Abstract
Good sleep quality is of primary importance in ensuring people’s health and well-being. In fact, sleep disorders have well-known adverse effects on quality of life, as they influence attention, memory, mood, and various physiological regulatory body functions. Sleep alterations are often strictly related to age and comorbidities. For example, in neurodegenerative diseases, symptoms may be aggravated by alterations in sleep cycles or, vice versa, may be the cause of sleep disruption. Polysomnography is the primary instrumental method to investigate sleep diseases; however, its use is limited to clinical practice. This review aims to provide a comprehensive overview of the available innovative technologies and methodologies proposed for less invasive sleep-disorder analysis, with a focus on neurodegenerative disorders. The paper intends to summarize the main studies, selected between 2010 and 2022, from different perspectives covering three relevant contexts, the use of wearable and non-wearable technologies, and application to specific neurodegenerative diseases. In addition, the review provides a qualitative summary for each selected article concerning the objectives, instrumentation, metrics, and impact of the results obtained, in order to facilitate the comparison among methodological approaches and overall findings.
1. Introduction
Sleep plays a fundamental role in the lives of many animals, from some invertebrates to humans. It has both physiological and behavioral connotations and, although its functions and evolutionary significance are not yet fully known, its fundamental role in the maintenance of homeostasis and the adverse effects due to its sub-optimality are well-known in humans. Indeed, it influences attention, memory, mood, blood pressure, immune and inflammatory response, and stress response [1,2,3]. Under physiological conditions, a sleep phase and a wakefulness phase alternate in a regular manner, constituting the sleep–wake circadian rhythm. The sleep phase is a dynamic process aimed at obtaining the required neurophysiological states at certain times, according to circadian and homeostatic needs and despite external or internal interfering stimuli. Moreover, the so-called macrostructure of sleep, as recorded by electroencephalography (EEG) during polysomnography (PSG), is characterized by a chain of regular and predictable events (cyclic alternation of rapid eye movements (REM) and non-REM (NREM) sleep stages). The process shows an intrinsic variability and has to finely modulate itself in order to maintain the maximum adaptability while preserving sleep macrostructure. In this context, peculiar transient EEG patterns (sleep microstructure) are supposed to play the main role in the building up of EEG synchronization and in the flexible adaptation against perturbations. Alterations in sleep macro- or microstructure provoke sleep disruption, sleep instability and loss of sleep quantity and quality [4,5]. Sleep and wakefulness influence each other; therefore, sleep quality degradation, when persisting over time, may translate into severe and irreversible symptoms, taking the form of a pathological framework. Therefore, it is very important to create the best possible sleeping conditions and to intervene promptly when sleep disturbances occur, both in their diagnosis and eventual treatments. Even though sleep time and quality lessen with age, sleep disorders are related to comorbidities rather than age [6]. In particular, sleep disorders have a high incidence in neurodegenerative diseases (ND) and are known to influence well-being and quality of life [7]. Indeed, the symptoms of the NDs may be worsened by the sleep disorders, but, at the same time, the latter may be caused or augmented by the neurodegenerative disease, creating a more complex clinical picture. Optimized, sometimes individualized, treatments are being developed in clinical practice [8]. The relationship between sleep abnormalities/disorders and NDs is so close that sleep disorders can be used as criteria for the diagnosis of specific NDs [9]. As an example, stridor co-occurs with multiple system atrophy (MSA), while a REM-sleep behavior disorder may discriminate between Alzheimer’s disease (AD) and dementia with Lewy body (DLB). The most interesting discovery in the field is that, in some cases, especially in Parkinson’s disease (PD), the onset of sleep disturbance could reflect early alterations in the neural pathways involved, thus constituting a prodromal symptom [10]. This allows earlier intervention in treatment and follow-up; moreover, it will be crucial when neuroprotective drugs become available [11]. The assessment of sleep macro- and microstructure, movements, respiratory pattern or other neurophysiological changes that occur during sleep is essential to verify the quality of sleep and detect sleep disorders. For clinical purposes, PSG is the gold standard for the assessment of sleep disorders, and guidelines are available for recommended uses. In PSG, selected electrophysiological signals are recorded along with other biological signals of interest, such as airflow, oxygen saturation, chest movements or snoring. The type and number of signals that are recorded depends on the reported symptoms and the aim of the PSG. EEG, plectrooculography (EOG), electrocardiography (ECG), and electromyography (EMG) are required for sleep staging, whereas in the detection of sleep apnea, for instance, the primary focus is on oxygen saturation, airflow, and thorax and abdominal movements [12]. Complete polysomnographic examinations are very complex and invasive; they need cumbersome instrumentation, a proper location, night-time assistance by experienced personnel, time, money and they bring discomfort for the patient as well. The medical inspection of the signals (many hours of recording) needs to be performed by qualified experts and it is, however, subjected to inter- operator variability [13,14]. For these reasons, PSG can only be performed in proper settings and usually for in-patients, mainly when precise diagnosis is essential for targeting therapy. Therefore, many alternatives have been proposed in the research to cope with this limitation, in particular for screening or monitoring purposes. They exploit, in general, new technologies and automatic algorithms to reduce the invasiveness of the instrumentation required and the intervention of specialized personnel. This would allow a much more frequent, if not continuous, assessment of the patients’ condition with reduced cost and discomfort, providing the conditions for optimized diagnosis and treatments. Research in this area has several objectives:
- To update and simplify the work of medical staff by automating or semi-automating certain procedures—such as sleep staging or sleep disorders diagnosis—through new instrumentation.
- To verify medical treatment efficacy and, eventually, to optimize it, through sleep monitoring.
- To ensure frequent or continuous follow-up by providing instrumentation and protocols to be used in non-hospital settings.
This review wants to explore the available new technologies for minimally invasive sleep monitoring, specifically applied to the field of the NDs, focusing on wearable and non-wearable solutions. The paper is organized as follows. The next Section 1.1 and Section 1.2 provides a general background on clinical aspects of sleep monitoring and an overview on the use of technological approaches in NDs. Section 2 provides the description of the methodology employed for the paper selection in this review, Section 3 illustrates results and, lastly, Section 4 contains discussion and conclusions.
1.1. Background of Sleep Monitoring in Neurodegenerative Diseases
In NDs, the progressive loss of neurons in particular structures of the central nervous system (CNS) causes dysfunctions of neural pathways, leading to the symptoms typical of each disease. In some cases, treatments are available for symptoms relief, but the neurodegeneration process is unstoppable and irreversible. AD and PD are among the most common neurodegenerative disorders worldwide, with a high incidence in the elderly population [15]. In fact, aging is one of the main risk factors in developing NDs, even though their etiology can vary, and are not completely understood. Moreover, genes and environment are believed to be together responsible of these diseases’ onset. Other less common NDs are Huntington disease, DLB, amyotrophic lateral sclerosis (ALS), Friedreich ataxia, and MSA. A brief description of the principal symptoms and characteristics is provided in Table 1, with a focus on the diseases’ effects on sleep. In fact, these pathologies have a complex relationship with the sphere of sleep. Sleep disruption and disorders can be commonly found in patients with ND and may constitute an early biomarker. Iranzo in [11] highlights the frequent occurrence of the subsequent sleep disorders in ND:

Table 1.
Neurodegenerative diseases (ND) and sleep-related symptoms, and sleep disorders incidence (sleep disorders incidence (SD)) [11].
- Insomnia.
- Excessive daytime sleepiness (EDS).
- Rapid eye movement (REM) sleep behavior disorder (RBD).
- Periodic leg movements in sleep (PLMS).
- Restless legs syndrome (RLS).
- Central or obstructive sleep apnea (CSA, OSA).
- Sleep disordered Breathing (SDS).
- Nocturnal stridor.
- Circadian rhythm disorders.
Further, sleep-quality impairment, sleep-time reduction, and presence of abnormal movements (both excessive and impaired) are other typical features. Sleep symptoms derive from multifactorial causes, including the deterioration of sleep–wake regulatory circuitries caused by the neurodegeneration itself and altered neural pathways, movement or respiratory symptoms specific to each pathology or several indirect mechanisms [16]. Sleep has, in turn, an influence on the neurodegeneration process, realizing a complex bi-directional relationship that could lead to new targeted interventions [17]. For instance, sub-optimal sleep—e.g., lack of sleep, disturbed sleep, sleep disorders—was found correlated to cognitive-impairment severity in AD patients and in the elderly, thus constituting a possible risk factor for the onset of cognitive impairment [18,19]. Lately, the discoveries regarding this relationship have been translated in the clinical practice, renovating disease diagnostic criteria and treatments [20]. However, sleep-related symptoms are still under-reported by patients and under-diagnosed by healthcare professionals. This is a flaw in optimized diagnosis and intervention, because of the reduced descriptive power of a complete clinical framework that considers these aspects. The result is a reduced quality of life for patients, sub-optimal treatments, and, sometimes, late diagnosis or misdiagnosis. In clinical practice, these sleep disruptions and disorders, including abnormal movements, are assessed through different tools, such as individual interviews (anamnesis), sleep diaries, sleep questionnaires, clinical scales, reduced or complete PSG, sleep diaries, and clinical scales; moreover, clinical protocols establish assessing procedures [21,22]. Typical sleep symptoms and main clinical assessing protocols are described in Table 2. PSG is the most complete clinical examination, able to evaluate every aspect of sleep and derive quantitative measures, constituting the gold standard in assessment and diagnosis of sleep-related problems. Sleep staging, REM sleep without atonia, apneas, oxygen saturation, sleep microstructure including the cyclic alternating pattern (CAP), and sleep parameters computation can be investigated by PSG. Some of the typical sleep parameters employed, besides sleep-stages descriptors, are total sleep time (TST), sleep latency, sleep efficiency, wake after sleep onset (WASO), and REM latency [23]. Standardized semiquantitative evaluation of symptom severity and quality-of-life reduction is provided by clinical rating scales, such as those shown in Table 2. The latter are employed for various sleep disturbances and disorders, including restless legs syndrome (RLS), insomnia, nocturia, breathing disorders, and daytime sleepiness [24]. It must be considered that each subject’s clinical history deeply influences the sleep evaluation tools; in fact, perception of symptoms is subjective and can be influenced by the clinical framework. As an example, in dementia, cognitive impairment can make it difficult to obtain a subject’s collaboration in clinical interviews and physical exams [25]. In synucleinopathies—such as PD, DBL, and MSA—RBD assessment is particularly relevant because its idiopathic occurrence is known to be a prodromal symptom that can anticipate any other symptom by decades [26]. In contrast, RBD developing after the onset of other symptoms may indicate a particular disease phenotype. For this reason, RBD screening and diagnosis have attracted much clinical attention in the last years.
Table 2.
Clinical assessing methods in sleep investigation.
1.2. Overview of Technologies for Neurodegenerative Diseases
Thanks to the progression of technology, many new-generation devices are available to the medical field. Reduction in costs and dimension for greater computational performances is the main followed trend in the hardware technology. This trend is influencing every aspect of medicine, from in-vitro studies to surgery, passing through virtual reality and robotics [39,40,41,42]. In particular, the development of good-quality low-cost sensors determined the development of new possible applications. In addition, the growing world population and the increase in life expectancy created new challenges that technologies, sensors, devices, and algorithms may help to resolve. Technologies in this field are being used to guarantee objectivity, continuity of care and massive screening for lower prices, employing wearable sensors, sensors networks, wireless communication, and automatic algorithms [43].
Companies are also riding the wave, in fact, many consumer products, including smartphones and smartwatches, integrate health monitoring tools and are available at affordable prices for the general population, providing new means for screening and the optimization of self-care. The information provided by this kind of technology does not usually have the aim of substituting standard clinical practice and is targeted to healthy population use; therefore, it is rare for these devices to comply with medical regulations. Nevertheless, some applications, such as heart-rate monitoring and movement analysis, have been proposed as medical tools and obtained American Food and Drug Administration (FDA) approval [44,45]. The gaming industry followed, as well, with the introduction of exergames for physical- and cognitive-health assistance and rehabilitation in neurodegenerative pathologies [46,47,48]. Sleep monitoring tools are also usually included in smartphones, smartwatches, and consoles, due to the well-known effects of sleep in cognitive and physical performances, as well as quality of life. However, the reliability of these devices in this field is not well-known yet [49,50]. Nevertheless, sleep monitoring is a wide field, where many aspects must be considered depending on the required observation (e.g., movements, sleep staging) and the final aim (e.g., diagnosis, screening) and it is influenced by many factors. Hence, it is very difficult to generalize results from general-purpose instrumentation, especially in the presence of diseases altering sleep characteristics. The latter is the case for NDs, for which sleep disturbances and disorders are important to consider, as presented in the previous section, but which manifest themselves through physical and cognitive symptoms which could influence monitoring tools in unknown and often unpredictable ways. From this perspective, a smaller portion of the research explores this declination, both for single-symptom assessment and generic care of the eldery or frail people. activity of daily living (ADL) recognition and assessment is one of the most interesting topics, because they allow continuous monitoring beyond clinic facilities and provide a multi-potential tool in the wide field of smart homes and assisted living. This is the main objective of Internet of Things (IoT) applications for the elderly. Indeed, due to the incidence of comorbidities in the elderly and their constantly growing number, management of their multiple needs will be possible only through new technologies. In the case of dementia and other NDs, this is one of the followed paths [51,52,53,54,55,56]. Besides ADLs monitoring, sleep patterns, disease diagnosis and progression assessment, vital signs, agitation, social interactions, compliance with medication intake, movement and fall detection/prevention are interests of these applications. Smart-home applications use a wide range of technological aids—such as radio frequency identification (RFID), wireless communication protocols, global positioning system (GPS), sensors, and cameras—frequently organized in a mixed architecture including wearable and non-wearable sensors. Studies on smart-home monitoring for NDs are reviewed in the dedicated results section (see Section 3.2).
Another trending topic in new technologies for sleep monitoring is the simplification of PSG. PSG is the gold-standard sleep-monitoring exam in clinical facilities. In its conventional set up, it involves multiple high-quality signals recordings. However, the instrumentation is cumbersome and uncomfortable for the subject to wear. In addition, the examination is long to carry out and to analyze, since clinicians have to deal with hours of recordings. This creates an imperative need for an intervention to simplify the whole procedure through new technologies. Moreover, the polysomnogram evaluation involves anomaly identification (REM sleep without atonia, arousals, apneas) and sleep staging which are subjected to intra- and inter-rater variability [13]. Simpler devices and methods are widely proposed in the literature: sleep staging through single-channel physiological recordings, actigraphy, respiratory dynamics and video were attempted [57,58,59,60]. Automatic sleep-staging solutions for NDs are reviewed in the dedicated results section (see Section 3.1).
Moreover, a wide range of unobtrusive sensors is employed in the literature for other aspects related to sleep monitoring, including wearables [61,62,63,64,65] or camera-based [66,67,68,69] systems. In PD and AD, sensors are widely used in symptoms management and assessment, also with a view to early diagnosis [70,71,72,73,74,75,76,77,78,79,80]. In these disorders, sleep is frequently investigated, especially in studies that focus on motor symptoms, such as the bradykinesia (BK) or dystonia in PD, which can lead to pain or create problems in changing positions or turning in bed. Actigraphy, which provides acceleration recordings from a wrist-worn unit, is already approved by the FDA in the medical field since it enables continuous monitoring (beyond single PSG evaluation). This approach is suitable for the evaluation of excessive daytime sleepiness (EDS), insomnia, and circadian-rhythm sleep disorders, where analysis of time spent in bed and asleep is more relevant. However, its boundary of use in sleep studies is still to be drawn and still a hot topic in the literature, such as in the assessment of NDs’ sleep symptoms. In this framework, studies dedicated to NDs compliant with the inclusion criteria of this review are reported in the results section.
2. Materials and Methods
To provide a general overview of the main recent technological approaches used for the analysis of sleep disorders in NDs, an extensive search of the literature was performed through the online databases Web of Science and PubMed over the last 12 years. The search focused on published studies concerning the NDs listed in Table 1 and on the more exploited unobtrusive approaches for sleep monitoring. To this end, the following search criteria were set through:
- Customized queries using keywords and Boolean operators in the form “(Neurodegenerative Disorder OR Parkinson OR Alzheimer OR Huntington OR Lewy Body OR amyotrophic lateral sclerosis OR Ataxia OR Dementia OR Tremor) AND (sleep monitoring) AND (sensor OR IoT OR smart sensor OR environmental sensor OR inertial sensor OR wearable sensor OR optical sensor OR camera OR bed sensor)”.
- Year range restriction to 2010–2022.
- Exclusion of pharmacology, veterinary and construction engineering categories.
- Writing language limitation to English.
No criterion was applied on the characteristics of studies participants, as long as the application proposed was explicitly aimed at use on ND-affected subjects.
3. Results
The total records found on Web of Science and PubMed were 142, of which 43 duplicates were excluded. Screening of the titles and abstracts reduced the records to 58. In the end, the full-text analysis of the remaining records led to a total of 26 articles. The selection procedure is shown in Figure 1.
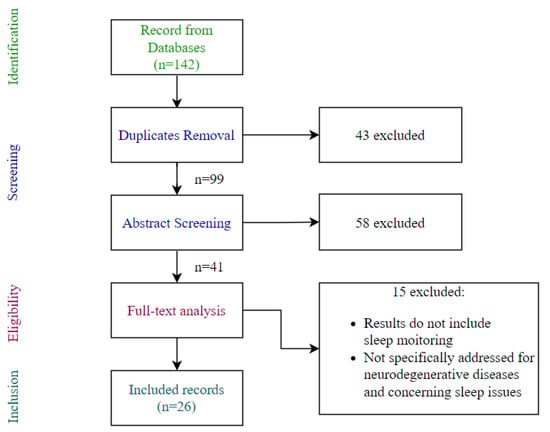
Figure 1.
Article selection process.
The selected articles were then categorized considering the three main application domains: automatic sleep staging, at-home sleep monitoring and sleep-quality and movement analysis tools. The papers’ distribution according to this categorization is shown in Figure 2a. Moreover, a qualitative synthesis is provided for each article, containing the main aim of the article, the instrumentation, the metrics and obtained results. The instrumentation employed in selected papers largely depended on the application and aims. Figure 2b shows the distribution of articles according to the use of wearable and non-wearable approaches, as well as the tested-sample-size type (e.g., PD-affected patients, healthy subjects). In addition, the collection of the sensors used in the reviewed paper was assessed; it includes: bed sensors, 3D cameras, infrared cameras, inertial sensors, smartwatches, headbands and novel tattooed electrodes. A pie chart summarizing sensors’ employment is shown in Figure 3.
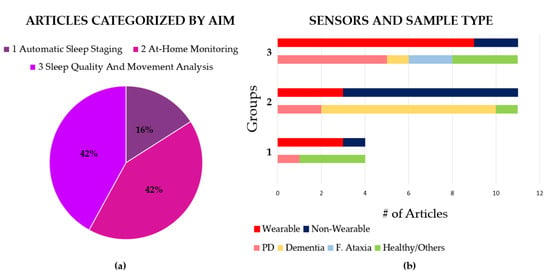
Figure 2.
Distribution of selected papers according to chosen categorization. (a) Pie chart reporting the percentage of articles for the three mainly investigated categories in the literature; (b) bar plots of the distribution of the articles in the three categories of aim, considered sensor type (wearable or non-wearable) and type of targeted population.
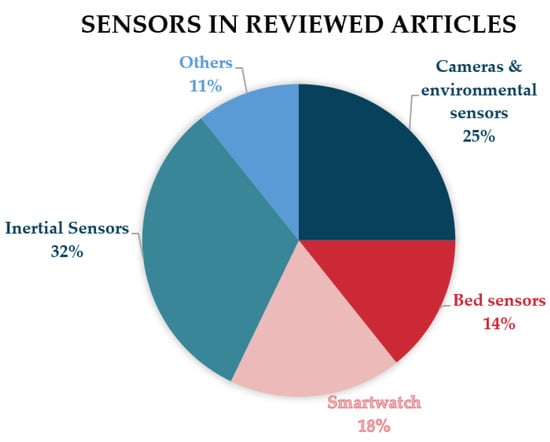
Figure 3.
Pie chart reporting the distribution of sensors employed in the reviewed articles.
3.1. Automatic Sleep-Staging Techniques
Various systems for simplifying the sleep-staging procedure are proposed in the literature, whether based on PSG or innovative instrumentation; however, few of these studies consider the peculiar condition of NDs, which, as already mentioned, can have a strong influence on the feasibility of the proposals and the generalizability of the results. Moreover, these diseases, together with their associated sleep disruptions, often require the observation of peculiar phenomena, to which the proposed new systems need to provide sensitivity. The gold-standard PSG or video-PSG procedure is the most descriptive and complete exam used in these cases. The research challenge is to reduce the cumbersome instrumentation needed, without losing the fundamental information for sleep-stage recognition and abnormality identification (e.g., k-complexes, sleep spindles, delta burst, apneas, muscle tone, eyes movements). To do so and understand the best configuration, automatic sleep-staging algorithms are also needed. From this perspective, the literature search provided four articles. Their qualitative analysis is displayed in Table 3.
Table 3.
Qualitative summary of the selected articles proposing automatic sleep staging.
Some potential solutions were explored by Casciola et al. in [81], Shustak et al. in [82] and Yi et al. [83], on healthy subjects, whereas Ko et al., in [84], tested the capability of the proposed system for abnormal REM detection on PD patients. Casciola, in [81], considered the condition of dementia in AD, where cumbersome instrumentation is a critical issue, due to the typical patient behavior (fear, confusion, aggressive behavior [85,86]). From this perspective, portable EEG headbands (HB) could provide a solution. The authors wanted to overcome the typical reduced signal quality in HB through a deep learning (DL) approach. Their approach was tested on EEG HB and simultaneous PSG recordings. Accuracies of their automatic scoring algorithm were calculated according to manual scoring of PSG in the two cases (HB and PSG signals). The signal processing of HB included band pass filtering and corrupted-epoch manual identification and removal. This cleaning procedure was further deepened through an automatic identification of corrupted epochs using correlation metrics between channels and amplitude values. Data were augmented exploiting windows overlapping, and a DL model, based on convolutional neural network (CNN) and long short-term memory (LSTM), was developed and applied. Authors also implemented traditional sleep-staging techniques for performance comparison. In the end, the proposed DL sleep-staging model achieved 74% accuracy on low-quality HB EEG data and 77% with gold-standard PSG with respect to manual scores. Moreover, the balanced accuracy of the proposed DL method increased by almost 20% compared to any other machine-learning sleep-staging method attempted by them. To better understand the power of their method in the NDs’ framework, their approach should be tested on a bigger and differentiated population, comprehending pathological subjects. Yi et al., in [83], proposed an automatic sleep-staging algorithm that exploits bed-sensor recordings consisting of four hydraulic bed transducers under the mattress. Their method aimed to classify sleep in awake, REM and NREM stages by computing 74 features and classifying them usingk-nearest neighbour (k-NN) and support vector machine (SVM) classifiers. Features related to temporal and frequency domains of heartbeat and respiration were considered (ballistocardiography signal analysis). The SVM classifier provided the best performances (accuracy 85.3%) and was also used in a hierarchical fashion (binary asleep–wake classification plus binary REM or NREM classification). In contrast, the other classifiers considered in this study showed inferior and similar performance when compared to the PSG manual score.
Regarding instrumentation developments, Shustak et al., in [82], proposed a wearable setup for sleep staging composed of temporary tattooed dry electrodes: two submental EMG, and two EOG and four forehead EEG electrodes. Data amplification and transfer to a laptop exploited a compact wireless recording system (a customized printed circuit board, a Bluetooth low-energy chip, and a battery). The electrode array employed is shown in Figure 4a. Signals were classically band-pass filtered, and a notch filter was also applied. The authors tested their system in three ways: firstly, they validated effectiveness of EOG, EMG, and EEG recordings using typical facial movements (e.g., smiling, blinking swallowing); secondly, they compared their EEG recordings to the gold-standard systems and, lastly, they assessed the feasibility in home environments. The tattooed electrodes provided signals visually similar to the ones from an EEG system with 10–20 international standard. It was possible to observe sleep spindles and k-complexes, and the recordings were easily interpretable for sleep technicians. Stable recordings were achieved both in a hospital environment and in home settings, where subjects reported good reviews and no impairments in sleep.
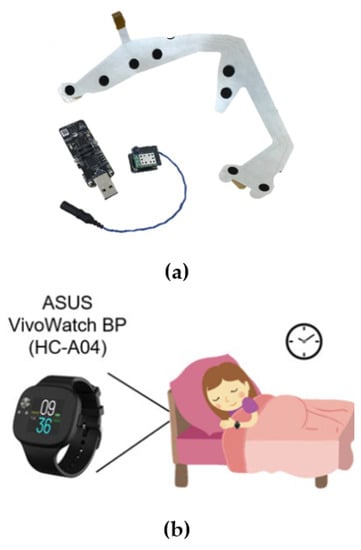
Figure 4.
Examples of sensors employed for automatic sleep staging. (a) Electrodes array system, adapted from electromyography, electrooculography and electroencephalography, adapted from [82]. (b) Smartwatch for cardiac and inertial evaluation, adapted from [84].
Lastly, Ko et al. in [84], provided a method for sleep staging and abnormal REM recognition using cardiac and acceleration signals provided by a smartwatch, see Figure 4c. The authors applied a hierarchical classification through machine-learning techniques, classifying firstly sleep/awake conditions with the Cole–Kripke algorithm, then deep and light sleep based on the G-value and, lastly, identifying REM through k-means clustering. They also defined identification criteria of abnormal REM stages, to be sensitive to REM parasomnias such as EDS typical in PD and MSA. They verified sleep-staging results in a clinical trial, comparing sleep stages and abnormal REM percentages in healthy-control versus PD patients treated with therapy for REM sleep behavior disorder (RBD) versus untreated PD patients. Although the classification accuracies were not very high, the results showed statistically significant differences between healthy-control and PD patients in the percentage of deep sleep. In addition, abnormal REM was found to be significantly different between PD patients with and without RBD therapy (in particular, using clonazepam).
3.2. At-Home Sleep Monitoring
The elderly population presents multiple needs simultaneously, since they are usually affected by several diseases with different symptoms. To cope with their conditions, more and more emphasis is being placed on wide-ranging monitoring over time within the home setting. In this way, various parameters can be monitored in a customized manner responding to multiple objectives: to verify health status; to assess the risks for the subject; to make preventive interventions; to diagnose diseases and observe their possible progression; ti check compliance with treatment and, finally, verify the effects of treatments. Such multi-approach monitoring is even more suitable in the presence of a diagnosed ND; in fact, significant efforts are focused on this line of research. Many of these studies include sleep monitoring in their set-up, given its importance for quality-of-life and symptom monitoring. Usually, these systems rely on a network of sensors, wearable and/or non-wearable, which transmit data to cloud services or platforms. In this way, subjects, caregiver, and clinicians can access the data and observe long-term results. Sometimes, these platforms provide custom-made analysis algorithms or they provide a summary of the outputs of the commercial/custom sensors employed. The literature search produced 11 articles in this framework; their summary description is presented in Table 4, where emphasis is placed on the advancement of the sleep-related study and instrumentation adopted.
Table 4.
Selected articles that present a system dedicated to neurodegenerative diseases in a smart-home monitoring framework, which includes sleep monitoring.
Regarding cognitive impairment, a smart-home environment for continuous monitoring of elders with dementia is presented by Lazarou et al. in [87]. The article presents the architecture developed in the framework of the Dem@Care FP71 project [88,89]. In the Dem@Care project, the monitoring of sleep, physical activity and ADL were the main goals. In their setup, also used in [90], a commercial under-mattress sensor was employed that was able to determine sleep duration and stages. The proposed solution also involved the integration of the automatic evaluation of daily activity and anomalies by a wide range of sensors, with the assessment and final opinion of clinical experts to target the treatment. In Ref. [87], the authors wanted to verify that their system and the adapted clinical interventions could have positive effects on the physical and cognitive functions of participants. Results concerning sleep included reports of four use cases where, in general, a reduced number of sleep interruptions and increased deep sleep and REM phases were found. Detailed data of sleep patterns were presented for the four subjects (use cases). In Ref. [90], the long-terms effects of the use of the system were evaluated on a bigger subject sample (twelve mildly cognitive-impaired subjects and six subjects with AD): the results confirmed the previous observations: reporting better sleep quality. The effects of this system installation, along with a personalized non-pharmaceutical intervention suggested by the system, were compared with a control group that underwent traditional interventions and with a second control group that did not receive neither personalized nor traditional interventions. Thomas et al., in [91], proposed an at-home smart monitoring system able to assess treatment efficacy for AD. Part of the platform is shown in Figure 5. They considered sleep monitoring using a smartwatch, evaluating TST and compliance to wearing the watch. Specifically, they found that the watch was worn more during the day than at night (compliance 60%), and that subjects often forgot to put the watch back on their wrist when they put it away for some reason. This last result may suggest that wearable solutions, such wrist bands, may not be optimal for continuous sleep monitoring in elders, especially with any kind of memory impairment such as in mild cognitive impairment (MCI) or dementia. Kikhia et al., in [92], focused on nursing homes and proposed the DemaWare@NH monitoring framework system. The aim was to assess behavioral and psychological symptoms of dementia. Concerning sleep, they employed a smart clock connected with a smartphone able to detect respiration signals and movements. The system provided sleep staging in terms of awake, light-sleep and deep-sleep periods, and a 1–100 sleep score. The clinical staff accepted the system, but the smart-clock recordings were made difficult by patients who frequently interacted with the clock-phone system, moving it during the day or pulling cables. This forced the clinical stuff to set up the sensor only during the night. However, the clinical stuff considered the data provided informative on the status of the subjects. Rose et al., in. [93], dealt with symptom assessment in AD. Specifically, they analyzed the correlation between nighttime agitation, sleep disturbances and urinary incontinence outside of the clinical setting. Even in this case, the authors designed a multiple-sensor network. To perform sleep monitoring, they used an under-mattress sensor, a microphone, and TEMPO nodes on wrists, i.e., a wireless inertial sensor net. They were able to detect the aforementioned symptoms and to find a correlation between them.
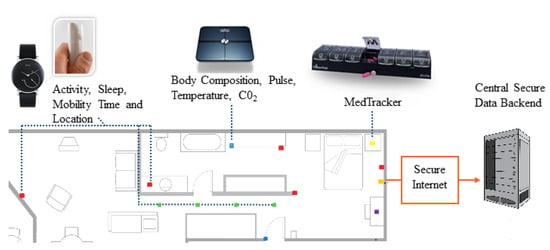
Figure 5.
Example of an at-home smart platform for broad-spectrum assessment, including sleep. The figure is adapted from [91], where a platform for the assessment of treatment efficacy in Alzheimer’s disease is presented.
Regarding continuous monitoring of AD, Oregon Center for Aging and Technology (ORCATECH) at the Oregon Health and Science University have been developing a home monitoring system since 2004. Their platform was meant to assess disease progression and intervention efficacy, relying on passive IR motion sensors and wireless magnetic-contact sensors. The project design and application are described in detail in [19]. Between the various activity recognition and evaluation, the findings regarding sleep by Heyes, in [94], are within the scope of this review. In this last study, the authors used a previously validated algorithm to automatically assess sleep, extracting sleep duration and permanence in bed features (e.g., WASO; TST; settling time: time from getting into bed until the start of the first 20 min period of no movement; times up at night: when the participant actually got out of bed; and total movement in bed at night). Authors also collected subjective sleep assessments and compared elderly volunteers with amnestic MCI and with non-amnestic MCI subjects. Passive sensing for dementia monitoring were also employed by Au-Yeung in [95]. Their study evaluated only four subjects, two with the ORCATECH platform and two with the Emerald platform (Emerald Innovations Inc., Cambridge, MA, USA), which provides movement, location, and activity info from radio-wave sensors. They compared sleep scores, as provided by the two systems, in different pharmacological interventions. They were able to detect periodic leg movements, associated with drug side effects, providing a tool for modifying interventions and treatments.
The works of Rawtaer et al. in Ref. [96] and of Abbate et al. in [97] were focused on the field of prevention and early detection. In Ref. [96], the authors evaluated the duration and quality of sleep with a sensor able to detect bed occupancy in terms of sleep duration and interruptions, both on healthy controls and subjects with MCI. The monitoring system reported a worse sleep quality in MCI subjects, in agreement with clinical questionnaires and almost all participants reported good acceptability (41 out of 49). In Ref. [97], the authors proposed a platform exploiting passive and physiological sensing. The study does not report any results on a specific group of subjects, but it claims the feasibility of sleep studies based on Enobio EEG HB (Starlab®, Neuroelectrics, Barcelona, Spain). From sleep data, they also intended to infer the risk of fall. Part of the presented platform architecture is shown in Figure 5a. Regarding Parkinson disease, Branco et al., in [98], presented a data platform (DataPark) able to collect continuous data from an accelerometer. The platform includes quantification algorithms of sleep and physical activity. They obtained preliminary results in a group of PD patients living in a rehabilitation clinic, observing sleep-position changes and wake-ups. In addition, authors reported that patient and personnel feedback were positive, especially regarding physical activity and sleep monitoring. Finally, Silva de Lima, in [99], presented their project and platform, feasibility study and recruiting procedure. Their system relied on a smartwatch connected to a smartphone to detect and analyze sleep movements.
3.3. Sleep Quality and Movement Analysis
In the literature, studies focused on sleep-quality evaluation and movements in sleep were found mainly addressed to PD, Friedreich ataxia and AD. The selected articles in this scope are shown in Table 5. Regarding PD, research focused on analyzing abnormal nocturnal movements during sleep. Those disturbances commonly affect PD patients because of disease-related symptoms or sleep disorders and are clinically assessed by PSG or video-PSG. Actigraphy is also commonly used for this purpose and is FDA-approved, while accelerometers and inertial sensors in various configurations have been gaining ground in this field in recent years [24,100].
Table 5.
Selected articles that present a system dedicated to neurodegenerative diseases for sleep-quality and nocturnal-movements assessment.
Boroojerdi et al., in [101], and Klingelhoefer, in [102], focus on sleep-quality evaluation in PD, assessing movements during the night. In particular, Boroojerdi et al., in [101], studied PD motor symptoms with an EMG patch and an accelerometer, evaluating sleep quality in terms of time asleep and postural changes. The authors could not find a correlation between sleep-quality measures and the sleep-diary reports of the subjects. In contrast, Klingelhoefer et al., in [102], studied the effects of disturbed nights, such as daytime sleepiness, through scores for BK and dyskinesia (DK) during sleep computed from Parkinson’s KinetiGraphTM (Global Kinectic Pty Ltd, Melbourne Victoria, Australia). The authors were able to correlate their algorithms for the definition of the quantity and quality of sleep, derived from immobility-period identification, to self-assessment reports, in the EDS affected group only. Nocturnal hypokinesia in PD was compared in [103] and [104]. Xue et al., in [103], compared standard clinical scores, such as Unified Parkinson’s Disease Rating Scale (UPDRS), Hoehn andYahr (HY), Pittsburg Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), Parkinson’s Disease Sleep Scale (PSS), with sleep-quality parameters extracted from inertial sensor analysis. They mainly considered TST, sleep efficiency and sleep turnings. In this way, they could find that sleep quality is influenced by turnings in bed and correlated to UPDRS or scores. Bhidayasiri et al., in [104], detected nocturnal movements with an inertial sensor as well. Specifically, the authors measured turning frequency and kinematic turnings parameters (e.g., degrees, velocities, accelerations). In addition, they compared turns in bed in PD patients and their spouses, finding significant impairment in PD subjects turnings (fewer, smaller, and slower turnings). The impact of PD on turning in bed was the main focus of [105] by Mirelman et al. as well. Specifically, the authors analyzed the influence of PD on sleep, obtaining information on sleep interruptions, turnings and laying from a single accelerometer, comparing data on 305 PD subjects and 205 healthy controls. In advanced PD, fewer turns, slower turns, and greater upright time were found, as expected. Moreover, newly diagnosed subjects were similar to controls in the number of turns, but differed in the speed and amplitude of turning, suggesting that this type of measurement can be used as a descriptive of disease progression and as a potential diagnostic tool.
Sleep quality and motion description were also considered relevant topics in Friedreich Ataxia by Gavriel et al. in ref. [106] and ref. [107], where a kinematic sensor network was used to assess disease progression and drug effect in an objective manner. Specific kinematic biomarkers were extracted from movement segmentation and compared with Scale for the Assessment and Rating of Ataxia (SARA) scores (standard assessing method). Finally, sleep quality was also explored in the field of dementia, where Wei et al., in [108], compared sleep-quality measures and outcomes in the presence of a dementia diagnosis and in subjects of different ages. They employed a commercial wristband together with a custom one equipped with actigraphy and temperature sensors, as shown in Figure 6a. The authors found significantly lower sleep and wake temperature difference in older adults with dementia. Furthermore, movements during sleep increased with age, and even more in the presence of dementia. Lastly, a group of innovative technologies related to RBD detection and evaluation were selected. In fact, RBD traditional assessment mainly relies on the identification of movements during the REM stage. Therefore, it requires the simultaneous identification of the REM stage and the analysis of EMG recordings, which constitutes one of the most complex procedures. Given its discovered importance in synucleinopathies, interest grew around prodromal RBD, also considering the difficulty in distinguishing it from mimics, i.e., other motor manifestations or parasomnias during sleep. An attempt at simplification was provided by Cesari and Waser in [109,110], respectively, which exploited 3D video analysis to evaluate limbs movements. They used custom algorithms to identify limb movements. The video analysis was based on the motion signal, corresponding to pixel-wise variation in the 3D video frames over time. Specifically, the authors grouped the automatically identified movements into three regions of interest (upper body, lower body, and full body) based on their duration, estimated movement features for each group and, finally, evaluated their accuracy. In addition, they correlated the estimated features, which could better discriminate isolated RBD- [111] from sleep-disordered breathing (SDB)-affected patients for each group regarding REM sleep without atonia episodes. Finally, Filardi et al., in [112], exploited the analysis of rest–wake-cycle analysis obtained from actigraphy to identify subjects with RBD and to compare their features with those of subjects presenting with symptoms that mimic RBD. A qualitative summary of these works is shown in Table 6.
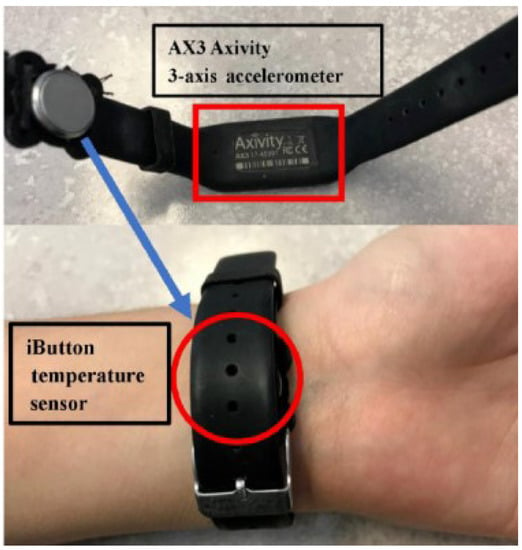
Figure 6.
Custom-built wristband for actigraphy and temperature measures, employed for sleep quality assessment. The figure is adapted from [108].
Table 6.
Selected articles that present a system dedicated to neurodegenerative diseases for nocturnal movements related to RBD.
4. Discussion and Conclusions
As discussed in the introduction section, sleep has an important role in guaranteeing a good quality of life, influencing cognitive and physical performances in healthy people and more extensively in the elderly, frail people or subjects with neurodegenerative disorders. Unobtrusive technologies for sleep monitoring are becoming the focus of many companies that develops health and well-being monitoring applications. The use of unobtrusive devices for sleep monitoring would also be of great value in the medical field, especially if applied to subjects affected by NDs, enabling more convenient and even continuous assessment of sleep-related disorders. However, analysis of the articles selected by this review showed that, in the latter area, the multiple proposed solutions still need further validation before application in clinical practice and in patients’ daily lives. In fact, many different sensors were used in the reviewed works, showing the feasibility of different sleep monitoring tools, but, it was infrequently considered how these systems could fit into the complex consolidated clinical practice related to NDs.
First, the smart-home monitoring approach, even if interesting, requires the integration of sensors, data and interactions from many stakeholders: the house owner (who is also probably the end user), the company providing the system and the clinical facility that relies on the system and provides the medical service through it. At the moment, there are few healthcare facilities that actually provide these types of telemedicine services. Moreover, the literature search highlighted many smart-home monitoring solutions aimed at ND that included sleep monitoring, but most of them involved feasibility studies or only preliminary results about sleep. Ref. [90] and ref. [94] constitute exceptions, providing results on a moderate number of subjects with cognitive impairment and AD. However, the setup employed by these solutions, consisting of a network of several sensors, presents some drawbacks. For example, the large amount of data collected from all the sensors in continuous monitoring are very difficult (and expensive) to manage and analyze to obtain clinically meaningful results. In addition, custom algorithms should consider many use cases to be robust and subject-oriented, but structured guidelines for continuous home-monitoring applications are lacking in the literature. Moreover, the overall cost could be excessively expensive even in the validation phase of the solution, making these applications apparently suffer from the bottleneck effect typical of many telemedicine solutions [113,114].
Secondly, when there are multiple needs, as in multi-disease patients, it would not be feasible to employ a single device to assess each symptom. Therefore, patients and healthcare institutions need to rely on few trusted tools. From this perspective, actigraphy and inertial sensors are the main solutions for the movement analysis of daytime and nighttime symptoms, in addition or complementary to PSG. The wide applications of these types of sensors (e.g., gait analysis, limb movements, bradykinesia, tremor) make them suitable for integration in patients’ daily life and hospitals. Indeed, they proved to be the most widespread and validated solutions. Actigraphy or “equivalent FDA approved devices that uses an accelerometer to measure limb activity associated with movement during sleep for physiologic applications” have already landed in the clinical sleep-monitoring field [115]. However, their use is always contingent on individual circumstances, such as the presence of ND. This is confirmed by the fact that the use of inertial sensors for sleep monitoring in ND is dominant between the reviewed articles, as shown in Figure 2, especially for sleep-quality assessment and movement analysis in a wearable configuration. The inertial sensors are mainly used to determine the permanence in bed, the number of sleep interruptions and the kinematic properties of the movements, such as the turning speed. This makes them good substitutes for sleep diaries, due to their ability to collect quantitative and objective information about sleep. In [102,103,104,105], inertial wearable sensors showed the ability of characterizing PD patients with respect to healthy subjects and disease progression; while in refs. [87,90], they were successfully used for AD treatment optimization and in refs. [106,107] for Ataxia characterization through the extraction of biomarkers correlated to standard scores. The feasibility and the importance of sleep evaluations in patients with ND is, therefore, undoubtable, but a structured protocol of assessment that exploits these sensors has still to be established. For instance, hte optimized number and positioning of inertial sensors in the different disciplines is still to be defined. Fewer sensors would provide a cheaper and more convenient solution, but may not provide sufficient sensitivity to events of interest (e.g., the accelerometer on the arm may ignore foot/limb movements), not to mention that the events of interest depend on the analysis to be performed, which is not always completely defined a priori. Bed sensors are known to be able to provide information on bed occupancy and nighttime movements [116], but no articles presenting their use in ND other than AD were found in the literature search.
A separate discussion should be conducted on movement detection during REM phase to assess REM sleep without atonia for the diagnosis of RBD. In this literature search, two main approaches were found in this direction: 3D-video analysis [109,110] and actigraphy [112]. Both of them showed good performance and are cost-effective solutions. However, they need prior sleep-stage scoring (such as REM-stage recognition for 3D video analysis) or manual event tagging (such as day–night stage recognition for actigraphy). The potential of this type of screening is huge due to the possibility of observing other types of movements of clinical interest, such as thorax/abdomen movements during breathing, or turnings in bed. Therefore, these technologies are a promising line of research that should be further explored, while also considering mixed approaches. Lastly, the selected articles about automatic sleep staging showed interesting results using several types of sensors. However, the samples tested are not sufficient to evaluate a trend in this category. For example, in refs. [81,82,83], only healthy subjects were enrolled, with sample sizes ranging from 5 to 12 subjects. In contrast, ref. [84] included PD subjects but did not provide an accuracy comparison with PSG results.
To conclude, the literature research conducted in this review seems to demonstrate the feasibility of many different types of unobtrusive methods and technologies for sleep monitoring in ND, but further exploration needs to be performed to better establish the possibilities and limitations of these solutions in this specific scenario. Furthermore, a structured revision of the possible intersection with the actual clinical practice should be considered in order to select and adapt the possible solutions capable to cover, for each neurodegenerative disorder, the widest possible number of their clinical needs.
Author Contributions
Conceptualization, G.M., C.F. and G.A.; methodology, G.M. and C.F.; formal analysis, G.M. and C.F.; investigation, G.M.; resources, G.M.; writing—original draft preparation, G.M. and G.A.; writing—review and editing, G.M., C.F., G.A. and L.P.; visualization, G.M. and G.A.; supervision, C.F. and L.P.; project administration, L.P.; funding acquisition, L.P. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Department of Excellence Grant of the Italian Ministry of Education, University and Research to the ’Rita Levi Montalcini’ Department of Neuroscience, University of Torino, Italy.
Data Availability Statement
Not applicable.
Acknowledgments
G.M. would like to to thank Rechichi I. for her mentoring and inspiration in this field.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AD | Alzheimer’s disease |
| ADL | activity of daily living |
| ALS | amyotrophic lateral sclerosis |
| BK | bradykinesia |
| CAP | cyclic alternating pattern |
| DK | dyskinesia |
| CNN | convolutional neural network |
| CNS | central nervous system |
| DL | deep learning |
| DLB | dementia with Lewy body |
| ECG | electrocardiography |
| EDS | excessive daytime sleepiness |
| EEG | electroencephalography |
| EMG | electromyography |
| EOG | electrooculography |
| ESS | Epworth Sleepiness Scale |
| FDA | American Food and Drug Administration |
| GPS | global positioning system |
| HY | Hoehn andYahr |
| IoT | Internet of Things |
| k-NN | k-nearest neighbour |
| LSTM | long short-term memory |
| MCI | mild cognitive impairment |
| MSA | multiple system atrophy |
| ND | neurodegenerative diseases |
| NREM | non-REM |
| ORCATECH | Oregon Center for Aging and Technology |
| OSA | obstructive sleep apnea |
| PD | Parkinson’s disease |
| PLMS | periodic leg movements in sleep |
| PSG | polysomnography |
| PSQI | Pittsburg Sleep Quality Index |
| PSS | Parkinson’s Disease Sleep Scale |
| RBD | REM sleep behavior disorder |
| REM | rapid eye movements |
| RFID | radio frequency identification |
| RLS | restless legs syndrome |
| SARA | Scale for the Assessment and Rating of Ataxia |
| SD | sleep disorders incidence |
| SDB | sleep-disordered breathing |
| SVM | support vector machine |
| TST | total sleep time |
| UPDRS | Unified Parkinson’s Disease Rating Scale |
| WASO | wake after sleep onset |
References
- Killgore, W.D.S. Effects of sleep deprivation on cognition. Prog. Brain Res. 2010, 185, 105–129. [Google Scholar]
- Spiegel, K. Effect of sleep deprivation on response to immunizaton. JAMA 2002, 288, 1471–1472. [Google Scholar] [CrossRef]
- Knutson, K.L.; Spiegel, K.; Penev, P.; Van Cauter, E. The metabolic consequences of sleep deprivation. Sleep Med. Rev. 2007, 11, 163–178. [Google Scholar] [CrossRef] [PubMed]
- Halász, P. Hierarchy of micro-arousals and the microstructure of sleep. Neurophysiol. Clin. Neurophysiol. 1998, 28, 461–475. [Google Scholar] [CrossRef]
- Parrino, L.; Ferrillo, F.; Smerieri, A.; Spaggiari, M.C.; Palomba, V.; Rossi, M.; Terzano, M.G. Is insomnia a neurophysiological disorder? The role of sleep EEG microstructure. Brain Res. Bull. 2004, 63, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disturbances and chronic disease in older adults: Results of the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Iranzo, A.; Santamaria, J. Sleep in Neurodegenerative Diseases. In Sleep Medicine; Springer: New York, NY, USA, 2015; pp. 271–283. [Google Scholar]
- Iranzo, A. Sleep in dementia and other neurodegenerative diseases. In Sleep Disorders in Neurology; John Wiley & Sons Ltd.: Chichester, UK, 2018; pp. 229–240. [Google Scholar]
- Abbott, S.M.; Videnovic, A. Chronic sleep disturbance and neural injury: Links to neurodegenerative disease. Nat. Sci. Sleep 2016, 8, 55–61. [Google Scholar]
- Priano, L.; Bigoni, M.; Albani, G.; Sellitti, L.; Giacomotti, E.; Picconi, R.; Cremascoli, R.; Zibetti, M.; Lopiano, L.; Mauro, A. Sleep microstructure in Parkinson’s disease: Cycling alternating pattern (CAP) as a sensitive marker of early NREM sleep instability. Sleep Med. 2019, 61, 57–62. [Google Scholar] [CrossRef]
- Iranzo, A. Sleep in neurodegenerative diseases. Sleep Med. Clin. 2016, 11, 1–18. [Google Scholar] [CrossRef]
- Mendonca, F.; Mostafa, S.S.; Ravelo-Garcia, A.G.; Morgado-Dias, F.; Penzel, T. A review of obstructive sleep apnea detection approaches. IEEE J. Biomed. Health Inform. 2019, 23, 825–837. [Google Scholar] [CrossRef]
- Younes, M.; Raneri, J.; Hanly, P. Staging sleep in polysomnograms: Analysis of inter-scorer variability. J. Clin. Sleep Med. 2016, 12, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Miladinović, Đ.; Muheim, C.; Bauer, S.; Spinnler, A.; Noain, D.; Bandarabadi, M.; Gallusser, B.; Krummenacher, G.; Baumann, C.; Adamantidis, A.; et al. SPINDLE: End-to-end learning from EEG/EMG to extrapolate animal sleep scoring across experimental settings, labs and species. PLoS Comput. Biol. 2019, 15, e1006968. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The emerging evidence of the Parkinson pandemic. J. Parkinsons. Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Raggi, A.; Ferri, R. Sleep disorders in neurodegenerative diseases: Sleep in neurodegenerative diseases. Eur. J. Neurol. 2010, 17, 1326–1338. [Google Scholar] [CrossRef]
- Fifel, K.; Videnovic, A. Circadian and sleep dysfunctions in neurodegenerative disorders-an update. Front. Neurosci. 2020, 14, 627330. [Google Scholar] [CrossRef]
- Zhang, Y.; Ren, R.; Yang, L.; Zhang, H.; Shi, Y.; Okhravi, H.R.; Vitiello, M.V.; Sanford, L.D.; Tang, X. Sleep in Alzheimer’s disease: A systematic review and meta-analysis of polysomnographic findings. Transl. Psychiatry 2022, 12, 136. [Google Scholar] [CrossRef] [PubMed]
- Lyons, B.E.; Austin, D.; Seelye, A.; Petersen, J.; Yeargers, J.; Riley, T.; Sharma, N.; Mattek, N.; Dodge, H.; Wild, K.; et al. Corrigendum: Pervasive computing technologies to continuously assess Alzheimer’s disease progression and intervention efficacy. Front. Aging Neurosci. 2015, 7, 232. [Google Scholar] [CrossRef] [PubMed]
- Voysey, Z.J.; Barker, R.A.; Lazar, A.S. The treatment of sleep dysfunction in neurodegenerative disorders. Neurotherapeutics 2021, 18, 202–216. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders—Third Edition (ICSD-3); American Academy of Sleep Medicine (AASM): Darien, IL, USA, 2014. [Google Scholar]
- Wood, E.A.; McCall, W.V. Assessment methodologies in sleep medicine clinical trials. Clin. Investig. 2013, 3, 791–800. [Google Scholar] [CrossRef]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to interpret the results of a sleep study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef]
- Zampogna, A.; Manoni, A.; Asci, F.; Liguori, C.; Irrera, F.; Suppa, A. Shedding light on nocturnal movements in Parkinson’s disease: Evidence from wearable technologies. Sensors 2020, 20, 5171. [Google Scholar] [CrossRef]
- Urrestarazu, E.; Iriarte, J. Clinical management of sleep disturbances in Alzheimer’s disease: Current and emerging strategies. Nat. Sci. Sleep 2016, 8, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Claassen, D.; Josephs, K.; Ahlskog, J.; Silber, M.; Tippmann-Peikert, M.; Boeve, B. Rem sleep behavior disorder preceding other aspects of synucleinopathies by up to half a century. Neurology 2011, 77, 1155. [Google Scholar] [CrossRef]
- Magrinelli, F.; Picelli, A.; Tocco, P.; Federico, A.; Roncari, L.; Smania, N.; Zanette, G.; Tamburin, S. Pathophysiology of motor dysfunction in Parkinson’s disease as the rationale for drug treatment and rehabilitation. Parkinsons Dis. 2016, 2016, 9832839. [Google Scholar] [CrossRef] [PubMed]
- Lajoie, A.C.; Lafontaine, A.L.; Kaminska, M. The spectrum of sleep disorders in Parkinson disease: A review. Chest 2021, 159, 818–827. [Google Scholar] [CrossRef]
- Lin, J.Y.; Zhang, L.Y.; Cao, B.; Wei, Q.Q.; Ou, R.W.; Hou, Y.B.; Liu, K.C.; Xu, X.R.; Jiang, Z.; Gu, X.J.; et al. Sleep-related symptoms in multiple system atrophy: Determinants and impact on disease severity. Chin. Med. J. 2020, 134, 690–698. [Google Scholar] [CrossRef]
- Ferman, T.J.; Smith, G.E.; Dickson, D.W.; Graff-Radford, N.R.; Lin, S.C.; Wszolek, Z.; Van Gerpen, J.A.; Uitti, R.; Knopman, D.S.; Petersen, R.C.; et al. Abnormal daytime sleepiness in dementia with Lewy bodies compared to Alzheimer’s disease using the Multiple Sleep Latency Test. Alzheimer Res. Ther. 2014, 6, 76. [Google Scholar] [CrossRef]
- Duncan, M.J.; Veasey, S.C.; Zee, P. Editorial: Roles of sleep disruption and circadian rhythm alterations on neurodegeneration and Alzheimer’s disease. Front. Neurosci. 2021, 15, 737895. [Google Scholar] [CrossRef]
- Herzog-Krzywoszanska, R.; Krzywoszanski, L. Sleep disorders in Huntington’s disease. Front. Psychiatry 2019, 10, 221. [Google Scholar] [CrossRef]
- Boentert, M. Sleep disturbances in patients with amyotrophic lateral sclerosis: Current perspectives. Nat. Sci. Sleep 2019, 11, 97–111. [Google Scholar] [CrossRef]
- Corben, L.A.; Ho, M.; Copland, J.; Tai, G.; Delatycki, M.B. Increased prevalence of sleep-disordered breathing in Friedreich ataxia. Neurology 2013, 81, 46–51. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef]
- Kohnen, R.; Allen, R.P.; Benes, H.; Garcia-Borreguero, D.; Hening, W.A.; Stiasny-Kolster, K.; Zucconi, M. Assessment of restless legs syndrome—Methodological approaches for use in practice and clinical trials. Mov. Disord. 2007, 22, S485–S494. [Google Scholar] [CrossRef] [PubMed]
- Skorvanek, M.; Feketeova, E.; Kurtis, M.M.; Rusz, J.; Sonka, K. Accuracy of rating scales and clinical measures for screening of rapid eye movement sleep behavior disorder and for predicting conversion to Parkinson’s disease and other synucleinopathies. Front. Neurol. 2018, 9, 376. [Google Scholar] [CrossRef] [PubMed]
- McWhirter, D.; Bae, C.; Budur, K. The assessment, diagnosis, and treatment of excessive sleepiness: Practical considerations for the psychiatrist. Psychiatry 2007, 4, 26–35. [Google Scholar]
- Riek, L.D. Healthcare robotics. Commun. ACM 2017, 60, 68–78. [Google Scholar] [CrossRef]
- Sivaparthipan, C.B.; Muthu, B.A.; Manogaran, G.; Maram, B.; Sundarasekar, R.; Krishnamoorthy, S.; Hsu, C.H.; Chandran, K. Innovative and efficient method of robotics for helping the Parkinson’s disease patient using IoT in big data analytics. Trans. Emerg. Telecommun. Technol. 2020, 31, e3838. [Google Scholar] [CrossRef]
- Moro, C.; Štromberga, Z.; Raikos, A.; Stirling, A. The effectiveness of virtual and augmented reality in health sciences and medical anatomy: VR and AR in Health Sciences and Medical Anatomy. Anat. Sci. Educ. 2017, 10, 549–559. [Google Scholar] [CrossRef]
- Walper, S.A.; Lasarte Aragonés, G.; Sapsford, K.E.; Brown, C.W., 3rd; Rowland, C.E.; Breger, J.C.; Medintz, I.L. Detecting biothreat agents: From current diagnostics to developing sensor technologies. ACS Sens. 2018, 3, 1894–2024. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lai, F.; Vespa, P. Enabling technologies facilitate new healthcare delivery models for acute stroke. Stroke 2010, 41, 1076–1078. [Google Scholar] [CrossRef] [PubMed]
- Guillodo, E.; Lemey, C.; Simonnet, M.; Walter, M.; Baca-García, E.; Masetti, V.; Moga, S.; Larsen, M.; HUGOPSY Network; Ropars, J.; et al. Clinical applications of mobile health wearable-based sleep monitoring: Systematic review. JMIR mHealth uHealth 2020, 8, e10733. [Google Scholar] [CrossRef] [PubMed]
- Rune Labs Secures FDA Clearance for Parkinson’s Disease Monitoring through StrivePD Ecosystem on Apple Watch. 2022. Available online: https://www.prnewswire.com/news-releases/rune-labs-secures-fda-clearance-for-parkinsons-disease-monitoring-through-strivepd-ecosystem-on-apple-watch-301566472.html (accessed on 16 December 2022).
- Ben-Sadoun, G.; Manera, V.; Alvarez, J.; Sacco, G.; Robert, P. Recommendations for the design of serious games in neurodegenerative diseases. Front. Aging Neurosci. 2018, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.L.M.; Mesquita, B.S.; Morais, W.S.; Leal, J.C.; Satler, C.E.; Dos Santos Mendes, F.A. Nintendo Wii™ versus Xbox Kinect™ for assisting people with Parkinson’s Disease. Percept. Mot. Skills 2018, 125, 31512518769204. [Google Scholar] [CrossRef]
- Amprimo, G.; Masi, G.; Priano, L.; Azzaro, C.; Galli, F.; Pettiti, G.; Mauro, A.; Ferraris, C. Assessment tasks and virtual exergames for remote monitoring of Parkinson’s disease: An integrated approach based on Azure Kinect. Sensors 2022, 22, 8173. [Google Scholar] [CrossRef]
- Fino, E.; Mazzetti, M. Monitoring healthy and disturbed sleep through smartphone applications: A review of experimental evidence. Sleep Breath. 2019, 23, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Qiu, L.; Wu, Y.; Tang, Y.; Cao, G. SleepMonitor: Monitoring respiratory rate and body position during sleep using smartwatch. In Proceedings of the ACM on Interactive Mobile, Wearable and Ubiquitous Technologies Association for Computing Machinery (ACM), New York, NY, USA, 11–15 September 2017; Volume 1, pp. 1–22. [Google Scholar]
- Giannakopoulou, K.M.; Roussaki, I.; Demestichas, K. Internet of Things technologies and machine learning methods for Parkinson’s disease diagnosis, monitoring and management: A systematic review. Sensors 2022, 22, 1799. [Google Scholar] [CrossRef]
- Sheikhtaheri, A.; Sabermahani, F. Applications and outcomes of Internet of Things for patients with Alzheimer’s disease/dementia: A scoping review. Biomed. Res. Int. 2022, 2022, 6274185. [Google Scholar] [CrossRef] [PubMed]
- Simonet, C.; Noyce, A.J. Domotics, smart homes, and Parkinson’s disease. J. Parkinsons. Dis. 2021, 11, S55–S63. [Google Scholar] [CrossRef] [PubMed]
- Alberdi, A.; Weakley, A.; Schmitter-Edgecombe, M.; Cook, D.J.; Aztiria, A.; Basarab, A.; Barrenechea, M. Smart home-based prediction of multidomain symptoms related to Alzheimer’s Disease. IEEE J. Biomed. Health Inform. 2018, 22, 1720–1731. [Google Scholar] [CrossRef] [PubMed]
- ROSETTA. 2012. Available online: http://www.aal-europe.eu/projects/rosetta/ (accessed on 16 December 2022).
- Home. 2014. Available online: https://www.neurodegenerationresearch.eu/ (accessed on 16 December 2022).
- Cooray, N.; Andreotti, F.; Lo, C.; Symmonds, M.; Hu, M.T.M.; De Vos, M. Proof of concept: Screening for REM sleep behaviour disorder with a minimal set of sensors. Clin. Neurophysiol. 2021, 132, 904–913. [Google Scholar] [CrossRef]
- Rechichi, I.; Zibetti, M.; Borzì, L.; Olmo, G.; Lopiano, L. Single-channel EEG classification of sleep stages based on REM microstructure. Healthc. Technol. Lett. 2021, 8, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Choi, S.H. Smart technologies toward sleep monitoring at home. Biomed. Eng. Lett. 2019, 9, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Nochino, T.; Ohno, Y.; Kato, T.; Taniike, M.; Okada, S. Sleep stage estimation method using a camera for home use. Biomed. Eng. Lett. 2019, 9, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Lin, M.; Chen, F.; Lane, N.; Cardone, G.; Wang, R.; Li, T.; Chen, Y.; Choudhury, T.; Cambell, A. Unobtrusive Sleep Monitoring using Smartphones. In Proceedings of the Proceedings of the ICTs for improving Patients Rehabilitation Research Techniques, Venice, Italy, 5–8 May 2013. [Google Scholar]
- Ya-Ti, P.; Ching-Yung, L.; Ming-Ting, S.; Landis, C.A. Multimodality sensor system for long-term sleep quality monitoring. IEEE Trans. Biomed. Circuits Syst. 2007, 1, 217–227. [Google Scholar] [CrossRef]
- Kwon, S.; Kim, H.; Yeo, W.H. Recent advances in wearable sensors and portable electronics for sleep monitoring. iScience 2021, 24, 102461. [Google Scholar] [CrossRef]
- Tran, V.P.; Al-Jumaily, A.A.; Islam, S.M.S. Doppler radar-based non-contact health monitoring for obstructive sleep apnea diagnosis: A comprehensive review. Big Data Cogn. Comput. 2019, 3, 3. [Google Scholar] [CrossRef]
- Ma, L.; Liu, S.Y.; Cen, S.S.; Li, Y.; Zhang, H.; Han, C.; Gu, Z.Q.; Mao, W.; Ma, J.H.; Zhou, Y.T.; et al. Detection of motor dysfunction with wearable sensors in patients with idiopathic rapid eye movement disorder. Front. Bioeng. Biotechnol. 2021, 9, 627481. [Google Scholar] [CrossRef]
- Febriana, N.; Rizal, A.; Susanto, E. Sleep monitoring system based on body posture movement using Microsoft Kinect sensor. In AIP Conference Proceedings; AIP Publishing LLC: New York, NY, USA, 2019. [Google Scholar]
- Lee, J.; Hong, M.; Ryu, S. Sleep monitoring system using Kinect sensor. Int. J. Distrib. Sens. Netw. 2015, 2015, 1–9. [Google Scholar] [CrossRef]
- Jakkaew, P.; Onoye, T. Non-contact respiration monitoring and body movements detection for sleep using thermal imaging. Sensors 2020, 20, 6307. [Google Scholar] [CrossRef]
- Veauthier, C.; Ryczewski, J.; Mansow-Model, S.; Otte, K.; Kayser, B.; Glos, M.; Schöbel, C.; Paul, F.; Brandt, A.U.; Penzel, T. Contactless recording of sleep apnea and periodic leg movements by nocturnal 3-D-video and subsequent visual perceptive computing. Sci. Rep. 2019, 9, 16812. [Google Scholar] [CrossRef]
- Ancona, S.; Faraci, F.D.; Khatab, E.; Fiorillo, L.; Gnarra, O.; Nef, T.; Bassetti, C.L.A.; Bargiotas, P. Wearables in the home-based assessment of abnormal movements in Parkinson’s disease: A systematic review of the literature. J. Neurol. 2022, 269, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Breasail, M.Ó.; Biswas, B.; Smith, M.D.; Mazhar, M.K.A.; Tenison, E.; Cullen, A.; Lithander, F.E.; Roudaut, A.; Henderson, E.J. Wearable GPS and accelerometer technologies for monitoring mobility and physical activity in neurodegenerative disorders: A systematic review. Sensors 2021, 21, 8261. [Google Scholar] [CrossRef] [PubMed]
- Channa, A.; Popescu, N.; Ciobanu, V. Wearable solutions for patients with Parkinson’s disease and neurocognitive disorder: A systematic review. Sensors 2020, 20, 2713. [Google Scholar] [CrossRef]
- Mughal, H.; Javed, A.R.; Rizwan, M.; Almadhor, A.S.; Kryvinska, N. Parkinson’s disease management via wearable sensors: A systematic review. IEEE Access 2022, 10, 35219–35237. [Google Scholar] [CrossRef]
- Woodberry, E.; Browne, G.; Hodges, S.; Watson, P.; Kapur, N.; Woodberry, K. The use of a wearable camera improves autobiographical memory in patients with Alzheimer’s disease. Memory 2015, 23, 340–349. [Google Scholar] [CrossRef]
- Lussier, M.; Lavoie, M.; Giroux, S.; Consel, C.; Guay, M.; Macoir, J.; Hudon, C.; Lorrain, D.; Talbot, L.; Langlois, F.; et al. Early detection of mild cognitive impairment with in-home monitoring sensor technologies using functional measures: A systematic review. IEEE J. Biomed. Health Inform. 2019, 23, 838–847. [Google Scholar] [CrossRef]
- Saner, H.; Schütz, N.; Botros, A.; Urwyler, P.; Buluschek, P.; du Pasquier, G.; Nef, T. Potential of ambient sensor systems for early detection of health problems in older adults. Front. Cardiovasc. Med. 2020, 7, 110. [Google Scholar] [CrossRef]
- Varatharajan, R.; Manogaran, G.; Priyan, M.K.; Sundarasekar, R. Wearable sensor devices for early detection of Alzheimer disease using dynamic time warping algorithm. Cluster Comput. 2018, 21, 681–690. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Del Din, S.; Galna, B.; Thomas, A.; Rochester, L. Differentiating dementia disease subtypes with gait analysis: Feasibility of wearable sensors? Gait Posture 2020, 76, 372–376. [Google Scholar] [CrossRef]
- Kourtis, L.C.; Regele, O.B.; Wright, J.M.; Jones, G.B. Digital biomarkers for Alzheimer’s disease: The mobile/ wearable devices opportunity. NPJ Digit. Med. 2019, 2, 9. [Google Scholar] [CrossRef]
- Sigcha, L.; Domínguez, B.; Borzì, L.; Costa, N.; Costa, S.; Arezes, P.; López, J.M.; De Arcas, G.; Pavón, I. Bradykinesia detection in Parkinson’s disease using smartwatches’ inertial sensors and deep learning methods. Electronics 2022, 11, 3879. [Google Scholar] [CrossRef]
- Casciola, A.A.; Carlucci, S.K.; Kent, B.A.; Punch, A.M.; Muszynski, M.A.; Zhou, D.; Kazemi, A.; Mirian, M.S.; Valerio, J.; McKeown, M.J.; et al. A deep learning strategy for automatic sleep staging based on two-channel EEG headband data. Sensors 2021, 21, 3316. [Google Scholar] [CrossRef] [PubMed]
- Shustak, S.; Inzelberg, L.; Steinberg, S.; Rand, D.; David Pur, M.; Hillel, I.; Katzav, S.; Fahoum, F.; De Vos, M.; Mirelman, A.; et al. Home monitoring of sleep with a temporary-tattoo EEG, EOG and EMG electrode array: A feasibility study. J. Neural Eng. 2019, 16, 026024. [Google Scholar] [CrossRef] [PubMed]
- Yi, R.; Enayati, M.; Keller, J.M.; Popescu, M.; Skubic, M. Non-Invasive In-Home Sleep Stage Classification Using a Ballistocardiography Bed Sensor. In Proceedings of the IEEE EMBS International Conference on Biomedical and Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019. [Google Scholar]
- Ko, Y.F.; Kuo, P.H.; Wang, C.F.; Chen, Y.J.; Chuang, P.C.; Li, S.Z.; Chen, B.W.; Yang, F.C.; Lo, Y.C.; Yang, Y.; et al. Quantification analysis of sleep based on smartwatch sensors for Parkinson’s disease. Biosensors 2022, 12, 74. [Google Scholar] [CrossRef]
- Mahoney, E.L.; Mahoney, D.F. Acceptance of wearable technology by people with Alzheimer’s disease: Issues and accommodations. Am. J. Alzheimer Dis. Other Demen. 2010, 25, 527–531. [Google Scholar] [CrossRef]
- Bate, G.; Richardson, S.; Taylor, J.P.; Burn, D.; Allan, L.; Yarnall, A.; Guan, Y.; Del-Din, S.; Lawson, R. Feasibility of using wearable sensors to monitor activity and sleep patterns in inpatients with delirium and Parkinson’s disease. Mov. Disord. 2022, 37, S365–S366. [Google Scholar]
- Lazarou, I.; Karakostas, A.; Stavropoulos, T.G.; Tsompanidis, T.; Meditskos, G.; Kompatsiaris, I.; Tsolaki, M. A novel and intelligent home monitoring system for care support of elders with cognitive impairment. J. Alzheimer Dis. 2016, 54, 1561–1591. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Meditskos, G.; Tsompanidis, T.; Andreadis, S.; Kompatsiaris, I. Dem@Home: Ambient Monitoring and Clinical Support for People Living with Dementia. In Proceedings of the 13th European Semantic Web Conference (ESWC), Crete, Greece, 29 May–2 June 2016; Volume 9989, pp. 26–29. [Google Scholar]
- Andreadis, S.; Stavropoulos, T.G.; Meditskos, G.; Kompatsiaris, I. Dem@Home: Ambient Intelligence for Clinical Support of People Living with Dementia. In Proceedings of the 13th European Semantic Web Conference (ESWC), Crete, Greece, 29 May–2 June 2016. [Google Scholar]
- Lazarou, I.; Stavropoulos, T.G.; Meditskos, G.; Andreadis, S.; Kompatsiaris, I.Y.; Tsolaki, M. Long-term impact of intelligent monitoring technology on people with cognitive impairment: An observational study. J. Alzheimer Dis. 2019, 70, 757–792. [Google Scholar] [CrossRef]
- Thomas, N.W.D.; Beattie, Z.; Marcoe, J.; Wright, K.; Sharma, N.; Mattek, N.; Dodge, H.; Wild, K.; Kaye, J. An Ecologically Valid, longitudinal, and Unbiased Assessment of Treatment Efficacy in Alzheimer disease (the EVALUATE-AD trial): Proof-of-concept study. JMIR Res. Protoc. 2020, 9, e17603. [Google Scholar] [CrossRef]
- Kikhia, B.; Stavropoulos, T.G.; Meditskos, G.; Kompatsiaris, I.; Hallberg, J.; Sävenstedt, S.; Melander, C. Utilizing ambient and wearable sensors to monitor sleep and stress for people with BPSD in nursing homes. J. Ambient Intell. Humaniz. Comput. 2018, 9, 261–273. [Google Scholar] [CrossRef]
- Rose, K.M.; Lach, J.; Perkhounkova, Y.; Gong, J.; Dandu, S.R.; Dickerson, R.; Emi, I.A.; Fan, D.; Specht, J.; Stankovic, J. Use of body sensors to examine nocturnal agitation, sleep, and urinary incontinence in individuals with Alzheimer’s disease. J. Gerontol. Nurs. 2018, 44, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Hayes, T.L.; Riley, T.; Mattek, N.; Pavel, M.; Kaye, J.A. Sleep habits in mild cognitive impairment. Alzheimer Dis. Assoc. Disord. 2014, 28, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Au-Yeung, W.T.M.; Miller, L.; Beattie, Z.; May, R.; Cray, H.V.; Kabelac, Z.; Katabi, D.; Kaye, J.; Vahia, I.V. Monitoring behaviors of patients with late-stage dementia using passive environmental sensing approaches: A case series. Am. J. Geriatr. Psychiatry 2022, 30, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rawtaer, I.; Mahendran, R.; Kua, E.H.; Tan, H.P.; Tan, H.X.; Lee, T.S.; Ng, T.P. Early detection of mild cognitive impairment with in-home sensors to monitor behavior patterns in community-dwelling senior citizens in Singapore: Cross-sectional feasibility study. J. Med. Internet Res. 2020, 22, e16854. [Google Scholar] [CrossRef]
- Abbate, S.; Avvenuti, M.; Light, J. MIMS: A minimally invasive monitoring sensor platform. IEEE Sens. J. 2012, 12, 677–684. [Google Scholar] [CrossRef]
- Branco, D.; Bouça, R.; Ferreira, J.; Guerreiro, T. Designing free-living reports for Parkinson’s disease. In Proceedings of the Extended Abstracts of the 2019 CHI Conference on Human Factors in Computing Systems—CHI EA ’19 Glasgow, Scotland, UK, 4–9 May 2019; ACM Press: New York, NY, USA, 2019. [Google Scholar]
- Silva de Lima, A.L.; Hahn, T.; de Vries, N.M.; Cohen, E.; Bataille, L.; Little, M.A.; Baldus, H.; Bloem, B.R.; Faber, M.J. Large-scale wearable sensor deployment in Parkinson’s patients: The Parkinson@home study protocol. JMIR Res. Protoc. 2016, 5, e172. [Google Scholar] [CrossRef] [PubMed]
- van Wamelen, D.J.; Sringean, J.; Trivedi, D.; Carroll, C.B.; Schrag, A.E.; Odin, P.; Antonini, A.; Bloem, B.R.; Bhidayasiri, R.; Chaudhuri, K.R.; et al. Digital health technology for non-motor symptoms in people with Parkinson’s disease: Futile or future? Parkinsonism Relat. Disord. 2021, 89, 186–194. [Google Scholar] [CrossRef]
- Boroojerdi, B.; Ghaffari, R.; Mahadevan, N.; Markowitz, M.; Melton, K.; Morey, B.; Otoul, C.; Patel, S.; Phillips, J.; Sen-Gupta, E.; et al. Clinical feasibility of a wearable, conformable sensor patch to monitor motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 61, 70–76. [Google Scholar] [CrossRef]
- Klingelhoefer, L.; Rizos, A.; Sauerbier, A.; McGregor, S.; Martinez-Martin, P.; Reichmann, H.; Horne, M.; Chaudhuri, K.R. Night-time sleep in Parkinson’s disease - the potential use of Parkinson’s KinetiGraph: A prospective comparative study. Eur. J. Neurol. 2016, 23, 1275–1288. [Google Scholar] [CrossRef]
- Xue, F.; Wang, F.Y.; Mao, C.J.; Guo, S.P.; Chen, J.; Li, J.; Wang, Q.J.; Bei, H.Z.; Yu, Q.; Liu, C.F. Analysis of nocturnal hypokinesia and sleep quality in Parkinson’s disease. J. Clin. Neurosci. 2018, 54, 96–101. [Google Scholar] [CrossRef]
- Bhidayasiri, R.; Sringean, J.; Taechalertpaisarn, P.; Thanawattano, C. Capturing nighttime symptoms in Parkinson disease: Technical development and experimental verification of inertial sensors for nocturnal hypokinesia. J. Rehabil. Res. Dev. 2016, 53, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Hillel, I.; Rochester, L.; Del Din, S.; Bloem, B.R.; Avanzino, L.; Nieuwboer, A.; Maidan, I.; Herman, T.; Thaler, A.; et al. Tossing and turning in bed: Nocturnal movements in Parkinson’s disease: Nocturnal movement in pd. Mov. Disord. 2020, 35, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Gavriel, C.; Thomik, A.A.C.; Lourencco, P.R.; Nageshwaran, S.; Athanasopoulos, S.; Sylaidi, A.; Festenstein, R.; Faisal, A.A. Kinematic body sensor networks and behaviourmetrics for objective efficacy measurements in neurodegenerative disease drug trials. In Proceedings of the 2015 IEEE 12th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Cambridge, MA, USA, 9–12 June 2015. [Google Scholar]
- Gavriel, C.; Thomik, A.A.C.; Lourenco, P.R.; Nageshwaran, S.; Athanasopoulos, S.; Sylaidi, A.; Festenstein, R.; Faisal, A.A. Towards neurobehavioral biomarkers for longitudinal monitoring of neurodegeneration with wearable body sensor networks. In Proceedings of the 2015 7th International IEEE/EMBS Conference on Neural Engineering (NER), Montpellier, France, 22–24 April 2015. [Google Scholar]
- Wei, J.; Boger, J. Sleep detection for younger adults, healthy older adults, and older adults living with dementia using wrist temperature and actigraphy: Prototype testing and case study analysis. JMIR mHealth uHealth 2021, 9, e26462. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Kohn, B.; Holzknecht, E.; Ibrahim, A.; Heidbreder, A.; Bergmann, M.; Brandauer, E.; Hogl, B.; Garn, H.; Stefani, A. Automatic 3D video analysis of upper and lower body movements to identify isolated REM sleep behavior disorder: A pilot study. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 7050–7053. [Google Scholar] [PubMed]
- Waser, M.; Stefani, A.; Holzknecht, E.; Kohn, B.; Hackner, H.; Brandauer, E.; Bergmann, M.; Taupe, P.; Gall, M.; Garn, H.; et al. Automated 3D video analysis of lower limb movements during REM sleep: A new diagnostic tool for isolated REM sleep behavior disorder. Sleep 2020, 43, zsaa100. [Google Scholar] [CrossRef]
- Högl, B.; Stefani, A.; Videnovic, A. Idiopathic REM sleep behaviour disorder and neurodegeneration—An update. Nat. Rev. Neurol. 2018, 14, 40–55. [Google Scholar] [CrossRef]
- Filardi, M.; Stefani, A.; Holzknecht, E.; Pizza, F.; Plazzi, G.; Högl, B. Objective rest-activity cycle analysis by actigraphy identifies isolated rapid eye movement sleep behavior disorder. Eur. J. Neurol. 2020, 27, 1848–1855. [Google Scholar] [CrossRef]
- Hjelm, N.M. Benefits and drawbacks of telemedicine. J. Telemed. Telecare 2005, 11, 60–70. [Google Scholar] [CrossRef]
- Dhanvijay, M.M.; Patil, S.C. Internet of Things: A survey of enabling technologies in healthcare and its applications. Comput. Netw. 2019, 153, 113–131. [Google Scholar] [CrossRef]
- Smith, M.T.; McCrae, C.S.; Cheung, J.; Martin, J.L.; Harrod, C.G.; Heald, J.L.; Carden, K.A. Use of Actigraphy for the Evaluation of Sleep Disorders and Circadian Rhythm Sleep-Wake Disorders: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med.. 2018, 14, 1231–1237. [Google Scholar] [CrossRef]
- Conti, M.; Orcioni, S.; Madrid, N.M.; Gaiduk, M.; Seepold, R. A review of health monitoring systems using sensors on bed or cushion. In Bioinformatics and Biomedical Engineering; Springer International Publishing: Cham, Switzerland, 2018; pp. 347–358. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).