


Do Mental Health Symptoms during the Pandemic Predict University Non-Completion in a Sample of UK Students? A Prospective Study

 ,
,
Abstract
:1. Introduction
1.1. Prevalence of Mental Health Symptoms in University Students
1.2. Associations between Mental Health Symptoms and Academic Performance
1.3. Rationale and Research Aim
2. Materials and Methods
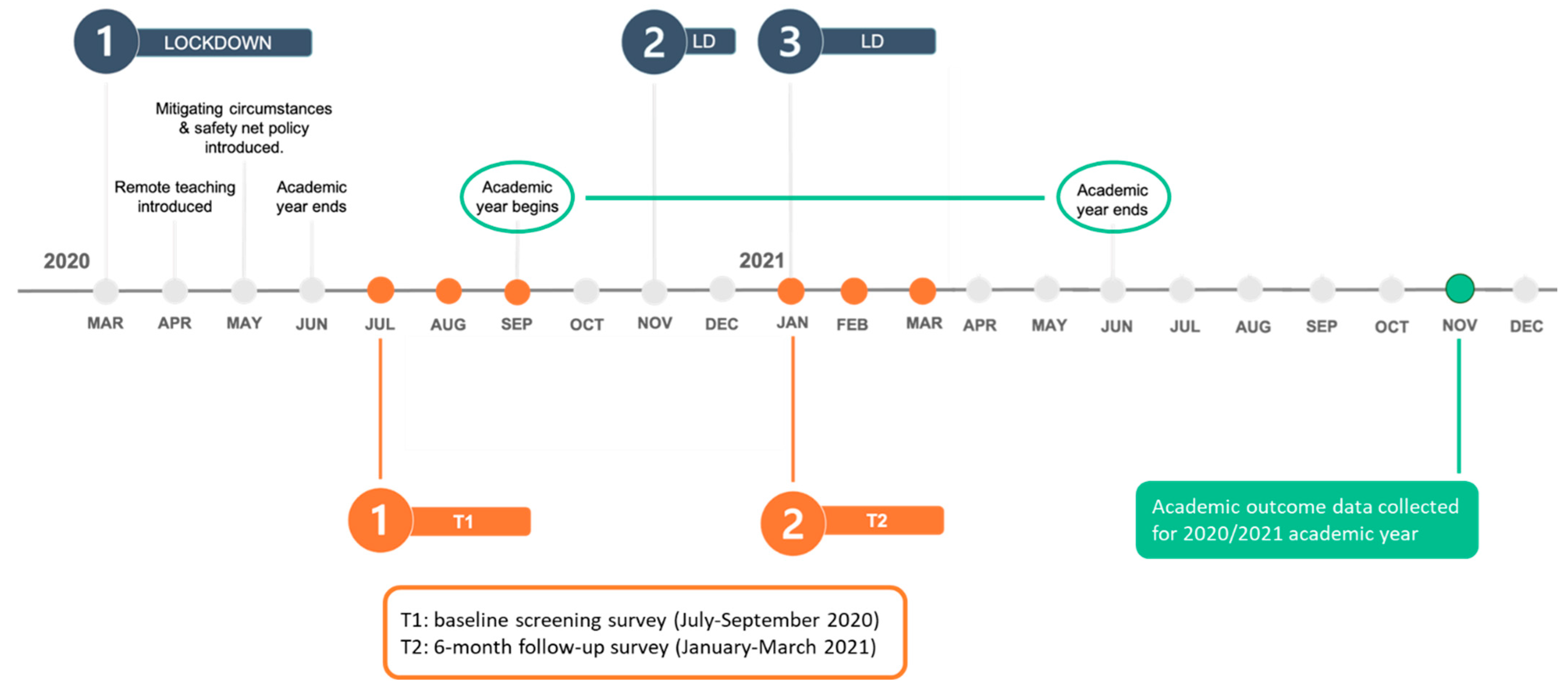
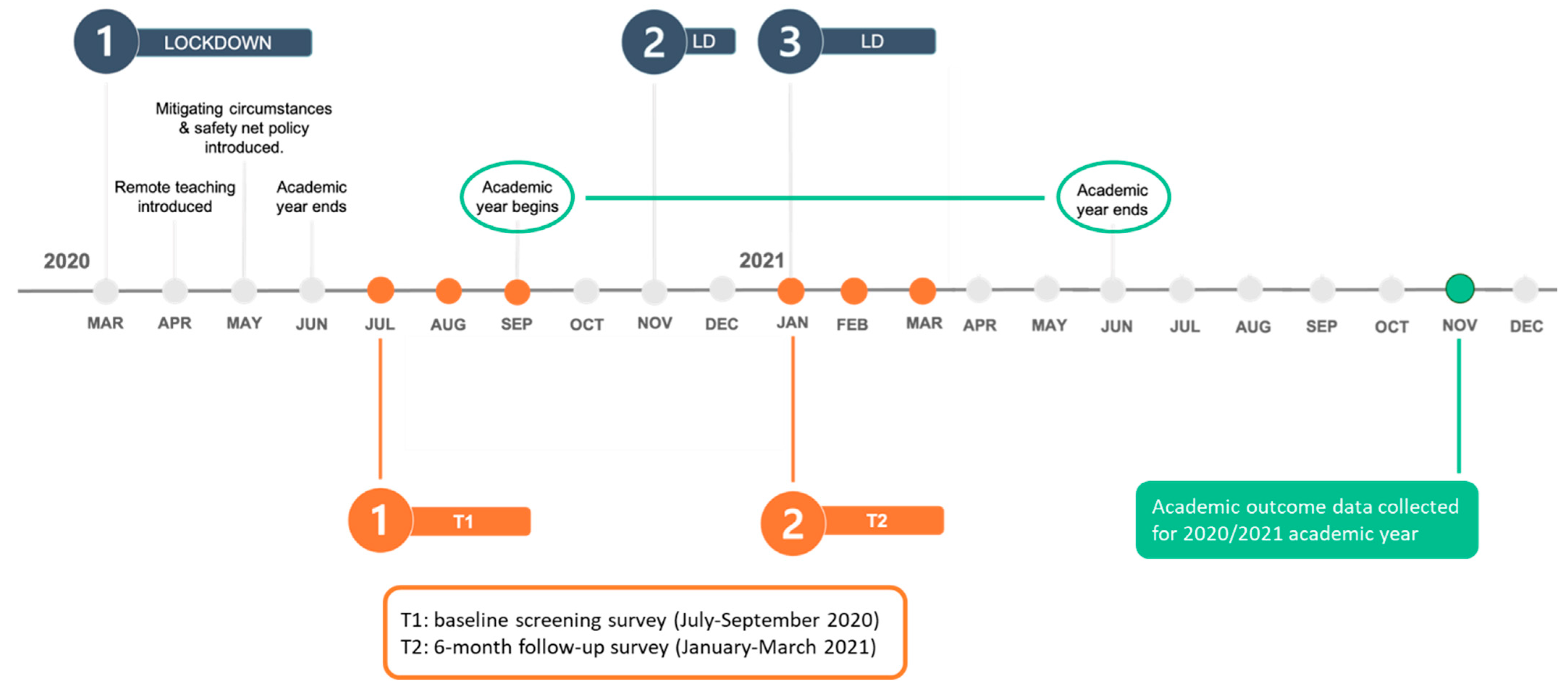
2.1. Study Design
2.2. Participants
2.3. Measures
2.3.1. Outcome Variable
2.3.2. Predictor Variables
2.3.3. Covariates
2.4. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Predictors of University Course Non-Completion
3.2.1. Anxiety
3.2.2. Depression
3.2.3. Insomnia
3.2.4. Suicidality
3.2.5. Substance Misuse Risk
3.2.6. Covariates
4. Discussion
4.1. Summary of Findings
4.2. Limitations of the Study
4.3. Implications for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bruffaerts, R.; Mortier, P.; Kiekens, G.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Nock, M.K.; Kessler, R.C. Mental Health Problems in College Freshmen: Prevalence and Academic Functioning. J. Affect. Disord. 2018, 225, 97–103. [Google Scholar] [CrossRef]
- Duffy, A.; Keown-Stoneman, C.; Goodday, S.; Horrocks, J.; Lowe, M.; King, N.; Pickett, W.; McNevin, S.H.; Cunningham, S.; Rivera, D.; et al. Predictors of Mental Health and Academic Outcomes in First-Year University Students: Identifying Prevention and Early-Intervention Targets. BJPsych Open 2020, 6, e46. [Google Scholar] [CrossRef]
- Liyanage, S.; Saqib, K.; Khan, A.F.; Thobani, T.R.; Tang, W.C.; Chiarot, C.B.; Alshurman, B.A.; Butt, Z.A. Prevalence of Anxiety in University Students during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 62. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Benatov, J.; Berger, R.; Korchagina, E.V.; et al. Mental Health Prevalence and Predictors among University Students in Nine Countries during the COVID-19 Pandemic: A Cross-National Study. Sci. Rep. 2021, 11, 18644. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Drakos, A.; Zuo, Q.K.; Huang, E. The Prevalence of Depressive Symptoms, Anxiety Symptoms and Sleep Disturbance in Higher Education Students during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Psychiatry Res. 2021, 301, 113863. [Google Scholar] [CrossRef]
- Husky, M.M.; Kovess-Masfety, V.; Swendsen, J.D. Stress and Anxiety among University Students in France during COVID-19 Mandatory Confinement. Compr. Psychiatry 2020, 102, 152191. [Google Scholar] [CrossRef]
- Evans, S.; Alkan, E.; Bhangoo, J.K.; Tenenbaum, H.; Ng-Knight, T. Effects of the COVID-19 Lockdown on Mental Health, Wellbeing, Sleep, and Alcohol Use in a UK Student Sample. Psychiatry Res. 2021, 298, 113819. [Google Scholar] [CrossRef]
- Chen, T.; Lucock, M. The Mental Health of University Students during the COVID-19 Pandemic: An Online Survey in the UK. PLoS ONE 2022, 17, e0262562. [Google Scholar] [CrossRef]
- Tang, N.K.Y.; McEnery, K.A.M.; Chandler, L.; Toro, C.; Walasek, L.; Friend, H.; Gu, S.; Singh, S.P.; Meyer, C. Pandemic and Student Mental Health: Mental Health Symptoms among University Students and Young Adults after the First Cycle of Lockdown in the UK. BJPsych Open 2022, 8, e138. [Google Scholar] [CrossRef]
- Sivertsen, B.; Vedaa, Ø.; Harvey, A.G.; Glozier, N.; Pallesen, S.; Aarø, L.E.; Lønning, K.J.; Hysing, M. Sleep Patterns and Insomnia in Young Adults: A National Survey of Norwegian University Students. J. Sleep Res. 2019, 28, e12790. [Google Scholar] [CrossRef]
- Jahrami, H.A.; Alhaj, O.A.; Humood, A.M.; Alenezi, A.F.; Fekih-Romdhane, F.; AlRasheed, M.M.; Saif, Z.Q.; Bragazzi, N.L.; Pandi-Perumal, S.R.; BaHammam, A.S.; et al. Sleep Disturbances during the COVID-19 Pandemic: A Systematic Review, Meta-Analysis, and Meta-Regression. Sleep Med. Rev. 2022, 62, 101591. [Google Scholar] [CrossRef]
- Wright, K.P.; Linton, S.K.; Withrow, D.; Casiraghi, L.; Lanza, S.M.; de la Iglesia, H.; Vetter, C.; Depner, C.M. Sleep in University Students Prior to and during COVID-19 Stay-at-Home Orders. Curr. Biol. 2020, 30, R797–R798. [Google Scholar] [CrossRef]
- Sivertsen, B.; Hysing, M.; Knapstad, M.; Harvey, A.G.; Reneflot, A.; Lønning, K.J.; O’Connor, R.C. Suicide Attempts and Non-Suicidal Self-Harm among University Students: Prevalence Study. BJPsych Open 2019, 5, e26. [Google Scholar] [CrossRef]
- El Ansari, W.; Salam, A. Multi-Substance Use Behaviors: Prevalence and Correlates of Alcohol, Tobacco and Other Drug (Atod) Use among University Students in Finland. Int. J. Environ. Res. Public Health 2021, 18, 6426. [Google Scholar] [CrossRef]
- Firkey, M.K.; Sheinfil, A.Z.; Woolf-King, S.E. Substance Use, Sexual Behavior, and General Well-Being of U.S. College Students during the COVID-19 Pandemic: A Brief Report. J. Am. Coll. Health 2022, 70, 2270–2275. [Google Scholar] [CrossRef]
- York, T.T.; Gibson, C.; Rankin, S. Defining and Measuring Academic Success. Pract. Assess. Res. Eval. 2015, 20, 5. [Google Scholar]
- Awadalla, S.; Davies, E.B.; Glazebrook, C. A Longitudinal Cohort Study to Explore the Relationship between Depression, Anxiety and Academic Performance among Emirati University Students. BMC Psychiatry 2020, 20, 448. [Google Scholar] [CrossRef]
- Gorman, E.L.; Burke, H.H.; Rubino, L.G.; Vargas, I.; Haeffel, G.J. Teasing Apart the Effect of Depression Specific and Anxiety Specific Symptoms on Academic Outcomes. Klin Spec Psihol (Clin. Psychol. Spec. Educ.) 2020, 9, 91–104. [Google Scholar] [CrossRef]
- Lipson, S.K.; Eisenberg, D. Mental Health and Academic Attitudes and Expectations in University Populations: Results from the Healthy Minds Study. J. Ment. Health 2018, 27, 205–213. [Google Scholar] [CrossRef]
- Hayley, A.C.; Sivertsen, B.; Hysing, M.; Vedaa, Ø.; Øverland, S. Sleep Difficulties and Academic Performance in Norwegian Higher Education Students. Br. J. Educ. Psychol. 2017, 87, 722–737. [Google Scholar] [CrossRef]
- Hartmann, M.E.; Prichard, J.R. Calculating the Contribution of Sleep Problems to Undergraduates’ Academic Success. Sleep Health 2018, 4, 463–471. [Google Scholar] [CrossRef]
- Vedaa, Ø.; Erevik, E.K.; Hysing, M.; Hayley, A.C.; Sivertsen, B. Insomnia, Sleep Duration and Academic Performance: A National Survey of Norwegian College and University Students. Sleep Med. X 2019, 1, 100005. [Google Scholar] [CrossRef]
- Bono, T.J.; Hill, P.L. Sleep Quantity and Variability during the First Semester at University: Implications for Well-Being and Academic Performance. Psychol. Health Med. 2021, 27, 931–936. [Google Scholar] [CrossRef]
- Okano, K.; Kaczmarzyk, J.R.; Dave, N.; Gabrieli, J.D.E.; Grossman, J.C. Sleep Quality, Duration, and Consistency Are Associated with Better Academic Performance in College Students. npj Sci. Learn. 2019, 4, 16. [Google Scholar] [CrossRef]
- Bücker, S.; Nuraydin, S.; Simonsmeier, B.A.; Schneider, M.; Luhmann, M. Subjective Well-Being and Academic Achievement: A Meta-Analysis. J. Res. Pers. 2018, 74, 83–94. [Google Scholar] [CrossRef]
- Jalali, R.; Khazaei, H.; Paveh, B.K.; Hayrani, Z.; Menati, L. The Effect of Sleep Quality on Students’ Academic Achievement. Adv. Med. Educ. Pract. 2020, 11, 497–502. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Nunnally, J.; Bernstein, I. Psychometric Theory, 3rd ed.; MacGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Thakral, M.; Von Korff, M.; McCurry, S.M.; Morin, C.M.; Vitiello, M.V. ISI-3: Evaluation of a Brief Screening Tool for Insomnia. Sleep Med. 2021, 82, 104–109. [Google Scholar] [CrossRef]
- Osman, A.; Bagge, C.; Gutierrez, P.; Konick, L.; Kooper, B.; Barrios, F. The Suicidal Behaviors Questionnaire- Revised (SBQ-R): Validation with Clinical and Nonclinical Samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef]
- National Institute for Health NIDA Quick Screen V1.0. Screening Measure. Available online: https://nida.nih.gov/sites/default/files/pdf/nmassist.pdf (accessed on 8 May 2020).
- JASP. JASP [Computer Software] 2022; Version 0.16.3; JASP: Amsterdam, The Netherlands, 2022. [Google Scholar]
- IBM Corp IBM SPSS Statistics for Windows. Version 27.0. 2020; SPSS Inc.: Chicago, IL, USA, 2020.
- Xu, S.; Ross, C.; Raebel, M.A.; Shetterly, S.; Blanchette, C.; Smith, D. Use of Stabilized Inverse Propensity Scores as Weights to Directly Estimate Relative Risk and Its Confidence Intervals. Value Health 2010, 13, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Pezzi, A.; Cavo, M.; Biggeri, A.; Zamagni, E.; Nanni, O. Inverse Probability Weighting to Estimate Causal Effect of a Singular Phase in a Multiphase Randomized Clinical Trial for Multiple Myeloma. BMC Med. Res. Methodol. 2016, 16, 150. [Google Scholar] [CrossRef] [PubMed]
- Lechner, W.V.; Laurene, K.R.; Patel, S.; Anderson, M.; Grega, C.; Kenne, D.R. Changes in Alcohol Use as a Function of Psychological Distress and Social Support Following COVID-19 Related University Closings. Addict. Behav. 2020, 110, 106527. [Google Scholar] [CrossRef]
- Charles, N.E.; Strong, S.J.; Burns, L.C.; Bullerjahn, M.R.; Serafine, K.M. Increased Mood Disorder Symptoms, Perceived Stress, and Alcohol Use among College Students during the COVID-19 Pandemic. Psychiatry Res. 2021, 296, 113706. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.C.; Hetrick, S.E.; Parker, A.G. The Impact of Stress on Students in Secondary School and Higher Education. Int. J. Adolesc. Youth 2020, 25, 104–112. [Google Scholar] [CrossRef]
- Ayala, J.C.; Manzano, G. Academic Performance of First-Year University Students: The Influence of Resilience and Engagement. High. Educ. Res. Dev. 2018, 37, 1321–1335. [Google Scholar] [CrossRef]
- Moss, R.A.; Gorczynski, P.; Sims-Schouten, W.; Heard-Laureote, K.; Creaton, J. Mental Health and Wellbeing of Postgraduate Researchers: Exploring the Relationship between Mental Health Literacy, Help-Seeking Behaviour, Psychological Distress, and Wellbeing. High. Educ. Res. Dev. 2022, 41, 1168–1183. [Google Scholar] [CrossRef]
- Levecque, K.; Anseel, F.; De Beuckelaer, A.; Van der Heyden, J.; Gisle, L. Work Organization and Mental Health Problems in PhD Students. Res. Policy 2017, 46, 868–879. [Google Scholar] [CrossRef]
- Fredricks, J.A.; Blumenfeld, P.C.; Paris, A.H. School Engagement: Potential of the Concept, State of the Evidence. Rev. Educ. Res. 2004, 74, 59–109. [Google Scholar] [CrossRef]
- Wester, E.R.; Walsh, L.L.; Arango-Caro, S.; Callis-Duehl, K.L. Student Engagement Declines in STEM Undergraduates during COVID-19–Driven Remote Learning. J. Microbiol. Biol. Educ. 2021, 22, 10–1128. [Google Scholar] [CrossRef]
- Daniels, L.M.; Goegan, L.D.; Parker, P.C. The Impact of COVID-19 Triggered Changes to Instruction and Assessment on University Students’ Self-Reported Motivation, Engagement and Perceptions. Soc. Psychol. Educ. 2021, 24, 299–318. [Google Scholar] [CrossRef] [PubMed]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the Rule of Ten Events per Variable in Logistic and Cox Regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Van Smeden, M.; De Groot, J.A.H.; Moons, K.G.M.; Collins, G.S.; Altman, D.G.; Eijkemans, M.J.C.; Reitsma, J.B. No Rationale for 1 Variable per 10 Events Criterion for Binary Logistic Regression Analysis. BMC Med. Res. Methodol. 2016, 16, 163. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Category | Completed Course (n = 134) | Did Not Complete Course (n = 13) | Total Participants (n = 147) |
|---|---|---|---|---|
| Age | 23.78 (7.388) | 25.92 (9.945) | 23.97 (7.630) | |
| Gender | ||||
| Female | 88 (65.7%) | 9 (69.2%) | 97 (66.0%) | |
| Male | 43 (32.1%) | 2 (15.4%) | 45 (30.6%) | |
| Other | 3 (2.2%) | 2 (15.4%) | 5 (3.4%) | |
| Ethnicity | ||||
| White/Caucasian | 80 (59.7%) | 6 (50.0%) | 86 (58.9%) | |
| Black/African/Caribbean/Black British | 7 (5.2%) | 2 (16.7%) | 9 (6.2%) | |
| Asian/Asian British | 28 (20.9%) | 4 (33.3%) | 32 (21.9%) | |
| Mixed | 16 (12.0%) | 0 | 16 (11.0%) | |
| Other | 3 (2.2%) | 0 | 3 (2.0%) | |
| Study level | ||||
| Undergraduate | 91 (67.9%) | 5 (38.5%) | 96 (65.3%) | |
| Postgraduate | 43 (32.1%) | 8 (61.5%) | 51 (34.7%) | |
| Type of course | ||||
| Undergraduate | 88 (65.7%) | 5 (38.5%) | 93 (63.3%) | |
| Master’s | 36 (26.9%) | 4 (30.8%) | 40 (27.2%) | |
| PhD or Professional Doctorate | 7 (5.2%) | 4 (30.8%) | 11 (7.5) | |
| Other | 3 (2.2%) | 0 | 3 (2.0%) | |
| Study mode | ||||
| Full Time | 128 (95.5%) | 12 (92.3%) | 140 (95.2%) | |
| Part Time | 6 (4.5%) | 1 (7.7%) | 7 (4.8%) | |
| Hours of study since COVID-19 | ||||
| Increased | 35 (26.1%) | 1 (7.7%) | 36 (25.2%) | |
| Decreased | 64 (47.8%) | 8 (61.5%) | 72 (50.3%) | |
| Stayed about the same | 32 (23.9%) | 3 (23.1%) | 35 (24.5%) | |
| N/A | 3 (2.2%) | 1 (7.7%) | ||
| Engagement in studies since COVID-19 | ||||
| Better | 23 (17.2%) | 5 (38.5%) | 28 (19.0%) | |
| Worse | 78 (58.2%) | 8 (61.5%) | 86 (58.5%) | |
| Stayed about the same | 33 (24.6%) | 0 | 33 (22.5%) | |
| Financial changes since COVID-19 | ||||
| Better | 41 (30.6%) | 4 (30.8%) | 45 (31.7%) | |
| Worse | 47 (35.1%) | 4 (30.8%) | 51 (35.9%) | |
| Stayed about the same | 41 (30.6%) | 5 (38.4%) | 46 (32.4%) | |
| N/A | 5 (3.7%) | 0 | ||
| Anxiety | 8.42 (5.700) | 9.77 (6.547) | 8.54 (5.767) | |
| None | 37 (27.6%) | 4 (30.8%) | 41 (27.9%) | |
| Mild | 44 (32.8%) | 1 (7.7%) | 45 (30.6%) | |
| Moderate | 31 (23.1%) | 5 (38.5%) | 36 (24.5%) | |
| Severe | 22 (16.4%) | 3 (23.0%) | 25 (17.0%) | |
| Depression | 8.13 (5.535) | 10.54 (6.936) | 8.34 (5.686) | |
| None | 38 (28.4%) | 3 (23.1%) | 41 (27.9%) | |
| Mild | 48 (35.8%) | 3 (23.1%) | 51 (34.7%) | |
| Moderate | 29 (21.6%) | 3 (23.1%) | 32 (21.8%) | |
| Moderately Severe | 14 (10.5%) | 2 (15.4%) | 16 (10.9%) | |
| Severe | 5 (3.7%) | 2 (15.4%) | 7 (4.8%) | |
| Insomnia | 3.77 (3.498) | 5.54 (4.719) | 3.93 (3.638) | |
| No Clinical Insomnia | 99 (73.9%) | 7 (53.8%) | 106 (72.1%) | |
| Clinical Insomnia | 35 (26.1%) | 6 (46.2%) | 41 (27.9%) | |
| Suicidality | 5.50 (3.028) | 6.46 (3.799) | 5.59 (3.101) | |
| Lower risk | 99 (73.9%) | 9 (69.2%) | 108 (73.5%) | |
| Higher risk | 35 (26.1%) | 4 (30.8%) | 39 (26.5%) | |
| Substance misuse risk | 2.12 (2.330) | 3.83 (4.016) | 2.28 (2.552) | |
| Low risk | 103 (77.4%) | 10 (77.0%) | 113 (77.4%) | |
| Moderate risk | 30 (22.6%) | 30 (23.0%) | 33 (22.6%) | |
| High risk | 0 | 0 | 0 |
| Predictor Variable | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Β [95% CI] | Weighted B | Β [95% CI] | Weighted B | |
| Anxiety Intercept | −2.695 [−3.789, −1.600] | −2.580 | −1.693 [−3.147, −0.239] | −3.339 |
| Anxiety | 0.040 [−0.057, 0.137] | 0.019 | 0.032 [−0.079, 0.143] | 0.015 |
| Study level (undergraduate) | −1.964 [−3.386, −0.543] ** | 1.728 * | ||
| Study hours (increased) | −3.095 [−5.608, −0.583] * | −2.807 * | ||
| Study engagement (better) | 2.369 [0.747, 3.991] ** | 2.197 * | ||
| Financial status (better) | −0.188 [−1.609, 1.232] | −0.334 | ||
| Nagelkerke R2 | 0.010 | 0.254 | ||
| Depression Intercept | −2.981 [−4.110, −1.852] | −3.002 | −2.244 [−3.799, −0.689] | −3.965 |
| Depression | 0.070 [−0.025, 0.164] | 0.063 | 0.081 [−0.024, 0.186] | 0.071 |
| Study level (undergraduate) | −1.978 [−3.414, −0.542] ** | 1.759 * | ||
| Study hours (increased) | −3.232 [−5.778, −0.685] * | −2.904 * | ||
| Study engagement (better) | 2.557 [0.901, 4.213] ** | 2.356 * | ||
| Financial status (better) | −0.049 [−1.480, 1.381] | −0.160 | ||
| Nagelkerke R2 | 0.031 | 0.281 | ||
| Insomnia Intercept | −2.946 [−3.968, −1.925] | −2.877 | −1.905 [−3.147, −0.663] | −3.701 |
| Insomnia | 0.132 [−0.025, 0.289] | 0.103 | 0.123 [−0.042, 0.288] | 0.110 |
| Study level (undergraduate) | −1.982 [−3.418, −0.547] ** | 1.778 * | ||
| Study hours (increased) | −3.123 [−5.666, −0.579] * | −2.841 * | ||
| Study engagement (better) | 2.360 [0.727, 3.993] ** | 2.216 * | ||
| Financial status (better) | −0.356 [−1.760, 1.047] | −0.415 | ||
| Nagelkerke R2 | 0.041 | 0.280 | ||
| Suicidality Intercept | −2.849 [−4.016, −1.681] | −3.072 | −2.009 [−3.541, −0.477] | −3.905 |
| Suicidality | 0.087 [−0.074, 0.247] | 0.107 | 0.101 [−0.078, 0.281] | 0.105 |
| Study level (undergraduate) | −2.038 [−3.474, −0.602] ** | 1.785 * | ||
| Study hours (increased) | −3.110 [ −5.638, −0.582] * | −2.725 * | ||
| Study engagement (better) | 2.418 [0.787, 4.048] ** | 2.169 * | ||
| Financial status (better) | −0.101 [−1.515, 1.312] | −0.211 | ||
| Nagelkerke R2 | 0.016 | 0.266 | ||
| Substance misuse risk Intercept | −2.878 [−3.717, −2.039] | −2.972 | −1.785 [−3.017, −0.554] | −3.482 |
| Substance misuse risk | 0.194 [0.019, 0.368] * | 0.196 * | 0.135 [−0.062, 0.331] | 0.137 |
| Study level (undergraduate) | −1.856 [−3.295, −0.418] * | 1.602 * | ||
| Study hours (increased) | −2.969 [−5.512, −0.426] * | −2.587 | ||
| Study engagement (better) | 2.339 [0.679, 3.999] ** | 2.079 * | ||
| Financial status (better) | −0.295 [−1.676, 1.086] | −0.394 | ||
| Nagelkerke R2 | 0.063 | 0.277 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandler, L.; McEnery, K.A.M.; Toro, C.; Singh, S.P.; Meyer, C.; Tang, N.K.Y. Do Mental Health Symptoms during the Pandemic Predict University Non-Completion in a Sample of UK Students? A Prospective Study. Educ. Sci. 2023, 13, 1227. https://doi.org/10.3390/educsci13121227
Chandler L, McEnery KAM, Toro C, Singh SP, Meyer C, Tang NKY. Do Mental Health Symptoms during the Pandemic Predict University Non-Completion in a Sample of UK Students? A Prospective Study. Education Sciences. 2023; 13(12):1227. https://doi.org/10.3390/educsci13121227
Chicago/Turabian StyleChandler, Laura, Katharine A. M. McEnery, Carla Toro, Swaran P. Singh, Caroline Meyer, and Nicole K. Y. Tang. 2023. "Do Mental Health Symptoms during the Pandemic Predict University Non-Completion in a Sample of UK Students? A Prospective Study" Education Sciences 13, no. 12: 1227. https://doi.org/10.3390/educsci13121227
APA StyleChandler, L., McEnery, K. A. M., Toro, C., Singh, S. P., Meyer, C., & Tang, N. K. Y. (2023). Do Mental Health Symptoms during the Pandemic Predict University Non-Completion in a Sample of UK Students? A Prospective Study. Education Sciences, 13(12), 1227. https://doi.org/10.3390/educsci13121227