Abstract
The style of parenting a child receives has profound long-term impacts on that child’s life. Yet, the rates of child maltreatment globally are high (in both developing and developed countries), indicating that many children around the world are being raised in toxic environments. Evidence-based parenting programs (EBPPs) have been demonstrated to have positive impacts on improving parenting style, whilst reducing childhood social, emotional and behavioural problems. EBPPs originated out of a need to address externalizing behaviour problems and to address conduct problems, and compliance became a key target of these parenting models. Thus, many EBPPs were developed in an era where operant and social learning theory-based approaches to parenting were most prominent and these parenting models still prevail today. This paper has one major aim—to demonstrate how the next generation of EBPPs need to be grounded in evolved caring motivational systems and affiliative emotion processing, which requires an understanding of the evolved processes involved in parent-offspring caring. This new approach to parenting is called, ‘compassion-focused parenting’, and this new approach to parenting will be described.
1. Nurturing Family Environments for Children: Compassion-Focused Parenting
The family environment in which children are raised can have long-lasting impacts on a range of developmental outcomes, including brain development [1], emotion regulation [2], and empathy [3], as well as mental and physical health [4]. The distinguishing features of nurturing environments include: (a) minimizing biologically and psychologically toxic environments; (b) promoting and reinforcing prosocial behaviours such as self-regulatory skills; (c) reducing the opportunities for problem behaviour; (d) encouraging psychological flexibility of individuals [5]. Biglan et al. [5] argue that family and school environments are of the highest priority when building nurturing environments, due to their influential impact on child and adolescent development, and that problems typically start to show during childhood or adolescence [6].
What is concerning is that, despite this knowledge on the importance of how children are nurtured, many children around the world continue to be raised in environments characterized by punishment, emotional and physical abuse, and neglect [7,8]. For example, a study in Brazil [9] aimed at estimating prevalence rates of corporal punishment found a rate of 10.1% for severe physical punishment (e.g., choking, shaking under 2 years of age, kicking, and beating), and 75.3% for non-severe physical punishment (e.g., spanking with hand, spanking with object, twisting ear). In the USA, a child maltreatment study found that at least 10% of parents will defer to using an object, like a spoon or belt, on a frequent or very frequent basis in order to discipline child misbehaviour [7]. Importantly, research shows smacking is ineffective at changing child behaviour in the long-term and can negatively impact parent–child attachment [7,10,11]. This has led to over 40 countries (e.g., Denmark, Germany, Israel, Sweden, Romania) introducing legislation to ban smacking and corporal punishment in order to reduce possible child maltreatment [12].
The US Department of Health and Human Services [13] reported that 3.6 million referrals were made for the maltreatment of 6.6 million children. Moreover, the World Health Organisation [14] has identified that the three key risk factors for child maltreatment are (1) the child being under 4 years of age; (2) the child being unwanted or failing to meet parent expectations; (3) the child having special needs, having abnormal physical features, or crying persistently. It is striking that the three key risk factors to maltreatment are childhood vulnerabilities, and rather than protecting our vulnerable, the vulnerable become punished. The question, therefore, is how does one facilitate change in these family environments?
There is a great need for our communities to invest in helping parents raise their children in a family context that fosters compassion and strengthens a prosocial phenotype, which in turn will benefit childhood physical health, as well as mental and social well-being, and society as a whole. One pathway to help promote more positive parenting and increase nurturing family environments is through using parenting programs. Although parenting programs have had a significant impact on improving parent–child interactions [15], a common criticism is that these programs are over-focused on reductions in negative parenting and child outcomes, without focusing on an improvement in positive behaviours and interactions (e.g., children offering to help others, interactions textured with warmth) [16]. Thus, the intention of this paper is to propose how the inclusion of affiliative processing (i.e., friendly verbal and non-verbal behaviours) and compassionate mind training can extend the impact of current parenting programs, and lead to a range of prosocial parenting and child outcomes that can help strengthen family dynamics.
The aim of this paper is to propose a new framework for understanding parenting and family interactions, referred to as compassion-focused parenting. This form of parenting is based on Gilbert’s [17] Compassion Focused Therapy model, and suggests that the next generation of parenting programs should move beyond the reductions of negative behaviours as the only metric of success, and look at measures of prosocial behaviour and affiliative relating between parents and children as crucial outcomes of success. First, this paper will outline how current Evidence-Based Parenting Programs (EBPPs) have been successful at addressing childhood difficulties by improving parenting practices; however, they have stagnated in terms of innovative growth, relying on operant and social learning theory-based approaches. Second, it will suggest how the next big innovation in EBPPs will be to adopt an evolutionary functional analysis approach examining parent physiology and emotional functioning. Finally, it will present emerging evidence supporting this compassion-focused approach to parenting. Importantly, this paper will be focused on examining the parent and child relationship (under 12 years of age).
2. A Brief History of Parenting Styles
There have been over five decades of experimental, clinical and developmental psychology research classifying parenting styles and demonstrating the impact of parenting styles on child outcomes [15,16]. Baumrind [18] originally classified three different styles of parenting: authoritative (i.e., firm boundaries but flexible, responsive to child, and recognizes the rights of the child), authoritarian (i.e., controlling, non-responsive, values obedience, and uses punitive practices), and permissive parenting (i.e., not demanding, child allowed to self-regulate). Maccoby and Martin [19], extended this work, and classified parenting as being along two dimensions of responsive or demanding parenting (also known as warmth and strictness), which resulted in four parenting styles: authoritative (demanding and responsive); authoritarian (demanding and unresponsive); indulgent (undemanding and responsive); neglectful (undemanding and unresponsive). The classification of parenting styles was an important step for the field, as it permitted developmental and parenting researchers to examine how parenting practices influenced childhood social, emotional, and behavioural outcomes.
There have been continued advances in understanding parenting style and family interactions, and researchers from around the world have also examined cultural differences [20,21]. Moreover, researchers are starting to suggest a third dimension to add to warmth and strictness, which is the ecological context in which the child grows. That is, children may respond more positively to different styles depending on context, and that perhaps regardless of context, parental warmth is the most important aspect to focus on [20]. Recent research has examined the association between parenting style and social competence among Spanish, North American, German and Brazilian adolescents in middle-class families [20]. The study had a large sample—comprising 2455 adolescents—and examined parenting style and socialization outcomes (measures of self-esteem and internalization of values). Surprisingly, adolescents from indulgent families obtained equal or higher scores on well-being than those from authoritative families, with neglectful and authoritarian families consistently reporting poor levels of self-esteem. Moreover, indulgent parenting outperformed authoritative parenting in the academic, emotional and family self-esteem domains. Moreover, recent research has also found that indulgent parenting and parenting characterized by warmth led to increases in positive adolescent development, such as school adjustment and self-esteem [21]. Yet, despite these important emerging findings highlighting the importance of warm and indulgent parenting styles, the majority of evidence-based parenting programs focuses on developing authoritative styles.
3. Evidence-Based Parenting Programs
Externalising behaviours and disobedience are the most frequently reported reasons parents refer their children to mental health professionals [22]. Thus, several parenting programs have been developed with the aim of facilitating compliance and prosocial behaviour from children, by educating parents around positive behaviour management strategies [22]. Indeed, several meta-analyses indicate that parenting programs derived from social learning principles are effective at improving child problems, child behaviour, parenting style and co-parenting relationships; with the effective sizes for treatment outcomes generally ranging from moderate to large [23,24].
There are a range of parenting programs shown to be effective at reducing coercive parenting practices and reducing child problem behaviour [25]. For example, the Triple P-Positive Parenting Program [26,27], and the Incredible Years Program [28], are two examples of programs that have had a significant impact on parenting practices and reductions in child behavior problems. Both of these programs have been referred to as evidence-based parenting programs (EBPPs) [24,27], as there are a significant number of randomized controlled trials supporting their efficacy. According to a meta-analysis by Kaminski and colleagues [22], the major components of EBPPs tend to be: (1) providing knowledge around positive parenting practices; (2) teaching parenting skills on how to relate positively to children; (3) teaching parents on how to be consistent with discipline; (4) providing opportunities for in vivo practice of these new parenting skills with the child. These components are informed predominantly from operant conditioning and a social learning theory model, and, indeed, these EBPPs emerged in an era where social learning theory was the prominent approach to understanding child development (1970s–1990s). Therefore, EBPPs originated to target the treatment of childhood conduct problems, where compliance and reduction of externalizing problem behaviours were the goals of these intervention models [22].
The previously described EBPPs (e.g., Incredible Years, Triple P) emerged during this period and are still the prevailing parenting interventions used and endorsed by organizations such as the WHO, and by evidence-based parenting lists (e.g., Blueprints for Healthy Development http://www.colorado.edu/cspv/blueprints/). What has been remarkable, is that due to the evidence supporting these EBPPs, governments are starting to provide free access to these programs to all parents, in a public health approach to supporting parents and family environments [27]. However, although EBPPs reduce externalizing behaviour problems, their potential at improving positive childhood social, emotional, and behavioural interactions (e.g., considerate behaviour, turn-taking, gratitude, empathy, and showing kindness), and improving childhood physiology (e.g., heart rate variability) remain largely unknown. Importantly, emerging research is starting to find that parenting styles characterized by warmth—compared to authoritative parenting—can have positive impacts on adolescent outcomes such as self-esteem and school adjustment [21]. However, further insights from evolutionary psychology can be helpful at furthering this impact.
4. An Evolutionary Background to Family Environments
During the last 20–30 years, there have been significant insights made into evolutionary approaches, and understanding physiology and the importance of affiliative approaches in helping understand autonomic functioning and regulation between sympathetic and parasympathetic systems, specifically for vagal tone [23,24]. Polyvagal theory, outlined by Porges [29], details how the activation of the myelinated parasympathetic nervous system helps in the regulation of the fight/flight response (autonomic sympathetic nervous system) in contexts of threat, thus enabling calmness and soothing to be achieved through having close proximity to others, and giving/receiving affiliative, caring, and prosocial behaviour [29,30]. The influence of the parasympathetic system on physiology is often measured using vagal tone, which is a measure of the activity the vagus nerve exerts. If one has high vagal tone, that indicates that their parasympathetic system is exerting pressure on the autonomic nervous system regulating the fight/flight tendency. If the vagal tone is low, one will have difficulty engaging in calming affiliative behaviour, as the fight/flight mechanism is dominant [29]. It is now known that the strength of vagal tone influences our emotions, health, and well-being [30,31]. Indeed, therapy aimed at addressing client suffering is beginning to recognise that it must be anchored in an integrative, evolutionary, contextual, biopsychosocial approach [32,33,34,35,36] if it is to be of any help at alleviating distress.
There are some specific psychotherapy models that are now adopting these new insights, such as Compassion-Focused Therapy (CFT) [37], which specifically targets physiological processes (e.g., facial expression, vocal tone, touch) in order to help stimulate vagal tone to help with the regulation of emotions and improve psychological well-being [29,30]. Through actively targeting physiological processes, one can improve heart rate variability (HRV)—a key indicator of vagal regulatory activity [24]. Indeed, a recent meta-analysis by Thayer and colleagues [31] concluded that “HRV may function as a proxy for ‘vertical integration’ of the brain mechanism that guide flexible control over behavior with peripheral physiology, and as such provides an important window into understanding stress and health.” When humans are under threat or stress, vagal tone flexibility reduces due to increases in the sympathetic system drive (particularly limbic system activation), which reduces the ability to access the pre-frontal cortex, and think laterally with empathic insight [29]. To date, CFT is the only psychotherapy to actively target physiological processes in therapy and, in a randomized controlled trial of CFT, researchers found that it was able to increase baseline HRV for participants [32].
These insights into how physiology influences emotional reactivity and behaviour have profound implications for how we consider the type of parenting our children receive. It is now known that the success of the attachment-caring strategies were key evolutionary drivers for a whole range of physiological infrastructures, such as oxytocin and the parasympathetic vagal system [33,34,35,36,37,38,39]. Yet no EBPP has a well-developed grounding in physiology or affiliative behaviours [40], and none have aimed to measure other outcomes, such as parent or child physiology (e.g., heart rate variability). This could be due to pragmatic issues, such as financial cost to conduct such studies, but also because these programs are not grounded in physiology or affiliative processing—thus they are not measured as important outcomes of interest.
Importantly, although current evidence indicates the positive impact of EBPPs, intervention models can still be improved, as other researchers in parenting also suggest [20,21]. As our understanding of the scientific processes involved in physiology and emotional functioning increases, so must our models of parenting interventions [25]. Most EBPPs, as mentioned earlier, were developed in the 1970s, where social learning theory and behavioural approaches to child and family functioning were the focus of improving parenting style and child outcomes [22]. With advances in understanding evolutionary psychology, and affective neuroscience with regard to emotion regulation systems, innovations in the EBPP model are warranted. Thus, the aim of the second part of this paper is to demonstrate how the model of EBPPs can be improved through the inclusion of compassion, which focuses on the importance of affiliative processing to facilitate change.
5. Compassion-Focused Parenting
One of the most important parenting provisions to create a safe and supportive environment for children, is to be sensitive to the child’s needs and distress and to respond appropriately. Indeed, in early childhood, the parent is typically the only source of need fulfilment, and emotion and distress regulation, as children are vulnerable and lack the required competencies to meet those needs [39]. Hence, in many ways the various motives and competencies that underpin compassion are crucial to the provision of safe, predictable, and secure environments for children.
Compassion can be defined as, “a sensitivity to the suffering in self and others, with a commitment to try and alleviate or prevent it.” [37]. Note that the prevention of suffering is important to compassionate motivation. This is especially important for childhood because a parent who is not empathetically sensitive to the needs of their child may cause a lot of suffering. For example, there can be potential neurological damage to the developing brain of babies who are left to cry alone regularly [38] and, at an extreme, unfed children tend to starve (an all too common occurrence in developing countries [39])—both examples of parental neglect.
Compassion involves two key aspects: (1) having a signal detection to suffering (i.e., sensitivity and awareness), and (2) having a signal responsiveness to suffering (i.e., taking some kind of action to alleviate and prevent suffering). Thus, compassion will involve a number of important competencies, such as how to pay attention; being emotionally moved by distress calls (rather than being disinterested or irritated by them)—that is, sympathy; having empathy—for example, knowing that a certain type of crying might mean wanting to eat, or feeling pain, distress or tiredness. In addition, as the child develops, knowing when to remove him/her from all anxiety, in contrast to helping the child stay with and cope with that anxiety (e.g., going to school). Thus, parents have to be able to tolerate distress and be non-judgmental—that is, non-condemning and non-critical [31]. The second component of compassion requires action and skills, and providing parents with specific evidence-based parenting training can be one effective way to help in the social, emotional and behavioural development of children [16]. Compassion includes three directions: giving compassion to others (e.g., friends or family members), being open and responding to receiving compassion from others, and self-compassion [40].
Compassion-focused parenting is the combination of the strategies and principles from current evidence-based parenting programs (EBPPs) with the principles of Compassion Focused Therapy (CFT). CFT, developed by Paul Gilbert over the last 20 years [37], draws upon evolutionary psychology, attachment theory, and applied psychology processes from neuroscience and social psychology [31]. CFT focuses on two psychologies of compassion. The first psychology is a motivation to engage with suffering, and the second psychology is focused on action, specifically acting to help alleviate and prevent suffering. CFT is an approach to therapy that emphasizes how the evolved brain was not developed ‘perfectly’ and rather has a host of complexities and ‘trade-offs’ that can cause suffering (e.g., shame, criticism, anxiety, depression). The emphasis of CFT is on the process of how therapy is delivered, focusing on the various fears, blocks and resistances people have to compassion, and utilizing physiological processes to help individuals embody change (e.g., body posture, vocal tone). To date, CFT has been examined in a number of trials, and a systematic review was conducted in 2014 that included 14 evaluation studies [41]. The review concluded that CFT shows promise as an intervention for mood disorders, particularly for those high in self-criticism, with further meta-analysis supporting this [42].
Importantly, CFT was initially developed for those who were not responding to cognitive-behaviour therapy in the treatment of depression [37]. Gilbert [37] found that many of the adults he was treating were raised in non-normative families of origin, where the child was subjected to physical and emotional abuse from their parents. Thus, he found many of his clients were fearful of compassion, as they were not raised in family environments characterized by warmth and affiliative behaviours. To understand how fears of compassion can manifest, Gilbert [37] draws upon evolutionary models, attachment theory and classical conditioning. For example, when a child is distressed, parental affiliative behaviours such as a warm, caring voice-tone and physical touch help to regulate the child’s distress, enabling secure attachments [37,43]. However, the attachment system can close down or ‘shut’ if the child does not have the opportunity to learn how affiliative and affectionate behaviours help regulate distress. That is, the parasympathetic system is not activated in order to downregulate threat processing, and this can lead to a heightened fear or anxiety towards affiliative behaviours [29,30]. Moreover, punitive parenting practices (e.g., over-reactive anger, criticism), particularly when children are joyful and loud, can also lead to a classically conditioned response for the individual, where positive emotions (e.g., joy, happiness) are paired with some form of punishment (e.g., being yelled at or physically hit in order to quiet down) [25]. Gilbert [37] proposes that in therapy, individuals can become quite fearful of positivity, kindness, and compassion from their therapist, as it can activate conditioned memories of loneliness, vulnerability, or shame [37]. It is hypothesized that kindness and compassion can be perceived as a source of potential threat, due to past aversive emotional memories (e.g., neglect and trauma), thus leading to fight, flight or shut-down responses by the individual. Thus, the focus of CFT is to work with the fears people have of compassion, and indeed meta-analyses have found that fears of compassion are strongly associated with depression, self-criticism and shame [39]. Indeed, research today is examining the impact of CFT for individuals who were raised in such non-normative environments, for example, CFT is now being used to help with complex trauma and adult survivors of sexual abuse [44].
Compassion-focused parenting is the application of CFT in a parenting context. Currently, parenting interventions are ‘technique’ oriented, aimed at reducing problematic behaviour [25], and are not grounded in the understanding of physiology and emotional function from an evolutionary perspective [37,45,46]. My premise is that many of the techniques in EBPPs will remain the same (e.g., attention and praise), but the model of how to facilitate positive parent–child relationships will shift to focus on evolved caring motivational systems and affiliative emotion processing, which requires an understanding of the evolved processes involved in parent–offspring caring and physiological regulating systems.
This is important because children are born prepared to respond to certain kinds of stimuli provided by the parent, such as voice tone, facial expression, and physical touch [45,46]. These processes are conveying important information about the safeness and parental investment available to the child, and set the physiological infrastructures for social–emotional development [46]. As Bowlby [43] pointed out, the provision of a secure base and safe-haven offers an evolved context for child development. Compassion is important because it brings out a range of recently evolved social intelligence competencies, such as empathy, mentalization, and self-other differentiation [45], that enable sensitive and physiologically wise parenting. Compassion-focused parenting not only is motivated towards reducing suffering and threats in the child’s environment but also providing the opportunity for exploration and social, emotional and behavioural growth. These are facilitated when parents themselves feel secure. When parents feel threatened and uncertain, they are more likely to engage defensively, responding potentially impulsively.
Thus, the compassion-focused parenting approach focuses on a range of social intelligence competencies, such as empathy, distress tolerance, and clarity of the intention in one’s parenting style. Not many parents wake in the morning with the intention to yell at their children or smack them for misbehaviour. Yet, when parents are stressed and children misbehave, these are very common techniques that parents will utilize in the moment [7]. This is typically a result of how the brain has evolved, as our threat system is the most dominant processing system [36]. Importantly, this is not the parent’s fault; parents did not choose to design their brain in this way—one focused on threat processing. Thus, compassion-focused parenting requires parents to understand how their brain functions, and how that will impact the interactions, relationship, and the development of their child’s social, emotional and behavioural growth.
Notably, compassion-focused parenting does not simply mean ‘being nice’ to your children; indeed, a compassion-focused parent will, for example, prevent a child from overeating or staying up too late despite protests from the child (this can take some courage). Indeed, there are many times when parenting your child or children is not easy, and the parent can have high levels of self-doubt, stress and guilt as to what to do in their role as caregiver [47]. Thus, compassion-focused parenting does require a number of competencies and capacities, that parents range in their ability to perform (for example distress tolerance). Therefore, in order to best help our children, we must help our parents, and provide them with the skills, knowledge, and confidence of a style of parenting that is compassion-focused, as this will help promote well-being in children and parents, whilst preventing and alleviating suffering.
6. The Caring System Motive and Parenting
Fogel, Melson, and Mistry [48] provide an influential framework to caring-nurturance and parental investment, which helps facilitate the attachment system. This includes five important capacities: (a) an awareness of the need to be nurturing; (b) a motivation to nurture; (c) an understanding of what is needed to be nurturing; (d) having the capacity to express nurturing feelings, and (e) having feedback systems—that is, having the ability to change behaviour depending on whether it has been successful or not (using the previous example of the newborn infant crying, if soothing through touch or voice does not work, the parent may need to feed the infant as he/she could have been hungry). This approach to caring and nurturing helps create the attachment system for the child [43,46]. There are three key components to attachment, proximity seeking—that is the child’s desire to have closeness to an attachment figure (typically mum or dad); secure base—the child having a source of security and guidance to go out and explore and develop confidence; and safe-haven—the child having a source of comfort when distressed to help facilitate emotion regulation [43,46]. The attachment system is critical to mammalian evolution, particularly for humans, as affiliative emotions and relating to others (e.g., parent, family, friends, others) are potentially the most significant in terms of affect regulation [35]. Affiliative connection can include touch, facial expression, and voice tone, among other factors [31,39,45].
7. Affect Regulation in Compassion-Focused Parenting
A key component of compassion-focused parenting is understanding emotion systems and affect regulation. Gilbert [37] proposed that emotion regulation occurs through three systems: threat (e.g., self-protection, safety-seeking), drive (e.g., achievement, incentive-focused, status), and soothe (e.g., non-wanting, safeness, interpersonal connection) (see Figure 1). The aim of CFT is to enhance insight into how individuals automatically respond to threat in defensive ways, which can have negative, unintended consequences, such as maladaptive self-criticism [37]. At a deeper level, cognitive processes such as rumination, negativity bias and self-critical monitoring may reflect evolutionary responses to threat employed by the human brain [45]. By developing awareness of the tricky interplay between old-brain emotions and new brain-capacities, a context for self-compassion can therefore be created [49]. Accordingly, self-compassion has been linked with enhanced distress-tolerance, clinically significant reductions in psychopathology, reflective and flexible perspective-taking, prosocial behaviour directed towards the self and others, and better adjustment to significant life stressors (e.g., infertility, cancer) [49,50,51].
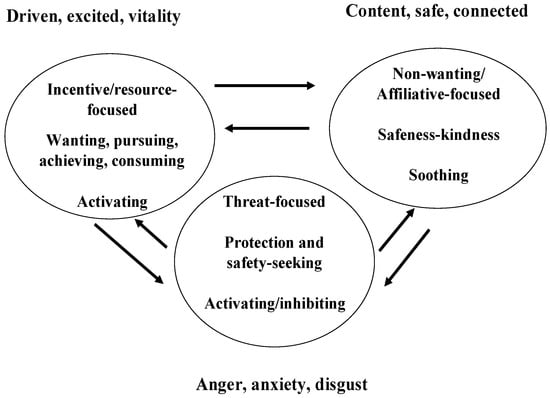
Figure 1.
The interaction between the three major emotion-regulation systems. From Gilbert, The Compassionate Mind [50], reprinted with permission from Constable & Robinson Ltd.
Compassion-focused parenting can be understood in terms of how parents increase conditions for the maturation of these three types of affective functioning, and how they can blend together and support each other.
Currently this model of emotion regulation has not been applied to EBPPs, despite the benefits that can be gained from understanding their functions. For example, children receive report cards from school indicating their level of performance compared to other children (activates a competitive motive). If the child has performed ‘average’ or ‘slightly below average’ the child can feel ‘anxious’ about showing these results to their parents. If the parent was oriented towards a threat-based approach, the parent would then respond with frustration, and perhaps anger, in the hope that this will propel the child to study harder. This can indeed have the desired result, with the child foregoing other activities, studying harder, and achieving better grades the following semester. This can result in a short-term feeling of excitement and achievement for the child, which is then reinforced by the parent. However, taking a long-term view, the child then realizes in order to continue to receive this type of reinforcement he/she needs to continue to study hard otherwise their parent will be upset with them again (anxiety or threat-based). So, we can see an interpersonal interaction between the parent and child of threat-drive-threat—a cycle which is internalized by the child. Consequently, the child is learning to regulate their emotions through these two systems, which is then continued into adulthood, and can lead to a drive of perfectionism as the child strives for success. This is concerning, as when we are trapped between the threat and reward systems (competitive motives) this can often lead to a sense of failure and high levels of self-criticism, with an inability to self-soothe or be one’s own secure base/safe-haven [50].
If we consider children raised in family homes where they are the recipients of high levels of punitive parenting practices, like smacking, or at its worst, child maltreatment, that child would be operating from their threat-based/self-protect system, as they would be scared and fearful of their parents. These situations can lead to high levels of motive conflict for the child, as the caregiver has been the activator of threat, as opposed to the activator of affiliative/soothing behaviour. This has led some to theorize that children who live in family environments where they receive high levels of punitive parenting and child maltreatment develop a self-identity where they are the ‘cause’ of the problem, and thus self-blame, as they believe that their care-giver would not engage in threat-based punitive practices unless they truly deserved them [50]. Coupled with this, is the key question, “who do children turn to for affiliative connection and soothing when they are hit by their parents?” Perhaps, if the child is lucky, another family member, say a sibling or grandparent. Unfortunately, though, the child will often be left to themselves, alone, which can reinforce a core belief of rejection, unworthiness and being unlovable. Moreover, threat can be activated from beyond the family home, with research by Horowitz, McKay, and Marshall [52] finding that 50% of children from inner cities in the USA show high rates of post-traumatic stress disorder symptoms, due to their exposure to community-level stressors such as violence involving crime and weapons use. So, it is critical to determine the environments in which children are being raised, as they will have life-long impacts on their ability to regulate their affect and form attachments with others [37].
8. Embedding a Compassion-Focused Parenting Approach in EBPPs
The impact and effectiveness of EBPPs could be improved through the adoption of a compassion-focused parenting approach. The overall aim of compassion-focused parenting is to create an internal secure-base/safe-haven in the parent or a ‘Compassionate Mind’ so that they can respond to parenting challenges as they arise at their compassionate best, as opposed to from a threat or defensive orientation. My prediction is that this orientation in parents will help improve childhood social, emotional, and behavioural development. However, randomized controlled trials are necessary to empirically test this proposition. There are many potential ways to embed a compassion-focused parenting approach in EBPPs, and I will outline a few possible pathways.
Although parenting can be extremely rewarding, parents can also struggle with finding emotional balance, and often parents indicate difficulties with failure, criticism, shame, and guilt concerning perceived parenting mistakes [47]. This is where a compassion-focused approach can be helpful, as CFT was developed to directly target high levels of self-criticism and shame [37], and there is evidence supporting the effectiveness of CFT [41,42].
One potential pathway in applying a compassion-focused parenting approach to EBPPs is helping parents understand physiology and to try and facilitate affiliative emotional relating between parent and child. Thus, the inclusion of the three circle model of emotion regulation in EBPPs will enable parents to understand the function of evolved emotion systems, so that they can gain insight into ‘what sits behind’ the interactions with their children and parenting partners (e.g., spouse, grandparent). The benefit of including the three circle model is that it will also enable a de-shaming and de-blaming process to occur for parents, as they begin to understand how they did not design the brain and body to function in that way [25]. In so doing, this process can start to facilitate a greater motivation for parents to take responsibility for how their affect regulation systems function in order to help their children’s social–emotional development.
To provide a practical example on some possible differences between compassion-focused parenting and typical evidence-based parenting programs, take the example of going shopping with a 4-year old child. Going shopping with children aged 3–9 is often regarded as a stressful parenting activity [53]. In most EBPPs, the key would be to prepare in advance and engage in a technique approach where you might, for example, (1) have activities prepared for your child as you engage in the shop (e.g., child has their own shopping list); (2) go at an appropriate time of day rather than when you are in rush; (3) decide on and discuss ground rules with the child before going shopping (e.g., stay close to mom/dad); (4) ensure you praise good behaviour whilst shopping, and (5) let the child know what consequences there might be if he/she does not follow your instructions (e.g., quiet time). A compassion-focused parenting approach would also engage in the same techniques; however, it would also focus on grounding behaviours for the parent. For example, before going shopping the parent might engage in soothing rhythm breathing—a technique which increases heart rate variability, so that the parent’s vagal tone is strengthened before going into the threatening context (e.g., the shops). With the increase in vagal tone, the parent’s emotional reactions to challenging child behaviour would be minimized, and parents can respond in more helpful ways, like remembering the planned routines as opposed to yelling or shouting at the child. The parent might focus on what ‘green circle’ strategies they might be able to use when stressed, for example, focus on body posture or tone of voice. Given the context of shopping is stressful, a compassion-focused parenting approach would also aim to normalise this, and recognise that it is not the fault of the parent that it is stressful, indeed shops have many design features that aim to take advantage of children asking for chocolate or toys. A final aspect that a compassion-focused parenting approach would be to consider how the parent is self-monitoring and judging themselves as they engage in this activity, paying particular attention to tone of inner voice. Indeed, activating a compassionate mind before going into the shops, one textured by the qualities of wisdom, strength and commitment, would be key, and is the focus of compassionate mind training [32,43]. These are just some small practical examples of what a compassion-focused parenting approach would include.
Finally, a key theoretical component of EBPPs is to ensure the parent is taking care of themselves, as if the parent’s needs are not being met this impacts their ability to meet the needs of their children [16]. A recent and significant finding in the parenting literature is that although children with empathic parents benefit significantly (i.e., experience less depression and less aggression) [54], this comes at a great cost for the parents. In two studies, researchers found that the higher the reported empathy of parents towards children [55] and adolescents [56], the greater the negative impact on the parents, specifically on inflammatory markers. The authors concluded that when children suffer psychologically, empathic parents’ immune systems suffer. Thus, although parental empathy is beneficial for children, parents must also take care of themselves. Therefore, a compassion-focused approach could be an avenue that could facilitate parenting self-care so that parents can best take care of their own needs and that of their children.
9. Emerging Evidence Supporting a Compassion-Focused Approach to Parenting
Importantly there is emerging evidence in the field of parenting research supporting a compassion-focused approach, indicating it is one which can be helpful not just for the parents, but also for the children. This research includes both cross-sectional survey design studies, along with experimental lab studies, as well as intervention evaluation of compassion-based approaches to help support parents.
To begin, research conducted by Kirby, Grzazek and Gilbert [57] examined whether goal orientation predicted parenting style. In this study, two goal orientations were examined: self-image goals (i.e., concerns with doing things wrong and being rejected) and compassionate goals (i.e., desires to be helpful), and assessed as to whether they predicted psychologically controlling parenting (i.e., controlling child’s thoughts and self-expression) or facilitative parenting (i.e., warm and responsive). The study included 151 mothers and the results found that goal orientation explained between 26–40% of the variance in parenting style, over and above child behaviour problems, parental mental health, and parental confidence. This finding is extremely important, as most parenting research indicates that it is the level of child behaviour which is most predictive of parenting style [24], whereas this research, the first to my knowledge, indicates that shifting motivational or goal orientation is a key pathway to parenting style.
Extending on these findings, Kirby, Sampson, Day, Hayes and Gilbert [58] examined the role that shame and compassion may play in texturing parenting style. The authors predicted that those parents who had high levels of shame (rank and self-image focused) and fears of compassion would engage in parenting styles that were both psychological controlling and dysfunctional. They conducted an online survey recruiting 333 parents of children aged between 3–9 years of age. Results from hierarchical and standard linear regressions found support for their hypotheses that shame and fears of compassion explain significant variances in parenting style, with models predicting 24% and 46% of the variance, respectively. These findings support past research indicating those who experience shame also find it difficult to experience compassion [39].
Following on from this, Kirby, Grzazek, and Gilbert [57] completed an experimental study where 198 mothers were randomly assigned to a compassion condition, a self-image condition or a control condition. Mothers would then be presented with stressful child scenarios, for example a temper tantrum at the shops, and told to relate to the themselves with either self-image instructions (i.e., we try to get out children to do things our way because we know what is best for them), or compassionate instructions (i.e., we all face challenges and setbacks and disappointments. Try not to be too hard on yourself). The authors predicted the prompting compassionate goals would lead to reduce negative emotional reactions compared to the self-image condition, however there were no differences between the conditions. The authors concluded that brief instructions are insufficient at shifting parental reactions to difficult child behaviour scenarios. Indeed, a greater level of intervention support is needed for parents.
In another study led by Kirby and Baldwin [59], they examined the impact of a 15-min loving–kindness meditation as way to help improve parental reactions to difficult child behaviour. In this brief intervention study, Kirby and Baldwin [59] examined the impact of loving–kindness meditation (LKM) for parents of children aged 2–12 years of age. LKM involves the repetition of short phrases (e.g., “May you be safe, may you be peaceful”) towards oneself and others. A meta-analysis has found that LKM has significant moderate effects on compassion, self-compassion, as well as decreasing depression [60]. The Kirby and Baldwin [59] study included 61 parents who were randomly assigned to receive LKM (15-min guided audio) or a Focused Imagery (FI) exercise. The authors found that this brief intervention was sufficient in leading to emotional reactions that were difference across the conditions, whereby in the LKM condition parents felt calmer and more sympathetic towards the children, and less frustrated and angry. Moreover, LKM also improved the parents’ level of self-compassion motivations compared to the FI condition. This study provides initial evidence for the use of LKM in a parenting context.
Finally, in an intervention design, we examined the feasibility and acceptability of a brief self-compassion intervention for mothers of infants [61]. The transition to motherhood can be challenging for many, especially when the mothering experience does not go as expected, which can lead mothers to feel guilty, ashamed, and distressed. For example, mothers can experience difficult and traumatic childbirth [62], and can have difficulty with breastfeeding attachment [63]. The aim of this study was to support mothers experiencing this transition to motherhood. We developed brief online resources, which were informed by CFT, and included two videos on self-compassion meditation, as well as a tip-sheet. Overall, 262 mothers were recruited for the intervention, and results were examined pre-post, as there was no control comparison, which is a limitation of the study. However, the intervention found that it was able to significantly improve self-compassion, decreases in posttraumatic symptoms, improve subjective breastfeeding experience, and satisfaction with infant feeding. However, the intervention was unable to change level of shame experienced. Indeed, shame is am embedded and multifaceted experience, and a longer intervention would likely be needed in order to help mothers with the shame experience.
10. Parenting Increasing Child’s Level of Compassion
An important rationale for the inclusion of a compassion-focused approach in EBPPs is the aim of raising more compassionate children. Research has documented that children with empathic parents show more empathy themselves [3]. In contrast, the Making Caring Common Project at Harvard University, surveyed 10,000 adolescents across the United States and found that 80% said that “achievement or happiness” is their top priority, compared to 20% saying “caring for others” is their top priority [64]. Moreover, the study found youths were three times more likely to agree than disagree with the statement: “my parents are prouder if I get good grades than if I’m a caring community member.” As a result, there is an important role for parenting interventions to help encourage compassion and caring behaviour in children and adolescents, as well as school-based educational programs, which need to be developed, applied, and evaluated.
11. Future Research Areas
There is great potential for compassion to play a central role in EBPPs, but much empirical research is required to determine its efficacy and impact on a range of important family outcomes. Such studies include measuring compassion as an outcome of interest in EBPP evaluations. For example, the measurement of HRV will become central, and correlating HRV to parenting style and child social, emotional and behavioural outcomes will provide greater insights into mechanisms underpinning parent–child interactions. In addition, there are many parents who do not respond to EBPPs [16]—could it be that non-responders to EBPPs have high HRV, indicating reduced vagal tone flexibility, indicating a reduced capacity to take on new parenting styles? Thus, would an approach that aimed to increase HRV make it more likely for these parents do feel a greater sense of safeness to adopt new parenting approaches and have less fears, blocks and resistances to positive parenting practices? These are important questions that remain unanswered, but could have significant implications for the future success of EBPPs.
Self-report measures already exist, such as the Fears of Compassion Scale [65] and the Self-Compassion Scale [66], and including these measures can also assist in determining whether compassion acts as a significant moderator or mediator to EBPPs, as determined by shift in parenting style and child social, emotional and behavioural outcomes. Moreover, there are some parents who are non-responders to EBPPs [19]—a potential reason for this could be due to the parents own fears, blockers and resistances (FBRs) to positive affiliative emotions and behaviours, which they are confronted with when participating in EBPPs. Thus, an important area of research is to examine whether the inclusion of compassion helps address these FBRs [65] to help increase responsiveness and maintain parent participation in EBPPs. Compassion may also have differential impacts on certain parenting populations. For example, would compassion-based exercises in EBPPs have greater impact on the parents of young children or teenagers? Or perhaps parents of children with long-standing difficulties, such as chronic health illnesses or clinical conditions such as Autism or Attention-Deficit/Hyperactivity Disorder, may benefit most from compassion-based EBPPs. Or potentially it is parents with high levels of shame and self-criticism who stand to benefit the most from compassionate based EBPPs.
A key future research question is to determine whether a compassion-focused approach to parenting increases the efficacy of EBPPs when compared to existing interventions. In evaluations, outcomes should not only be focused on short-term (e.g., pre, post and six-month follow-up), but also longitudinal (5, 10, 30 years), outcomes to determine the impacts of compassion-focused parenting. Multiple sources of assessment would be helpful to understand the impact of compassion-focused parenting, so through observation of parent–child interactions, sibling-interactions, and physiological measurements (e.g., heart rate variability) of children and parents, as well as self-report scales.
12. Conclusions
To conclude, with the advances in the understanding of how the brain functions and the importance of understanding evolved caring motivational systems and affiliative emotion processing, the next generation of EBPPs have an exciting future. Compassion-focused parenting has the potential to help de-stigmatize and de-shame parenting experiences, helping parents with the rewarding and at times challenging experiences that occur when raising children. The further benefit of a compassion-focused parenting approach is the hope it will also raise compassionate children. In summarizing, Paul Gilbert provides a poignant insight into why this area of compassion-focused parenting is so important:
It is quite extraordinary that, given what we know about how early lives effect brain maturation and even genetic expression, we have such limited resources dedicated to the desire for “every child to grow-up in a compassionate environment”. This failure to grasp the size and nature of the problem of, ‘how children around the world are raised in appalling conditions’ is probably humanity’s greatest compassion failure!
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Beaver, K.M.; Belsky, J. Gene-environment interaction and the intergenerational transmission of parenting: Testing the differential-susceptibility hypothesis. Psychiatry Q. 2012, 83, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Cecil, C.A.M.; Barker, E.D.; Jaffee, S.; Viding, E. Association between maladaptive parenting and child self-control over time: Cross-lagged study using a monozygotic twin difference design. Br. J. Psychiatry 2012, 201, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, N.; Fabes, R.A.; Schaller, M.; Carlo, G.; Miller, P.A. The relations of parental characteristics and practices to children’s vicarious emotional responding. Child Dev. 1991, 62, 1393–1408. [Google Scholar] [CrossRef] [PubMed]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.; Caspi, A. A gradient of childhood self-control predicts health, wealth, and public safety. Proc. Natl. Acad. Sci. 2011, 108, 2693–2698. [Google Scholar] [CrossRef]
- Biglan, A.; Flay, B.R.; Embry, D.D.; Sandler, I.N. The critical role of nurturing environments for promoting human well-being. Am. Psychol. 2012, 67, 257–271. [Google Scholar] [CrossRef]
- National Research Council & Institute of Medicine. Preventing Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities; National Academie Press: Washington, DC, USA, 2012. [Google Scholar]
- Prinz, R.J.; Sanders, M.R.; Shapiro, C.J.; Whitaker, D.J.; Lutzker, J.R. Population-based prevention of child maltreatment: The U.S. Triple P system population trial. Prev. Sci. 2009, 10, 1–12. [Google Scholar] [CrossRef]
- Zolotor, A.J.; Theodore, A.D.; Coyne-Beasley, T.; Runyan, D.K. Intimate partner violence and child maltreatment: Overlapping risk. Brief Treat. Crisis Interv. 2007, 7, 305–321. [Google Scholar] [CrossRef]
- Bordin, I.A.S.; Paula, C.S.; do Nascimento, R.; Duarte, C.S. Severe physical punishment and mental health problems in an economically disadvantaged population of children and adolescents. Braz. J. Psychiatry 2006, 28, 290–296. [Google Scholar] [CrossRef]
- D’Souza, A.J.; Russell, M.; Wood, B.; Signal, L.; Elder, D. Attitudes to physical punishment of children are changing. Arch. Dis. Child 2016, 101, 690–693. [Google Scholar] [CrossRef]
- Klevens, J.; Whitaker, D.J. Primary prevention of child physical abuse and neglect: Gaps and promising directions. Child Maltreat. 2007, 12, 364–377. [Google Scholar] [CrossRef]
- United Nations Tribune. The 42 Countries That Have Banned Corporal Punishment. Available online: http://untribune.com/42-countries-banned-corporal-punishment/ (accessed on 12 September 2019).
- U.S. Department of Health and Human Services. Child Maltreatment. Available online: https://www.acf.hhs.gov/sites/default/files/cb/cm2016.pdf (accessed on 12 September 2019).
- World Health Organization. Child Maltreatment. WHO: Geneva, Switzerland. Available online: www.who.int/mediacentre/factsheets/fs150/en/ (accessed on 12 September 2019).
- Patterson, G.R. The next generation of PMTO models. Behav. Ther. 2005, 28, 25–32. [Google Scholar]
- Sanders, M.R.; Kirby, J.N. Parental programs for preventing behavioural and emotional problems in children. In Oxford Guide to Low Intensity CBT Interventions; Bennett-Levy, J., Richards, D., Farrand, P., Christensen, H., Griffiths, K., Kavanagh, D., Klein, B., Lau, M.A., Proudfoot, J., Ritterband, L., et al., Eds.; Oxford University Press: New York, NY, USA, 2010; pp. 399–406. [Google Scholar]
- Gilbert, P. Psychotherapy for the 21st century: An integrative, evolutionary, contextual biopsychosocial approach. Psychol. Psychother. Theory Res. Pract. 2019, 92, 164–189. [Google Scholar] [CrossRef] [PubMed]
- Baumrind, D. Effects of authoritative parental control on child behavior. Child Dev. 1966, 37, 887–907. [Google Scholar] [CrossRef]
- Maccoby, E.E.; Martin, J.A. Socialization in the context of the family: Parent-child interaction. In Handbook of Child Psychology; Mussen, P.H., Ed.; Wiley: New York, NY, USA, 1983; Volume 4, pp. 1–101. [Google Scholar]
- Garcia, F.; Serra, E.; Garcia, O.F.; Martinez, I.; Cruise, E. A third emerging stage for the current digital society? Optimal parenting styles in Spain, the United States, Germany, and Brazil. Int. J. Environ. Res. Public Health 2019, 16, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Martinez, I.; Garcia, F.; Fuentes, M.C.; Veiga, F.; Garcia, O.F.; Rodrigues, Y.; Cruise, E.; Serra, E. Researching parental socialization styles across three cultural contexts: Scale ESPA29 bi-dimensional validity in Spain, Portugal and Brazil. Int. J. Environ. Res. Public Health 2019, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, J.W.; Valle, L.A.; Filene, J.H.; Boyle, C.L. A meta-analytic review of components associated with parent training program effectiveness. J. Abnorm. Child Psychol. 2008, 36, 567–589. [Google Scholar] [CrossRef]
- Kirby, J.N. The role of mindfulness and compassion in enhancing nurturing family environments. Clin. Psychol. Sci. Prac. 2016, 23, 142–157. [Google Scholar] [CrossRef]
- Morawska, A.; Haslam, D.; Milne, D.; Sanders, M.R. Evaluation of a brief parenting discussion group for parents of young children. J. Dev. Behav. Pediatr. 2011, 32, 136–145. [Google Scholar] [CrossRef]
- Mingebach, T.; Kamp-Becker, I.; Christiansen, H.; Weber, L. Meta-meta-analysis on the effectiveness of parent-based interventions for the treatment of child externalizing behavior problems. PLos ONE 2018, 13, 1–21. [Google Scholar] [CrossRef]
- Sanders, M.R.; Kirby, J.N.; Tellegen, C.L.; Day, J.J. The Triple P-Positive Parenting Program: A systematic review and meta-analysis. Clin. Psychol. Rev. 2014, 34, 337–357. [Google Scholar] [CrossRef]
- Sanders, M.R.; Kirby, J.N. A Public-health approach to improving parenting and promoting children’s well-being. Child Dev. Perspect. 2014, 8, 250–257. [Google Scholar] [CrossRef]
- Webster-Stratton, C. Preventing conduct problems in Head Start children: Strengthening parenting competencies. J. Consult. Clin. Psychol. 1998, 66, 715–730. [Google Scholar] [CrossRef] [PubMed]
- Porges, S.W. The polyvagal perspective. Biol. Psychol. 2007, 74, 116–143. [Google Scholar] [CrossRef] [PubMed]
- Thayer, J.F.; Lane, R.D. A model of neurovisceral integration in emotion regulation and dysregulation. J. Affect. Disord. 2000, 61, 201–216. [Google Scholar] [CrossRef]
- Thayer, J.F.; Ahs, F.; Fredrickson, M.; Sollers, J.J.; Wager, T.D. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health. Neurosci. Biobehav. Rev. 2012, 36, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Matos, M.; Duarte, C.; Duarte, J.; Pinto-Gouveia, J.; Petrocchi, N.; Basran, J.; Gilbert, P. Psychological and physiological effects of Compassionate Mind Training: A pilot randomized controlled study. Mindfulness 2017, 8, 1699–1712. [Google Scholar] [CrossRef]
- Colonnello, V.; Petrocchi, N.; Heinrichs, M. The psychobiological foundation of interpersonal relationships: The role of oxytocin in daily social exchanges. In Compassion: Concepts, Research, and Applications; Gilbert, P., Ed.; Routledge: Abingdon-on-Thames, UK, 2012; pp. 105–119. [Google Scholar]
- Davidson, R.J. The biology of compassion. In Wisdom and Compassion in Psychotherapy: Deepening Mindfulness in Clinical Practice; Germer, C., Siegel, D., Eds.; Guilford Press: New York, NY, USA, 2012; pp. 111–118. [Google Scholar]
- Depue, R.A.; Morrone-Strupinsky, J.V. A neurobehavioral model of affiliative bonding. Behav. Brain Sci. 2005, 28, 313–395. [Google Scholar] [CrossRef]
- Swain, J.E.; Ho, S.S. Parental brain—The crucible of compassion. In Oxford Handbook on Compassion Science; Seppälä, E., Simon-Thomas, E., Brown, S.L., Worline, M.C., Cameron, C.D., Doty, J.R., Eds.; Oxford University Press: Oxford, MS, USA, 2017. [Google Scholar]
- Gilbert, P. The origins and nature of compassion focused therapy. Br. J. Clin. Psychol. 2014, 53, 6–41. [Google Scholar] [CrossRef]
- Bugental, D.B.; Martorell, G.A.; Barraza, V. The hormonal costs of subtle forms of infant maltreatment. Horm. Behav. 2003, 43, 237–244. [Google Scholar] [CrossRef]
- Maternal and Child Nutrition Study Group. Maternal and child nutrition: Building momentum for impact. Lancet 2013, 382, 372–375. [Google Scholar] [CrossRef]
- Kirby, J.N.; Day, J.; Sagar, V. The ‘Flow’ of compassion: A meta-analysis of the fears of compassion scales and psychological functioning. Clin. Psychol. Rev. 2019, 70, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Leaviss, J.; Uttley, L. Psychotherapeutic benefits of compassion-focused therapy: An early systematic review. Psychol. Med. 2015, 45, 927–945. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.N.; Tellegen, C.L.; Steindl, S.R. A meta-analysis of compassion-based interventions: Current state of knowledge and future directions. Behav. Ther. 2017, 48, 778–792. [Google Scholar] [CrossRef] [PubMed]
- Bowlby, J. Attachment and Loss, 2nd ed.; Basic Books: New York, NY, USA, 1969. [Google Scholar]
- McLean, L.; Steindl, S.R.; Bambling, M. Compassion-focused therapy as an intervention for adult survivors of sexual abuse. J. Child Sex. Abus. 2018, 27, 161–175. [Google Scholar] [CrossRef]
- Dunbar, R.I.M. The social role of touch in humans and primates: Behavioural function and neurobiological mechanisms. Neurosci. Biobehav. Rev. 2010, 34, 260–268. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. An attachment perspective on compassion and prosocial virtues. In Compassion: Concepts, Research, and Applications; Gilbert, P., Ed.; Routledge: Abingdon-on-Thames, UK, 2017; pp. 187–202. [Google Scholar]
- Haslam, D.M.; Patrick, P.; Kirby, J.N. Giving voice to working mothers: A consumer informed study to program design for working mothers. J. Child Fam. Stud. 2015, 24, 2463–2473. [Google Scholar] [CrossRef]
- Fogel, A.; Melson, G.F.; Mistry, J. Conceptualising the determinants of nurturance: A reassessment of sex differences. In Origins of Nurturance: Developmental, Biological and Cultural Perspectives on Caregiving; Fogel, A., Melson, F., Eds.; Lawrence Erlbaum Associates Inc.: Hillsdale, NJ, USA, 1986; pp. 69–90. [Google Scholar]
- Gilbert, P. The Compassionate Mind; Constable & Robinson Ltd.: London, UK, 2009. [Google Scholar]
- Goetz, J.L.; Keltner, D.; Simon-Thomas, E. Compassion: An evolutionary analysis and empirical review. Psychol. Bull. 2010, 136, 351–374. [Google Scholar] [CrossRef]
- MacBeth, A.; Gumley, A. Exploring compassion: A meta-analysis of the association between self-compassion and psychopathology. Clin. Psychol. Rev. 2012, 32, 545–552. [Google Scholar] [CrossRef]
- Horowitz, K.; McKay, M.; Marshall, R. Community violence and urban families: Experiences, effects, and directions for intervention. Am. J. Orthopsychiatr. 2005, 75, 356–368. [Google Scholar] [CrossRef]
- Kirby, J.N. Compassion interventions: The programs, the evidence, and implications for research and practice. Psychol. Psychother. Theory Res. Pract. 2017, 90, 432–455. [Google Scholar] [CrossRef]
- Chase-Lansdale, P.L.; Wakschlag, L.S.; Brooks-Gunn, J. A psychological perspective on the development of caring in children and youth: The role of the family. J. Adolesc. 1995, 18, 515–556. [Google Scholar] [CrossRef]
- Manczak, E.; DeLongis, A.; Chen, E. Does empathy have a cost? Diverging psychological and physiological effects within families. Health Psychol. 2016, 35, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Manczak, E.M.; Basu, D.; Chen, E. The Price of Perspective Taking: Child Depressive Symptoms Interact with Parental Empathy to Predict Immune Functioning in Parents. Clin. Psychol. Sci. 2015, 4, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.N.; Grzazek, O.; Gilbert, P. The role of compassionate and self-image goals in predicting psychological controlling and facilitative parenting styles. Front. Psychol. 2019, 10, 1041. [Google Scholar] [CrossRef]
- Kirby, J.N.; Sampson, H.; Day, J.; Hayes, A.; Gilbert, P. Human evolution and culture in relationship to shame in the parenting role: Implications for psychology and psychotherapy. Psychol. Psychother. Theory Res. Pract. 2019, 92, 238–260. [Google Scholar] [CrossRef]
- Kirby, J.N.; Baldwin, S. A randomized micro-trial of a loving-kindness meditation to help parents respond to difficult child behaviour vignettes. J. Child Fam. Stud. 2018, 27, 1614–1628. [Google Scholar] [CrossRef]
- Galante, J.; Galante, I.; Bekkers, M.J.; Gallacher, J. Effect of kindness-based meditation on health and well-being: A systematic review and meta-analysis. J. Consult. Clin. Psychol. 2014, 82, 1101–1114. [Google Scholar] [CrossRef]
- Mitchell, A.; Whittingham, K.; Steindl, R.S.; Kirby, J.N. Feasibility and acceptability of a brief online self-compassion intervention for mothers of infants. Arch. Women’s Ment. Health 2018, 21, 553–561. [Google Scholar] [CrossRef]
- Soet, J.E.; Brack, G.A.; DiIorio, C. Prevalence and predictors of women’s experience of psychological trauma during childbirth. Birth 2003, 30, 36–46. [Google Scholar] [CrossRef]
- Hall, H.; McLelland, G.; Gilmour, C.; Cant, R. ‘It’s those first few weeks’: Women’s views about breastfeeding support in an Australian outer metropolitan region. Women Birth 2014, 27, 259–265. [Google Scholar] [CrossRef]
- Harvard University. Making Caring Common Project. Available online: https://mcc.gse.harvard.edu/reports/children-mean-raise (accessed on 9 October 2019).
- Gilbert, P.; McEwan, K.; Matos, M.; Rivis, A. Fears of compassion: Development of three self-report measures. Psychol. Psychother. Theory Res. Pract. 2010, 84, 239–255. [Google Scholar] [CrossRef] [PubMed]
- Neff, K. The development and validation of a scale to measure self-compassion. Self Identity 2003, 2, 223–250. [Google Scholar] [CrossRef]

© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).