
A Systematic Comparison of Protocols for Recovery of High-Quality RNA from Human Islets Extracted by Laser Capture Microdissection


Abstract
1. Introduction
2. List of Equipment and Reagents
- Tissue-Tek OCT medium (Sakura Finetek, Flemingweg, NL, USA, Cat# 4583)
- Isopentane (2-methylbutane) (Fisher Scientific, Waltham, MA, USA, Cat# 03551-4)
- DEPC-treated water (Invitrogen, Carlsbad, CA, USA, Cat# 750024)
- Ethanol 100% (Pharmco, Brookfield, CT, USA Cat# 1000200SG)
- Ethanol 70% (dilute 100% ethanol with DEPC-treated water to obtain 70% ethanol solution)
- Xylene (Fisher Scientific, Waltham, MA, USA, Cat# UN1307)
- SUPERase·IN (Ambion, Austin, TX, USA, Cat# AM2694)
- RNeasy Micro Kit 50 (Qiagen, Germantown, MD, USA, Cat# 740049)
- Qiazol lysis reagent, 50 mL (Qiagen, Germantown, MD, USA, Cat#55402828)
- RNeasyMinElute Clean-up Kit 50 (Qiagen, Germantown, MD, USA, Cat#74204)
- PicoPure RNA isolation kit (Applied Biosystems by Thermo Fisher Scientific, Vilnius, Lithuania, Cat# KIT0204)
- RNase-Free DNase Set 50 (Qiagen, Germantown, MD, USA, Cat# 79254)
- Cryomold (Fisher Scientific, Waltham, MA, USA, Cat# 22-038217)
- Frosted microscope slides (Corning, New York, NY, USA, Cat# 2948-75X25)
- Polypropylene Falcon Tube (Fisher Scientific, Waltham, MA, USA, Cat# 14-959-49A)
- RNaseZap, 250 mL (Ambion, Austin, TX, USA, Cat# 9780)
- CapSure HS LCM Caps (Arcturus Engineering, Mountain View, CA, Cat# LCM0214)
- GeneAmp® Autoclaved Thin-Walled Reaction Tubes (Applied Biosystems by Thermo Fisher Scientific, Vilnius, Lithuania, Cat# N801-0611)
- Tweezers and forceps
- Pipettes: 20–200 µL and nuclease-free pipette tips
- Cryostat
- Fume hood
- PixCell® IIe Laser Capture Microdissection System (Arcturus Engineering, Mountain View, CA, USA)
- Incubator (Fisher Scientific, Waltham, MA, USA, Cat# 11690506D)
- Microcentrifuge (Fisher Scientific, Waltham, MA, USA, Cat# 05-090-128)
3. Materials and Methods
3.1. Sample Processing and Sectioning
3.2. Laser Capture Microdissection
- Rinsing in diethylpyrocarbonate (DEPC)-treated water
- 70% ethanol for 30 s
- 100% ethanol twice for 1 min
- Xylene for 4 min
3.3. RNA Extraction: Methods
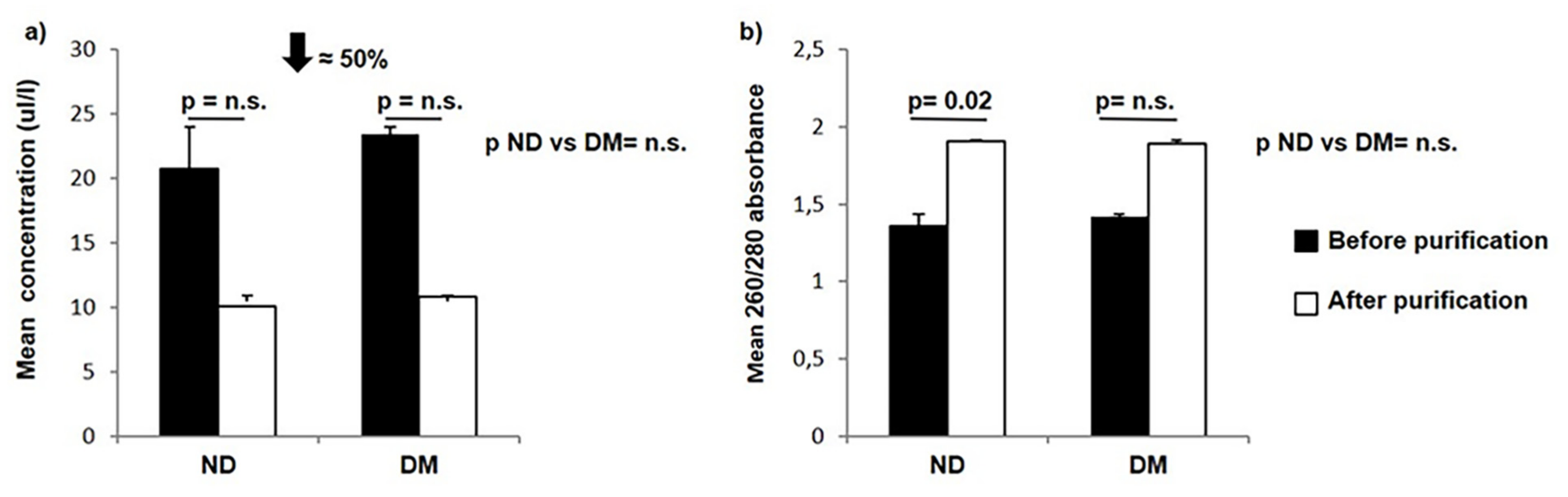
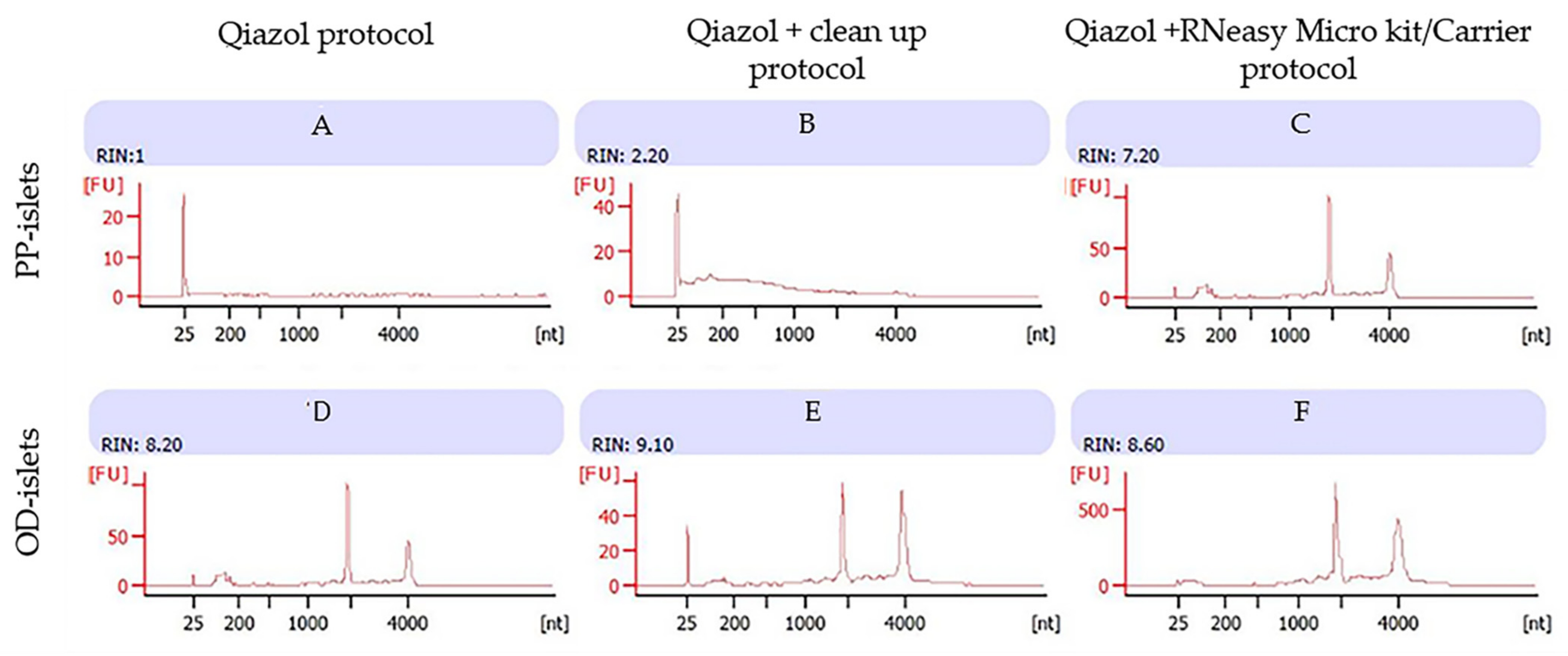
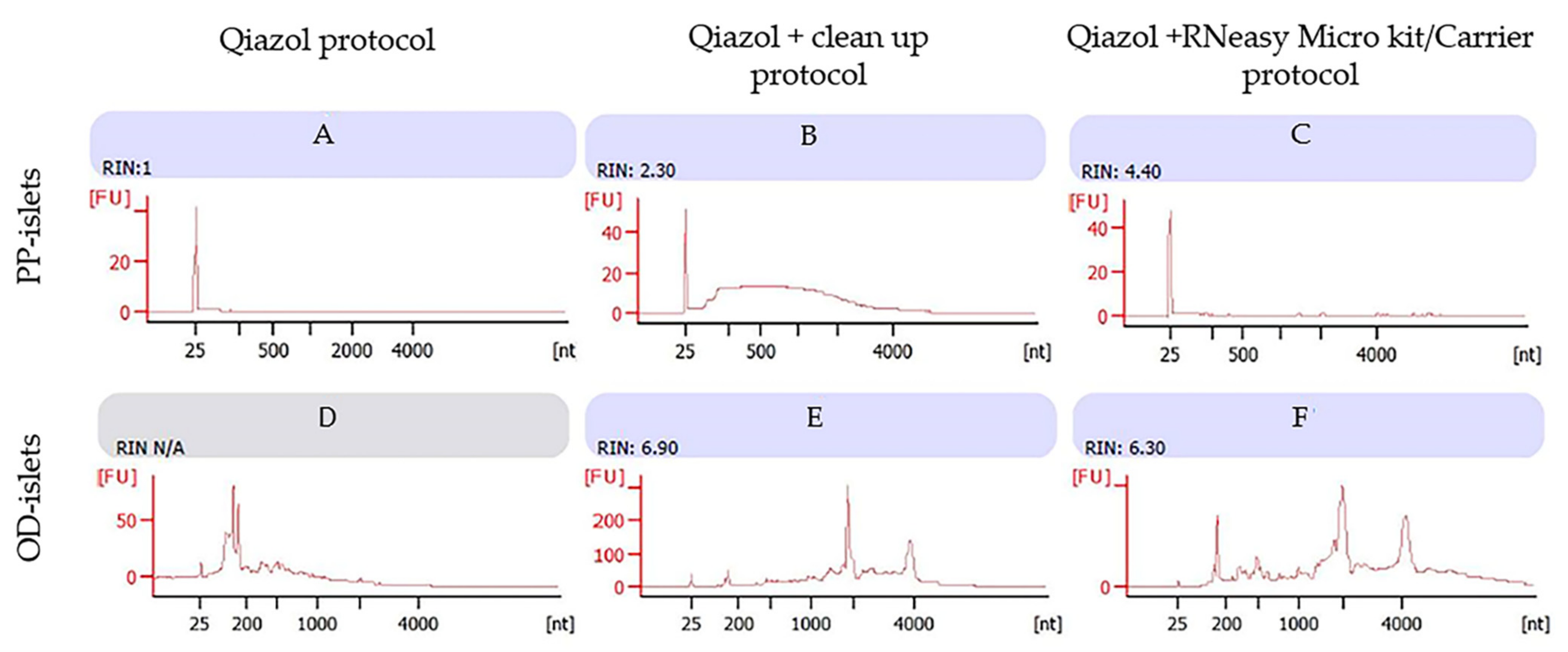
- PicoPure Extraction Kit: First, we used the PicoPure extraction kit by Applied Biosystems by Thermo Fisher Scientific, Vilnius, Lithuania), using a 1:1 ratio of extraction buffer (guanidine isothiocianate) to 70% ethanol. We included DNase treatment by incubating extracted RNA with RNase-free DNase reagent (Qiagen, Germantown, MD, USA) for 15 min. Subsequently, to obtain better RNA quality compared to previous reports (e.g., mean RIN of 5.8) [13], we added a purification step using the RNeasy Mini Clean-up kit (Qiagen, Germantown, MD, USA), which allows the concentration of at least 100 μg of total RNA (≥200 nucleotides) in an elution volume of 30–100 µL. We performed this process on islets extracted from 7 non-diabetic PP samples and 2 diabetic PP samples.To improve both the quantity and the quality of the RNA, we first performed RNA extraction on LCM-collected islets from one non-diabetic and one diabetic subject using Qiazol reagent as lysis cell buffer, which has been reported to produce high-quality RNA from rat pancreas [16]. We used samples that showed a better RIN after bioanalyzer evaluation following the purification step with the RNeasy Mini Clean-up kit (Qiagen Germantown, MD, USA).Then, to optimize the use of the extremely limited material, we performed LCM on all samples and pooled all material obtained from non-diabetic (n = 7) and diabetic (n = 2) subjects; finally, we optimized the process comparing the total amount and the integrity of the RNA extracted from the two samples with three other protocols.
- Qiazol: In this protocol, we avoided the use of binding columns to minimize the loss of material; thus, 700 µL of Qiazol lysis reagent (Qiagen, Germantown, MD, USA) was added to each sample to permit dissociation and homogenization of nucleoprotein complexes, followed by transfer of the supernatant to a new tube. Addition of 140 µL of chloroform followed by a 15 min centrifugation step allowed the separation of the colorless aqueous upper phase containing the ribonucleic acid from the pink lower phase rich in organic proteins and included the interphase where DNA was present. Total RNA was precipitated in a gel-like pellet on the sides and bottom of the tube by mixing the aqueous phase with 350 µL of isopropyl alcohol. To avoid DNA contamination, we incubated the extracted material for 15 min with RNase-free DNase reagent (Qiagen, Germantown, MD, USA). Two washing steps with ethanol were performed to remove contamination, and the extracted RNA was dissolved in 40 µL of DEPC-treated water for downstream analysis.
- Qiazol/Clean-up: In testing this method, we used the previous protocol that included a purification step using the RNeasy Mini Clean-up kit (Qiagen, Germantown, MD, USA, Cat#74204), according to the protocol suggested by the manufacturer (Qiagen). The use of a mini spin column allowed binding of total RNA to the membrane, while the contaminants were efficiently washed away. The final RNA was dissolved in 14 µL of DEPC-treated water.
- Microkit/Carrier: In this protocol, we used Qiazol as lysis cell buffer and performed RNA extraction using the RNeasy Microkit 50 (Qiagen, Germantown, MD, USA, Cat# 740049). This method was designed for isolation of total RNA (up to 45 µg) from small samples. To improve the recovery of total RNA from small samples, we added 5 μL of a 4 ng/μL working solution of poly-ARNA carrier to the lysate. Subsequently, the first steps of the column-based isolation protocol were the same as the first method tested (PicoPure extraction kit by Applied Biosystems by Thermo Fisher Scientific, Vilnius, Lithuania) and involved Qiazol and chloroform solutions to lyse and homogenize samples. Ethanol was added to reach ideal binding conditions, and the lysate contained in the aqueous phase was transferred into the RNeasy MinElute spin column to allow RNA binding to the silica membrane. DNase and any contaminants were efficiently washed away with ethanol, and pure concentrated RNA was eluted in 14 µL of DEPC-treated water.
4. RNA Extraction: Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Emmert-Buck, M.R.; Bonner, R.F.; Smith, P.D.; Chuaqui, R.F.; Zhuang, Z.; Goldstein, S.R.; Weiss, R.A.; Liotta, L.A. Laser capture microdissection. Science 1996, 274, 998–1001. [Google Scholar] [CrossRef]
- Zhang, L.; Lanzoni, G.; Battarra, M.; Inverardi, L.; Zhang, Q. Proteomic profiling of human islets collected from frozen pancreata using laser capture microdissection. J. Proteom. 2017, 150, 149–159. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, T.; Braakman, R.B.; Stingl, C.; van Duijn, M.M.; Smid, M.; Foekens, J.A.; Luider, T.M.; Martens, J.W.; Umar, A. The advantage of laser-capture microdissection over whole tissue analysis in proteomic profiling studies. Proteomics 2016, 16, 1474–1485. [Google Scholar] [CrossRef] [PubMed]
- Marselli, L.; Thorne, J.; Dahiya, S.; Sgroi, D.C.; Sharma, A.; Bonner-Weir, S.; Marchetti, P.; Weir, G.C. Gene expression profiles of Beta-cell enriched tissue obtained by laser capture microdissection from subjects with type 2 diabetes. PLoS ONE 2010, 5, e11499. [Google Scholar] [CrossRef] [PubMed]
- Mo, A.; Jackson, S.; Varma, K.; Carpino, A.; Giardina, C.; Devers, T.J.; Rosenberg, D.W. Distinct Transcriptional Changes and Epithelial-Stromal Interactions Are Altered in Early-Stage Colon Cancer Development. Mol. Cancer Res. 2016, 14, 795–804. [Google Scholar] [CrossRef]
- Chen, H.; Liu, Z.; Gong, S.; Wu, X.; Taylor, W.L.; Williams, R.W.; Matta, S.G.; Sharp, B.M. Genome-Wide Gene Expression Profiling of Nucleus Accumbens Neurons Projecting to Ventral Pallidum Using both Microarray and Transcriptome Sequencing. Front. Neurosci. 2011, 5, 98. [Google Scholar] [CrossRef] [PubMed]
- Marselli, L.; Sgroi, D.C.; Bonner-Weir, S.; Weir, G.C. Laser capture microdissection of human pancreatic beta-cells and RNA preparation for gene expression profiling. Methods Mol. Biol. 2009, 560, 87–98. [Google Scholar] [PubMed]
- Marselli, L.; Thorne, J.; Ahn, Y.B.; Omer, A.; Sgroi, D.C.; Libermann, T.; Otu, H.H.; Sharma, A.; Bonner-Weir, S.; Weir, G.C. Gene expression of purified beta-cell tissue obtained from human pancreas with laser capture microdissection. J. Clin. Endocrinol. Metab. 2008, 93, 1046–1053. [Google Scholar] [CrossRef]
- Negi, S.; Jetha, A.; Aikin, R.; Hasilo, C.; Sladek, R.; Paraskevas, S. Analysis of beta-cell gene expression reveals inflammatory signaling and evidence of dedifferentiation following human islet isolation and culture. PLoS ONE 2012, 7, e30415. [Google Scholar] [CrossRef]
- Beintema, J.J.; Scheffer, A.J.; van Dijk, H.; Welling, G.W.; Zwiers, H. Pancreatic ribonuclease distribution and comparisons in mammals. Nat. New Biol. 1973, 241, 76–78. [Google Scholar] [CrossRef]
- Beintema, J.J.; Campagne, R.N.; Gruber, M. Rat pancreatic ribonuclease. I. Isolation and properties. Biochim. Biophys. Acta 1973, 310, 148–160. [Google Scholar] [CrossRef]
- Butler, A.E.; Matveyenko, A.V.; Kirakossian, D.; Park, J.; Gurlo, T.; Butler, P.C. Recovery of high-quality RNA from laser capture microdissected human and rodent pancreas. J. Histotechnol. 2016, 39, 59–65. [Google Scholar] [CrossRef]
- Sturm, D.; Marselli, L.; Ehehalt, F.; Richter, D.; Distler, M.; Kersting, S.; Grutzmann, R.; Bokvist, K.; Froguel, P.; Liechti, R.; et al. Improved protocol for laser microdissection of human pancreatic islets from surgical specimens. J. Vis. Exp. 2013, 71. [Google Scholar] [CrossRef]
- Zhang, X.; Huang, Q.H.; Han, Z.G. Generation of cDNA libraries for profiling gene expression of given tissues or cells. Methods Mol. Biol. 2003, 221, 179–195. [Google Scholar]
- Puavilai, G.; Chanprasertyotin, S.; Sriphrapradaeng, A. Diagnostic criteria for diabetes mellitus and other categories of glucose intolerance: 1997 criteria by the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (ADA), 1998 WHO consultation criteria, and 1985 WHO criteria. World Health Organization. Diabetes Res. Clin. Pr. 1999, 44, 21–26. [Google Scholar]
- Mezza, T.; Cefalo, C.M.A.; Cinti, F.; Quero, G.; Pontecorvi, A.; Alfieri, S.; Holst, J.J.; Giaccari, A. Endocrine and Metabolic. Insights from Pancreatic Surgery. Trends Endocrinol. Metab. 2020, 31, 760–772. [Google Scholar] [CrossRef]
- Li, D.; Ren, W.; Wang, X.; Wang, F.; Gao, Y.; Ning, Q.; Han, Y.; Song, T.; Lu, S. A modified method using TRIzol reagent and liquid nitrogen produces high-quality RNA from rat pancreas. Appl. Biochem. Biotechnol. 2009, 158, 253–261. [Google Scholar] [CrossRef]
- Mack, E.; Neubauer, A.; Brendel, C. Comparison of RNA yield from small cell populations sorted by flow cytometry applying different isolation procedures. Cytom. A 2007, 71, 404–409. [Google Scholar] [CrossRef]
- Muyal, J.P.; Muyal, V.; Kaistha, B.P.; Seifart, C.; Fehrenbach, H. Systematic comparison of RNA extraction techniques from frozen and fresh lung tissues: Checkpoint towards gene expression studies. Diagn. Pathol. 2009, 4, 9. [Google Scholar] [CrossRef]
- Wilusz, J.E.; Sunwoo, H.; Spector, D.L. Long noncoding RNAs: Functional surprises from the RNA world. Genes Dev. 2009, 23, 1494–1504. [Google Scholar] [CrossRef]
- Srinivasan, M.; Sedmak, D.; Jewell, S. Effect of fixatives and tissue processing on the content and integrity of nucleic acids. Am. J. Pathol. 2002, 161, 1961–1971. [Google Scholar] [CrossRef]
- Evers, D.L.; Fowler, C.B.; Cunningham, B.R.; Mason, J.T.; O’Leary, T.J. The effect of formaldehyde fixation on RNA: Optimization of formaldehyde adduct removal. J. Mol. Diagn. 2011, 13, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Daub, C.D.; Wang, J.; Kudesia, S.; Bratko, D.; Luzar, A. The influence of molecular-scale roughness on the surface spreading of an aqueous nanodrop. Faraday Discuss. 2010, 146, 67–77, Discussion 79–101, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Mezza, T.; Cinti, F.; Cefalo, C.M.A.; Pontecorvi, A.; Kulkarni, R.N.; Giaccari, A. Beta-Cell Fate in Human Insulin Resistance and Type 2 Diabetes: A Perspective on Islet Plasticity. Diabetes 2019, 68, 1121–1129. [Google Scholar] [CrossRef]
- Mezza, T.; Muscogiuri, G.; Sorice, G.P.; Clemente, G.; Hu, J.; Pontecorvi, A.; Holst, J.J.; Giaccari, A.; Kulkarni, R.N. Insulin resistance alters islet morphology in nondiabetic humans. Diabetes 2014, 63, 994–1007. [Google Scholar] [CrossRef]
- Mezza, T.; Sorice, G.P.; Conte, C.; Sun, V.A.; Cefalo, C.M.; Moffa, S.; Pontecorvi, A.; Mari, A.; Kulkarni, R.N.; Giaccari, A. Beta-Cell Glucose Sensitivity Is Linked to Insulin/Glucagon Bihormonal Cells in Nondiabetic Humans. J. Clin. Endocrinol. Metab. 2016, 101, 470–475. [Google Scholar] [CrossRef]
- Philips, T.; Kusmartseva, I.; Gerling, I.C.; Campbell-Thompson, M.; Wasserfall, C.; Pugliese, A.; Longmate, J.A.; Schatz, D.A.; Atkinson, M.A.; Kaddis, J.S. Factors That Influence the Quality of RNA From the Pancreas of Organ Donors. Pancreas 2017, 46, 252–259. [Google Scholar] [CrossRef][Green Version]
- Ebrahimi, A.; Jung, M.H.; Dreyfuss, J.M.; Pan, H.; Sgroi, D.; Bonner-Weir, S.; Weir, G.C. Evidence of stress in beta cells obtained with laser capture microdissection from pancreases of brain dead donors. Islets 2017, 9, 19–29. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-Diabetic (n = 7) | Diabetic (n = 2) | p-Value |
|---|---|---|---|
| Age (years) | 57.2 ± 18.8 | 62.1 ± 22.1 | 0.70 |
| Sex (F/M) | 6/1 | 1/1 | |
| Body mass index (kg/m2) | 24.4 ± 5.76 | 30.5 ± 1.34 | 0.20 |
| Fasting glucose (mg/dL) | 81.6 ± 16.8 | 135±16.6 | 0.006 |
| 2 h OGTT glucose (mg/dL) | 109±21.5 | 225± 7.07 | 0.008 |
| Fasting insulin (mUI/mL) | 3.90 ± 2.41 | 9.95 ± 4.01 | 0.05 |
| 2 h OGTT insulin(mUI/mL) | 20.3 ± 15.7 | 56.3 ± 6.17 | 0.17 |
| Matsuda index | 8.45 ± 2.73 | 5.33 ± 2.44 | 0.26 |
| Triglycerides (mg/dL) | 101 ± 37.6 | 95.5± 26.2 | 0.83 |
| Total cholesterol (mg/dL) | 182 ± 25.5 | 185 ± 20.6 | 0.94 |
| Cholesterol LDL (mg/dL) | 134 ± 19.2 | 126 ± 30.3 | 0.83 |
| HbA1c (mmol/mol) | 30.0 ± 6.95 | 40.5 ± 6.36 | 0.11 |
| Before Purification | After Purification | |||
|---|---|---|---|---|
| ID | ng/µL * | 260/280 | ng/µL ¶ | 260/280 |
| Non-diabetic | ||||
| Sample 01 | 23.59 | 1.45 | 12.34 | 1.59 |
| Sample 02 | 9.40 | 1.57 | 16.73 | 1.55 |
| Sample 03 | 25.05 | 1.45 | 12.66 | 1.47 |
| Sample 04 | 1.94 | 1.53 | 2.47 | 2.60 |
| Sample 05 | 3.85 | 0.97 | 2.85 | 2.15 |
| Sample 06 | 35.97 | 1.23 | 13.51 | 1.45 |
| Sample 07 | 45.40 | 1.35 | 10.41 | 2.57 |
| Mean value ± SD | 20.74 ± 16.5 | 1.36 ± 0.20 | 10.13 ± 5.44 | 1.91 ± 0.51 |
| Diabetic | ||||
| Sample 01 | 15.28 | 1.49 | 9.29 | 1.56 |
| Sample 02 | 31.60 | 1.36 | 5.43 | 2.23 |
| Mean value ± SD | 23.44 ± 11.5 | 1.42 ± 0.09 | 10.79 ± 2.15 | 1.89 ± 0.47 |
| Sample | Bio. Conc. (pg/µL) | Final Bio. Conc. (ng/µL) | RIN |
|---|---|---|---|
| ND_01 | 150 | 0.075 | 1 |
| ND_02 | 147 | 0.0735 | 1 |
| ND_03 | 93 | 0.0465 | 1 |
| ND_04 | 655 | 0.3275 | 1.9 |
| ND_05 | 533 | 0.2665 | 2.5 |
| ND_06 | 988 | 0.494 | 2.6 |
| ND_07 | 45 | 0.0225 | 3.1 |
| Mean value ± SD | 373 ± 358 | 0.18 ± 0.17 | 1.87 ± 0.89 |
| DM_01 | 233 | 0.1165 | 2 |
| DM_02 | 96 | 0.048 | 1.1 |
| Mean value ± SD | 164 ± 96.9 | 0.08 ± 0.04 | 1.55 ± 0.64 |
| Pico RNA Bioanalysis Control | 10 |
| Sample ID | Protocol | ng/µL | 260/280 |
|---|---|---|---|
| PP islets: non-diabetic | Qiazol * | 23.19 | 1.37 |
| Qiazol/Clean-up ¶ | 45.61 | 1.36 | |
| Microkit/Carrier ¶ | 20.68 | 1.48 | |
| OD islets: non-diabetic | Qiazol * | 33.9 | 1.73 |
| Qiazol/Clean-up ¶ | 7.61 | 1.43 | |
| Microkit/Carrier ¶ | 23.85 | 1.86 | |
| PP islets: diabetic | Qiazol * | 23.95 | 1.80 |
| Qiazol/Clean-up ¶ | 10.63 | 1.25 | |
| Microkit/Carrier ¶ | 16.24 | 1.52 | |
| OD islets: diabetic | Qiazol * | 45.82 | 1.50 |
| Qiazol/Clean-up ¶ | 14.31 | 1.78 | |
| Microkit/Carrier ¶ | 33.45 | 1.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cefalo, C.M.A.; Mezza, T.; Giaccari, A.; Kulkarni, R.N. A Systematic Comparison of Protocols for Recovery of High-Quality RNA from Human Islets Extracted by Laser Capture Microdissection. Biomolecules 2021, 11, 625. https://doi.org/10.3390/biom11050625
Cefalo CMA, Mezza T, Giaccari A, Kulkarni RN. A Systematic Comparison of Protocols for Recovery of High-Quality RNA from Human Islets Extracted by Laser Capture Microdissection. Biomolecules. 2021; 11(5):625. https://doi.org/10.3390/biom11050625
Chicago/Turabian StyleCefalo, Chiara M. A., Teresa Mezza, Andrea Giaccari, and Rohit N. Kulkarni. 2021. "A Systematic Comparison of Protocols for Recovery of High-Quality RNA from Human Islets Extracted by Laser Capture Microdissection" Biomolecules 11, no. 5: 625. https://doi.org/10.3390/biom11050625
APA StyleCefalo, C. M. A., Mezza, T., Giaccari, A., & Kulkarni, R. N. (2021). A Systematic Comparison of Protocols for Recovery of High-Quality RNA from Human Islets Extracted by Laser Capture Microdissection. Biomolecules, 11(5), 625. https://doi.org/10.3390/biom11050625