
Benzodiazepine Boom: Tracking Etizolam, Pyrazolam, and Flubromazepam from Pre-UK Psychoactive Act 2016 to Present Using Analytical and Social Listening Techniques

 ,
,  , , ,
, , ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Forensic Analyses
2.1.1. Reference Materials and Reagents
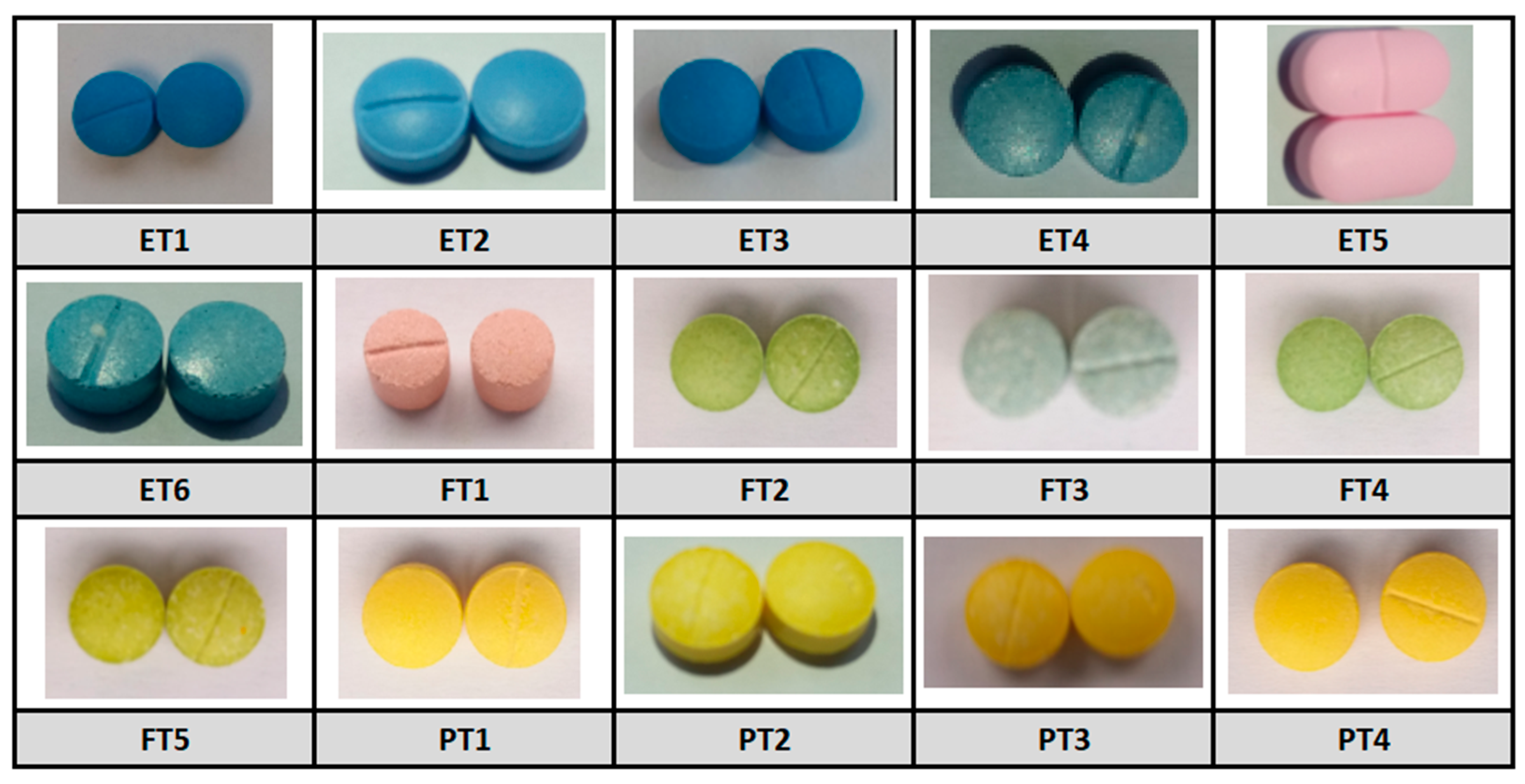
2.1.2. Drug Samples
2.1.3. UHPLC-MS
2.1.4. 1H NMR
2.1.5. Sample Analysis
2.2. Netnographic Methods
2.2.1. Primary Data Search
- X Search: Using the X search function, several broad date range operators (1 January–31 December 2016–2022 and 1 January–15 May 2023) were applied, using a single search term, in each case the name of the drug compound, i.e., etizolam, flubromazepam, or pyrazolam. Additional filtering criteria were applied to include tweets (X posts) in English and exclude re-tweets.
- Reddit Search: Using the Reddit search function, single search terms were applied, in each case the name of the drug compound, i.e., etizolam, flubromazepam, or pyrazolam. Every thread identified through the applied searches were reviewed, and all relevant posts recorded within the target date range (1 January–31 December 2016 up to 15 May 2023) were included for analysis; posts falling outside of the timeframe were discarded. Additional filtering criteria, including duplicates analysis and thread re-posts, were applied manually, using Microsoft 365 Excel (version no. 2311, 2023).
2.2.2. Data Cleaning
2.2.3. Data Analyses
- Manual Discussion/Theme Analysis: Each post was assessed for keywords and identified themes. Any key words/origination sources matching the experimental inclusion criteria were recorded for quantitative purposes. Any content found to bridge multiple topics was included in each associated theme.
- Numerous.ai Analysis. All cleaned data sets were exported to Google sheets for analysis within their annual grouping, for example, 1 January 2017 to 31 December 2017. Due to the program’s restrictions on the numbers of characters per data set, in terms of both input and output [36], it was necessary to further group the annual data sets into subsets of 10. Using a blank cell adjacent to the data, the following command prompt was typed into that cell, [=ai (“i want you to act as an expert in qualitative content analysis and analyse this post for me. Identify all the themes and then present them in bullet points. Please also consider any potential biases or contextual factors that may impact your analysis”)], followed by the manual selection of the cell subset range within the spreadsheet to be analysed. Each set of numerous.ai responses was captured, cut and pasted into a Microsoft 365 Word (Version no. 2311, 2023) document in preparation for ChatGPT analysis.
- ChatGPT Analysis: Analytical functionality on ChatGPT is less restricted in terms of character input and output; therefore, using ChatGPT version 3.5, we were able to group all numerous.ai responses, per drug, into three individual drug-specific Microsoft Word (version no. 2311. 2023) documents for analysis. To process the numerous.ai responses, we typed the following input into each Word document: [“could you resume the 5 most frequent themes/biases among these; and rank these is order or prevalence?”]. This resulted in the five most common themes and biases being identified by the application of this dual-AI method. The responses were then collated using Microsoft 365 Word (version no. 2023), for final assessment and inclusions.
3. Results
3.1. UHPLC-MS
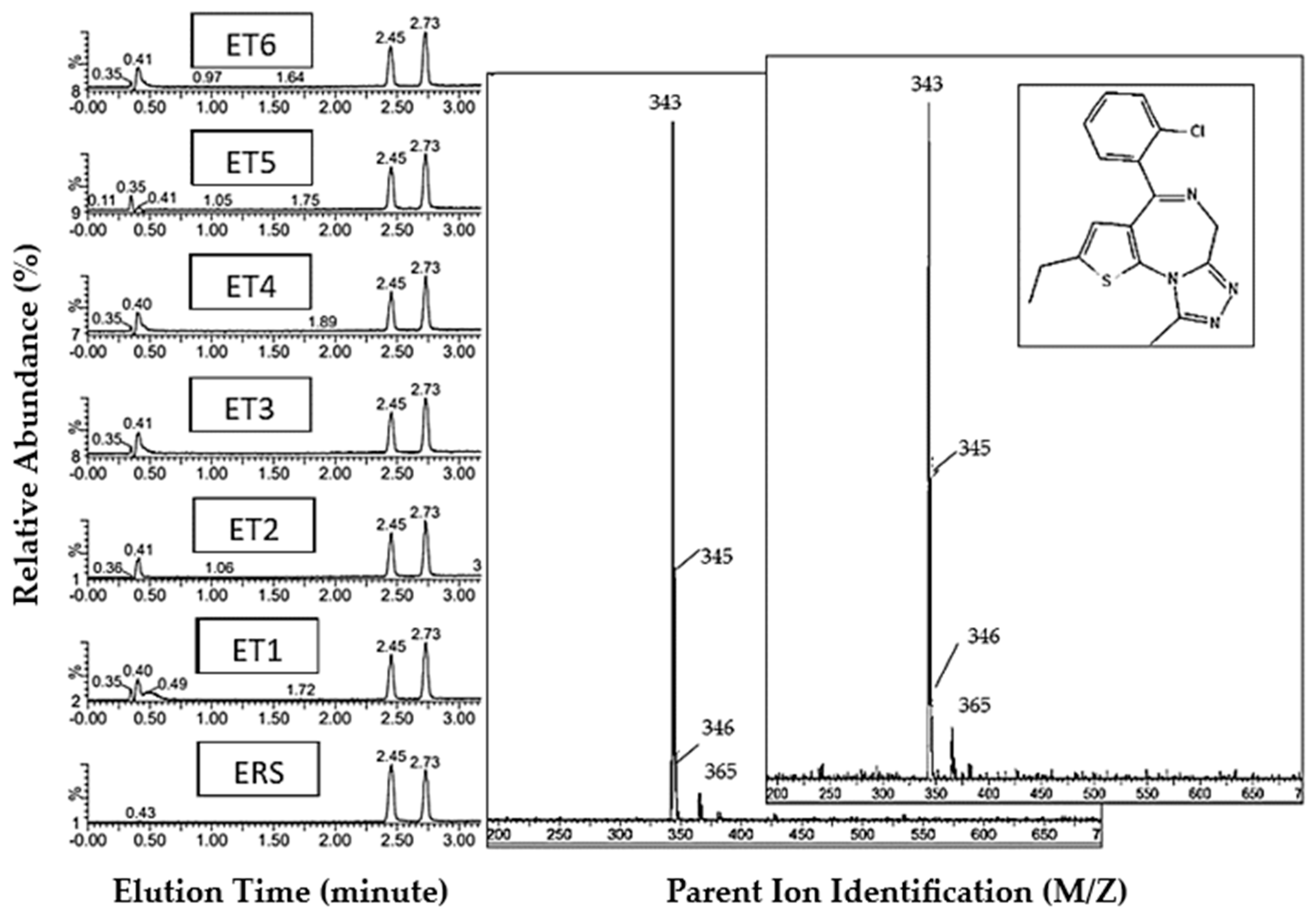
3.1.1. Etizolam Reference Standard and ET1-6 Tablets
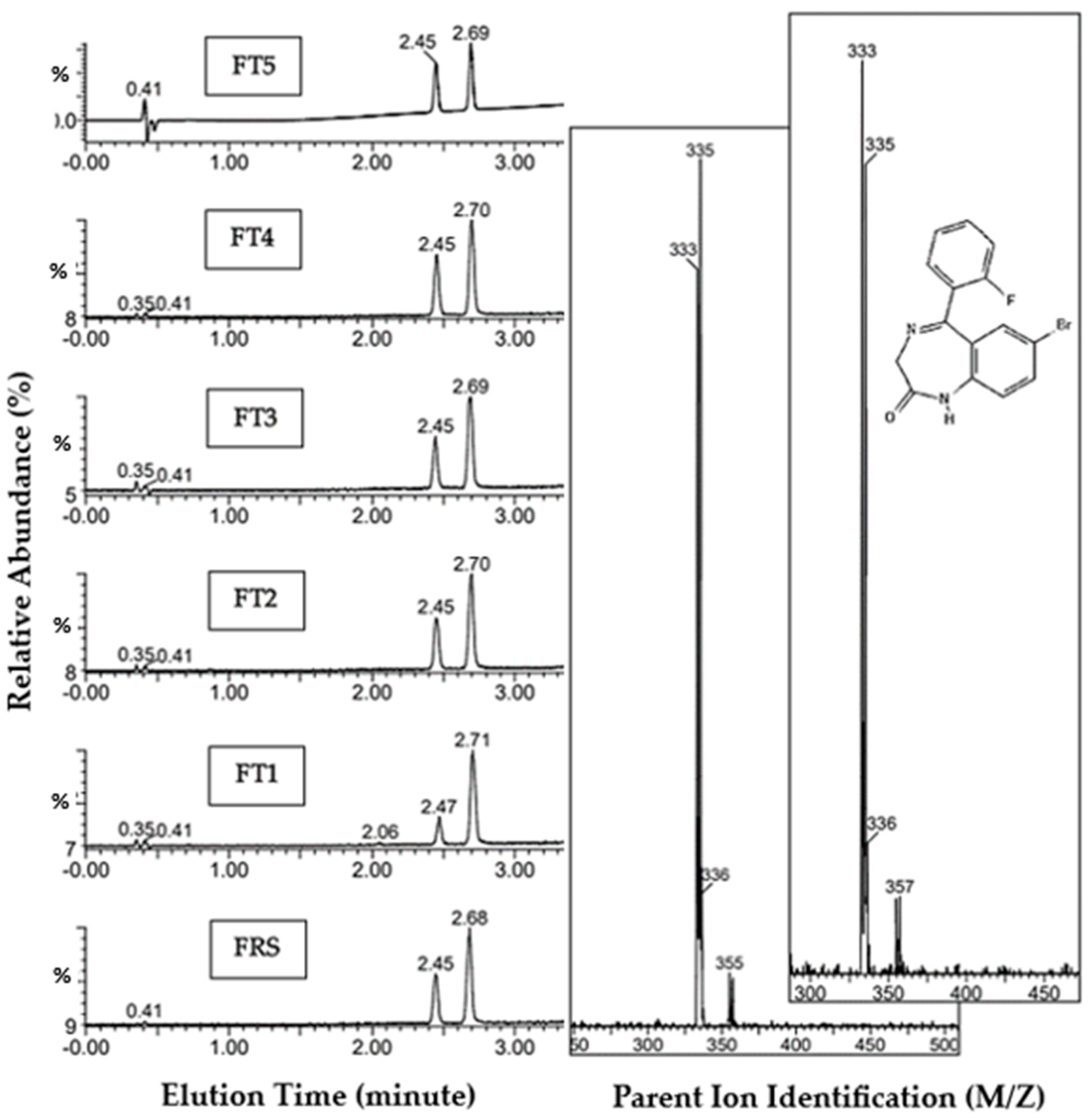
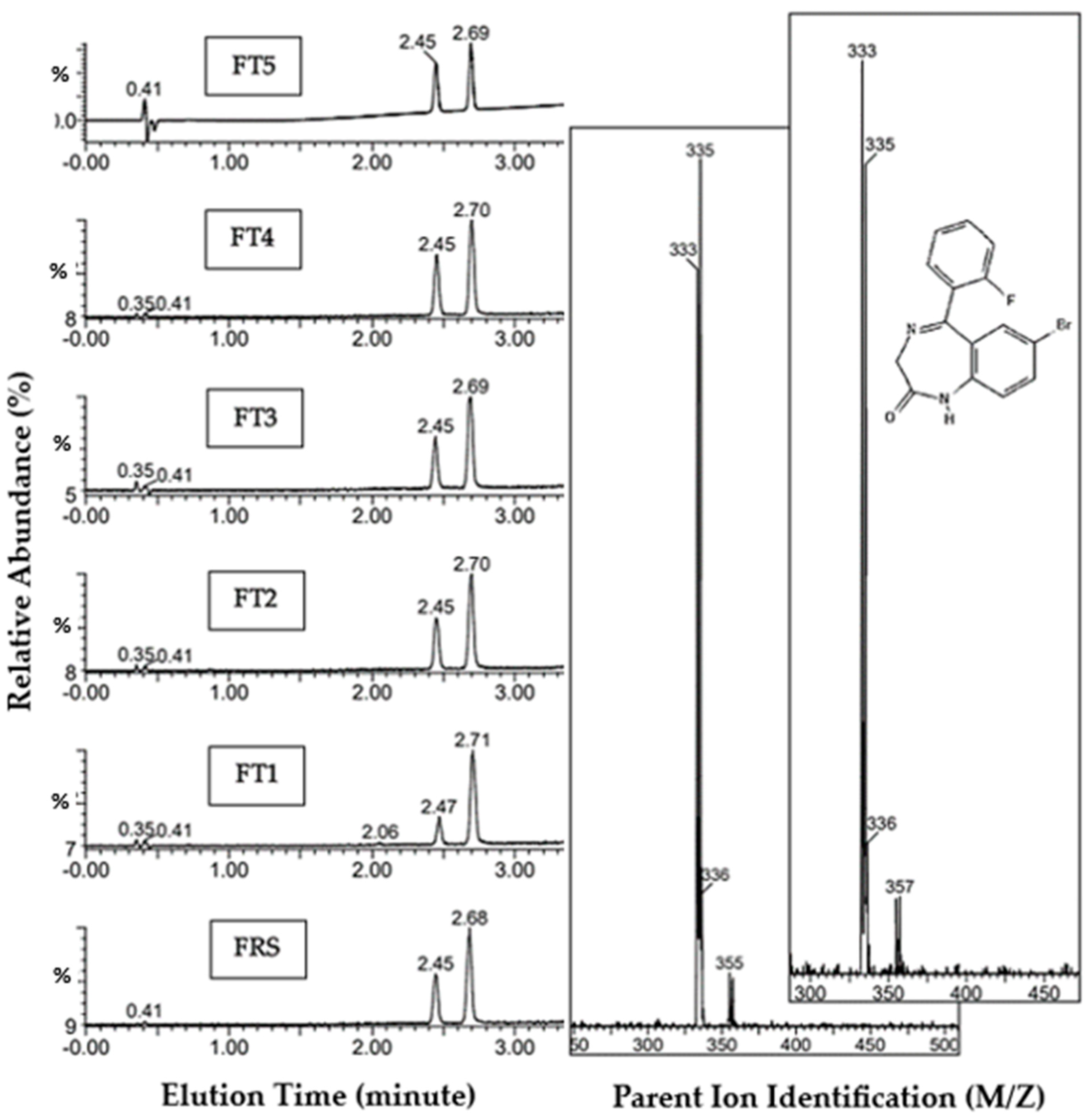
3.1.2. Flubromazepam Reference Standard and FT1-5 Tablets
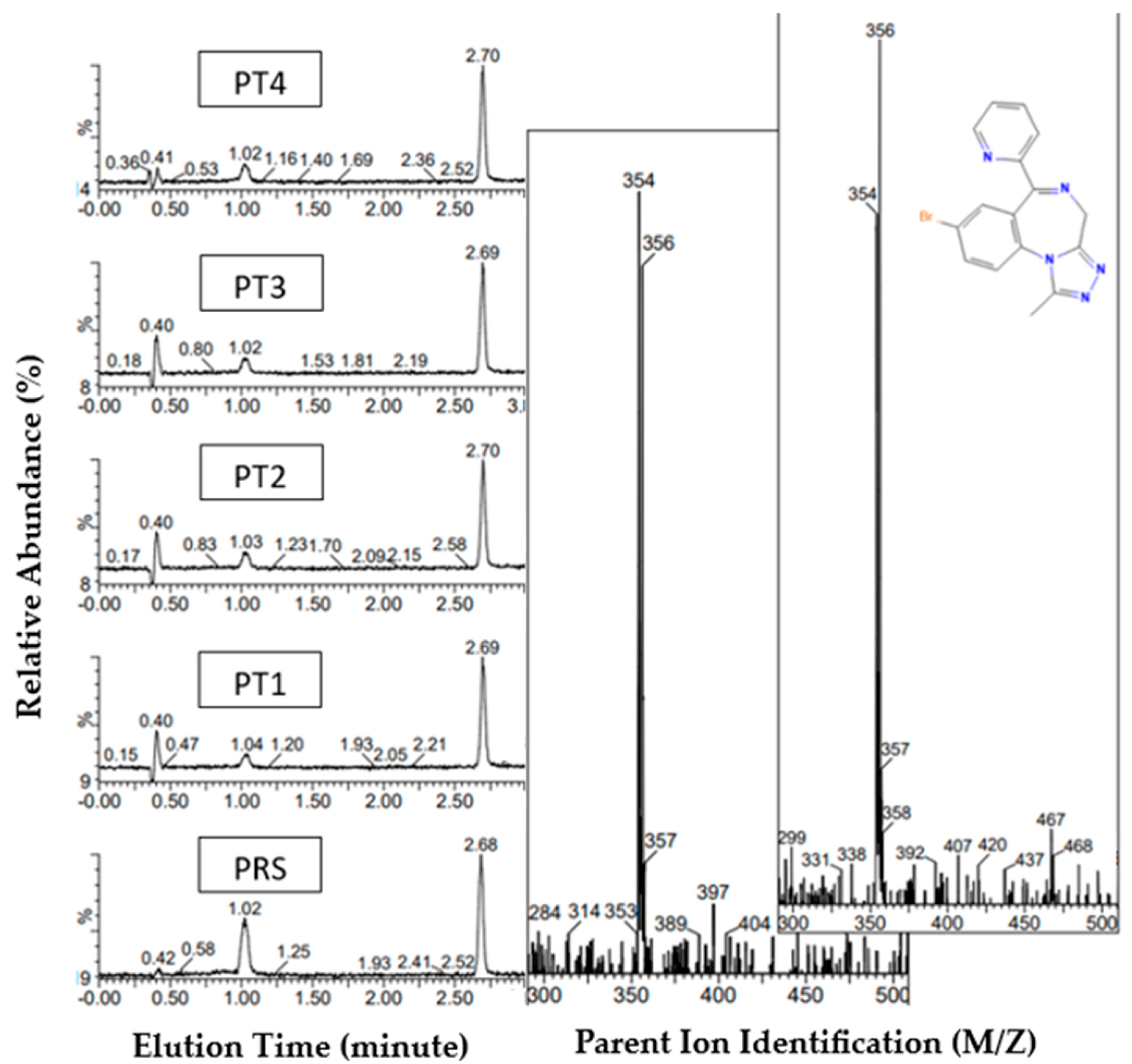
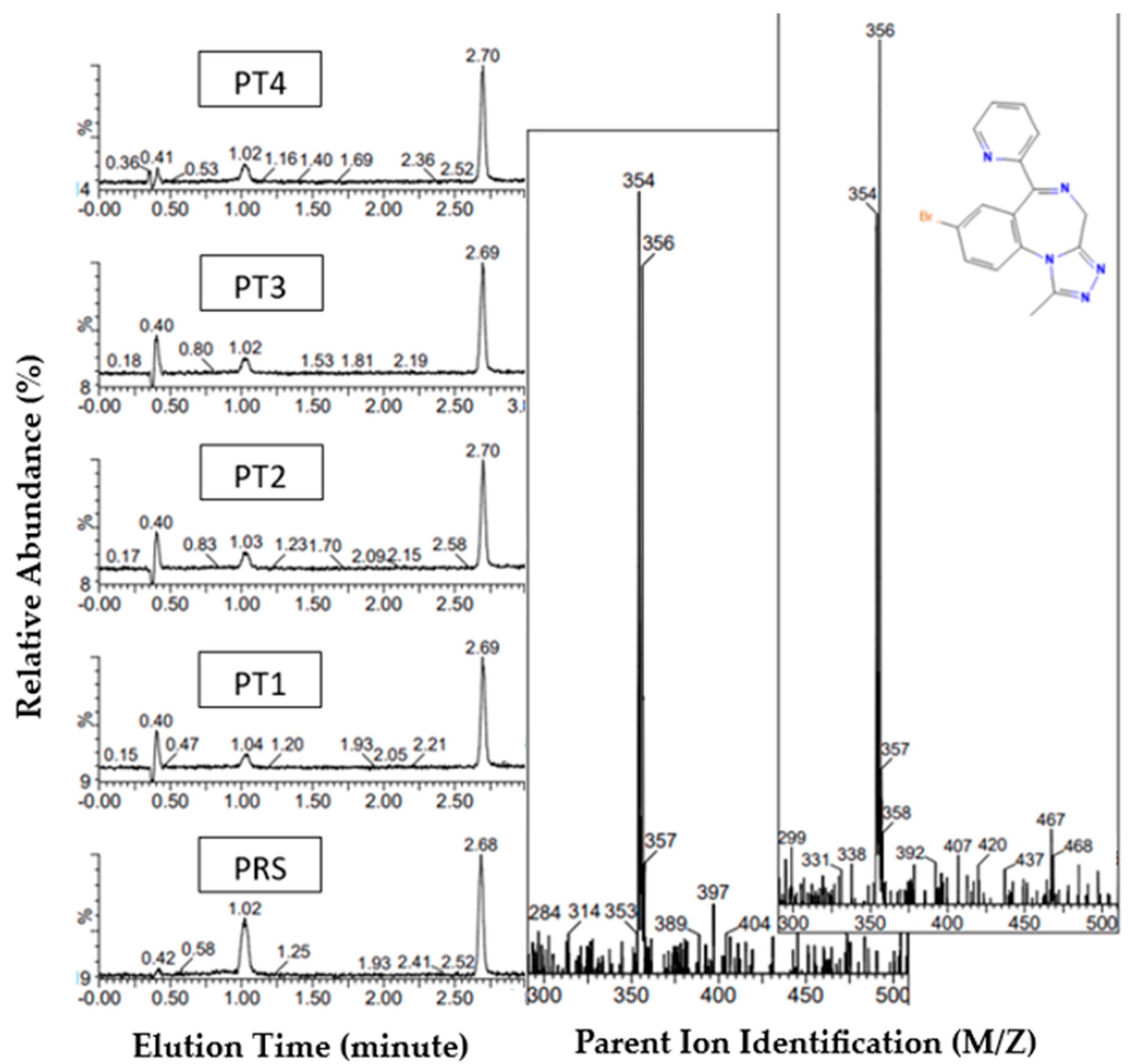
3.1.3. Pyrazolam Reference Standard and PT1-4 Tablets
3.2. 1H NMR Discussion
3.2.1. Etizolam
3.2.2. Flubromazepam
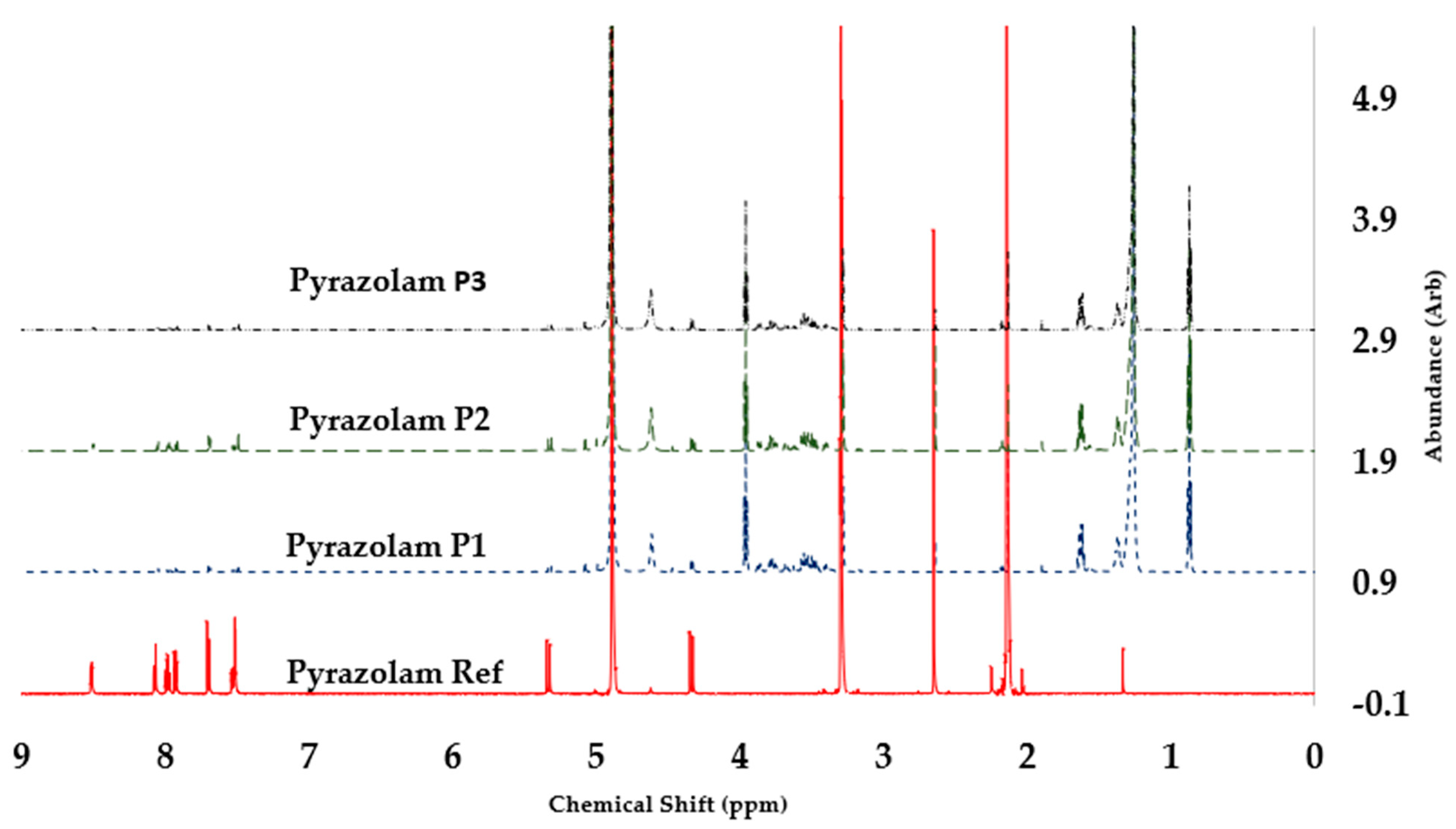
3.2.3. Pyrazolam
3.3. Quantitative Netnographic Analysis
3.3.1. Manual Qualitative and Quantitative Thematic Analysis
3.3.2. AI-Driven Qualitative and Quantitative Thematic Analysis
4. Discussion and Conclusions
5. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- EMCDDA (European Monitoriing Centre for Drugs and Drug Addiction). European Drug Report 2021: Trends and Developments; EMCDDA: Luxembourg, 2021; Available online: https://www.emcdda.europa.eu/publications/edr/trends-developments/2021_en (accessed on 6 December 2023).
- UNODC. World Drug Report 2023. (United Nations Publication, 2023). 2023. Available online: https://www.unodc.org/res/WDR-2023/WDR23_Exsum_fin_SP.pdf (accessed on 9 September 2023).
- Kleinman, R.A.; Weiss, R.D. Benzodiazepine-involved overdose deaths in the USA: 2000–2019. J. Gen. Intern. Med. 2022, 37, 2103–2109. [Google Scholar] [CrossRef] [PubMed]
- Tori, M.E.; Larochelle, M.R.; Naimi, T.S. Alcohol or benzodiazepine co-involvement with opioid overdose deaths in the United States, 1999–2017. JAMA Netw. Open 2020, 3, e202361. [Google Scholar] [CrossRef]
- National Records of Scotland (NRS). Drug-Related Deaths in Scotland in 2021; National Records of Scotland: Edinburgh, UK, 28 July 2022. Available online: https://www.nrscotland.gov.uk/files/statistics/drug-related-deaths/21/drug-related-deaths-21-report.pdf (accessed on 17 October 2023).
- National Records of Scotland (NRS). Drug-Related Deaths in Scotland in 2022; National Records of Scotland: Edinburgh, UK, 22 August 2023. Available online: https://www.nrscotland.gov.uk/files//statistics/drug-related-deaths/22/drug-related-deaths-22-report.pdf (accessed on 17 October 2023).
- Corkery, J.M.; Guirguis, A.; Chiappini, S.; Martinotti, G.; Schifano, F. Alprazolam-related deaths in Scotland, 2004–2020. J. Psychopharmacol. 2022, 36, 1020–1035. [Google Scholar] [CrossRef]
- Jones, C.M.; McAninch, J.K. Emergency department visits and overdose deaths from combined use of opioids and benzodiazepines. Am. J. Prev. Med. 2015, 49, 493–501. [Google Scholar] [CrossRef]
- White, J.M.; Irvine, R.J. Mechanisms of fatal opioid overdose. Addiction 1999, 94, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.D.; Mogali, S.; Comer, S.D. Polydrug abuse: A review of opioid and benzodiazepine combination use. Drug Alcohol Depend. 2012, 125, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Griffin, C.E.; Kaye, A.M.; Bueno, F.R.; Kaye, A.D. Benzodiazepine pharmacology and central nervous system–mediated effects. Ochsner J. 2013, 13, 214–223. [Google Scholar] [PubMed]
- Orsolini, L.; Corkery, J.M.; Chiappini, S.; Guirguis, A.; Vento, A.; De Berardis, D.; Papanti, D.; Schifano, F. ‘New/Designer Benzodiazepines’: An analysis of the literature and psychonauts’ trip reports. Curr. Neuropharmacol. 2020, 18, 809–837. [Google Scholar] [CrossRef]
- Singer, J.A. Will US Drug Policymakers Blow It Again—This Time with Benzodiazepines? CATO Institute: Washington, DC, USA, 2019; Available online: https://www.cato.org/blog/will-us-drug-policymakers-blow-it-again-time-benzodiazepines (accessed on 20 October 2023).
- Moosmann, B.; King, L.A.; Auwärter, V. Designer benzodiazepines: A new challenge. World Psychiatry 2015, 14, 248. [Google Scholar] [CrossRef]
- Di Trana, A.; Berardinelli, D.; Montanari, E.; Berretta, P.; Basile, G.; Huestis, M.A.; Busardò, F.P. Molecular Insights and Clinical Outcomes of Drugs of Abuse Adulteration: New Trends and New Psychoactive Substances. Int. J. Mol. Sci. 2022, 23, 14619. [Google Scholar] [CrossRef]
- EMCDDA (European Monitoring Centre for Drugs and Drug Addiction). Timeline of Benzodiazepines Formally Notified to the EU Early Warning System for the First Time, 2007–2020; EMCDDA: Luxembourg, 2021; Available online: www.emcdda.europa.eu (accessed on 9 October 2023).
- Home Office. Psychoactive Substance Act 2016; The Stationery Office Limited: Norwich, UK, 2016; Available online: http://services.parliament.uk/bills/2015-16/psychoactivesubstances.html (accessed on 20 October 2023).
- O’Connor, L.C.; Torrance, H.J.; McKeown, D.A. ELISA detection of phenazepam, etizolam, pyrazolam, flubromazepam, diclazepam and delorazepam in blood using Immunalysis® benzodiazepine kit. J. Anal. Toxicol. 2016, 40, 159–161. [Google Scholar] [CrossRef]
- Moosmann, B.; Huppertz, L.M.; Hutter, M.; Buchwald, A.; Ferlaino, S.; Auwärter, V. Detection and identification of the designer benzodiazepine flubromazepam and preliminary data on its metabolism and pharmacokinetics. J. Mass Spectrom. 2013, 48, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Moosmann, B.; Hutter, M.; Huppertz, L.M.; Ferlaino, S.; Redlingshöfer, L.; Auwärter, V. Characterization of the designer benzodiazepine pyrazolam and its detectability in human serum and urine. Forensic Toxicol. 2013, 31, 263–271. [Google Scholar] [CrossRef]
- Schmid, M.G. Optical Detection of NPS Internet Products via HPLC-DAD Systems: A Selective Review. In Light in Forensic Science: Issues and Applications; Royal Society of Chemistry: London, UK, 2018; pp. 301–332. ISBN 978-1-78262-768-5. [Google Scholar]
- Home Office. Review of the Psychoactive Act 2016; Home Office: London, UK, 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/756896/Review_of_the_Psychoactive_Substances_Act__2016___web_.pdf (accessed on 9 September 2023).
- Sarker, A.; Al-Garadi, M.A.; Ge, Y.; Nataraj, N.; McGlone, L.; Jones, C.M.; Sumner, S.A. Evidence of the emergence of illicit benzodiazepines from online drug forums. Eur. J. Public Health 2022, 32, 939–941. [Google Scholar] [CrossRef] [PubMed]
- Arillotta, D.; Guirguis, A.; Corkery, J.M.; Scherbaum, N.; Schifano, F. COVID-19 pandemic impact on substance misuse: A social media listening, mixed method analysis. Brain Sci. 2021, 11, 907. [Google Scholar] [CrossRef] [PubMed]
- Catalani, V.; Arillotta, D.; Corkery, J.M.; Guirguis, A.; Vento, A.; Schifano, F. Identifying New/Emerging Psychoactive Substances at the Time of COVID-19; A Web-Based Approach. Front. Psychiatry 2011, 11, 632405. [Google Scholar] [CrossRef]
- Priya, S.; Sequeira, R.; Chandra, J.; Dandapat, S.K. Where should one get news updates: X or Reddit. Online Soc. Netw. Media 2019, 9, 17–29. [Google Scholar] [CrossRef]
- Dean, B. Reddit Users and Growth Stats; BacklinKo: Cheyenne, WY, USA, 2023; Available online: https://backlinko.com/reddit-users (accessed on 24 October 2023).
- Dean, B. How Many People Use Twitter in 2023; BacklinKo: Cheyenne, WY, USA, 2023; Available online: https://backlinko.com/twitter-users (accessed on 24 October 2023).
- Seaman, I.; Giraud-Carrier, C. Prevalence and attitudes about illicit and prescription drugs on Twitter. In Proceedings of the 2016 IEEE International Conference on Healthcare Informatics (ICHI), Chicago, IL, USA, 4–7 October 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 14–17. [Google Scholar]
- European Medicines Agency (EMA). ICH Harmonised Guideline: Validation of Analytical Procedures—Q2(R2). 2022. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-guideline-q2r2-validation-analytical-procedures-step-2b_en.pdf (accessed on 17 October 2023).
- Food and Drug Administration (FDA). Analytical Procedures and Methods Validation for Drugs and Biologics. 2015. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/analytical-procedures-and-methods-validation-drugs-and-biologics (accessed on 17 October 2023).
- X Fair Usage Policy. 2023. Available online: https://help.X.com/en/rules-and-policies/fair-use-policy (accessed on 25 August 2023).
- Reddit. Reddit User Agreement. 2023. Available online: https://www.redditinc.com/policies/user-agreement (accessed on 25 August 2023).
- Numerous.ai. Numerous.ai Internet Analysis Tool. 2023. Available online: https://numerous.ai/ (accessed on 7 September 2023).
- ChatGPT. ChatGPT Internet Analysis Tool. 2023. Available online: https://openai.com/chatgpt (accessed on 7 September 2023).
- Wankhede, C. Does ChatGPT Have a Character Limit? Here’s How to Bypass It. 2023. Available online: https://www.androidauthority.com/chatgpt-character-limit-3292997/ (accessed on 9 September 2023).
- Cayman Chemicals. Etizolam Monograph. 2023. Available online: https://cdn.caymanchem.com/cdn/gcms/12063-0480732-GCMS.pdf (accessed on 11 October 2023).
- Mullin, A.; Scott, M.; Vaccaro, G.; Gittins, R.; Ferla, S.; Schifano, F.; Guirguis, A. Handheld Raman Spectroscopy in the First UK Home Office Licensed Pharmacist-Led Community Drug Checking Service. Int. J. Environ. Res. Public Health 2023, 20, 4793. [Google Scholar] [CrossRef]
- Cayman Chemicals. Flubromazepam Monograph. 2023. Available online: https://cdn.caymanchem.com/cdn/gcms/15157-0570041-GCMS.pdf (accessed on 11 October 2023).
- Gundersen, P.O.M.; Broecker, S.; Slørdal, L.; Spigset, O.; Josefsson, M. Retrospective screening of synthetic cannabinoids, synthetic opioids and designer benzodiazepines in data files from forensic postmortem samples analysed by UHPLC-QTOF-MS from 2014 to 2018. Forensic Sci. Int. 2020, 311, 110274. [Google Scholar] [CrossRef]
- Cayman Chemicals. Pyrazolam Monograph. 2023. Available online: https://cdn.caymanchem.com/cdn/gcms/14901-0455692-GCMS.pdf (accessed on 11 October 2023).
- SWGDRUG. Etizolam. 2023. Available online: https://www.swgdrug.org/Monographs/Etizolam.pdf (accessed on 11 October 2023).
- Ligon, E.S.; Nawyn, J.; Jones, L.V.; Allred, B.M.; Reinhardt, D.V., Jr.; France, S. Synthesis of Flubromazepam Positional Isomers for Forensic Analysis. J. Org. Chem. 2019, 84, 10280–10291. [Google Scholar] [CrossRef]
- Abouchedid, R.; Gilks, T.; Dargan, P.I.; Archer, J.R.; Wood, D.M. Assessment of the availability, cost, and motivations for use over time of the new psychoactive substances—Benzodiazepines diclazepam, flubromazepam, and pyrazolam—In the UK. J. Med. Toxicol. 2018, 14, 134–143. [Google Scholar] [CrossRef] [PubMed]
- EMCDDA (European Monitoring Centre for Drugs and Drug Addiction). European Legal Database on Drugs. 2011. Available online: http://www.emcdda.europa.eu/eldd (accessed on 9 October 2023).
- EMCDDA (European Monitoring Centre for Drugs and Drug Addiction). 2021a (2021) New benzodiazepines in Europe—A review; EMCDDA: Luxemburg, 2021; Available online: https://www.emcdda.europa.eu/publications/rapid-communications/new-benzodiazepines-europe-review_en (accessed on 9 October 2023).
- ACMD (Advisory Council on the Misuse of Drugs). Novel Benzodiazepines. A Review of Evidence of Use and Harms of Novel Benzodiazepines. 2020. Available online: https://assets.publishing.service.gov.uk/media/5ea95a1cd3bf7f6523c81c01/ACMD_report_-_a_review_of_the_evidence_of_use_and_harms_of_novel_benzodiazepines.pdf (accessed on 11 October 2023).
- UNODC Laboratory and Scientific Service Portals. Twelve Substances and One Precursor “Scheduled” at the 63rd Session of the Commission on Narcotic Drugs. 2020. Available online: https://www.unodc.org/LSS/Announcement/Details/165b82de-e7ef-4a92-8614-9f8ad4819083 (accessed on 6 December 2023).
- Fracasso, C.; Confalonieri, S.; Garattini, S.; Caccia, S. Single and multiple dose pharmacokinetics of etizolam in healthy subjects. Eur. J. Clin. Pharmacol. 1991, 40, 181–185. [Google Scholar] [CrossRef] [PubMed]
- DGHSC (Director General Health and Social Care). Benzodiazepine Use—Current Trends: Evidence Review; Scottish Government: Edinburgh, UK, 2022. Available online: https://www.gov.scot/publications/evidence-review-current-trends-benzodiazepine-use-scotland/pages/3/ (accessed on 11 October 2023).
- Sternbach, L.H.; Fryer, R.Y.; Metlesics, W.; Reeder, E.; Sach, G.; Saucy, G.; Stempel, G. Quinazolines and 1,4-Benzodiazepines. VI.1a Halo-, Methyl-, and Methoxy-substituted 1,3-Dihydro-5-phenyl-2H-1,4-benzodiazepin-2-ones1b,c. J. Org. Chem. 1962, 27, 3788. [Google Scholar] [CrossRef]
- Stahl, S.M. Essential psychopharmacology: Neuroscientific basis and practical applications. In Stahl’s Essential Psychopharmacology. Neuroscientific Basis and Practical Applications, 5th ed.; Cambridge University Press: San Diego, CA, USA, 2021; ISBN 9781108838573. [Google Scholar]
- Edinoff, A.N.; Nix, C.A.; Odisho, A.S.; Babin, C.P.; Derouen, A.G.; Lutfallah, S.C.; Cornett, E.M.; Murnane, K.S.; Kaye, A.M.; Kaye, A.D. Novel designer benzodiazepines: Comprehensive review of evolving clinical and adverse effects. Neurol. Int. 2022, 14, 648–663. [Google Scholar] [CrossRef] [PubMed]
- SpectraBase. Etizolam. 2023. Available online: https://spectrabase.com/compound/FXsiIsWI1Tn (accessed on 11 October 2023).
- SWGDRUG. Flubromazepam. 2023. Available online: https://www.swgdrug.org/Monographs/Flubromazepam.pdf (accessed on 11 October 2023).
- SpectraBase. Flubromazepam. 2023. Available online: https://spectrabase.com/compound/6ohTApdCf (accessed on 11 October 2023).
- PubChem. Pyrazolam. 2023. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Pyrazolam#section=FTIR-Spectra (accessed on 11 October 2023).
- SpectraBase. Pyrazolam. 2023. Available online: https://spectrabase.com/compound/DtfWZ5VhSzm (accessed on 11 October 2023).
- Statistica. Social Media Use During COVID-19 World-Wide—Statistics & Facts. 2020. Available online: https://www.statista.com/topics/7863/social-media-use-during-coronavirus-covid-19-worldwide/#topicOverview (accessed on 11 October 2023).
- Shapiro, A.P.; Krew, T.S.; Vazirian, M.; Jerry, J.; Sola, C. Novel ways to acquire designer benzodiazepines: A case report and discussion of the changing role of the internet. Psychosomatics 2019, 60, 625–629. [Google Scholar] [CrossRef]
- Littlejohn, C.; Baldacchino, A.; Schifano, F.; Deluca, P. Internet pharmacies and online prescription drug sales: A cross-sectional study. Drugs: Educ. Prev. Policy 2005, 12, 75–80. [Google Scholar] [CrossRef]
- Kim, S.J.; Marsch, L.A.; Hancock, J.T.; Das, A.K. Scaling up research on drug abuse and addiction through social media big data. J. Med. Internet Res. 2017, 19, e353. [Google Scholar] [CrossRef]
- Pandrekar, S.; Chen, X.; Gopalkrishna, G.; Srivastava, A.; Saltz, M.; Saltz, J.; Wang, F. Social media-based analysis of opioid epidemic using Reddit. In AMIA Annual Symposium Proceedings; American Medical Informatics Association: Bethesda, MD, USA, 2018; Volume 2018, p. 867. [Google Scholar]
- Sarker, A.; O’connor, K.; Ginn, R.; Scotch, M.; Smith, K.; Malone, D.; Gonzalez, G. Social media mining for toxicovigilance: Automatic monitoring of prescription medication abuse from Twitter. Drug Saf. 2016, 39, 231–240. [Google Scholar] [CrossRef]
- EMCDDA (European Monitoring Centre for Drugs and Drug Addiction). Drug-Related Deaths and Mortality in Europe; EMCDDA: Luxembourg, 2021; Available online: https://www.emcdda.europa.eu/publications/meeting-reports-and-conference-proceedings/drug-related-deaths-and-mortality-europe_en (accessed on 9 October 2023).
- Guirguis, A.; Girotto, S.; Berti, B.; Stair, J.L. Identification of new psychoactive substances (NPS) using handheld Raman spectroscopy employing both 785 and 1064 nm laser sources. Forensic Sci. Int. 2017, 273, 113–123. [Google Scholar] [CrossRef]
- McAuley, A. The Role of Etizolam in Scottish Drug-Related Deaths; Glasgow Caledonian University: Glasgow, UK, 2018; Available online: https://www.emcdda.europa.eu/system/files/attachments/12056/3.2%20Andy%20McAuley_DRD_NPS%20Benzo.pptx.pdf (accessed on 11 October 2023).
- WEDINOS (Welsh Emerging Drugs & Identification of Novel Substances). Annual Report April 2022–March 2023. 2023. Available online: https://www.wedinos.org/resources/downloads/Annual-Report-22-23-English.pdf (accessed on 12 October 2023).
- Coleman, J.J. Benzodiazepines Today and Tomorrow. In The Benzodiazepines Crisis; Peppin, J., Pergolizzi, J.V., Raffa, R.B., Wright, S.L., Eds.; Oxford University Press: Oxford, UK, 2020; Online ISBN 9780197517307, Print ISBN 9780197517277. [Google Scholar] [CrossRef]
- Gevorkyan, J.; Kinyua, J.; Pearring, S.; Rodda, L.N. A case series of etizolam in opioid-related deaths. J. Anal. Toxicol. 2021, 45, e4–e17. [Google Scholar] [CrossRef]
- Laing, M.K.; Ti, L.; Marmel, A.; Tobias, S.; Shapiro, A.M.; Laing, R.; Lysyshyn, M.; Socías, M.E. An outbreak of novel psychoactive substance benzodiazepines in the unregulated drug supply: Preliminary results from a community drug checking program using point-of-care and confirmatory methods. Int. J. Drug Policy 2021, 93, 103169. [Google Scholar] [CrossRef] [PubMed]
- Papsun, D.M.; Chan-Hosokawa, A.; Lamb, M.E.; Logan, B. Increasing Prevalence of Designer Benzodiazepines in Impaired Driving; a 5 Year Analysis from 2017–2021. J. Anal. Toxicol. 2023, 47, 668–679. [Google Scholar] [CrossRef] [PubMed]
- National Records of Scotland (NRS). Drug-Related Deaths in Scotland in 2020; National Records of Scotland: Edinburgh, UK, 2020. Available online: https://www.nrscotland.gov.uk/statistics-and-data/statistics/statistics-by-theme/vital-events/deaths/drug-related-deaths-in-scotland/2020 (accessed on 6 December 2023).
- Busardò, F.P.; Di Trana, A.; Montanari, E.; Mauloni, S.; Tagliabracci, A.; Giorgetti, R. Is etizolam a safe medication? Effects on psychomotor perfomance at therapeutic dosages of a newly abused psychoactive substance. Forensic Sci. Int. 2019, 301, 137–141. [Google Scholar] [CrossRef] [PubMed]
- National Records of Scotland (NRS). Drug-Related Deaths in Scotland in 2019; National Records of Scotland: Edinburgh, UK, 2019. Available online: https://www.nrscotland.gov.uk/statistics-and-data/statistics/statistics-by-theme/vital-events/deaths/drug-related-deaths-in-scotland/2019 (accessed on 17 October 2023).
- WEDINOS (Welsh Emerging Drugs & Identification of Novel Substances). Annual Report April 2019–March 2020. 2020. Available online: https://www.wedinos.org/resources/downloads/WEDINOS-results-161220.pdf (accessed on 12 October 2023).
- Dikeos, D.; Theleritis, C.G.; Soldatos, C.R. (Eds.) Benzodiazepines: An overview. In Sleep Disorders: Diagnosis and Therapeutics, 1st ed.; CRC Press: Boca Raton, FL, USA, 2008; Chapter 10; pp. 116–124. ISBN 9780429075254. [Google Scholar]
- WEDINOS (Welsh Emerging Drugs & Identification of Novel Substances). Annual Report April 2021–March 2022. 2022. Available online: https://www.wedinos.org/resources/downloads/Annual-Report-21-22-English.pdf (accessed on 12 October 2023).
- Reddit. Flubromazepam vs. Flubromazolam. 2017. Available online: https://www.reddit.com/r/researchchemicals/comments/4ifzlb/flubromazepam_vs_flubromazolam/ (accessed on 12 October 2023).
- Reddit. Flubromazepam vs. Flubromazolam. 2022. Available online: https://www.reddit.com/r/researchchemicals/comments/vxei0l/popular_rc_benzo_pyrazolam_dangerously_wrong_dose/ (accessed on 12 October 2023).
- Marland, V.; Reid, R.; Brandon, A.; Hill, K.; Cruickshanks, F.; McKenzie, C.; Norman, C.; Nic Daéid, N.; Menard, H. Changing trends in novel benzodiazepine use within Scottish prisons: Detection, quantitation, prevalence, and modes of use. Drug Test. Anal. 2023. [Google Scholar] [CrossRef]
- Rousis, N.; Li, Z.; Bade, R.; McLachlan, M.; Mueller, J.; O’Brien, J.; Samanipour, S.; Tscharke, B.; Thomaidis, N.; Thomas, K. Socioeconomic Status and Public Health in Australia: A Wastewater-Based Study. Environment International. 2022. Available online: https://api.semanticscholar.org/CorpusID:251121788 (accessed on 6 December 2023).
- Lyphout, C.; Yates, C.; Margolin, Z.R.; Dargan, P.I.; Dines, A.M.; Heyerdahl, F.; Hovda, K.E.; Giraudon, I.; Bucher-Bartelson, B.; Green, J.L. Presentations to the emergency department with non-medical use of benzodiazepines and Z-drugs: Profiling and relation to sales data. Eur. J. Clin. Pharmacol. 2019, 75, 77–85. [Google Scholar] [CrossRef]
- Ramos, T.B.; Bokehi, L.C.; Oliveira, E.B.D.; Gomes, M.D.S.A.; Bokehi, J.R.; Castilho, S.R.D. Information about benzodiazepines: What does the internet offer us? Ciência Saúde Coletiva 2020, 25, 4351–4360. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Terms | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Etizolam, flubromazepam, and pyrazolam | Tweets and Reddit threads posted in English | Tweets and Reddit threads posted in another language other than English |
|
| |
|
| |
|
| |
|
|
| Drug Sample ID * | UHPLC-MS | 1H-NMR (600 MHz, METHANOL-D4) | |||||
|---|---|---|---|---|---|---|---|
| Drug Compound Retention Time (min) | Molecular Mass (m/z) | Base Peak (m/z) | Collection of Molecular Ions and Adducts | Confirmed ID * Using Literature (Cayman Chemical) | J Couplings Report | Confirmed ID * (Ref Std ** or Literature) | |
| ERS | 2.45 | 342.8 | 343 | 343, 345, 346 | Etizolam | δ 7.52–7.42 (m, 4H), 6.47 (d, J = 1.4 Hz, 1H), 4.92–4.87 (m, 7H), 3.31–3.30 (m, 3H), 2.86–2.81 (m, 2H), 2.73–2.69 (m, 3H), 1.28 (t, J = 7.6 Hz, 3H) | Etizolam not confirmed |
| ET1 | 2.45 | 342.8 | 343 | 343, 345, 346, 365 | Etizolam | δ 7.51–7.40 (m, 4H), 6.45 (s, 1H), 4.48 (d, J = 7.6 Hz, 1H), 4.34 (d, J = 7.6 Hz, 2H), 2.82 (q, J = 7.6 Hz, 2H), 2.69 (s, 3H), 2.25 (t, J = 7.6 Hz, 2H), 2.13 (s, 2H) | Etizolam not confirmed |
| ET2 | 2.45 | 342.8 | 343 | 343, 345, 346, 365 | Etizolam | δ 7.51–7.40 (m, 4H), 6.45 (s, 1H), 4.48 (d, J = 7.6 Hz, 1H), 4.34 (d, J = 7.6 Hz, 2H), 3.18 (dd, J = 9.3, 7.9 Hz, 0H), 2.82 (q, J = 7.6 Hz, 2H), 2.69 (s, 3H), 2.25 (t, J = 7.6 Hz, 2H), 2.13 (s, 2H) | Etizolam not confirmed |
| ET3 | 2.45 | 342.8 | 343 | 343, 345, 346, 365 | Etizolam | δ 7.51–7.40 (m, 4H), 6.45 (d, J = 1.4 Hz, 1H), 4.48 (d, J = 7.6 Hz, 1H), 4.34 (d, J = 7.6 Hz, 2H), 3.18 (dd, J = 9.3, 7.9 Hz, 1H), 2.84–2.81 (m, 2H), 2.69 (s, 3H), 2.25 (t, J = 7.2 Hz, 2H) | Etizolam not confirmed |
| ET4 | 2.45 | 342.8 | 343 | 343, 345, 346, 365 | Etizolam | 7.52–7.42 (m, 4H), 6.47 (s, 1H), 2.84 (dd, J = 7.6, 1.4 Hz, 2H), 2.71 (s, 3H), 2.26 (t, J = 7.6 Hz, 3H), 2.04 (s, 0H), 1.92 (s, 1H), 1.58 (d, J = 7.6 Hz, 2H), 0.89 (t, J = 6.9 Hz, 4H) | Etizolam not confirmed |
| ET5 | 2.45 | 342.8 | 343 | 343, 345, 346, 365, 367 | Etizolam | δ 7.52–7.39 (m, 4H), 6.45 (s, 1H), 2.83 (q, 2H), 1.27 (s, 1H), 1.27–1.26 (m, 4H), 0.859–0.85 (2H) | Etizolam not confirmed |
| ET6 | 2.45 | 342.8 | 343 | 343, 345, 346, 365 | Etizolam | δ 7.50–7.40 (m, 4H), 6.45 (s, 1H), 3.60 (d, J = 28.2 Hz, 0H), 2.83 (q, J = 7.6 Hz, 2H), 2.69 (s, 3H), 2.18–2.14 (m, 3H), 1.57 (t, J = 7.2 Hz, 2H), 0.87 (t, J = 7.2 Hz, 3H) | Etizolam not confirmed |
| Sample ID * | Average Drug Content Tablet (mg) with Standard Deviation (mg) | Sample ID * | Average Drug Content Tablet (mg) with Standard Deviation (mg) | Sample ID * | Average Drug Content Tablet (mg) with Standard Deviation (mg) |
|---|---|---|---|---|---|
| ET1 B1 R1-3 | 21.8 ± 0.8 | ET6 B1 R1-3 | 21.7 ± 1.0 | FT5 B1 R1-3 | 22.7 ± 0.7 |
| ET1 B2 R1-3 | 24.7 ± 0.9 | ET6 B2 R1-3 | 22.8 ± 0.9 | FT5 B2 R1-3 | 23.5 ± 0.8 |
| ET1 B3 R1-3 | 23.6 ± 0.9 | ET6 B3 R1-3 | 22.1 ± 1.0 | FT5 B3 R1-3 | 23.4 ± 0.8 |
| ET2 B1 R1-3 | 24.8 ± 1.1 | FT1 B1 R1-3 | 4.5 ± 0.2 | PT1 B1 R1-3 | 5.4 ± 0.2 |
| ET2 B2 R1-3 | 24.6 ± 1.2 | FT1 B2 R1-3 | 4.0 ± 0.2 | PT1 B2 R1-3 | 8.2 ± 0.3 |
| ET2 B3 R1-3 | 23.4 ± 1.2 | FT1 B3 R1-3 | 4.3 ± 0.2 | PT1 B3 R1-3 | 6.0 ± 0.2 |
| ET3 B1 R1-3 | 21.0 ± 1.0 | FT2 B1 R1-3 | 14.2 ± 0.6 | PT2 B1 R1-3 | 11.1 ± 0.4 |
| ET3 B2 R1-3 | 21.5 ± 1.1 | FT2 B2 R1-3 | 22.2 ± 0.7 | PT2 B2 R1-3 | 10.2 ± 0.3 |
| ET3 B3 R1-3 | 20.7 ± 0.9 | FT2 B3 R1-3 | 20.7 ± 0.6 | PT2 B3 R1-3 | 7.1 ± 0.3 |
| ET4 B1 R1-3 | 23.6 ± 1.4 | FT3 B1 R1-3 | 9.3 ± 0.3 | PT3 B1 R1-3 | 8.5 ± 0.3 |
| ET4 B2 R1-3 | 23.9 ± 1.1 | FT3 B2 R1-3 | 8.6 ± 0.3 | PT3 B2 R1-3 | 9.6 ± 0.3 |
| ET4 B3 R1-3 | 24.7 ± 0.8 | FT3 B3 R1-3 | 9.0 ± 0.3 | PT3 B3 R1-3 | 11.0 ± 0.4 |
| ET5 B1 R1-3 | 15.2 ± 0.6 | FT4 B1 R1-3 | 19.1 ± 0.7 | PT4 B1 R1-3 | 10.2 ± 0.3 |
| ET5 B2 R1-3 | 13.8 ± 0.6 | FT4 B2 R1-3 | 22.6 ± 0.7 | PT4 B2 R1-3 | 11.5 ± 0.4 |
| ET5 B3 R1-3 | 14.2 ± 0.5 | FT4 B3 R1-3 | 21.4 ± 0.7 | PT4 B3 R1-3 | 10.6 ± 0.4 |
| Drug Sample ID * | UHPLC-MS | 1H-NMR (600 MHz, METHANOL-D4) | |||||
|---|---|---|---|---|---|---|---|
| Drug Compound Retention Time (min) | Molecular Mass (m/z) | Base Peak (m/z) | Collection of Molecular ions and adducts | Confirmed ID * Using Literature (Cayman Chemical) | J Couplings Report | Confirmed ID * (Ref Std ** or Literature) | |
| FRS | 2.45 | 333.15 | 333 | 333, 335, 336, 355 | Flubromazepam | δ 7.69–7.67 (m, 1H), 7.58–7.54 (m, 2H), 7.34–7.27 (m, 2H), 7.18–7.15 (m, 2H), 4.35–4.20 (s, 2H) | Flubromazepam identified |
| FT1 | 2.47 | 333.15 | 333 | 333, 335, 336, 357 | Flubromazepam | δ 7.67 (dd, J = 8.6, 2.4 Hz, 1H), 7.57–7.53 (m, 2H), 7.32–7.25 (m, 2H), 7.15 (t, J = 9.6 Hz, 2H), 4.26 (s, 2H), 2.17 (t, J = 7.6 Hz, 1H), 1.57 (s, 1H), 0.87 (t, J = 7.2 Hz, 1H)] | Flubromazepam identified |
| FT2 | 2.45 | 333.15 | 333 | 333, 335, 336, 357 | Flubromazepam | δ 7.66 (dd, J = 8.6, 2.4 Hz, 1H), 7.56–7.53 (m, 2H), 7.32–7.25 (m, 2H), 7.16–7.13 (m, 2H), 4.63 (s, 3H), 4.25 (s, 2H), 3.29 (t, J = 1.7 Hz, 1H), 1.27 (d, J = 17.2 Hz, 3H), 0.87 (d, J = 6.9 Hz, 0H) | Flubromazepam identified |
| FT3 | 2.44 | 333.15 | 333 | 333, 335, 336, 357 | Flubromazepam | δ 7.67 (dd, J = 8.6, 2.4 Hz, 1H), 7.57–7.53 (m, 2H), 7.32–7.25 (m, 2H), 7.16–7.13 (m, 2H), 4.63 (s, 4H), 4.26 (s, 2H), 2.13 (s, 0H), 1.29–1.26 (m, 5H), 0.87 (t, J = 6.9 Hz, 1H) | Flubromazepam identified |
| FT4 | 2.44 | 333.15 | 333 | 333, 335, 336, 357 | Flubromazepam | δ 7.66 (dd, J = 8.6, 2.4 Hz, 1H), 7.56–7.53 (m, 2H), 7.32–7.25 (m, 2H), 7.14 (t, J = 9.3 Hz, 2H), 4.63 (s, 2H), 4.25 (s, 2H), 1.27 (d, J = 17.2 Hz, 3H), 0.87 (d, J = 6.9 Hz, 0H) | Flubromazepam identified |
| FT4 | 2.45 | 333.15 | 333 | 333, 335, 336, 357 | Flubromazepam | δ 7.66 (dd, J = 8.9, 2.1 Hz, 1H), 7.55 (q, J = 6.9 Hz, 2H), 7.32–7.25 (m, 2H), 7.15 (dd, J = 10.3, 8.9 Hz, 2H), 4.63 (s, 3H), 4.25 (s, 2H), 1.26 (s, 2H), 0.87 (s, 0H) | Flubromazepam identified |
| Drug Sample ID * | UHPLC-MS | 1H-NMR (600 MHz, METHANOL-D4) | |||||
|---|---|---|---|---|---|---|---|
| Drug Compound Retention Time (min) | Molecular Mass (m/z) | Base Peak (m/z) | Collection of Molecular Ions and Adducts | Confirmed ID * Using Literature (Cayman Chemical) | J Couplings Report | Confirmed ID * (Ref Std ** or Literature) | |
| PRS | 1.02 | 354.2 | 354 | 117, 131, 141, 354, 356, 357 | Pyrazolam | δ 8.52 (q, J = 2.3 Hz, 1H), 8.08–7.92 (m, 3H), 7.70 (d, J = 8.2 Hz, 1H), 7.54–7.51 (m, 2H), 5.34 (d, J = 13.1 Hz, 1H), 4.34 (d, J = 13.1 Hz, 1H), 2.65 (s, 3H), 1.34 (s, 0H) | Pyrazolam identified |
| PT1 | 1.02 | 354.2 | 354 | 117, 131, 141, 354, 356, 357 | Pyrazolam | δ 8.50 (d, J = 4.8 Hz, 1H), 8.06–7.91 (m, 3H), 7.69 (d, J = 8.2 Hz, 1H), 7.53–7.49 (m, 2H), 5.32 (d, J = 13.1 Hz, 1H), 4.48 (d, J = 7.6 Hz, 0H), 4.34–4.32 (m, 2H), 2.64 (s, 3H), 2.19–2.14 (m, 3H), 1.90 (s, 0H) | Pyrazolam identified |
| PT2 | 1.03 | 354.2 | 354 | 117, 131, 141, 354, 356, 357 | Pyrazolam | δ 8.50 (q, J = 2.1 Hz, 1H), 8.06–7.91 (m, 3H), 7.69 (d, J = 8.2 Hz, 1H), 7.53–7.49 (m, 2H), 5.32 (d, J = 12.4 Hz, 1H), 4.32 (d, J = 13.1 Hz, 1H), 2.64 (s, 3H) | Pyrazolam identified |
| PT3 | 1.03 | 354.2 | 354 | 117, 131, 141, 354, 356, 357 | Pyrazolam | δ 8.50 (d, J = 4.8 Hz, 1H), 8.06–7.92 (m, 3H), 7.69 (d, J = 8.9 Hz, 1H), 7.53–7.49 (m, 2H), 5.32 (d, J = 13.1 Hz, 1H), 4.48 (d, J = 8.2 Hz, 1H), 4.34–4.32 (m, 4H), 2.64 (s, 3H), 1.90 (s, 1H) | Pyrazolam identified |
| (weak signal) | |||||||
| PT4 | 1.02 | 354.2 | 354 | 117, 131, 141, 354, 356, 357 | Pyrazolam | δ 8.50 (dd, J = 7.2, 2.4 Hz, 1H), 8.06–7.91 (m, 3H), 7.69 (d, J = 8.9 Hz, 1H), 7.53–7.49 (m, 2H), 5.32 (d, J = 13.1 Hz, 1H), 4.48 (d, J = 7.6 Hz, 1H), 4.34–4.32 (m, 5H), 2.64 (s, 3H), 1.90 (s, 1H) | Pyrazolam identified |
| (weak signal) | |||||||
| Thematic Analysis Performed by ChatGPT | |
|---|---|
| Ranked Analysis of Social Media Data | Relevant Social Media Posts Compared to AI Analysis |
|
|
|
|
|
|
|
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mullin, A.; Scott, M.; Vaccaro, G.; Floresta, G.; Arillotta, D.; Catalani, V.; Corkery, J.M.; Stair, J.L.; Schifano, F.; Guirguis, A. Benzodiazepine Boom: Tracking Etizolam, Pyrazolam, and Flubromazepam from Pre-UK Psychoactive Act 2016 to Present Using Analytical and Social Listening Techniques. Pharmacy 2024, 12, 13. https://doi.org/10.3390/pharmacy12010013
Mullin A, Scott M, Vaccaro G, Floresta G, Arillotta D, Catalani V, Corkery JM, Stair JL, Schifano F, Guirguis A. Benzodiazepine Boom: Tracking Etizolam, Pyrazolam, and Flubromazepam from Pre-UK Psychoactive Act 2016 to Present Using Analytical and Social Listening Techniques. Pharmacy. 2024; 12(1):13. https://doi.org/10.3390/pharmacy12010013
Chicago/Turabian StyleMullin, Anthony, Mark Scott, Giorgia Vaccaro, Giuseppe Floresta, Davide Arillotta, Valeria Catalani, John M. Corkery, Jacqueline L. Stair, Fabrizio Schifano, and Amira Guirguis. 2024. "Benzodiazepine Boom: Tracking Etizolam, Pyrazolam, and Flubromazepam from Pre-UK Psychoactive Act 2016 to Present Using Analytical and Social Listening Techniques" Pharmacy 12, no. 1: 13. https://doi.org/10.3390/pharmacy12010013
APA StyleMullin, A., Scott, M., Vaccaro, G., Floresta, G., Arillotta, D., Catalani, V., Corkery, J. M., Stair, J. L., Schifano, F., & Guirguis, A. (2024). Benzodiazepine Boom: Tracking Etizolam, Pyrazolam, and Flubromazepam from Pre-UK Psychoactive Act 2016 to Present Using Analytical and Social Listening Techniques. Pharmacy, 12(1), 13. https://doi.org/10.3390/pharmacy12010013