

Heterogeneity in Response to MCT and Psychoeducation: A Feasibility Study Using Latent Class Mixed Models in First-Episode Psychosis

 , , , , , , , , , , , , ,
, , , , , , , , , , , , , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
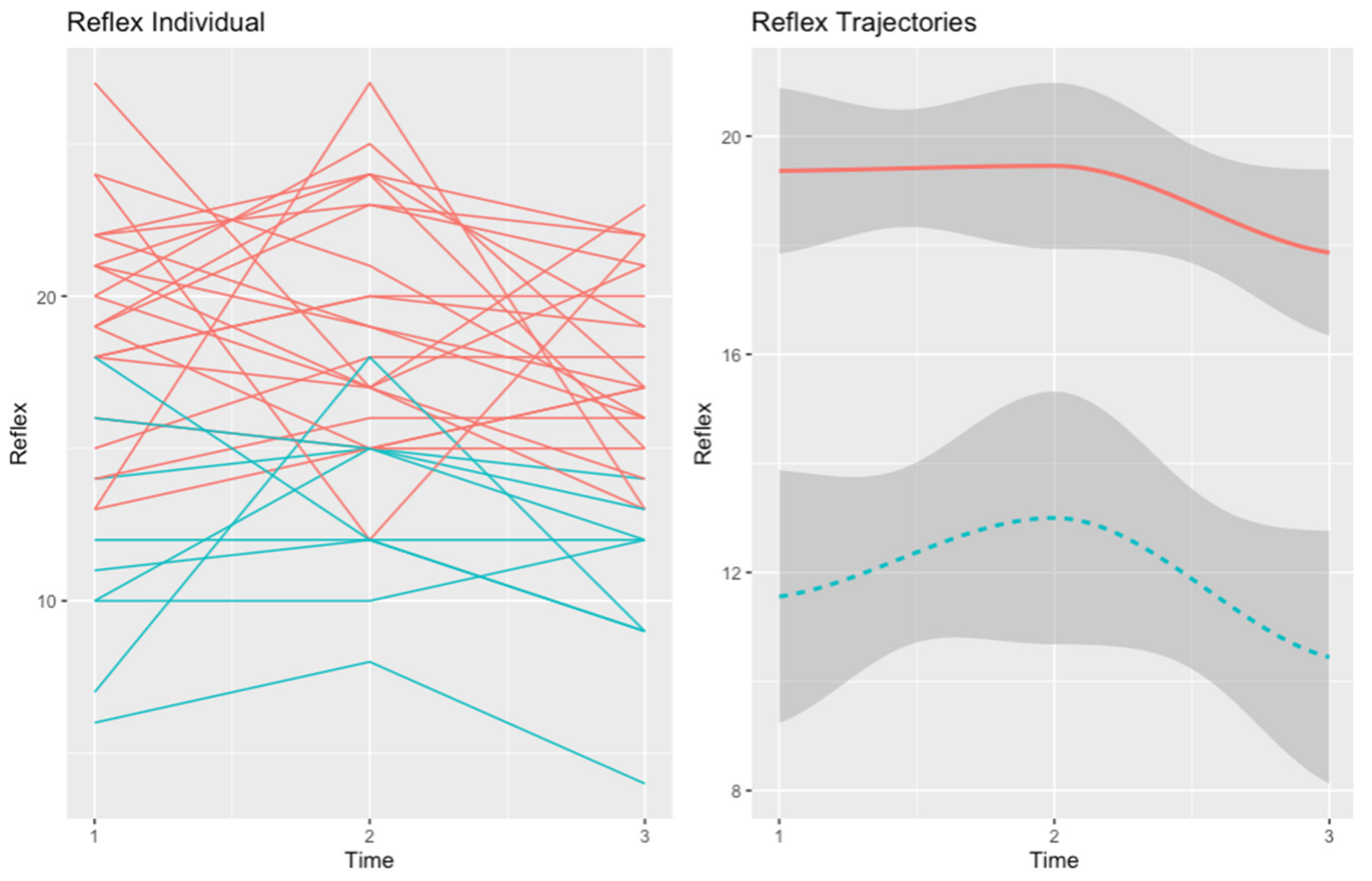
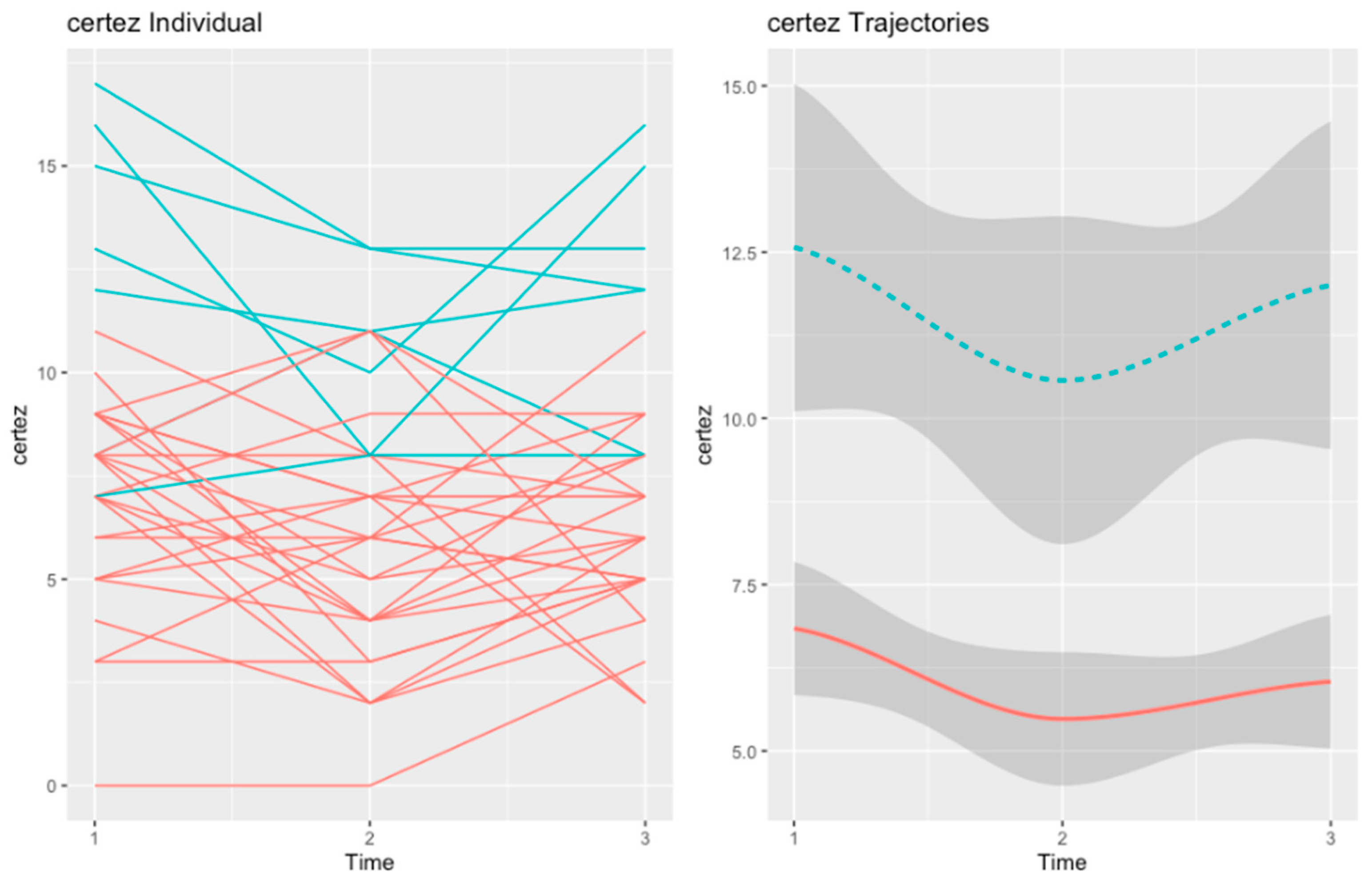
3.1. Cognitive Insight Trajectories in the MCT Group
3.1.1. Self-Reflectivity
3.1.2. Self-Certainty
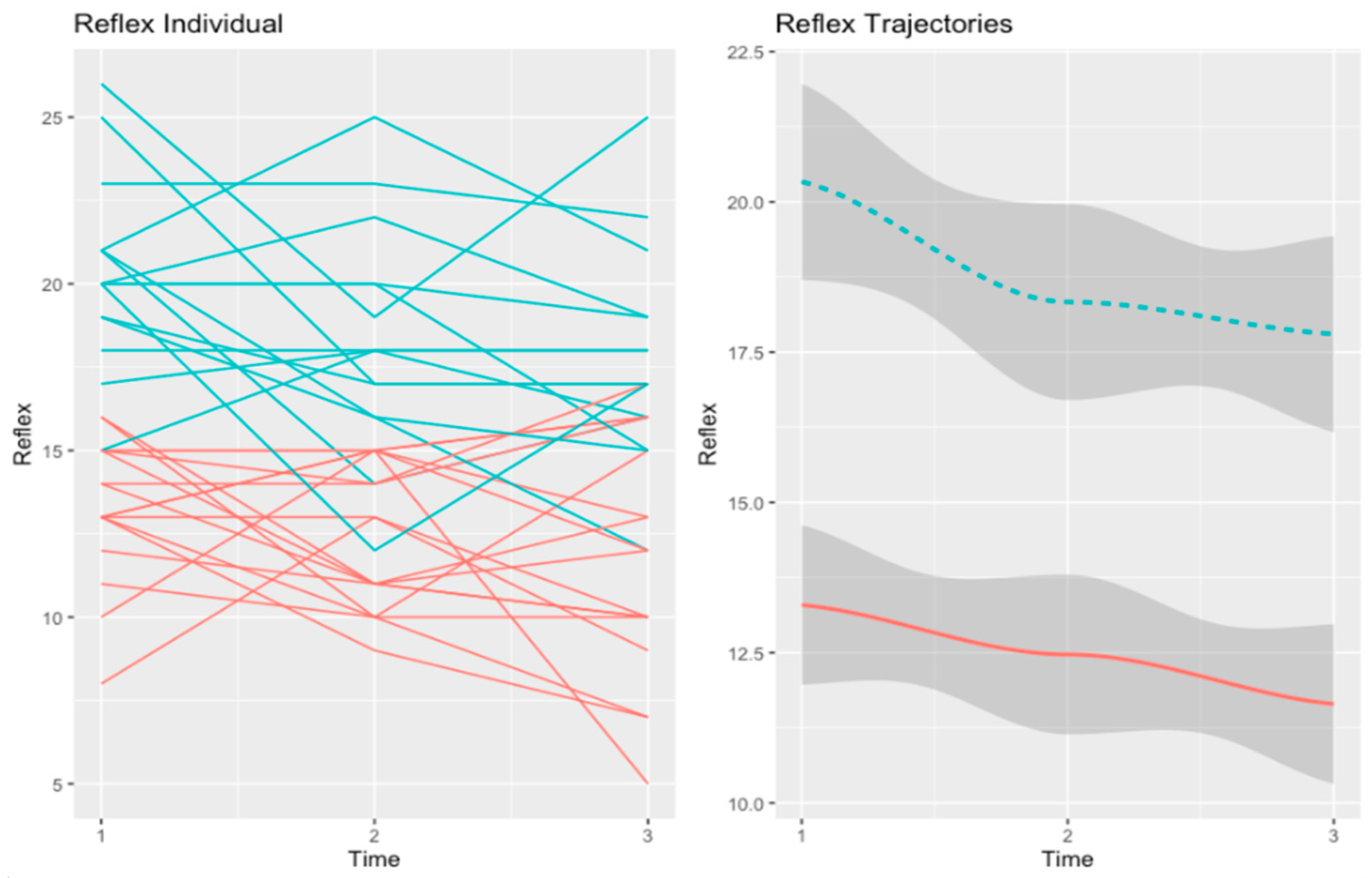
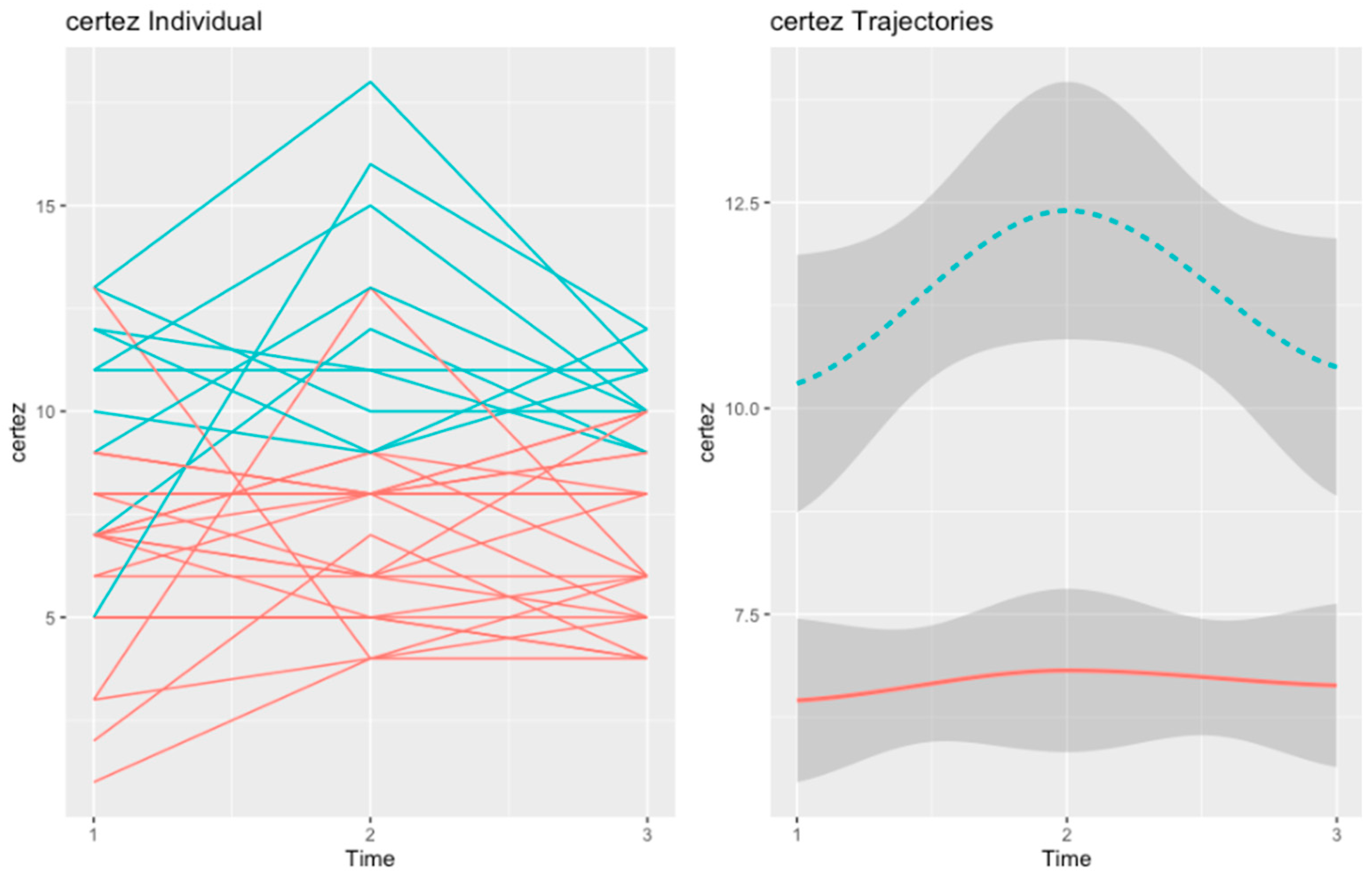
3.2. Cognitive Insight Trajectories in the Psychoeducation Group
3.2.1. Self-Reflectivity
3.2.2. Self-Certainty
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hall, M.-H.; Holton, K.M.; Öngür, D.; Montrose, D.; Keshavan, M.S. Longitudinal Trajectory of Early Functional Recovery in Patients with First Episode Psychosis. Schizophr. Res. 2019, 209, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Liemburg, E.J.; Castelein, S.; van Es, F.; Scholte-Stalenhoef, A.N.; van de Willige, G.; Smid, H.; Visser, E.; Knegtering, H.; Bruggeman, R. The Psychosis Recent Onset GRoningen Survey (PROGR-S): Defining Dimensions and Improving Outcomes in Early Psychosis. PLoS ONE 2014, 9, e113521. [Google Scholar] [CrossRef] [PubMed]
- Suvisaari, J.; Mantere, O.; Keinänen, J.; Mäntylä, T.; Rikandi, E.; Lindgren, M.; Kieseppä, T.; Raij, T.T. Is It Possible to Predict the Future in First-Episode Psychosis? Front. Psychiatry 2018, 9, 580. [Google Scholar] [CrossRef]
- Gawęda, Ł.; Moritz, S.; Ochoa, S.; So, S.H. Editorial: The Relationship Between Cognitive Biases and Psychosis: Searching for Mechanisms. Front. Psychiatry 2021, 12, 753317. [Google Scholar] [CrossRef]
- Saha, S.; Chant, D.; Welham, J.; McGrath, J. A Systematic Review of the Prevalence of Schizophrenia. PLoS Med. 2005, 2, e141. [Google Scholar] [CrossRef]
- Moritz, S.; Woodward, T.S. Metacognitive Training in Schizophrenia: From Basic Research to Knowledge Translation and Intervention. Curr. Opin. Psychiatry 2007, 20, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Penney, D.; Sauvé, G.; Mendelson, D.; Thibaudeau, É.; Moritz, S.; Lepage, M.; Mental, D. Immediate and Sustained Outcomes and Moderators Associated With Metacognitive Training for Psychosis: A Systematic Review and Meta-Analysis. JAMA 2022, 79, 417–429. [Google Scholar] [CrossRef] [PubMed]
- Moritz, S.; Andreou, C.; Schneider, B.C.; Wittekind, C.E.; Menon, M.; Balzan, R.P.; Woodward, T.S. Sowing the Seeds of Doubt: A Narrative Review on Metacognitive Training in Schizophrenia. Clin. Psychol. Rev. 2014, 34, 358–366. [Google Scholar] [CrossRef]
- Moritz, S.; Klein, J.P.; Lysaker, P.H.; Mehl, S. Metacognitive and Cognitive-Behavioral Interventions for Psychosis: New developments. Dialogues Clin. Neurosci. 2019, 21, 309. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Zhang, L.; Zhu, Z.; Li, W.; Li, C. Metacognitive Training for Schizophrenia: A Systematic Review. Shanghai Arch. Psychiatry 2015, 27, 149–157. [Google Scholar] [CrossRef]
- Ochoa, S.; López-Carrilero, R.; Barrigón, M.L.; Pousa, E.; Barajas, A.; Lorente-Rovira, E.; González-Higueras, F.; Grasa, E.; Ruiz-Delgado, I.; Cid, J.; et al. Randomized Control Trial to Assess the Efficacy of Metacognitive Training Compared with a Psycho-Educational Group in People with a Recent-Onset Psychosis. Psychol. Med. 2017, 47, 1573–1584. [Google Scholar] [CrossRef] [PubMed]
- Fett, A.K.J.; Viechtbauer, W.; Dominguez, M.d.G.; Penn, D.L.; van Os, J.; Krabbendam, L. The Relationship between Neurocognition and Social Cognition with Functional Outcomes in Schizophrenia: A Meta-Analysis. Neurosci. Biobehav. Rev. 2011, 35, 573–588. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.A.; Murray, R.M.; O’Connor, J.A.; Hockey, L.N.; Gardner-Sood, P.; Di Forti, M.; Freeman, D.; Jolley, S. Jumping to Conclusions and the Persistence of Delusional Beliefs in First Episode Psychosis. Schizophr. Res. 2015, 165, 243–246. [Google Scholar] [CrossRef]
- Falcone, M.A.; Murray, R.M.; Wiffen, B.D.R.; O’Connor, J.A.; Russo, M.; Kolliakou, A.; Stilo, S.; Taylor, H.; Gardner-Sood, P.; Paparelli, A.; et al. Jumping to Conclusions, Neuropsychological Functioning, and Delusional Beliefs in First Episode Psychosis. Schizophr. Bull. 2015, 41, 411–418. [Google Scholar] [CrossRef]
- Tripoli, G.; Quattrone, D.; Ferraro, L.; Gayer-Anderson, C.; Rodriguez, V.; La Cascia, C.; La Barbera, D.; Sartorio, C.; Seminerio, F.; Tarricone, I.; et al. Jumping to Conclusions, General Intelligence, and Psychosis Liability: Findings from the Multi-Centre EU-GEI Case-Control Study. Psychol. Med. 2021, 51, 623–633. [Google Scholar] [CrossRef]
- Díaz-Cutraro, L.; López-Carrilero, R.; García-Mieres, H.; Ferrer-Quintero, M.; Verdaguer-Rodriguez, M.; Barajas, A.; Grasa, E.; Pousa, E.; Lorente, E.; Barrigón, M.L.; et al. The Relationship between Jumping to Conclusions and Social Cognition in First-Episode Psychosis. Schizophrenia 2022, 8, 1–7. [Google Scholar] [CrossRef]
- Díaz-Cutraro, L.; García-Mieres, H.; López-Carrilero, R.; Ferrer, M.; Verdaguer-Rodriguez, M.; Barrigón, M.L.; Barajas, A.; Grasa, E.; Pousa, E.; Lorente, E.; et al. Jumping to Conclusions Is Differently Associated with Specific Subtypes of Delusional Experiences: An Exploratory Study in First-Episode Psychosis. Schizophr. Res. 2021, 228, 357–359. [Google Scholar] [CrossRef]
- Lopez-Morinigo, J.-D.; Ajnakina, O.; Martínez, A.S.-E.; Escobedo-Aedo, P.-J.; Ruiz-Ruano, V.G.; Sánchez-Alonso, S.; Mata-Iturralde, L.; Muñoz-Lorenzo, L.; Ochoa, S.; Baca-García, E.; et al. Can Metacognitive Interventions Improve Insight in Schizophrenia Spectrum Disorders? A Systematic Review and Meta-Analysis. Psychol. Med. 2020, 50, 2289. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Pattison, M.L.; Leonhardt, B.L.; Phelps, S.; Vohs, J.L. Insight in Schizophrenia Spectrum Disorders: Relationship with Behavior, Mood and Perceived Quality of Life, Underlying Causes and Emerging Treatments. World Psychiatry 2018, 17, 12–23. [Google Scholar] [CrossRef]
- Beck, A.T.; Baruch, E.; Balter, J.M.; Steer, R.A.; Warman, D.M. A New Instrument for Measuring Insight: The Beck Cognitive Insight Scale. Schizophr. Res. 2004, 68, 319–329. [Google Scholar] [CrossRef]
- O’Connor, J.A.; Ellett, L.; Ajnakina, O.; Schoeler, T.; Kollliakou, A.; Trotta, A.; Wiffen, B.D.; Falcone, A.M.; Di Forti, M.; Murray, R.M.; et al. Can Cognitive Insight Predict Symptom Remission in a First Episode Psychosis Cohort? BMC Psychiatry 2017, 17, 54. [Google Scholar] [CrossRef] [PubMed]
- Cooke, M.A.; Peters, E.R.; Fannon, D.; Aasen, I.; Kuipers, E.; Kumari, V. Cognitive Insight in Psychosis: The Relationship between Self-Certainty and Self-Reflection Dimensions and Neuropsychological Measures. Psychiatry Res. 2010, 178, 284. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Engh, J.A.; Friis, S.; Birkenaes, A.B.; Jónsdóttir, H.; Klungsøyr, O.; Ringen, P.A.; Simonsen, C.; Vaskinn, A.; Opjordsmoen, S.; Andreassen, O.A. Delusions Are Associated with Poor Cognitive Insight in Schizophrenia. Schizophr. Bull. 2010, 36, 830–835. [Google Scholar] [CrossRef]
- Liu, Y.C.; Tang, C.C.; Hung, T.T.; Tsai, P.C.; Lin, M.F. The Efficacy of Metacognitive Training for Delusions in Patients With Schizophrenia: A Meta-Analysis of Randomized Controlled Trials Informs Evidence-Based Practice. Worldviews Evidence-Based Nurs. 2018, 15, 130–139. [Google Scholar] [CrossRef]
- Sauvé, G.; Lavigne, K.M.; Pochiet, G.; Brodeur, M.B.; Lepage, M. Efficacy of Psychological Interventions Targeting Cognitive Biases in Schizophrenia: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2020, 78, 101854. [Google Scholar] [CrossRef]
- Moritz, S.; Mahlke, C.I.; Westermann, S.; Ruppelt, F.; Lysaker, P.H.; Bock, T.; Andreou, C. Embracing Psychosis: A Cognitive Insight Intervention Improves Personal Narratives and Meaning-Making in Patients With Schizophrenia. Schizophr. Bull. 2018, 44, 307–316. [Google Scholar] [CrossRef]
- Moritz, S.; Veckenstedt, R.; Andreou, C.; Bohn, F.; Hottenrott, B.; Leighton, L.; Köther, U.; Woodward, T.S.; Treszl, A.; Menon, M.; et al. Sustained and “Sleeper” Effects of Group Metacognitive Training for Schizophrenia: A Randomized Clinical Trial. JAMA Psychiatry 2014, 71, 1103–1111. [Google Scholar] [CrossRef]
- Ishikawa, R.; Ishigaki, T.; Shimada, T.; Tanoue, H.; Yoshinaga, N.; Oribe, N.; Morimoto, T.; Matsumoto, T.; Hosono, M. The Efficacy of Extended Metacognitive Training for Psychosis: A Randomized Controlled Trial. Schizophr. Res. 2020, 215, 399–407. [Google Scholar] [CrossRef]
- Fusar-Poli, P.; McGorry, P.D.; Kane, J.M. Improving Outcomes of First-Episode Psychosis: An Overview. World Psychiatry 2017, 16, 251–265. [Google Scholar] [CrossRef]
- Jung, T.; Wickrama, K.A.S. An Introduction to Latent Class Growth Analysis and Growth Mixture Modeling. Soc. Personal. Psychol. Compass 2008, 2, 302–317. [Google Scholar] [CrossRef]
- Chang, W.C.; Ho, R.W.H.; Tang, J.Y.M.; Wong, C.S.M.; Hui, C.L.M.; Chan, S.K.W.; Lee, E.M.H.; Suen, Y.N.; Chen, E.Y.H. Early-Stage Negative Symptom Trajectories and Relationships With 13-Year Outcomes in First-Episode Nonaffective Psychosis. Schizophr. Bull. 2019, 45, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Salagre, E.; Grande, I.; Solé, B.; Mezquida, G.; Cuesta, M.J.; Díaz-Caneja, C.M.; Amoretti, S.; Lobo, A.; González-Pinto, A.; Moreno, C.; et al. Exploring Risk and Resilient Profiles for Functional Impairment and Baseline Predictors in a 2-Year Follow-Up First-Episode Psychosis Cohort Using Latent Class Growth Analysis. J. Clin. Med. 2020, 10, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Merinder, L.B.; Belgamwar, M.R. Psychoeducation for Schizophrenia. Cochrane Database Syst. Rev. 2011, 6, 21–22. [Google Scholar] [CrossRef]
- Dondé, C.; Senn, M.; Eche, J.; Kallel, L.; Saoud, M.; Brunelin, J. Well-Informed but Not Aware: The P.A.C.T.® Psychoeducation Program for Schizophrenia Improves Knowledge about, but Not Insight into, the Illness. Asian J. Psychiatr. 2019, 46, 15–18. [Google Scholar] [CrossRef]
- Ahuir, M.; Cabezas, Á.; Miñano, M.J.; Algora, M.J.; Estrada, F.; Solé, M.; Gutiérrez-Zotes, A.; Tost, M.; Barbero, J.D.; Montalvo, I.; et al. Improvement in Cognitive Biases after Group Psychoeducation and Metacognitive Training in Recent-Onset Psychosis: A Randomized Crossover Clinical Trial. Psychiatry Res. 2018, 270, 720–723. [Google Scholar] [CrossRef]
- Leucht, S.; Samara, M.; Heres, S.; Davis, J.M. Dose Equivalents for Antipsychotic Drugs: The DDD Method. Schizophr. Bull. 2016, 42, 90–94. [Google Scholar] [CrossRef]
- Kay, S.R.; Fiszbein, A.; Opler, L.; Kay, S.R.; Fiszbein, A.; Opler, L.A.; Kay, S.R.; Fiszbein, A.; Opler, L. The Positive and Negative Syndrome Scale (PANSS) for Schizophrenia. Schizophr. Bull. 1987, 13, 261–276. [Google Scholar] [CrossRef]
- Peralta, V.; Cuesta, M.J. Psychometric Properties of the Positive and Negative Syndrome Scale (PANSS) in Schizophrenia. Psychiatry Res. 1994, 53, 31–40. [Google Scholar] [CrossRef]
- Amador, X.F.; Strauss, D.H.; Yale, S.A.; Flaum, M.M.; Endicott, J.; Gorman, J.M. Assessment of Insight in Psychosis. Am. J. Psychiatry 1993, 150, 873–879. [Google Scholar] [CrossRef]
- Ruiz Ripoll, A.I.; Pousa, E.; Duñó, R.; Crosas, J.M.; Cuppa, S.; García-Ribera, C. Adaptación Al Español de La Escala de Valoración de La No Conciencia de Trastorno Mental (SUMD). Actas Esp. Psiquiatr. 2008, 36, 111–119. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Gutiérrez-Zotes, J.A.; Valero, J.; Cortés, M.J.; Labad, A.; Ochoa, S.; Ahuir, M.; Carlson, J.; Bernardo, M.; Cañizares, S.; Escartin, G.; et al. Spanish Adaptation of the Beck Cognitive Insight Scale (BCIS) for Schizophrenia. Actas Esp. Psiquiatr. 2012, 40, 2–9. [Google Scholar] [PubMed]
- Brett-Jones, J.; Garety, P.; Hemsley, D. Measuring Delusional Experiences: A Method and Its Application. Br. J. Clin. Psychol. 1987, 26, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Kinderman, P.; Bentall, R.P. The Development of a Novel Measure of Causal Attributions: The Internal Personal and Situational Attributions Questionnaire. Pers. Individ. Dif. 1996, 20, 261–264. [Google Scholar] [CrossRef]
- Langdon, R.; Corner, T.; McLaren, J.; Ward, P.B.; Coltheart, M. Externalizing and Personalizing Biases in Persecutory Delusions: The Relationship with Poor Insight and Theory-of-Mind. Behav. Res. Ther. 2006, 44, 699–713. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Jolliffe, T. Is There a “Language of the Eyes”? Evidence from Normal Adults, and Adults with Autism or Asperger Syndrome. Vis. Cogn. 1997, 4, 311–331. [Google Scholar] [CrossRef]
- Huerta-Ramos, E.; Ferrer-Quintero, M.; Gómez-Benito, J.; González-Higueras, F.; Cuadras, D.; del Rey-Mejías, Á.L.; Usall, J.; Ochoa, S. Translation and Validation of Baron Cohen’s Face Test in a General Population from Spain. Actas Esp. Psiquiatr. 2020; in press. [Google Scholar]
- Corcoran, R.; Mercer, G.; Frith, C.D. Schizophrenia, Symptomatology and Social Inference: Investigating “Theory of Mind” in People with Schizophrenia. Schizophr. Res. 1995, 17, 5–13. [Google Scholar] [CrossRef]
- Gil, D.; Fernández-Modamio, M.; Bengochea, R.; Arrieta, M. Adaptation of the Hinting Task Theory of the Mind Test to Spanish. Rev. Psiquiatr. Salud Ment. (Engl. Ed.) 2012, 5, 79–88. [Google Scholar] [CrossRef]
- Endicott, J. The Global Assessment Scale: A Procedure for Measuring Overall Severity of Psychiatric Disturbance. Arch. Gen. Psychiatry 1976, 33, 766–771. [Google Scholar] [CrossRef]
- Proust-Lima, C.; Philipps, V.; Liquet, B. Estimation of Extended Mixed Models Using Latent Classes and Latent Processes: The R Package Lcmm. J. Stat. Softw. 2017, 78, 1–56. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Nagin, D.S.; Tremblay, R.E.; Sampson, R.J.; Laub, J.H. Developmental Trajectory Groups: Fact or a Useful Statistical Fiction? Criminology 2005, 43, 873–904. [Google Scholar] [CrossRef]
- Tein, J.Y.; Coxe, S.; Cham, H. Statistical Power to Detect the Correct Number of Classes in Latent Profile Analysis. Struct. Equ. Model. 2013, 20, 640. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T.M.; Atkinson, E.J. An Introduction to Recursive Partitioning Using the RPART Routines. 2019. Available online: https://cran.r-project.org/web/packages/rpart/vignettes/longintro.pdf (accessed on 10 October 2022).
- Wright, A.C.; Lysaker, P.H.; Fowler, D.; Greenwood, K. Clinical Insight in First Episode Psychosis: The Role of Metacognition. J. Ment. Health 2021, 17, 1–9. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MCT (n = 28) | Psychoeducation (n = 34) | |||||
|---|---|---|---|---|---|---|
| Mean/% | SD | Mean/% | SD | t/χ2 | p | |
| Age | ||||||
| Sex (% males) | 75.00 | 73.50 | 0.17 | 0.90 | ||
| Number of hospital admissions | ||||||
| Education (%) | 4.665 | 0.46 | ||||
| Incomplete primary education | 21.40 | 11.80 | ||||
| Complete primary education | 28.60 | 17.60 | ||||
| Incomplete secondary education | 10.70 | 20.60 | ||||
| Complete secondary education | 25.00 | 26.50 | ||||
| Incomplete superior education | 3.60 | 14.70 | ||||
| Complete superior education | 10.70 | 8.80 | ||||
| Diagnosis (%) | 4.929 | 0.43 | ||||
| Schizophrenia | 46.40 | 55.90 | ||||
| Non-specified psychotic disorder | 21.40 | 11.80 | ||||
| Schizoaffective disorder | 3.60 | 11.80 | ||||
| Delusional disorder | 7.10 | 11.80 | ||||
| Brief psychotic episode | 10.70 | 11.80 | ||||
| Schizophreniform disorder | 7.10 | 8.80 | ||||
| PANSS | ||||||
| Positive symptoms | 12.25 | 3.874 | 12.53 | 4.487 | 0.26 | 0.80 |
| Negative symptoms | 14.54 | 7.162 | 15.15 | 4.794 | 0.40 | 0.69 |
| General symptoms | 27.36 | 7.790 | 27.26 | 5.920 | −0.05 | 0.96 |
| Total | 54.14 | 15.717 | 54.94 | 12.110 | 0.23 | 0.82 |
| GAF | 66.61 | 13.331 | 57.50 | 11.758 | −2.86 | 0.01 |
| SUMD global score | 5.82 | 2.695 | 6.03 | 3.639 | 0.25 | 0.80 |
| Beads task | ||||||
| 85–15 | 3.6296 | 3.85455 | 5.3529 | 4.27737 | 1.632 | 0.11 |
| 60–40 | 6.4444 | 3.99358 | 8.5294 | 5.16536 | 1.726 | 0.09 |
| Affective | 6.3704 | 4.50767 | 7.7941 | 4.11781 | 1.286 | 1.286 |
| IPSAQ | ||||||
| Externalizing bias | 0.1481 | 3.44968 | 1.5588 | 3.85488 | 1.486 | 0.14 |
| Personalizing bias | 1.2569 | 0.72667 | 1.2183 | 0.50730 | −0.24 | 0.81 |
| Hinting task | 4.7143 | 1.01314 | 4.6765 | 0.97610 | −0.15 | 0.88 |
| Rosenberg self-esteem | 27.5714 | 6.42004 | 27.3824 | 5.03933 | −0.13 | 0.90 |
| Faces test | 17.6786 | 1.82683 | 17.4706 | 1.39773 | −0.51 | 0.61 |
| Estimated premorbid IQ | 99.4231 | 14.85442 | 96.7188 | 13.71421 | −0.72 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer-Quintero, M.; Fernández, D.; López-Carrilero, R.; Díaz-Cutraro, L.; Verdaguer-Rodríguez, M.; García-Mieres, H.; Huerta-Ramos, E.; Gómez-Benito, J.; Peláez, T.; Birulés, I.; et al. Heterogeneity in Response to MCT and Psychoeducation: A Feasibility Study Using Latent Class Mixed Models in First-Episode Psychosis. Healthcare 2022, 10, 2155. https://doi.org/10.3390/healthcare10112155
Ferrer-Quintero M, Fernández D, López-Carrilero R, Díaz-Cutraro L, Verdaguer-Rodríguez M, García-Mieres H, Huerta-Ramos E, Gómez-Benito J, Peláez T, Birulés I, et al. Heterogeneity in Response to MCT and Psychoeducation: A Feasibility Study Using Latent Class Mixed Models in First-Episode Psychosis. Healthcare. 2022; 10(11):2155. https://doi.org/10.3390/healthcare10112155
Chicago/Turabian StyleFerrer-Quintero, Marta, Daniel Fernández, Raquel López-Carrilero, Luciana Díaz-Cutraro, Marina Verdaguer-Rodríguez, Helena García-Mieres, Elena Huerta-Ramos, Juana Gómez-Benito, Trini Peláez, Irene Birulés, and et al. 2022. "Heterogeneity in Response to MCT and Psychoeducation: A Feasibility Study Using Latent Class Mixed Models in First-Episode Psychosis" Healthcare 10, no. 11: 2155. https://doi.org/10.3390/healthcare10112155
APA StyleFerrer-Quintero, M., Fernández, D., López-Carrilero, R., Díaz-Cutraro, L., Verdaguer-Rodríguez, M., García-Mieres, H., Huerta-Ramos, E., Gómez-Benito, J., Peláez, T., Birulés, I., Barajas, A., Pousa, E., Barrigón, M., Gutiérrez-Zotes, A., Grasa, E., Ruiz-Delgado, I., Lorente-Rovira, E., Cid, J., on behalf of the Spanish Metacognition Study Group, & Ochoa, S. (2022). Heterogeneity in Response to MCT and Psychoeducation: A Feasibility Study Using Latent Class Mixed Models in First-Episode Psychosis. Healthcare, 10(11), 2155. https://doi.org/10.3390/healthcare10112155