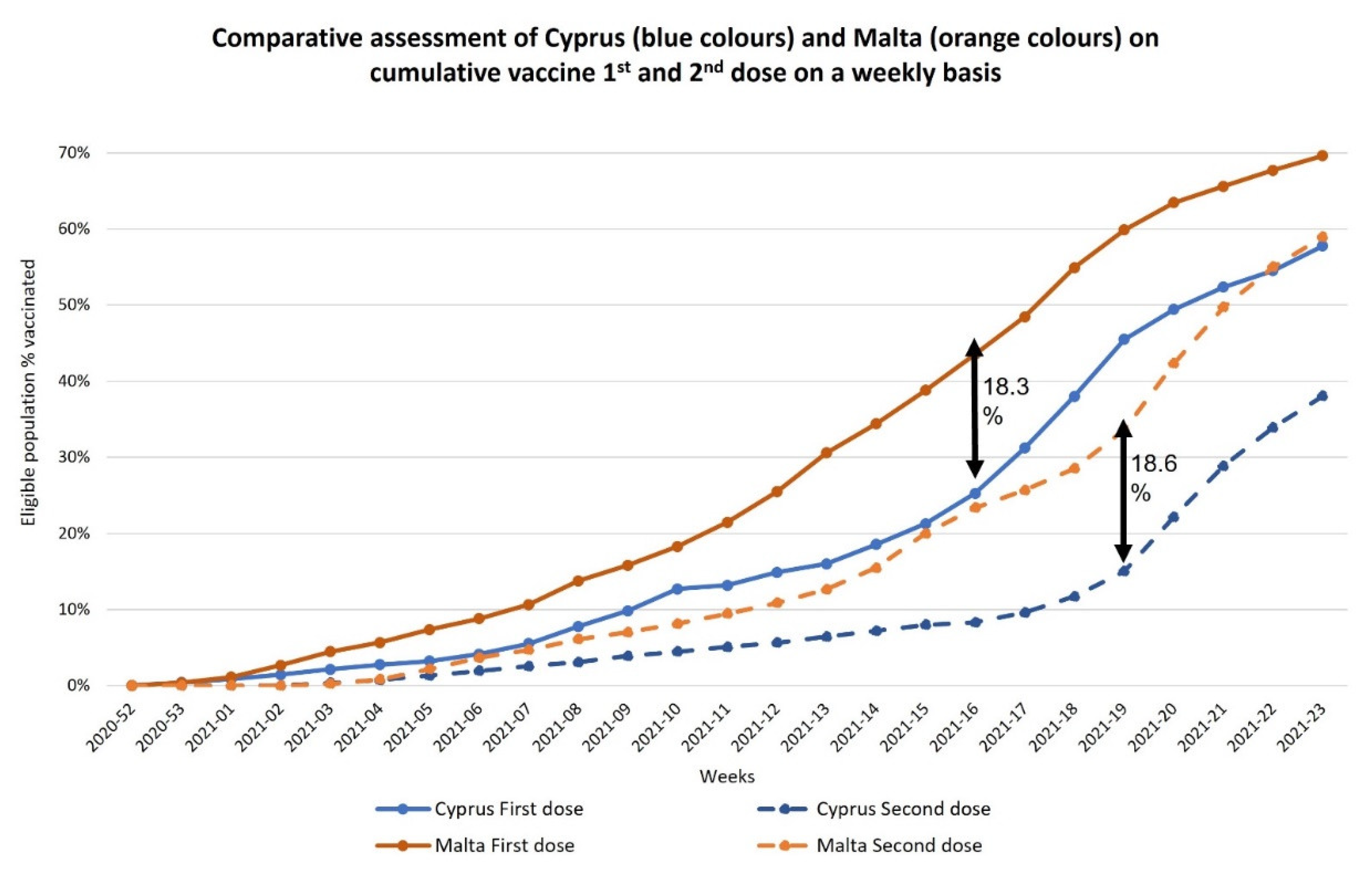
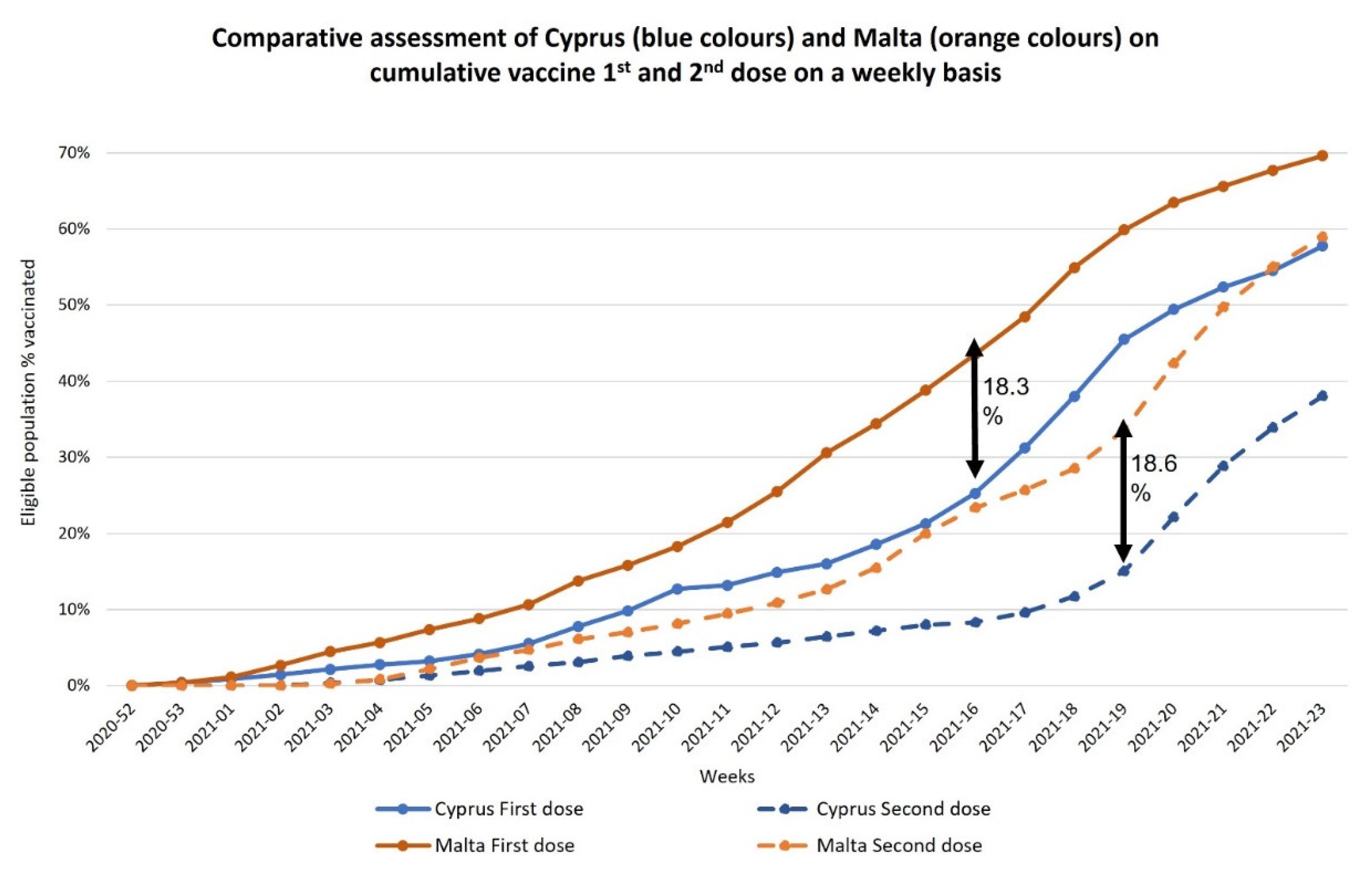
3.2. COVID-19 Vaccines
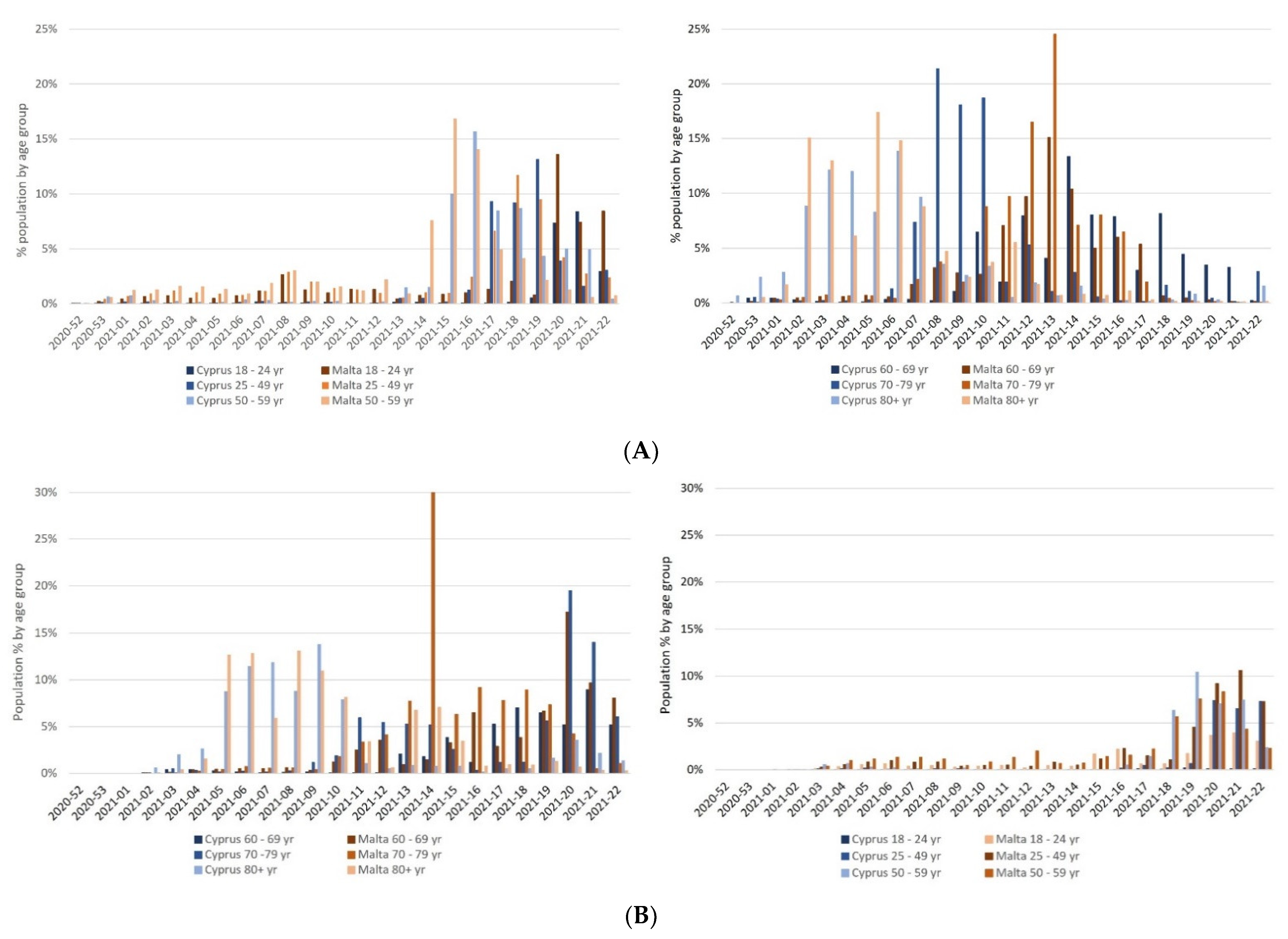
3.3. COVID-19 Vaccination Roll-Out Strategies
3.4. Vaccination Infrastructure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Medical Agency. EMA Recommends First COVID-19 Vaccine for Authorisation in the EU. EMA News. 2020. Available online: https://www.ema.europa.eu/en/news/ema-recommends-first-COVID-19-vaccine-authorisation-eu (accessed on 11 May 2021).
- European Medical Agency. COVID-19 Vaccines: Authorised. COVID-19. 2021. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-COVID-19/treatments-vaccines/vaccines-COVID-19/COVID-19-vaccines-authorised (accessed on 11 May 2021).
- Mills, M.C.; Salisbury, D. The challenges of distributing COVID-19 vaccinations. EclinicalMedicine 2021, 31, 100674. [Google Scholar] [CrossRef] [PubMed]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA 2020, 323, 2458. [Google Scholar] [CrossRef] [PubMed]
- Harris, C. COVID Vaccine: Who in Europe is Leading the Race to Herd Immunity? Euronews. 2021. Available online: https://www.euronews.com/2021/05/10/COVID-19-vaccinations-in-europe-which-countries-are-leading-the-way (accessed on 11 May 2021).
- Wang, J.; Peng, Y.; Xu, H.; Cui, Z.; Williams, R.O. The COVID-19 Vaccine Race: Challenges and Opportunities in Vaccine Formulation. AAPS PharmSciTech 2020, 21, 225. [Google Scholar] [CrossRef] [PubMed]
- Hogenauer, A.-L.; Sarapuu, K.; Trimikliniotis, N. Small states and the governance of the COVID-19 pandemic. Small States Territ. 2021, 4, 3–12. Available online: https://www.um.edu.mt/library/oar/handle/123456789/74992 (accessed on 5 June 2021).
- Cuschieri, S.; Pallari, E.; Hatziyianni, A.; Sigurvinsdottir, R.; Sigfusdottir, I.D.; Sigurðardóttir, Á.K. Mortality comparisons of COVID-19 with all-cause and non-communicable diseases in Cyprus, Iceland and Malta: Lessons learned and forward planning. Public Health 2021, 202, 52–57. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. COVID-19 Vaccine Rollout Overview; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2021; Available online: https://covid19-vaccine-report.ecdc.europa.eu/#Key_figures_on_the_vaccine_rollout_in_the_EUEEA_as_of_week_16,_2021_(25_April_2021) (accessed on 5 June 2021).
- Ministry of Health Cyprus. Answers to Frequently Asked Questions about Vaccines/Vaccination Against COVID-19 Disease. 2021. Available online: https://www.pio.gov.cy/coronavirus/uploads/15122020_answers.pdf (accessed on 7 July 2021).
- COVID-19 Public Health Response Team—Ministry for Health. COVID-19 Data Management System. 2021. Available online: https://deputyprimeminister.gov.mt/en/health-promotion/COVID-19/Pages/COVID-19-infographics.aspx (accessed on 5 June 2021).
- University of Cyprus. COVID-19 Spread in Cyprus. University of Cyprus Research and Innovation Center of Excellence. 2021. Available online: https://covid19.ucy.ac.cy/ (accessed on 1 April 2021).
- European Centre for Disease Prevention and Control. COVID-19 Situation Update for the EU/EEA; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2021; Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 5 June 2021).
- European Center for Disease Prevention and Control. Interpretation of Data. 2021. Available online: https://www.ecdc.europa.eu/en/COVID-19/data-collection (accessed on 26 July 2021).
- World Health Organization (WHO). Estimating Mortality from COVID-19: Scientific Brief, 4 August 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- European Commission. EU Vaccines Strategy. Public Health. 2021. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/public-health/eu-vaccines-strategy_en (accessed on 5 June 2021).
- Τύπου, Δ. ΚΥΠΡΙAΚH ΔHΜOΚΡAΤΙA ΥΠOΥΡΓΕΙO ΥΓΕΙAΣ. Available online: https://www.pio.gov.cy/coronavirus/uploads/26122020--ΠαραλήφθηκεηπρώτηπαρτίδαεμβολίωνγιατηνCOVID-19.pdf (accessed on 26 July 2021).
- Ministry of Health Malta. Vaccines; Ministry of Health Malta: Valletta, Malta, 2021. Available online: https://deputyprimeminister.gov.mt/en/health-promotion/COVID-19/Pages/vaccines.aspx (accessed on 26 July 2021).
- Sansone, K. COVID-19 Herd Immunity Target to Be Reached on 19 May. Malta Today. 2021. Available online: https://www.maltatoday.com.mt/news/national/109565/covid19_herd_immunity_target_to_be_reached_on_19_may_#.YJ0ggC8Rocg (accessed on 13 May 2021).
- Bonnici, J. COVID-19 Vaccine Registration Opens to 12 to 15-Year-Olds in Malta. Lovin Malta. 2021. Available online: https://lovinmalta.com/lifestyle/health/COVID-19/COVID-19-vaccine-registration-opens-to-12-to-15-year-olds-in-malta/ (accessed on 6 July 2021).
- Press and Information Office—Cyprus. The Effort to Increase the Vaccination Coverage Continues—The Target for the Vaccination of 65% of the Population with the 1st Dose Has Been Achieved; Press and Information Office: Nicosia, Cyprus, 2021. Available online: https://www.pio.gov.cy/en/press-releases-article.html?id=21295#flat (accessed on 26 July 2021).
- Farrugia, C. Meet the Volunteers Giving Their Time to Malta’s Vaccine Drive. Times of Malta. 2021. Available online: https://timesofmalta.com/articles/view/meet-the-volunteers-giving-their-time-to-maltas-vaccine-drive.867451 (accessed on 8 May 2021).
- University of Malta. UM Staff and Students Step Up to the Frontline by Helping with National COVID-19 Vaccine Roll-Out—Newspoint—University of Malta; Newspoint—University of Malta: Msida, Malta, 2021; Available online: https://www.um.edu.mt/newspoint/news/2021/02/students-frontline-covid (accessed on 8 May 2021).
- Times of Malta. Mobile COVID-19 Vaccination Clinic to Be Set Up. Times of Malta. 2021. Available online: https://timesofmalta.com/articles/view/mobile-COVID-19-vaccination-clinic-set-up.886234?utm_source=tom&utm_campaign=newsletter&utm_medium=email&utm_content=2021-07-13 (accessed on 26 July 2021).
- Ministry of Health. The Access of Citizens to Vaccination Is Facilitated through the Walk-In Centres; Ministry of Health: Nicosia, Cyprus, 2021. Available online: https://www.pio.gov.cy/coronavirus/uploads/14072021_walk-invaccinationcentresEN.pdf (accessed on 26 July 2021).
- Sanche, S.; Lin, Y.T.; Xu, C.; Romero-Severson, E.; Hengartner, N.; Ke, R. High Contagiousness and Rapid Spread of Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2020, 26, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. Delta coronavirus variant: Scientists brace for impact. Nature 2021, 595, 17–18. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Public Opinion on COVID-19 Vaccination in the EU. 2020. Available online: https://ec.europa.eu/info/sites/default/files/COVID-19_vaccination_in_the_eu_desk_research_eurobarometer.pdf (accessed on 26 July 2021).
- Cuschieri, S.; Grech, V. A comparative assessment of attitudes and hesitancy for influenza vis-à-vis COVID-19 vaccination among healthcare students and professionals in Malta. Z. Gesundh. J. Public Health 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- The Economic Times. Countries Halting AstraZeneca Vaccine. The Economic Times. 2021. Available online: https://economictimes.indiatimes.com/news/international/world-news/countries-halting-astrazeneca-vaccine/articleshow/81525013.cms?from=mdr (accessed on 8 May 2021).
- Diacono, T. Six Secrets to Success: How Malta Became One of the World’s Best COVID-19 Vaccinators. Lovin Malta. 2021. Available online: https://lovinmalta.com/opinion/analysis/six-secrets-to-success-how-malta-became-one-of-the-worlds-best-COVID-19-vaccinators/ (accessed on 8 May 2021).
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Teslya, A.; Rozhnova, G.; Pham, T.M.; van Wees, D.; Nunner, H.; Godijk, N.; Bootsma, M.; Kretzschmar, M. The importance of sustained compliance with physical distancing during COVID-19 vaccination rollout. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Gozzi, N.; Bajardi, P.; Perra, N. The importance of non-pharmaceutical interventions during the COVID-19 vaccine rollout. medRxiv 2021. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Cyprus | Malta | Cyprus | Malta | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 1st Dose | 1st Dose | Fully Vaccinated | Fully Vaccinated | ||||||
| N | %* | N | %* | N | %* | N | %* | ||
| 18–24 years | Pfizer | 12,878 | 15.18% | 14,749 | 35.00% | 376 | 0.44% | 5513 | 13.08% |
| Moderna | 3477 | 4.10% | 2177 | 5.17% | 44 | 0.05% | 158 | 0.37% | |
| AZ | 1153 | 1.36% | 3747 | 8.89% | 317 | 0.37% | 3609 | 8.57% | |
| J&J | 26 | 0.03% | 53 | 0.13% | |||||
| Total | 17,508 | 20.63% | 20,673 | 49.06% | 763 | 0.90% | 9333 | 22.15% | |
| 25–49 years | Pfizer | 89,889 | 27.21% | 80,926 | 39.45% | 71,277 | 21.58% | 68,505 | 33.39% |
| Moderna | 16,334 | 4.95% | 7756 | 3.78% | 3227 | 0.98% | 2125 | 1.04% | |
| AZ | 34,304 | 10.39% | 30,826 | 15.03% | 2799 | 0.85% | 21,455 | 10.46% | |
| J&J | 5211 | 1.58% | 170 | 0.08% | |||||
| Total | 140,527 | 42.55% | 119,508 | 58.25% | 82,514 | 24.98% | 92,255 | 44.97% | |
| 50–59 years | Pfizer | 43,972 | 40.85% | 20,942 | 35.39% | 38,122 | 35.42% | 20,812 | 35.17% |
| Moderna | 5215 | 4.85% | 1433 | 2.42% | 954 | 0.89% | 557 | 0.94% | |
| AZ | 19,743 | 18.34% | 20,960 | 35.42% | 1434 | 1.33% | 5644 | 9.54% | |
| J&J | 37 | 0.03% | 26 | 0.04% | |||||
| Total | 68,930 | 64.04% | 43,335 | 73.24% | 40,547 | 37.67% | 27,039 | 45.70% | |
| 60–69 years | Pfizer | 35,071 | 37.03% | 18,503 | 31.07% | 31,378 | 33.13% | 19,306 | 32.42% |
| Moderna | 6378 | 6.73% | 2876 | 4.83% | 4268 | 4.51% | 4560 | 7.66% | |
| AZ | 30,048 | 31.72% | 22,861 | 38.39% | 10,503 | 11.09% | 18,311 | 30.75% | |
| J&J | 285 | 0.30% | 5 | 0.01% | |||||
| Total | 71,497 | 75.49% | 44,240 | 74.29% | 46,434 | 49.03% | 42,182 | 70.83% | |
| 70–79 years | Pfizer | 20,878 | 31.43% | 36,209 | 80.61% | 18,729 | 28.19% | 36,847 | 82.03% |
| Moderna | 3427 | 5.16% | 4828 | 10.75% | 3364 | 5.06% | 5517 | 12.28% | |
| AZ | 33,305 | 50.14% | 1673 | 3.72% | 29,020 | 43.69% | 485 | 1.08% | |
| J&J | 47 | 0.07% | 3 | 0.01% | |||||
| Total | 57,610 | 86.72% | 42,710 | 95.08% | 51,160 | 77.01% | 42,852 | 95.40% | |
| 80+ years | Pfizer | 24,479 | 73.01% | 21,543 | 99.33% | 23,629 | 70.47% | 19,797 | 91.28% |
| Moderna | 824 | 2.46% | 42 | 0.19% | 808 | 2.41% | 53 | 0.24% | |
| AZ | 4307 | 12.85% | 34 | 0.16% | 2832 | 8.45% | 56 | 0.26% | |
| J&J | 2 | 0.01% | 1 | 0.00% | |||||
| Total | 29,610 | 88.31% | 21,619 | 99.68% | 27,271 | 81.33% | 19,907 | 91.78% | |
| Priority Groups Schedule | ||
|---|---|---|
| Initiation of Vaccination Appointments | Cyprus | Malta |
| 27 December 2020 | Healthcare workers | Healthcare workers and long-term care facility |
| 11 January 2021 | Persons living in long-term care facilities—elderly and mental health, and 85+ years | |
| 27 January 2021 | 88+ years | |
| 29 January 2021 | 86+ years | |
| 1 February 2021 | 84+ years | All other frontliners and 80–85 years |
| 3 February 2021 | 83+ years | |
| 8 February 2021 | Vulnerable population * | |
| 9 February 2021 | 75–79 years | |
| 17 February 2021 | 74+ years | |
| 23 February 2021 | 71+ years | |
| 24 February 2021 | Staff at schools and child-care centers | |
| 1 March 2021 | 70–80 years | |
| 3 March 2021 | 69+ years | |
| 6 March 2021 | 60+ years | |
| 9 March 2021 | 67+ years | |
| 20 March 2021 | 66+ years | |
| 29 March 2021 | Diabetes and Obese | |
| 1 April 2021 | 64+ years | |
| 7 April 2021 | 61–63 years | |
| 9 April 2021 | 59–60 years | |
| 10 April 2021 | 57–58 years | 50+ years |
| 11 April 2021 | Specific vulnerable groups | |
| 13 April 2021 | 55–56 years | |
| 16April 2021 | 53–54 years | |
| 19 April 2021 | Bedridden patients | |
| 21 April 2021 | 51–52 years | |
| 23 April 2021 | 40+ years | |
| 26 April 2021 | 43–44 years | |
| 27 April 2021 | 42 years | |
| 28 April 2021 | 41 years | |
| 29 April 2021 | 39–40 years | |
| 4 May 2021 | 37–38 years | |
| 5 May 2021 | 30 + years | |
| 6 May 2021 | 35–36 years | |
| 7 May 2021 | 33–34 years | |
| 9 May 2021 | 31–32 years | |
| 10 May 2021 | 29–30 years | |
| 11 May 2021 | 27–28 years | |
| 12 May 2021 | 25–26 years | |
| 19 May 2021 | 16+ years | |
| 7 June 2021 | 23–27 years | |
| 9 June 2021 | 18–22 years | |
| 16 June 2021 | 12+ years | |
| 18 June 2021 | 18+ years | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuschieri, S.; Hatziyianni, A.; Kantaris, M.; Kontemeniotis, A.; Theodorou, M.; Pallari, E. Same Pandemic Yet Different COVID-19 Vaccination Roll-Out Rates in Two Small European Islands: A Comparison between Cyprus and Malta. Healthcare 2022, 10, 222. https://doi.org/10.3390/healthcare10020222
Cuschieri S, Hatziyianni A, Kantaris M, Kontemeniotis A, Theodorou M, Pallari E. Same Pandemic Yet Different COVID-19 Vaccination Roll-Out Rates in Two Small European Islands: A Comparison between Cyprus and Malta. Healthcare. 2022; 10(2):222. https://doi.org/10.3390/healthcare10020222
Chicago/Turabian StyleCuschieri, Sarah, Amalia Hatziyianni, Marios Kantaris, Antonis Kontemeniotis, Mamas Theodorou, and Elena Pallari. 2022. "Same Pandemic Yet Different COVID-19 Vaccination Roll-Out Rates in Two Small European Islands: A Comparison between Cyprus and Malta" Healthcare 10, no. 2: 222. https://doi.org/10.3390/healthcare10020222
APA StyleCuschieri, S., Hatziyianni, A., Kantaris, M., Kontemeniotis, A., Theodorou, M., & Pallari, E. (2022). Same Pandemic Yet Different COVID-19 Vaccination Roll-Out Rates in Two Small European Islands: A Comparison between Cyprus and Malta. Healthcare, 10(2), 222. https://doi.org/10.3390/healthcare10020222