
Declining but Pronounced State-Level Disparities in Prescription Opioid Distribution in the United States

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Data Analysis
3. Results
3.1. Production
3.2. Distribution
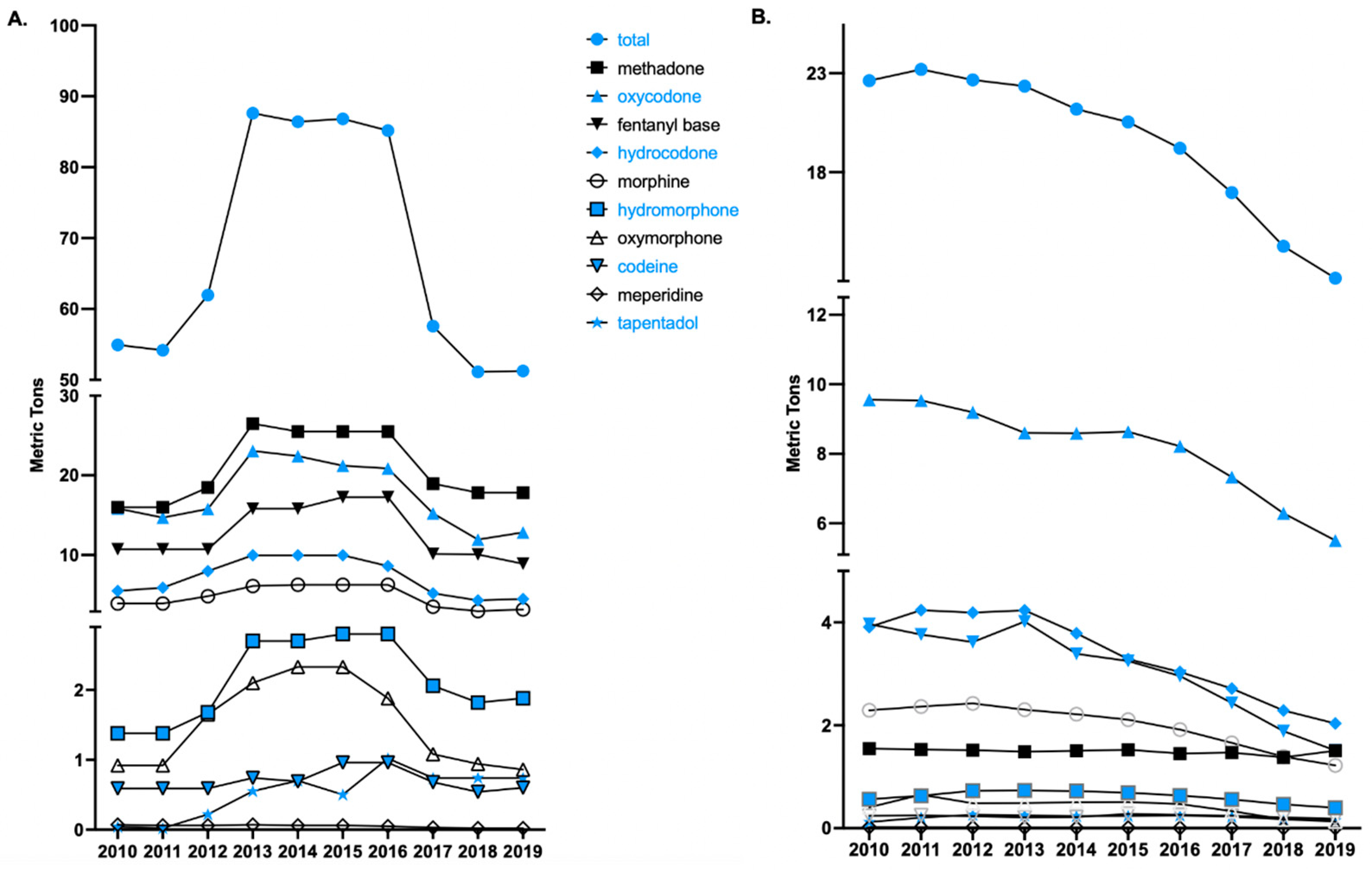
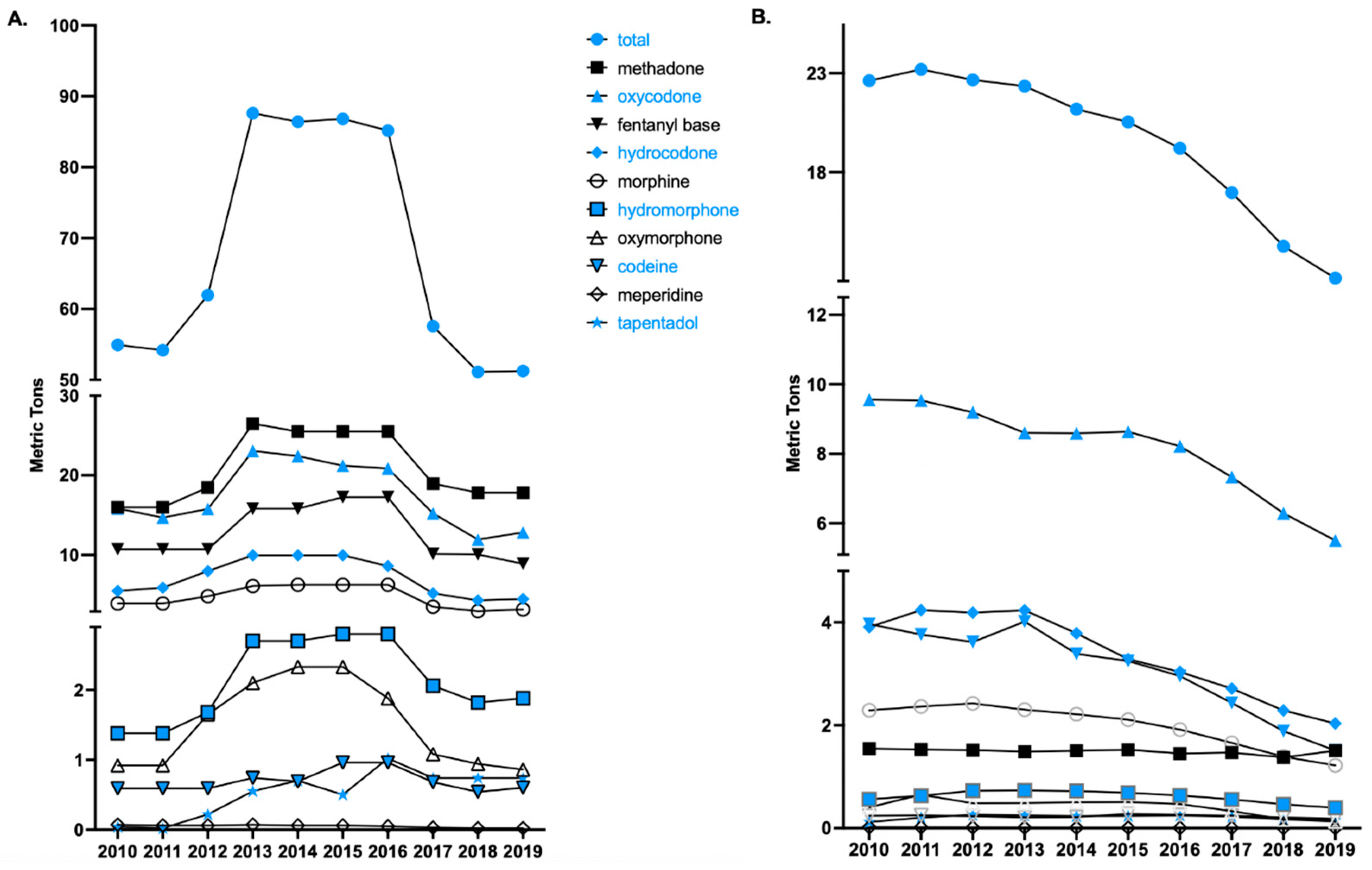
3.2.1. National Opioid Distribution by Drug
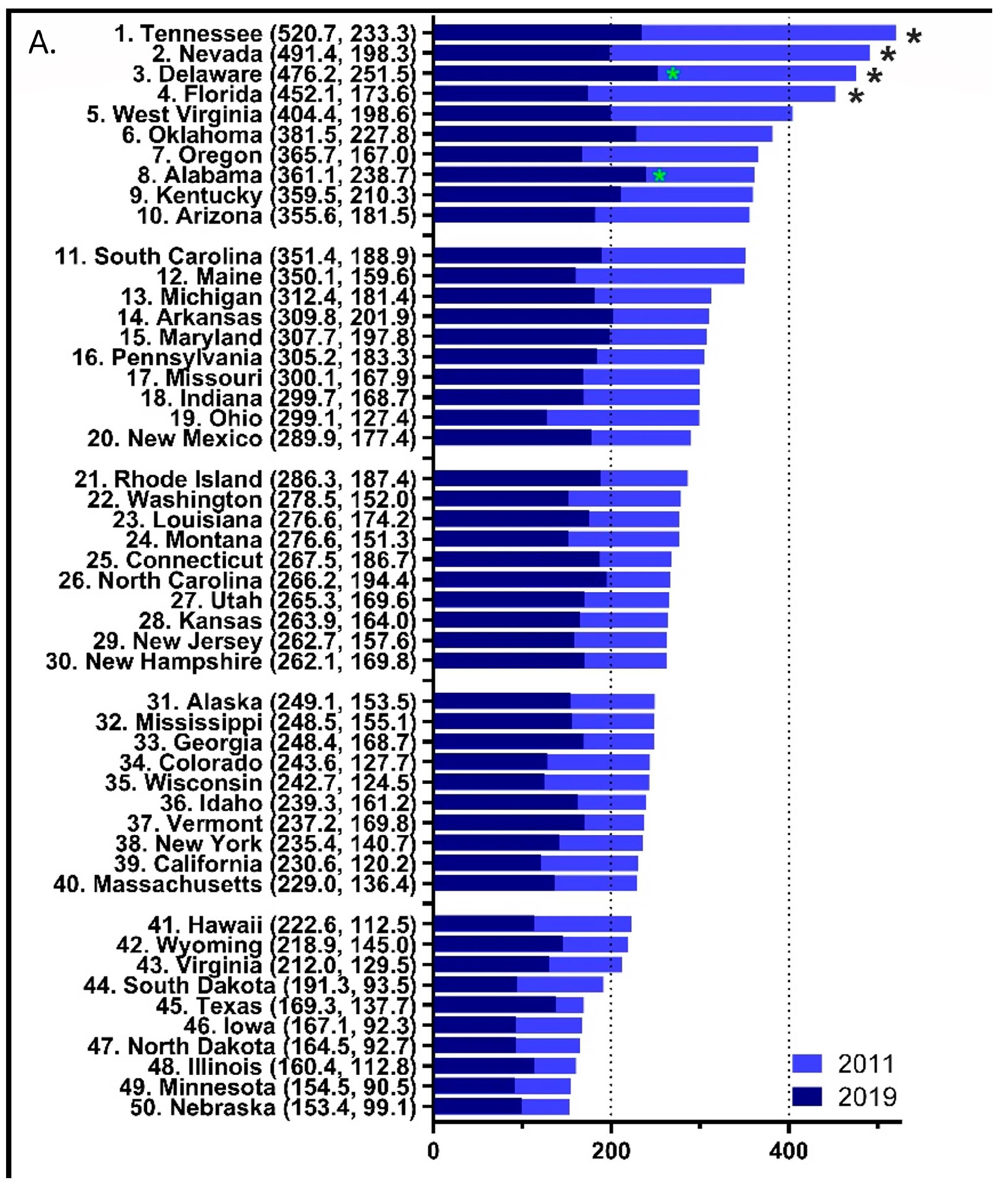
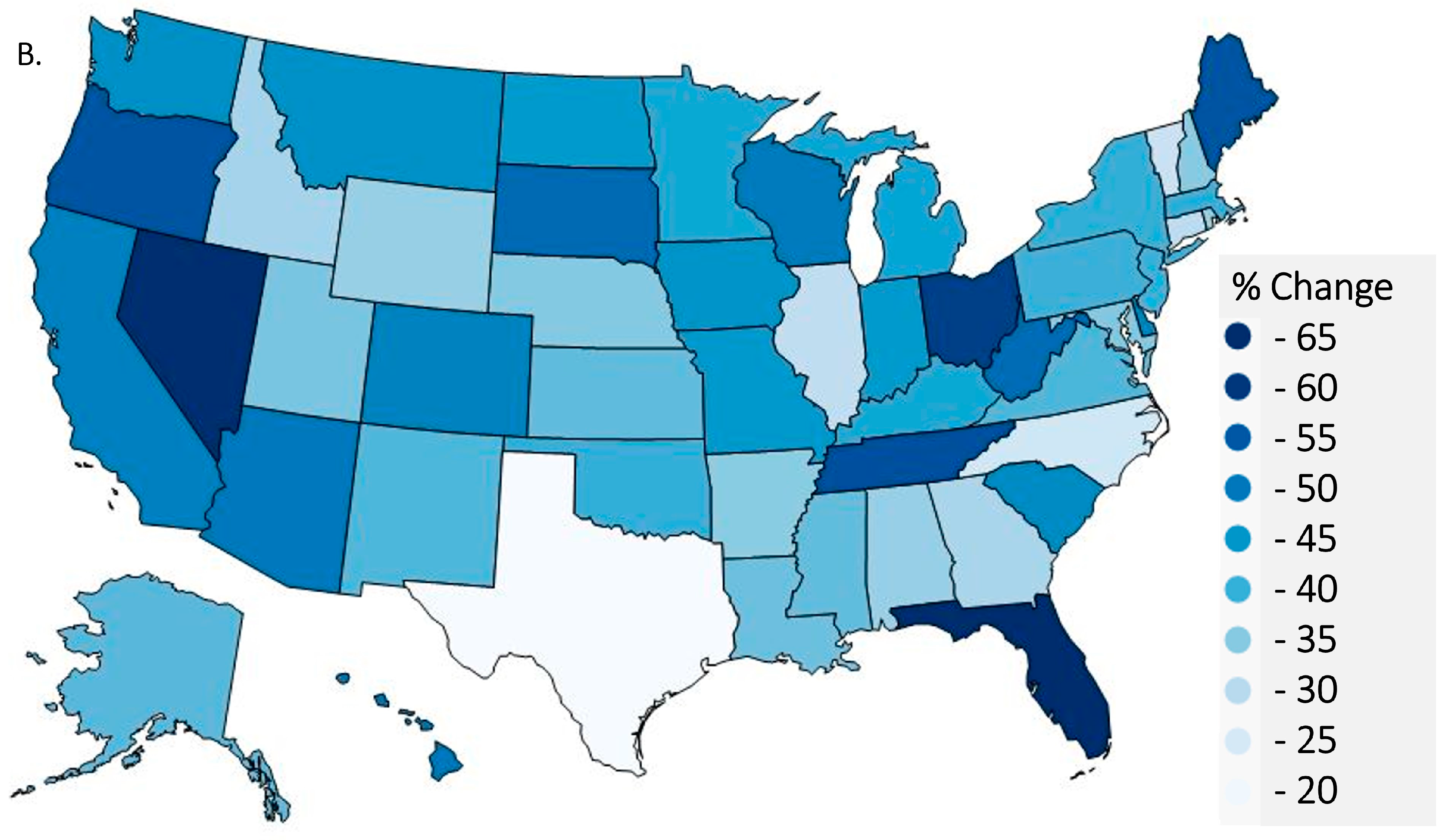
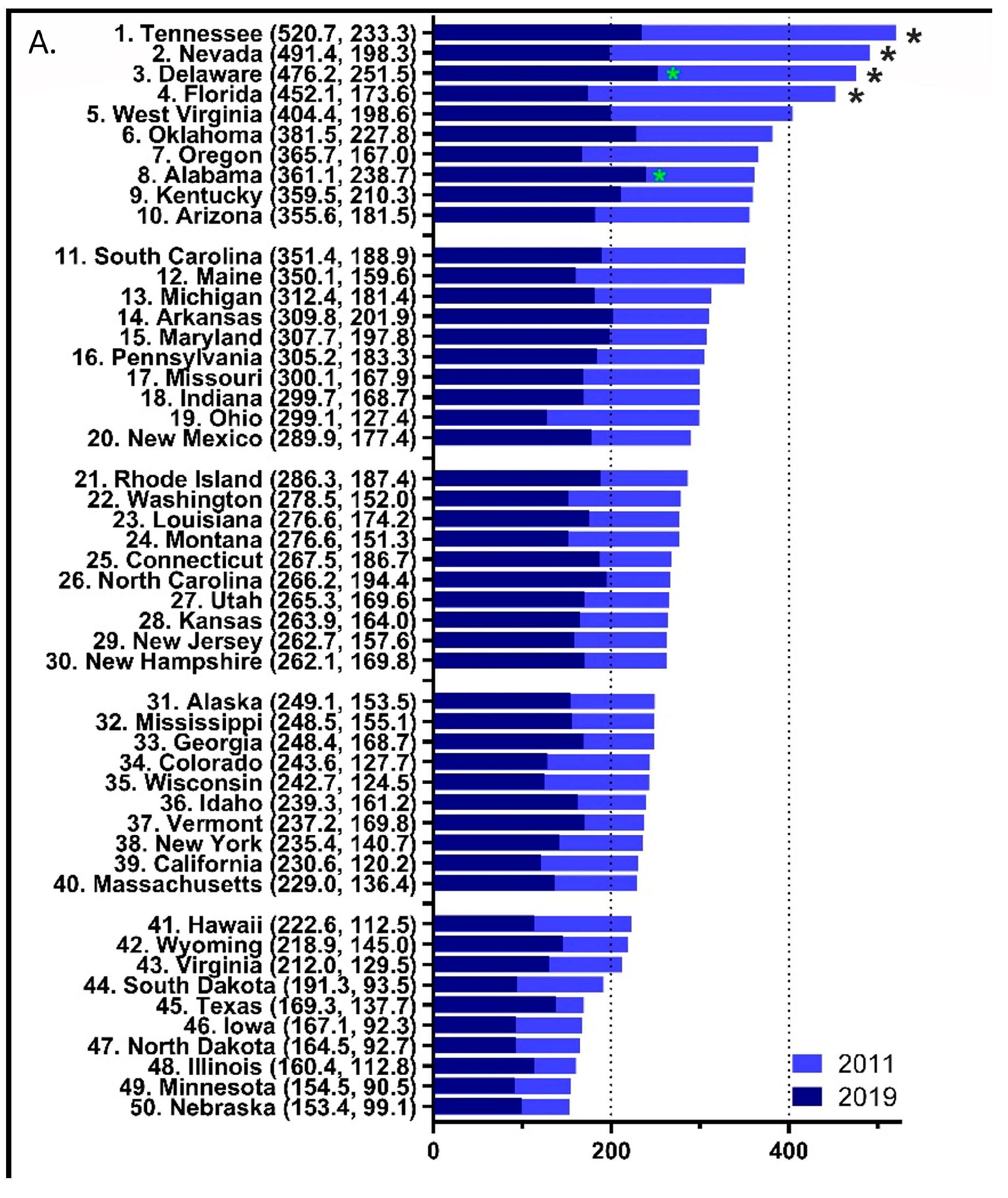
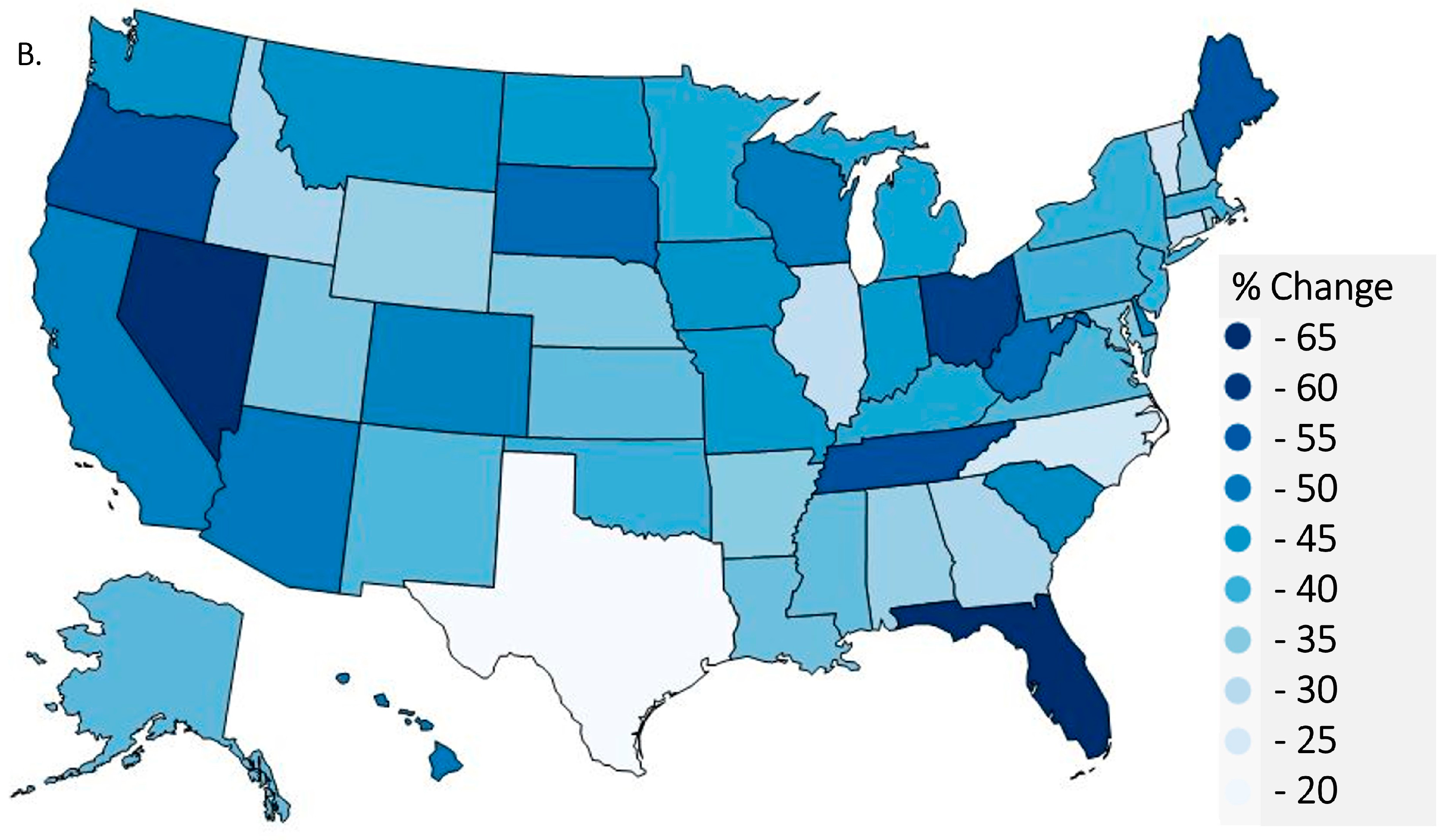
3.2.2. State-Level per Capita Total Opioid Distribution
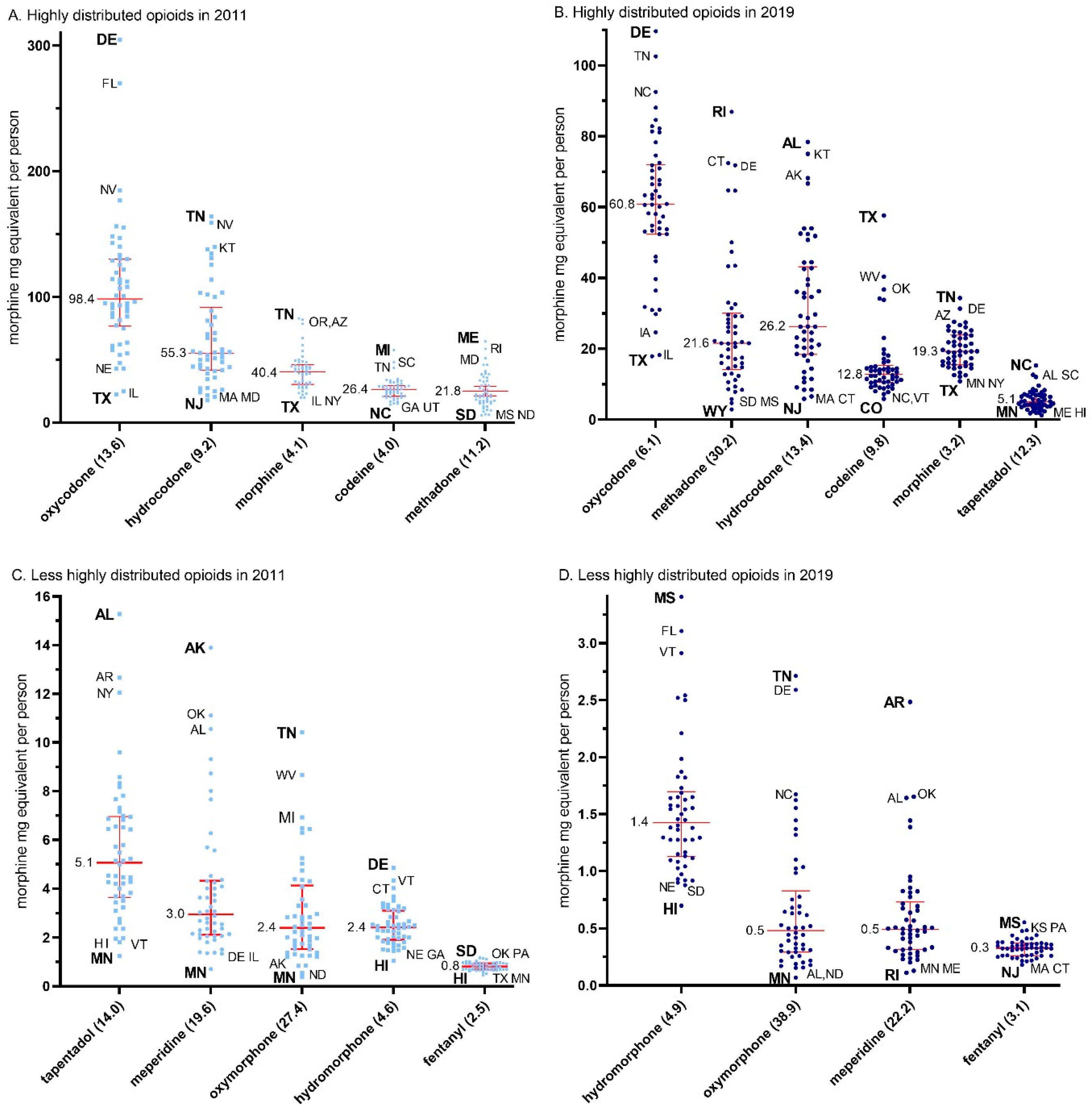
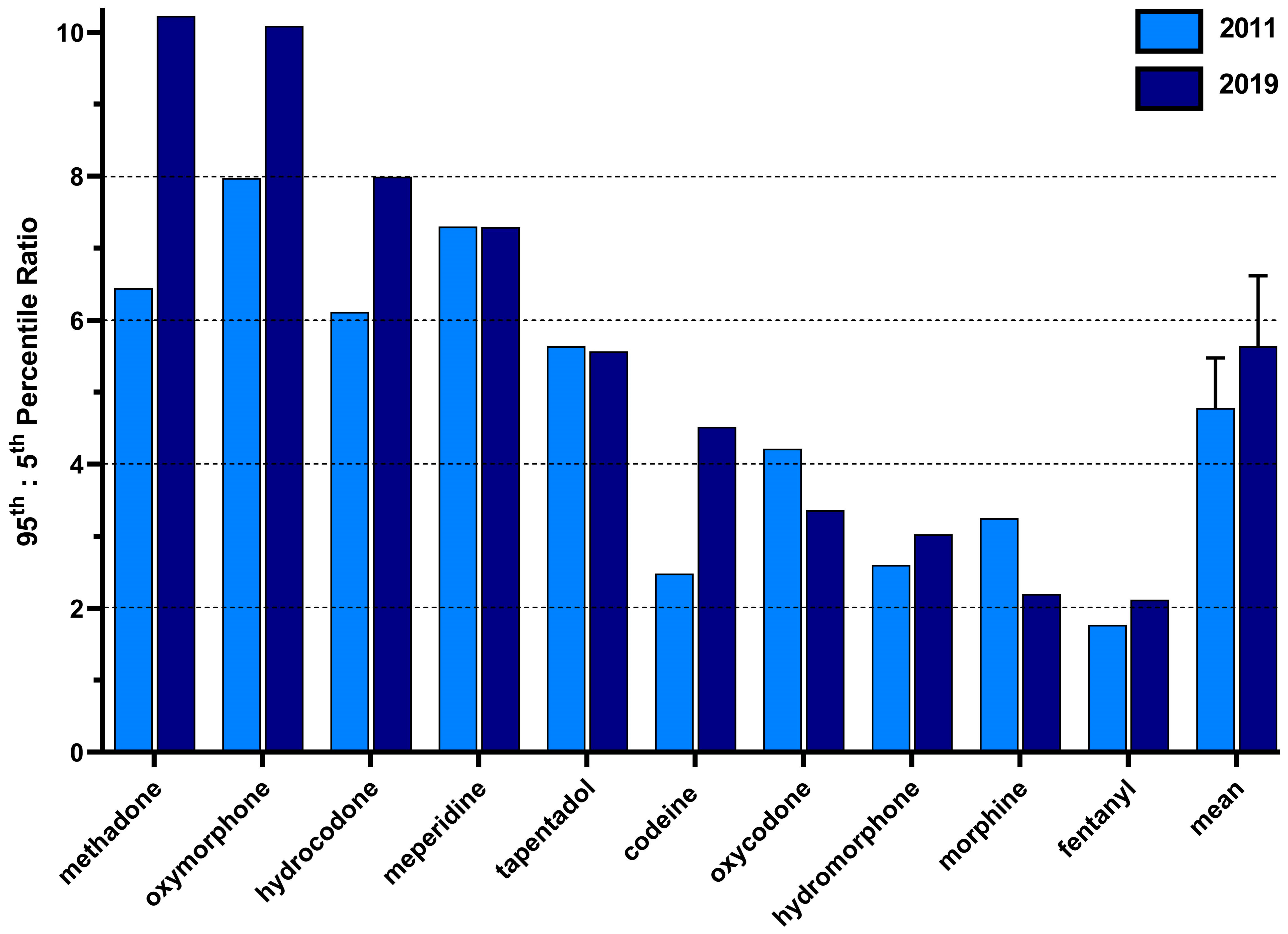
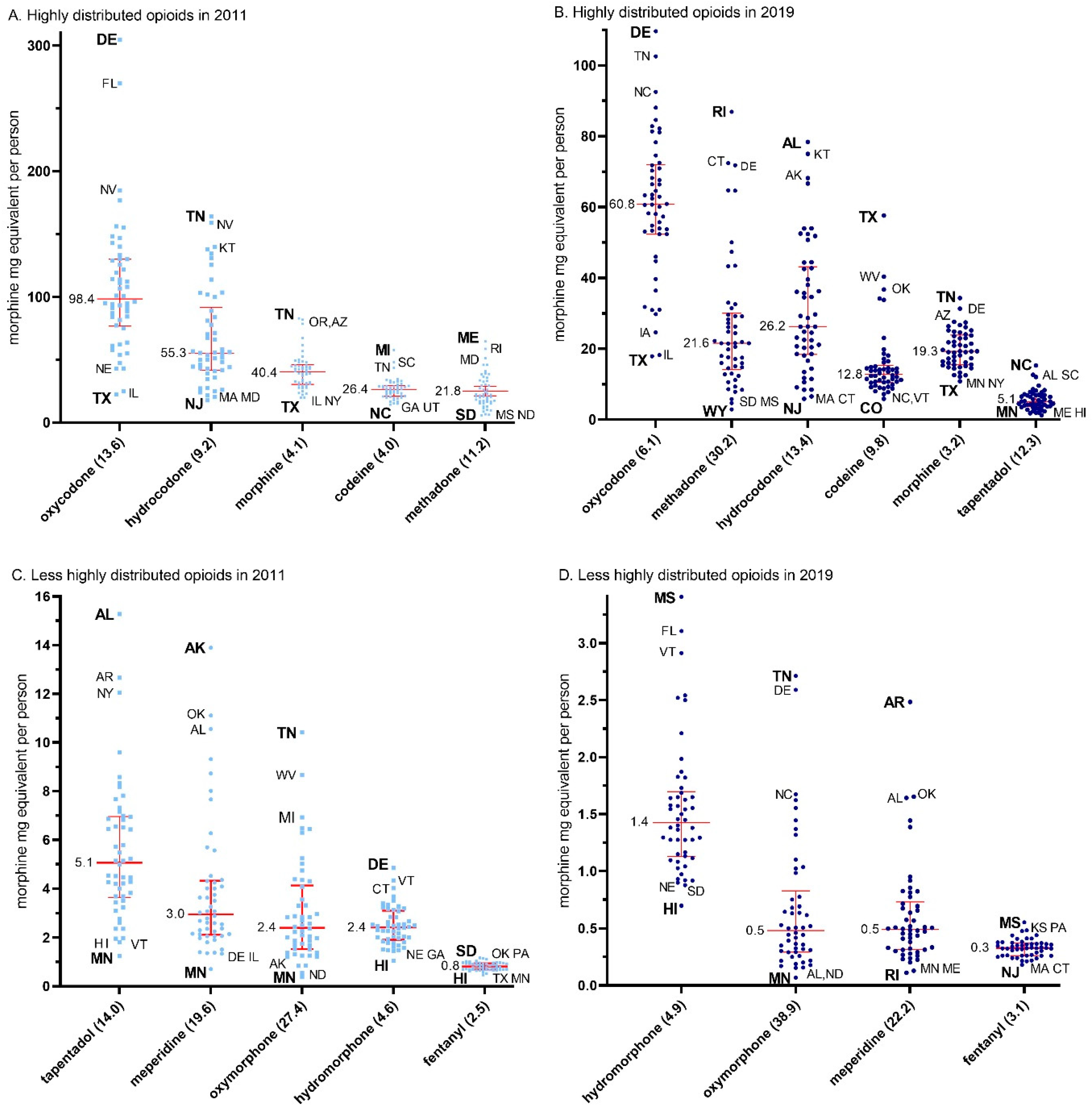
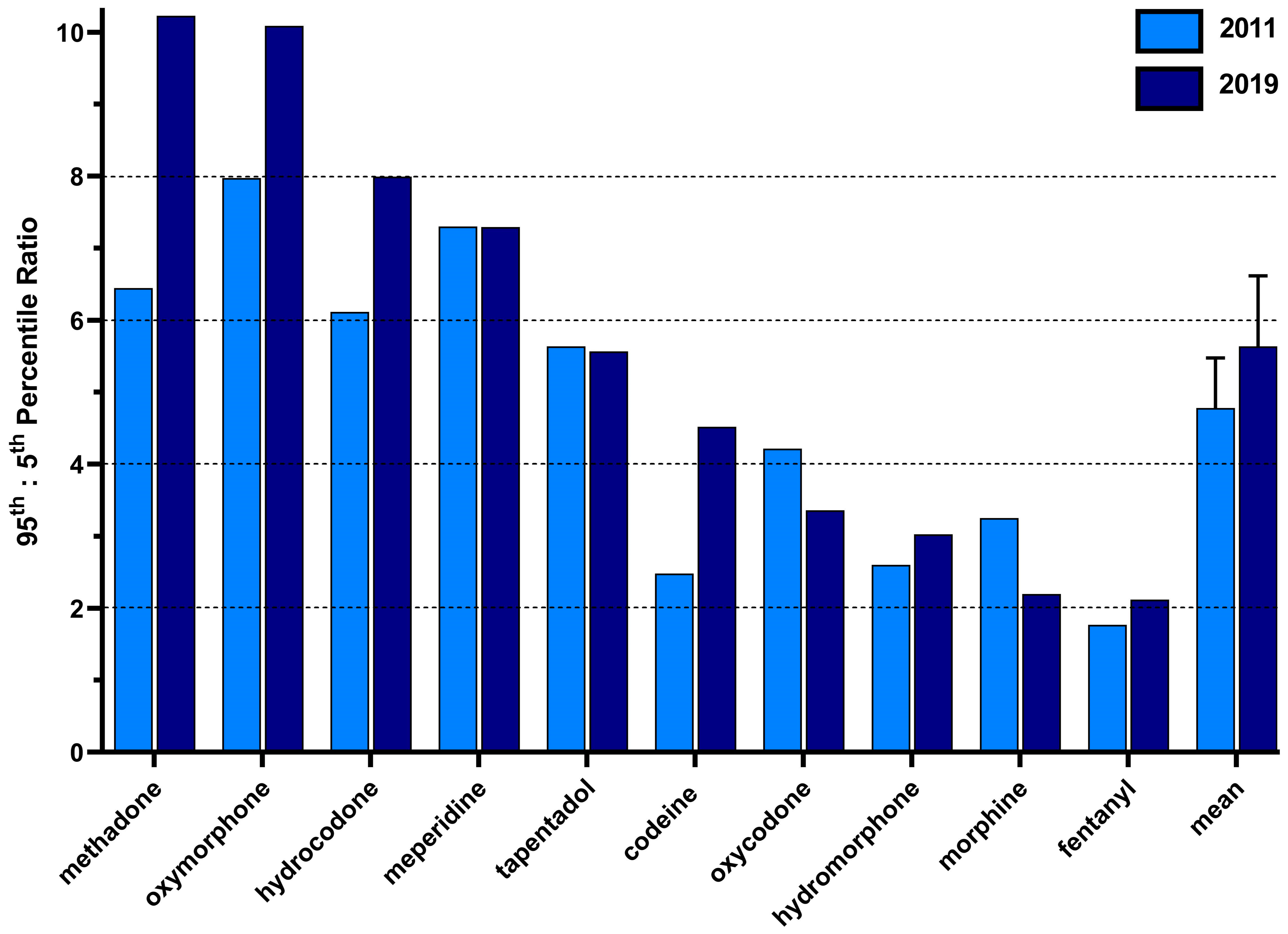
3.2.3. State-Level per Capita Variability in Opioid Distribution by Drug
3.2.4. Correlations in the per Capita MME Distribution between Each Opioid
4. Discussion
4.1. Production
4.2. Distribution
4.3. Limitations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (US). Products—Vital Statistics Rapid Release—Provisional Drug Overdose Data. Available online: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm (accessed on 2 May 2023).
- Seth, P.; Rudd, R.A.; Noonan, R.K.; Haegerich, T.M. Quantifying the Epidemic of Prescription Opioid Overdose Deaths. Am. J. Public Health 2018, 108, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Paulozzi, L.; Mack, K.A.; Jones, C.M. Trends in opioid analgesic–prescribing rates by specialty, U.S., 2007–2012. Am. J. Prev. Med. 2015, 49, 409–413. [Google Scholar] [CrossRef]
- Piper, B.J.; Shah, D.T.; Simoyan, O.M.; McCall, K.L.; Nichols, S.D. Trends in medical use of opioids in the U.S., 2006–2016. Am. J. Prev. Med. 2018, 54, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Eidbo, S.A.; Lopez, A.K.K.; Hagedorn, J.D.; Mathew, V.; Kaufman, D.E.; Nichols, S.D.; McCall, K.L.; Piper, B.J. Declines and regional variation in opioid distribution to U.S. hospitals. Pain 2022, 163, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Guy, G.P.; Zhang, K.; Bohm, M.K.; Losby, J.; Lewis, B.; Young, R.; Murphy, L.B.; Dowell, D. Vital signs: Changes in opioid prescribing in the United States, 2006–2015. MMWR. Morb. Mortal. Wkly. Rep. 2017, 66, 697–704. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (US). Opioid Prescribing. Available online: https://www.cdc.gov/vitalsigns/opioids/infographic.html (accessed on 1 May 2023).
- Fischer, B.; Jones, W.; Vojtila, L.; Kurdyak, P. Patterns, changes, and trends in prescription opioid dispensing in Canada, 2005–2016. Pain Physician 2018, 21, 219–228. [Google Scholar] [CrossRef]
- Cabrera, F.F.; Gamarra, E.R.; Garcia, T.E.; Littlejohn, A.D.; Chinga, P.A.; Pinentel-Morillo, L.D.; Tirado, J.R.; Chung, D.Y.; Pande, L.J.; McCall, K.L.; et al. Opioid distribution trends (2006–2017) in the US Territories. PeerJ 2019, 7, e6272. [Google Scholar] [CrossRef]
- Furst, J.A.; Mynarski, N.J.; McCall, K.L.; Piper, B.J. Pronounced Regional Disparities in United States Methadone Distribution. Ann. Pharmacother. 2022, 56, 271–279. [Google Scholar] [CrossRef]
- Collins, L.K.; Pande, L.J.; Chung, D.Y.; Nichols, S.D.; McCall, K.L.; Piper, B.J. Trends in the medical supply of fentanyl and fentanyl analogues: United States, 2006 to 2017. Prev. Med. 2019, 123, 95–100. [Google Scholar] [CrossRef]
- Boyle, J.M.; McCall, K.L.; Nichols, S.D.; Piper, B.J. Declines and pronounced regional disparities in meperidine use in the United States. Pharmacol. Res. Perspect. 2021, 9, e00809. [Google Scholar] [CrossRef]
- Davis, C.S.; Piper, B.J.; Gertner, A.K.; Rotter, J.S. Opioid prescribing laws are not associated with short-term declines in prescription opioid distribution. Pain Med. 2020, 21, 532–537. [Google Scholar] [CrossRef] [PubMed]
- American Society of Hospital Pharmacies. Drug Shortage Detail: Meperidine Hydrochloride Injection. Available online: https://www.ashp.org/drug-shortages/current-shortages/drug-shortage-detail.aspx?id=347&loginreturnUrl=SSOCheckOnly (accessed on 1 May 2023).
- National Archives. Federal Register: Established Aggregate Production Quotas for Schedule I and II Controlled Substances and Assessment of Annual Needs for the List I Chemicals Ephedrine, Pseudoephedrine, and Phenylpropanolamine for 2020. Available online: https://www.federalregister.gov/documents/2019/12/02/2019-26119/established-aggregate-production-quotas-for-schedule-i-and-ii-controlled-substances-and-assessment (accessed on 1 May 2023).
- US Department of Justice. ARCOS Retail Drug Summary Reports. Available online: https://www.deadiversion.usdoj.gov/arcos/retail_drug_summary/index.html (accessed on 1 May 2023).
- Bokhari, F.; Mayes, R.; Scheffler, R.M. An analysis of the significant variation in psychostimulant use across the U.S. Pharmacoepidemiol. Drug Saf. 2004, 14, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Hudnall, M.; Yang, X.; Melnykov, Y.; Zhu, X.; Lewis, D.; Parton, J. Finite mixture modeling of change point processes to discover opioid prescribing patterns: A case study of automated reports and consolidated ordering system data. Commun. Stat. Case Stud. Data Anal. Appl. 2022, 8, 199–212. [Google Scholar] [CrossRef]
- Schuler, M.S.; Saloner, B.; Gordon, A.J.; Dick, A.W.; Stein, B.D. National Trends in Buprenorphine Treatment for Opioid Use Disorder From 2007 to 2018. Subst. Abus. 2023, 44, 154–163. [Google Scholar] [CrossRef] [PubMed]
- United States Census Bureaus. American Community Survey. Available online: https://www.census.gov/programs-surveys/acs (accessed on 1 May 2023).
- Steinman, M.A.; Yang, K.Y.; Byron, S.C.; Maselli, J.H.; Gonzales, R. Variation in outpatient antibiotic prescribing in the United States. Am. J. Manag. Care 2009, 15, 861–868. [Google Scholar] [PubMed]
- US National Archives and Records Administration. Code of Federal Regulations. Aggregate Production Quotas, 21 C.F.R. § 1303.11 (2018). Available online: https://www.ecfr.gov/current/title-21/chapter-II/part-1303/subject-group-ECFR2b8c25396f0c33e/section-1303.11 (accessed on 1 May 2023).
- Department of Justice. Review of the Drug Enforcement Administration’s Regulatory and Enforcement Efforts to Control the Diversion of Opioids. Available online: https://oig.justice.gov/reports/2019/e1905.pdf (accessed on 1 May 2023).
- Controlled Substances Quotas, 83 F.R. § 32784 (2018). Available online: https://www.govinfo.gov/app/details/FR-2018-07-16/2018-15141 (accessed on 1 May 2023).
- Jones, G.H.; Bruera, E.; Abdi, S.; Kantarjian, H.M. The opioid epidemic in the United States—Overview, origins, and potential solutions. Cancer 2018, 124, 4279–4286. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Digital Communications Division (DCD): Opioid Crisis Statistics. Available online: https://www.hhs.gov/opioids/about-the-epidemic/index.html (accessed on 11 November 2021).
- Haegerich, T.M.; Paulozzi, L.J.; Manns, B.J.; Jones, C.M. What we know, and don’t know, about the impact of state policy and systems-level interventions on prescription drug overdose. Drug Alcohol Depend. 2014, 145, 34–47. [Google Scholar] [CrossRef]
- Ayres, I.; Jalal, A. The impact of prescription drug monitoring programs on US opioid prescriptions. J. Law Med. Ethics 2018, 46, 387–403. [Google Scholar] [CrossRef]
- Chua, K.-P.; Kimmel, L.; Brummett, C.M. Disappointing early results from opioid prescribing limits for acute pain. JAMA Surg. 2020, 155, 375–376. [Google Scholar] [CrossRef]
- Larochelle, M.R.; Zhang, F.; Ross-Degnan, D.; Wharam, J.F. Rates of opioid dispensing and overdose after introduction of abuse-deterrent extended-release oxycodone and withdrawal of propoxyphene. JAMA Intern. Med. 2015, 175, 978–987. [Google Scholar] [CrossRef]
- Davis, C.S.; Lieberman, A.J.; Hernandez-Delgado, H.; Suba, C. Laws limiting the prescribing or dispensing of opioids for acute pain in the United States: A national systematic legal review. Drug Alcohol Depend. 2019, 194, 166–172. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (US). Menu of Selected Provisions. Available online: https://www.cdc.gov/phlp/docs/menu_prescriptionlimits.pdf (accessed on 1 May 2023).
- Usmani, S.A.; Hollmann, J.; Goodin, A.; Hincapie-Castillo, J.M.; Adkins, L.E.; Ourhaan, N.; Oueini, R.; Bhagwandass, H.; Easey, T.; Vouri, S.M. Effects of hydrocodone rescheduling on opioid use outcomes: A systematic review. J. Am. Pharm. Assoc. 2020, 61, e20–e44. [Google Scholar] [CrossRef]
- Ighodaro, E.O.; McCall, K.L.; Chung, D.Y.; Nichols, S.D.; Piper, B.J. Dynamic changes in prescription opioids from 2006 to 2017 in Texas. PeerJ 2019, 7, e8108. [Google Scholar] [CrossRef] [PubMed]
- Geller, J.S.; Milner, J.E.; Pandya, S.; Mohile, N.V.; Massel, D.H.; Eismont, F.J.; Al Maaieh, M. The impact of the Florida law HB21 on opioid prescribing patterns after spine surgery. N. Am. Spine Soc. J. (NASSJ) 2023, 14, 100202. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.M.; Baldwin, G.T.; Manocchio, T.; White, J.O.; Mack, K.A. Trends in methadone distribution for pain treatment, methadone diversion, and overdose deaths—United States, 2002–2014. Morb. Mortal. Wkly. Rep. 2016, 65, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Paulozzi, L.J.; Mack, K.A.; Hockenberry, J.M. Variation among states in prescribing of opioid pain relievers and benzodiazepines—United States, 2012. J. Saf. Res. 2014, 51, 125–129. [Google Scholar] [CrossRef]
- Mark, T.L.; Kassed, C.A.; Vandivort-Warren, R.; Levit, K.R.; Kranzler, H.R. Alcohol and opioid dependence medications: Prescription trends, overall and by physician specialty. Drug Alcohol Depend. 2009, 99, 345–349. [Google Scholar] [CrossRef]
- US National Archives and Records Administration. Federal Register. Schedules of Controlled Substances: Placement of Tramadol Into Schedule IV. Available online: https://www.federalregister.gov/documents/2014/07/02/2014-15548/schedules-of-controlled-substances-placement-of-tramadol-into-schedule-iv (accessed on 1 May 2023).
- Manubay, J.; Davidson, J.B.; Vosburg, S.; Jones, J.; Comer, S.; Sullivan, M. Sex differences among opioid-abusing patients with chronic pain in a clinical trial. J. Addict. Med. 2015, 9, 46–52. [Google Scholar] [CrossRef]
- Friedman, J.; Kim, D.; Schneberk, T.; Bourgois, P.; Shin, M.; Celious, A.; Schriger, D.L. Assessment of racial/ethnic and income disparities in the prescription of opioids and other controlled medications in California. JAMA Intern. Med. 2019, 179, 469–476. [Google Scholar] [CrossRef]
- Singhal, A.; Tien, Y.-Y.; Hsia, R.Y. Racial-ethnic disparities in opioid prescriptions at emergency department visits for conditions commonly associated with prescription drug Abuse. PLoS ONE 2016, 11, e0159224. [Google Scholar] [CrossRef]
- Schieber, L.Z.; Guy, G.P.; Seth, P.; Losby, J.L. Variation in adult outpatient opioid prescription dispensing by age and sex—United States, 2008–2018. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Burgess, D.J.; Nelson, D.B.; Gravely, A.A.; Bair, M.J.; Kerns, R.D.; Higgins, D.M.; van Ryn, M.; Farmer, M.; Partin, M.R. Racial differences in prescription of opioid analgesics for chronic noncancer pain in a national sample of veterans. J. Pain 2014, 15, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.; Tscheng, D.; Hamilton, M.; Hyland, B.; Reding, R.; Trbovich, P. Diversion of Controlled Drugs in Hospitals: A Scoping Review of Contributors and Safeguards. J. Hosp. Med. 2019, 14, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Hulme, S.; Bright, D.; Nielsen, S. The source and diversion of pharmaceutical drugs for non-medical use: A systematic review and meta-analysis. Drug Alcohol Depend. 2018, 186, 242–256. [Google Scholar] [CrossRef]
- Berge, K.H.; Dillon, K.R.; Sikkink, K.M.; Taylor, T.K.; Lanier, W.L. Diversion of drugs within health care facilities, a multiple-victim crime: Patterns of diversion, scope, consequences, detection, and prevention. Mayo Clin. Proc. 2012, 87, 674–682. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2011 | A | B | C | D | E | F | G | H | I | Mean | Standard Error |
| codeine (A) | 1.00 | 0.15 | 0.05 | ||||||||
| fentanyl (B) | 0.31 | 1.00 | 0.23 | 0.04 | |||||||
| hydrocodone (C) | 0.17 * | 0.16 | 1.00 | 0.13 | 0.09 | ||||||
| hydromorphone (D) | 0.16 * | 0.28 | −0.30 | 1.00 | 0.13 | 0.09 | |||||
| meperidine (E) | −0.10 | 0.10 | 0.62 | −0.22 | 1.00 | 0.10 | 0.09 | ||||
| methadone (F) | 0.08 | 0.06 | −0.15 * | 0.40 | −0.20 | 1.00 | 0.16 | 0.10 | |||
| morphine (G) | 0.33 | 0.39 | 0.24 | 0.29 | 0.18 | 0.35 | 1.00 | 0.26 | 0.07 | ||
| oxycodone (H) | 0.19 | 0.26 | −0.12 | 0.44 | 0.02 | 0.66 * | 0.50 | 1.00 | 0.29 | 0.09 | |
| oxymorphone (I) | 0.25 | 0.36 | 0.32 | 0.18 | 0.16 | 0.35 | 0.28 | 0.50 | 1.00 | 0.32 | 0.04 |
| tapentadol (J) | 0.01 | 0.14 | 0.24 | −0.04 | 0.38 | −0.08 | −0.21 | 0.13 | 0.51 | 0.12 | 0.08 |
| 2019 | A | B | C | D | E | F | G | H | I | Mean | Standard Error |
| codeine (A) | 1.00 | 0.08 | 0.08 | ||||||||
| fentanyl (B) | 0.07 | 1.00 | 0.15 | 0.06 | |||||||
| hydrocodone (C) | 0.54 * | 0.33 | 1.00 | 0.12 | 0.12 | ||||||
| hydromorphone (D) | −0.31 * | 0.14 | −0.33 | 1.00 | 0.06 | 0.08 | |||||
| meperidine (E) | 0.17 | 0.29 | 0.58 | −0.07 | 1.00 | 0.17 | 0.09 | ||||
| methadone (F) | −0.10 | −0.26 | −0.45 * | 0.31 | −0.39 | 1.00 | −0.02 ** | 0.10 | |||
| morphine (G) | 0.13 | 0.31 | 0.26 | 0.30 | 0.26 | 0.13 | 1.00 | 0.25 | 0.05 | ||
| oxycodone (H) | 0.10 | 0.05 | 0.02 | 0.25 | 0.21 | 0.39 * | 0.51 | 1.00 | 0.29 | 0.07 | |
| oxymorphone (I) | 0.12 | 0.24 | 0.14 | 0.16 | 0.10 | 0.23 | 0.29 | 0.61 | 1.00 | 0.27 | 0.06 |
| tapentadol (J) | −0.03 | 0.21 | 0.03 | 0.05 | 0.34 | −0.02 | 0.02 | 0.43 | 0.49 | 0.17 | 0.07 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madera, J.D.; Ruffino, A.E.; Feliz, A.; McCall, K.L.; Davis, C.S.; Piper, B.J. Declining but Pronounced State-Level Disparities in Prescription Opioid Distribution in the United States. Pharmacy 2024, 12, 14. https://doi.org/10.3390/pharmacy12010014
Madera JD, Ruffino AE, Feliz A, McCall KL, Davis CS, Piper BJ. Declining but Pronounced State-Level Disparities in Prescription Opioid Distribution in the United States. Pharmacy. 2024; 12(1):14. https://doi.org/10.3390/pharmacy12010014
Chicago/Turabian StyleMadera, Joshua D., Amanda E. Ruffino, Adriana Feliz, Kenneth L. McCall, Corey S. Davis, and Brian J. Piper. 2024. "Declining but Pronounced State-Level Disparities in Prescription Opioid Distribution in the United States" Pharmacy 12, no. 1: 14. https://doi.org/10.3390/pharmacy12010014
APA StyleMadera, J. D., Ruffino, A. E., Feliz, A., McCall, K. L., Davis, C. S., & Piper, B. J. (2024). Declining but Pronounced State-Level Disparities in Prescription Opioid Distribution in the United States. Pharmacy, 12(1), 14. https://doi.org/10.3390/pharmacy12010014