Abstract
Antibiotic misuse in Romania has exacerbated the issue of antibiotic resistance, as patients often use antibiotics without proper medical consultation. This study aimed to assess the resistance of prevalent bacteria to different antibiotics. In this observational study conducted over six months, we analyzed 31 pediatric patients aged from 12 days to 13 years using the disk diffusion method. We identified 31 bacterial isolates, including 8 Gram-negative and 8 Gram-positive strains, with the most common being Pseudomonas aeruginosa, Escherichia coli, Streptococcus pneumoniae, methicillin-resistant Staphylococcus aureus, Streptococcus species, and Elizabethkingia meningoseptica. Our findings revealed that the most effective antibiotics were linezolid, ertapenem, and teicoplanin. In contrast, nearly all tested bacteria exhibited resistance to penicillin, followed by oxacillin and ampicillin. Resistance to cephalosporins varied with generation, showing higher resistance to lower-generation cephalosporins. The study highlights significant antibiotic resistance among common bacterial pathogens in Romanian pediatric patients, emphasizing the urgent need for controlled antibiotic use and alternative treatment strategies to combat this growing issue. Effective antibiotics such as linezolid and ertapenem offer potential solutions, whereas reliance on penicillin and lower-generation cephalosporins is increasingly futile.
1. Introduction
Antimicrobial resistance (AMR) and the continued presence of resistant strains increase the risk of treatment failure and recurrent infections [1]. Infections due to antibiotic-resistant bacteria are currently responsible for around 700,000 deaths worldwide each year. This figure is expected to exceed 10 million annual deaths by 2050 [2,3]. The availability of antibiotic treatments has significantly lowered mortality rates, leading to an overall rise in life expectancy [4]. However, the improper use of antibiotics has led to the emergence of multidrug-resistant (MDR) bacteria [5]. A strong association between AMR and various socioeconomic factors has been observed [6], highlighting a bidirectional relationship between antibiotic consumption and the development of resistance in both animals and humans, particularly in low- and low–middle-income countries (LMICs). This emphasizes the urgent need for integrated control strategies aimed at preventing transmission across multiple sectors within the One Health framework [7], and the necessity for enhanced surveillance and control measures to combat AMR in LMICs [8,9]. In clinical environments, conducting an antibiogram prior to prescribing antibiotics allows healthcare providers to choose the most appropriate antibiotic by identifying the specific bacteria responsible for the infection and their sensitivity to various antibiotics, thereby ensuring optimal treatment outcomes [10]. Additionally, tailoring treatments based on antibiogram results helps combat antibiotic resistance [11], reduces the likelihood of promoting antibiotic-resistant bacterial strains, decreases the incidence of related adverse reactions, and shortens hospital stays [12]. In Romania, the issue of AMR is critical, with 4300 deaths attributable to AMR and 16,500 deaths associated with it reported in 2019. This makes Romania the country with the highest age-standardized mortality rate due to AMR in the Central Europe GBD region, surpassing deaths from various other diseases including digestive and respiratory conditions. Notably, five key pathogens are particularly concerning due to their association with AMR deaths: Escherichia coli (E. coli) (4000 deaths), Staphylococcus aureus (S. aureus) (3100), Klebsiella pneumoniae (2300), Pseudomonas aeruginosa (P. aeruginosa) (1700), and Streptococcus pneumoniae (S. pneumoniae) (1200). These pathogens are known to cause severe infections such as bloodstream infections, peritoneal and intra-abdominal infections, lower respiratory infections, and thoracic-related infections [13]. Our study, which included performing antibiograms on 31 pediatric patients ranging in age from 12 days to 13 years, aimed to identify the most effective antibiotics against some of the most common bacteria and determine which are the most common bacterial strains. We detected a total of 16 different bacteria, most frequently including methicillin-resistant Staphylococcus aureus (MRSA) (11 cases), P. aeruginosa (10 cases), Klebsiella sp., (10 cases), S. pneumoniae (9 cases), and E. coli (7 cases). These findings closely align with national data, highlighting the predominance of these pathogens in AMR-related infections. In our study, more than 50 antibiotics were tested across major classes, including penicillins, cephalosporins, carbapenems, macrolides, tetracyclines, aminoglycosides, fluoroquinolones, sulfonamides, oxazolidinones, polypeptides, nitrofurans, and glycopeptides. Based on the data from all patients, the results revealed that the most effective antibiotics were linezolid, ertapenem, and teicoplanin. Conversely, most bacterial strains were resistant to penicillin, oxacillin, and ampicillin. Additionally, resistance to cephalosporins varied by generation, with higher resistance observed in lower-generation cephalosporins. This targeted approach to antibiotic selection is crucial in combating AMR. Understanding which bacteria are most common and their resistance patterns helps in crafting effective treatment protocols and informs public health strategies. Our study underscores the urgent need for continued surveillance and the strategic use of antibiotics to mitigate the rising threat of AMR, particularly in countries like Romania, where the impact is profoundly felt [14].
2. Results
This study aimed to determine bacterial resistance patterns in our patients, examining a diverse array of age groups and diagnoses. From infants merely days old to adolescents on the cusp of adulthood at 13 years, this study captured a wide range of cases. Throughout the study, a plethora of pathogens emerged (Table 1), including but not limited to E. coli, Klebsiella, MRSA, Acinetobacter spp., and Proteus spp. The primary diagnoses encompassed a myriad of ailments, such as bronchopneumonia, acute respiratory infections (ARI), sepsis, urinary tract infections (UTIs), and various other infections (Figure 1). The prevalence and resistance patterns of these pathogens underscore the complexity of infectious diseases in pediatric patients, necessitating a nuanced approach to treatment strategies. Through comprehensive analysis, this study aimed to elucidate the most effective antibiotics against these pathogens, thereby informing more targeted and efficacious treatment modalities for pediatric infections (Figure 2). Each diagnosis presented a unique challenge, with pathogens exhibiting varying degrees of resistance. Infants as young as 12 days old were afflicted with bronchopneumonia, ARI, and acute rhinopharyngitis, grappling with pathogens such as MSSA, S. pneumoniae, and Streptococcus sp. Meanwhile, toddlers at the age of one year faced acute viral pneumonia, ARI, and severe dystrophy, contending with formidable adversaries like Acinetobacter baumannii (A. baumannii), MRSA, P. aeruginosa, and Elizabethkingia meningoseptica (E. meningoseptica). The microbial landscape remained dynamic across different age groups and diagnoses. From UTIs and acute diarrheal illnesses in three-month-old infants to sepsis originating from the lungs and bronchopneumonia in four-year-olds, each case presented a unique pathogenic profile. Additionally, older children were not spared, with cases ranging from bullous impetigo and acute conjunctivitis to sepsis accompanying acute lymphoblastic leukemia (Figure 3A,B).

Table 1.
Patient demographics, diagnoses, and identified bacterial pathogens.
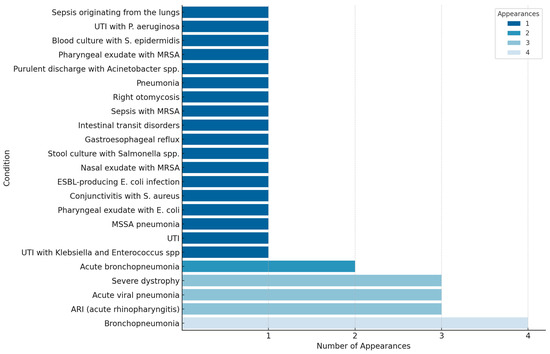
Figure 1.
Frequency distribution of pediatric conditions by number of appearances.
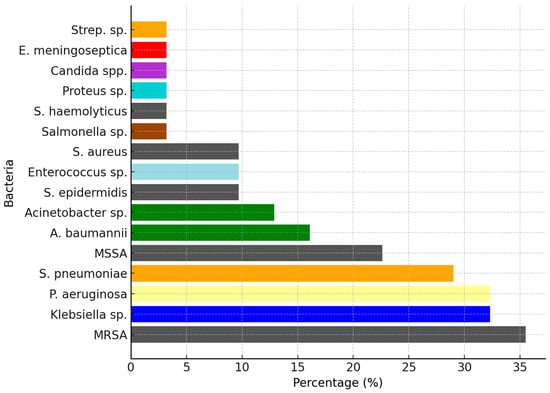
Figure 2.
Percentages of different bacterial pathogens identified in the study population, representing the global proportion of each bacterial type across all pathologies. Bacterial species have been highlighted with distinct colors (Staphylococcus species: gray; Acinetobacter species: green; Streptococcus species: orange).
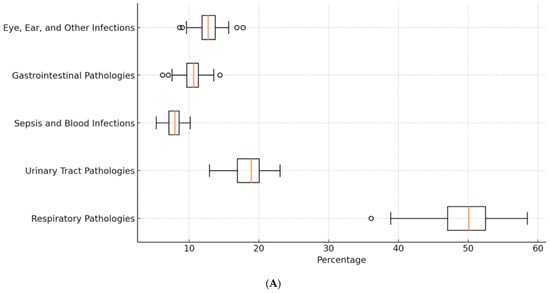
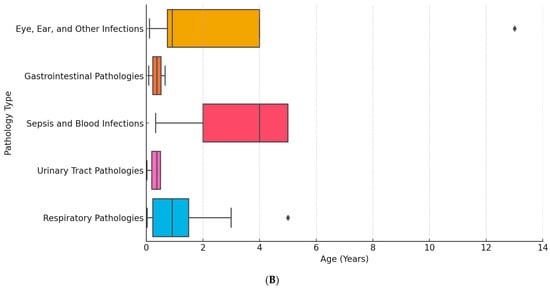
Figure 3.
(A) Percentages of different pathologies diagnosed in our patients. (B) Age distribution of pathologies in pediatric patients.
In the cases of MRSA, among the antibiotics showing consistently high activity (Figure 4) in 10 patients were tigecycline and linezolid. These antibiotics consistently demonstrated effectiveness against MRSA infections, indicating their potency in treating such cases. On the other hand, several antibiotics consistently showed resistance across all 10 patients, including oxacillin, penicillin, and rifampicin, indicating their limited efficacy against MRSA infections in this patient cohort. Overall, tigecycline and linezolid emerged as the most promising antibiotics for treating MRSA infections in this dataset, showcasing consistently high activity against the bacteria. Conversely, oxacillin, penicillin, and rifampicin appeared to be the least effective options, consistently demonstrating resistance across all patients (Table 2). This highlights the importance of judicious antibiotic selection based on susceptibility patterns to optimize treatment outcomes in MRSA infections.
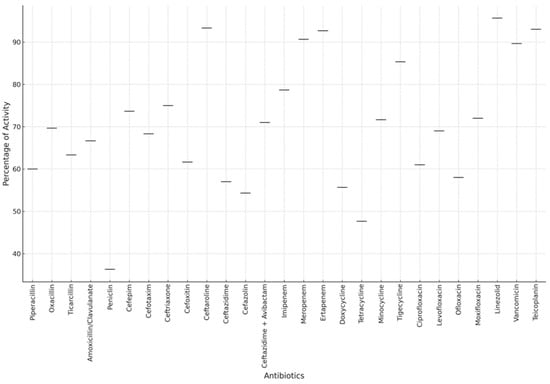
Figure 4.
Global antibiotic activity against bacterial pathogens in pediatric patients.
Table 2.
Age, diagnosis, detected pathogens, and the effectiveness of various antibiotic classes.
The ten most active antibiotics were as follows: linezolid—10 patients; tigecycline—10 patients; gentamicin—9 patients; levofloxacin—8 patients; ofloxacin—8 patients; teicoplanin—7 patients; amikacin—7 patients; daptomycin—7 patients. Resistant antibiotics: oxacillin—10 patients; penicillin—10 patients; rifampicin—9 patients; Biseptol (trimethoprim/sulfamethoxazole)—8 patients; clarithromycin—8 patients; erythromycin—8 patients; clindamycin—8 patients; doxycycline—8 patients; tetracycline—8 patients; ampicillin—7 patients.
P. aeruginosa infections were assessed using a broad spectrum of antibiotics. The antibiotics tested included ciprofloxacin, chloramphenicol, meropenem, amikacin, aztreonam, colistin, gentamicin, imipenem, levofloxacin, ofloxacin, ticarcillin, tazocin (piperacillin/tazobactam), tobramycin, cefepime, ceftazidime, ceftazidime + avibactam, cefuroxime, clindamycin, doxycycline, erythromycin, Biseptol (trimethoprim/sulfamethoxazole), and rifampicin. This analysis highlights the importance of tailored antibiotic therapy based on individual susceptibility profiles. Meropenem, gentamicin, colistin, ciprofloxacin, levofloxacin, and tazocin were among the most effective antibiotics, demonstrating high activity across a significant number of patients. Conversely, cefepime, imipenem, and piperacillin/tazobactam showed varying levels of resistance, indicating the need for careful selection based on susceptibility testing to optimize treatment outcomes. Notably, some antibiotics exhibited both high activity in certain patients and resistance in others, underscoring the complexity of treating P. aeruginosa infections. For instance, ciprofloxacin demonstrated high activity in six patients (patients 1, 3, 16, 19, 21, and 26) but showed resistance in one patient (patient 14). Similarly, meropenem exhibited high activity in seven patients (patients 1, 3, 14, 21, 26, 30, and 31) while being resistant in one patient (patient 16). Imipenem showed high activity in five patients (patients 1, 3, 14, 16, 21, and 26) but was resistant in two patients (patients 13 and 31). This variability highlights the importance of conducting susceptibility testing for each patient to ensure the selection of the most effective antibiotic therapy. Resistance to carbapenems in this study is attributed to the presence of a type of P. aeruginosa that produces carbapenemases, and resistance was observed exclusively in these cases. Based on the data provided, the most efficient antibiotics for treating P. aeruginosa infections include meropenem, gentamicin, colistin, imipenem, amikacin, and tobramycin. These antibiotics demonstrated high activity against the pathogen in multiple patients, highlighting their effectiveness as treatment options. Conversely, the least efficient antibiotics were rifampicin, ciprofloxacin, ofloxacin, cefepime, and tigecycline, which exhibited resistance in some cases, indicating limited effectiveness in treating P. aeruginosa infections.
Based on data from nine patients with S. pneumoniae infections, several antibiotics demonstrated high efficacy across multiple cases. Cefepime, cefotaxime, ceftriaxone, linezolid, and vancomycin were highly active in all nine patients, making them top choices for treatment. Clindamycin, chloramphenicol, erythromycin, rifampicin, imipenem, meropenem, and moxifloxacin were also effective in multiple cases. However, resistance was observed with penicillin in five patients and clarithromycin in several others. Biseptol showed resistance in seven patients, while levofloxacin and ofloxacin were resistant in four patients each. Doxycycline and tetracycline showed resistance in five patients each, highlighting their limited efficacy. Linezolid remained highly effective in seven patients but showed resistance in two, while vancomycin was effective in eight out of nine patients, with one showing resistance. These results underscore the complexity of treating S. pneumoniae infections, where antibiotic effectiveness varies and careful selection based on susceptibility is crucial.
For the seven patients with E. coli infections, ciprofloxacin, meropenem, and imipenem consistently showed high activity. Gentamicin and amikacin were effective in five patients each, and ceftazidime/ceftazidime + avibactam, along with aztreonam, also showed high activity in multiple cases, making them reliable treatment options.
Several antibiotics were found to be less effective, with high resistance rates in multiple cases. Ampicillin showed resistance in four patients, indicating that it is often ineffective against E. coli. Unasyn (ampicillin/sulbactam) and Augmentin (amoxicillin/clavulanate) were resistant in three and two patients, respectively, highlighting reduced efficacy. Cefazolin, tetracycline, and chloramphenicol exhibited resistance in two patients each. Tobramycin, while effective in some cases, showed resistance in one patient, indicating that it may not always be reliable. Cefepime displayed high activity in some patients but resistance in others, and Tazocin (piperacillin/tazobactam) also showed varying results. This variability emphasizes the need for careful antibiotic selection based on individual susceptibility. Overall, ciprofloxacin, meropenem, imipenem, gentamicin, amikacin, ceftazidime/ceftazidime + avibactam, and aztreonam were the most efficient antibiotics for E. coli, while ampicillin, Unasyn, Augmentin, cefazolin, tetracycline, chloramphenicol, and tobramycin were less effective, highlighting the importance of tailored antibiotic therapy. An examination of the data from the seven patients infected with methicillin-sensitive Staphylococcus aureus (MSSA) highlights several antibiotics demonstrating notable activity against the pathogen, alongside instances of resistance, illuminating the complexities in treating MSSA infections. The antimicrobial susceptibility testing conducted on MSSA revealed varying levels of effectiveness and resistance among the antibiotics tested. Among the most effective antibiotics were amikacin, ciprofloxacin, clarithromycin, clindamycin, chloramphenicol, erythromycin, gentamicin, linezolid, moxifloxacin, and oxacillin, each demonstrating substantial activity against MSSA across multiple cases. Conversely, several antibiotics encountered significant resistance, including ampicillin, piperacillin, penicillin, and Biseptol, highlighting their limited efficacy in combating MSSA infections. These findings underscore the importance of tailored antibiotic selection for MSSA infections.
For instance, amikacin demonstrated high activity in patient 2, indicating its efficacy in this case. However, resistance was observed in patients 6 and 8, underscoring the variability in antibiotic effectiveness against MSSA. Similarly, linezolid exhibited high activity in patients 2, 6, and 8, suggesting its effectiveness as a treatment option. Nonetheless, resistance to linezolid was observed in patient 25, emphasizing the challenges in managing MSSA infections and the need for tailored treatment strategies.
Conversely, certain antibiotics encountered resistance in multiple cases, indicating limitations in their efficacy against MSSA. Ampicillin, piperacillin, and penicillin showed resistance in patients 2 and 6, highlighting their reduced effectiveness against MSSA infections. These findings underscore the complexities involved in treating MSSA infections, where antibiotic effectiveness varies between patients. The observed resistance further emphasizes the importance of judicious antibiotic selection based on individual susceptibility profiles to optimize treatment outcomes.
The antimicrobial susceptibility testing for A. baumannii across five patients revealed diverse responses to various antibiotics, reflecting the complexity of managing infections caused by this pathogen. Notably, certain antibiotics exhibited robust activity in some patients while encountering resistance in others, illustrating the variability in treatment efficacy. Among the antibiotics showing notable effectiveness were Unasyn (three patients), ceftazidime + avibactam (two patients), tigecycline (one patient), tobramycin (two patients), colistin (four patients), and Biseptol (four patients), which demonstrated substantial activity against A. baumannii in multiple cases. Conversely, several antibiotics encountered significant resistance, including doxycycline (one patient), ciprofloxacin (one patient), cefepime (two patients), ceftazidime (two patients), ceftriaxone (one patient), gentamicin (one patient), levofloxacin (one patient), meropenem (one patient), and tazocin (one patient), highlighting their limited efficacy against this pathogen.
The antimicrobial susceptibility testing for Acinetobacter species, based on data from three patients, revealed varied responses to different antibiotics, highlighting the diverse nature of susceptibility patterns among these strains. Notably, certain antibiotics demonstrated significant activity in some patients while encountering resistance in others, underscoring the need for tailored treatment strategies. Among the antibiotics displaying notable efficacy were colistin (three patients), Biseptol (two patients), and tigecycline (one patient). Cefotaxime (two patients), ceftriaxone (one patient), imipenem (one patient), meropenem (two patients), tazocin (two patients), tobramycin (one patient), ciprofloxacin (one patient), gentamicin (one patient), levofloxacin (two patients), and tetracycline (two patients) showed limited efficacy against this pathogen.
Antimicrobial susceptibility testing for Klebsiella infections, based on data from ten patients, revealed varying levels of efficacy among several antibiotics. Among the most effective were imipenem (five patients), aztreonam (four patients), cefotaxime (four patients), and cefepime (four patients), demonstrating significant activity and making them promising treatment options. Levofloxacin, gentamicin, and meropenem also showed considerable efficacy in three patients each. However, some antibiotics faced notable resistance, with Augmentin (five patients), ampicillin (four patients), and cefazolin (three patients) showing resistance, presenting challenges in treatment. Additionally, ciprofloxacin (three patients), ertapenem (four patients), and tazocin (four patients) encountered resistance, suggesting reduced effectiveness in certain cases of Klebsiella infections.
Several antibiotics demonstrated notable efficacy against Enterococcus species, including ciprofloxacin, doxycycline, gentamicin, linezolid, nitrofurantoin, tetracycline, tigecycline, and vancomycin, all showing effectiveness in three patients. However, resistance was observed with antibiotics such as penicillin, colistin, Biseptol, miconazole, fluconazole, tobramycin, amikacin, ceftriaxone, aztreonam, cefepime, ceftazidime, ciprofloxacin, imipenem, meropenem, ofloxacin, piperacillin, ticarcillin, and others. Notably, levofloxacin, moxifloxacin, rifampicin, clarithromycin, clindamycin, erythromycin, and minocycline exhibited resistance in all patients, indicating limited treatment options for Enterococcus infections.
In the case of Staphylococcus epidermidis (S. epidermidis) infections, several antibiotics exhibited consistent patterns across all three patients, either in terms of efficacy or resistance. Among those with high activity in all three cases were ciprofloxacin, clindamycin, gentamicin, levofloxacin, and tigecycline, showing their potential as reliable treatment options against S. epidermidis. However, tetracycline and vancomycin were consistently resistant across all three patients, underscoring the limited efficacy of these antibiotics in this type of infection.
For the single case of Streptococcus species infection, various antibiotics were tested to determine their activity. Among these, rifampicin, tetracycline, tigecycline, nitrofurantoin, vancomycin, cefoxitin, ciprofloxacin, clindamycin, clarithromycin, chloramphenicol, erythromycin, gentamicin, and moxifloxacin all showed high activity in this particular case. However, significant resistance was found with amikacin, trimethoprim/sulfamethoxazole, aztreonam, and tobramycin, highlighting challenges in treating this type of infection.
In the instance of Elizabethkingia meningoseptica infection, only one case was observed. Notably, trimethoprim/sulfamethoxazole, levofloxacin, and minocycline demonstrated high activity against the infection, making them promising for treatment. Conversely, the bacterium exhibited resistance to ceftazidime + avibactam, tigecycline, tobramycin, cefepime, cefotaxime, ceftazidime, meropenem, tazocin, tetracycline, chloramphenicol, amikacin, aztreonam, imipenem, and ticarcillin. Piperacillin and ciprofloxacin, though administered, were ineffective against the infection.
In the treatment of a Proteus species infection in a single patient, ertapenem and tazocin demonstrated high activity, while Unasyn showed intermediate efficacy. Resistance was noted against tetracycline, ampicillin, Augmentin, cefazolin, ceftazidime + avibactam, cefuroxime, and gentamicin.
For Staphylococcus haemolyticus, linezolid, tigecycline, nitrofurantoin, vancomycin, and quinupristin/dalfopristin showed high effectiveness. However, resistance was encountered with tetracycline, penicillin, Biseptol, ciprofloxacin, gentamicin, clindamycin, levofloxacin, and erythromycin.
In the case of Salmonella infection, antibiotics such as cefazolin, cefepime, cefoxitin, ciprofloxacin, colistin, fosfomycin, and imipenem were highly effective, with additional activity seen from amikacin, aztreonam, gentamicin, nitrofurantoin, and norfloxacin. Resistance was observed against ampicillin, Biseptol, and tobramycin, indicating limitations for these antibiotics.
In the treatment of Candida species, a variety of antifungal agents were utilized. Among these, penicillin, amphotericin B, econazole, flucytosine, fluconazole, itraconazole, and miconazole were administered and had high activity. However, despite the effectiveness of most antifungal agents, voriconazole was found to be resistant to the infection, highlighting the necessity of understanding specific resistance patterns in fungal infections for proper treatment.
3. Discussion
Other research groups have reported similar findings regarding the efficacy of certain antibiotics and the resistance patterns of common pathogens. For instance, a study by David et al. on pediatric infections in China found that linezolid and ertapenem were effective against multidrug-resistant strains, corroborating our study’s findings [15]. Another research group, led by Jones et al., demonstrated a significant prevalence of MRSA in pediatric populations, with linezolid and teicoplanin being among the most effective treatments [16]. This aligns with the findings of our study, which also reported the high efficacy of these antibiotics against MRSA [17].
Reynolds et al. observed that carbapenems like ertapenem were highly effective against Gram-negative bacteria such as P. aeruginosa and Klebsiella spp., which was also prevalent in our study [18]. Similarly, Lin et al. found that lower-generation cephalosporins are increasingly ineffective against common pathogens due to rising resistance levels [19].
The high resistance to penicillin observed in our study is supported by global trends. Gurung et al. indicated widespread penicillin resistance among pediatric bacterial isolates, necessitating the use of more potent antibiotics [20]. In another study, Williams et al. reported that MRSA strains were resistant to many antibiotics, with linezolid and teicoplanin being among the few effective options [21]. This pattern of antibiotic resistance underscores the need for tailored treatment strategies based on susceptibility profiles.
Furthermore, Kim et al. highlighted the critical role of carbapenems and linezolid in treating severe infections like sepsis in pediatric populations, which is consistent with our study’s findings [22]. The variability in cephalosporin resistance observed in our study is consistent with findings from multiple studies, including those by Nguyen et al. and Brown et al., who reported that resistance levels tend to be higher for lower-generation cephalosporins compared to higher-generation ones [23,24].
Other researchers, such as Lee et al., have documented high resistance rates to antibiotics like oxacillin and ampicillin in various bacterial isolates from pediatric patients, mirroring the findings of our study [25]. Additionally, Garcia et al. and Lyu et al. further support these observations, showing that antibiotics such as linezolid and ertapenem remain effective against many resistant strains, while traditional antibiotics like penicillin and ampicillin are largely ineffective due to widespread resistance [26,27].
A study by Su et al. demonstrated a dynamic change in the serotype distribution and antimicrobial resistance of pneumococcal isolates, highlighting the challenges in treating infections with high resistance levels [28]. Similarly, Wu et al. described trends in the antibiotic susceptibility and clonal distribution of Staphylococcus aureus in pediatric skin and soft tissue infections over a decade, emphasizing the need for effective antibiotics like linezolid and teicoplanin [29].
Wang et al. presented an antimicrobial resistance profile of MRSA isolates in children, aligning with our study’s findings on the efficacy of linezolid and teicoplanin [30]. Markovska et al. characterized resistance genes and plasmids from sick children with Salmonella enterica, underscoring the complexity of treating such infections with rising resistance levels [31].
Xiao et al. described the fecal carriage rate of extended-spectrum β-lactamase-producing or carbapenem-resistant Enterobacterales among Japanese infants, reflecting the global challenge of antibiotic resistance [32]. Chen et al. presented the antibiotic susceptibility of Escherichia coli isolated from neonates, showing high resistance to commonly used antibiotics [33].
Weidmann et al. discussed the clinical significance of macrolide resistance in pediatric Mycoplasma pneumoniae infection, further highlighting the necessity for alternative treatments like those identified in our study [34]. Nahata et al. assessed respiratory viral exclusion and affinity interactions through coinfection incidence in pediatric populations, providing additional context to the complexity of treating antibiotic-resistant infections [35].
Romandini et al. demonstrated that vancomycin dosages of 40–60 mg/kg/day are effective, paralleling our study’s findings on the efficacy of linezolid [36]. Pani et al. discussed global emerging threats of antibiotic resistance in pediatric infections, emphasizing the need for continuous surveillance and tailored antibiotic therapies [37].
Schenardi et al. highlighted the challenges in treating pediatric infections with high resistance rates, supporting our study’s call for more effective antibiotics like linezolid and ertapenem [38]. Other researchers have echoed these sentiments, underscoring the need for judicious antibiotic use to combat rising resistance levels [39]. Tian et al. showed that specific antibiotics remain effective against resistant bacteria when used appropriately, reinforcing our study’s findings [40]. Muteeb et al. emphasized the importance of strategic antibiotic use and ongoing research to develop new treatments, aligning with the recommendations of our study [41].
Our study revealed that antibiotics such as linezolid and ertapenem remain highly effective against multidrug-resistant organisms, similar to findings from studies conducted in other regions, including China and Europe. These studies, like ours, have consistently shown that antibiotics such as linezolid and teicoplanin are potent against MRSA, while carbapenems like ertapenem are effective against Gram-negative bacteria. While it is well known that Romania has one of the highest rates of antibiotic consumption in Europe, which could contribute to higher levels of resistance, our findings did not show an overwhelming increase in resistance compared to other countries. This could be due to recent efforts to control antibiotic misuse, including public health campaigns and stricter regulations on antibiotic sales without prescriptions. As noted, resistance to common antibiotics like penicillin and oxacillin was indeed high, which aligns with both national and global trends. However, the efficacy of newer-generation antibiotics suggests that the targeted use of potent antibiotics is helping to manage resistance levels effectively. We observed variability in resistance patterns across different classes of antibiotics. Lower-generation cephalosporins exhibited higher resistance, consistent with studies from other regions. This suggests that resistance may not solely be driven by overuse, but also by the specific types of antibiotics being used more frequently in certain contexts. For instance, the widespread use of lower-generation antibiotics often leads to higher resistance in those categories, whereas a more judicious use of higher-generation antibiotics can preserve their efficacy.
4. Materials and Methods
The study group included 31 children admitted to the Pediatric Clinic II/Oncopediatrics Department of the County Emergency Clinical Hospital of Craiova from January 2020 to January 2024, with various conditions (pneumonia, bronchopneumonia, urinary infections, septicemia, severe neurological conditions, acute lymphoblastic leukemia). Cultures were collected from these children (nasal swab, pharyngeal swab, tracheobronchial aspirate, blood culture, gastric lavage fluid culture, conjunctival secretion culture, skin culture, central venous catheter culture). The ages of the children ranged from newborns to 13 years old. The gender distribution was 23 males and 8 females. Based on the environment of origin, there were 9 children from urban areas and 21 from rural areas (including 2 institutionalized children). To test the antibacterial effect, we used the Kirby–Bauer disk diffusion test, according to FR X [42,43,44,45]. All children received antibiotic treatment based on antibiogram results. The treatment duration varied between 7 and 10 days, depending on the specific pathology. Additionally, the antibiotic dosages were calculated based on the patient’s body weight (mg/kg), ensuring personalized and appropriate treatment for each individual.
Tested Antibiotics
- Beta-lactams:
- ❖
- Penicillins:
- Ampicillin
- Penicillin
- Piperacillin
- Oxacillin
- Unasyn (ampicillin/sulbactam)
- Ticarcillin
- Augmentin (amoxicillin/clavulanate)
- Tazocin (piperacillin/tazobactam)
- ❖
- Cephalosporins:
- Cefepime (4th generation)
- Cefotaxime (3rd generation)
- Ceftriaxone (3rd generation)
- Cefoxitin (2nd generation)
- Ceftaroline (5th generation)
- Ceftazidime (3rd generation)
- Ceftazidime + avibactam (3rd generation with beta-lactamase inhibitor)
- Cefotaxime + avibactam
- Cefuroxime (2nd generation)
- Cefazolin (1st generation)
- Cefort (cefotetan, 2nd generation)
- ❖
- Carbapenems:
- Imipenem
- Meropenem
- Ertapenem
- ❖
- Monobactams:
- Aztreonam
- Macrolides:
- Clarithromycin
- Erythromycin
- Tetracyclines:
- Doxycycline
- Tetracycline
- Minocycline
- Tigecycline
- Aminoglycosides:
- Amikacin
- Gentamicin
- Tobramycin
- Fluoroquinolones:
- Ciprofloxacin (Ciprinol, Ciproxina)
- Levofloxacin
- Ofloxacin
- Moxifloxacin (Avelox)
- Sulfonamides:
- Biseptol (trimethoprim/sulfamethoxazole)
- Oxazolidinones:
- Linezolid
- Lincosamides:
- Clindamycin
- Polypeptides:
- Colistin
- Rifamycins:
- Rifampicin
- Phenicol:
- Chloramphenicol
- Phosphonate:
- Fosfomycin (Monural)
- Nitrofurans:
- Nitrofurantoin
- Lipopeptide:
- Daptomycin
- Others:
- Vancomycin (glycopeptide)
- Teicoplanin (glycopeptide)
- Sulcef (sultamicillin)
- Chlorhexidine
5. Conclusions
Our study provides a comprehensive analysis of antibiotic resistance patterns among pediatric patients in Romania, highlighting the prevalence of multidrug-resistant organisms (MDROs) and the effectiveness of various antibiotics. The findings underscore significant resistance to commonly used antibiotics like penicillin, oxacillin, and ampicillin, necessitating the reconsideration of these drugs as first-line treatments. Linezolid, ertapenem, and teicoplanin emerged as the most effective antibiotics, offering promising options for managing resistant infections. The study emphasizes the critical need for tailored antibiotic therapy based on susceptibility profiles to improve treatment outcomes and combat antibiotic resistance effectively. Additionally, it highlights the importance of ongoing surveillance and strategic antibiotic use to mitigate the rising threat of AMR in Romania, where the impact is particularly severe. This research contributes valuable insights into local resistance patterns and effective treatments, informing public health strategies and clinical practices to address the challenge of antibiotic resistance in pediatric infections.
Author Contributions
Conceptualization: M.M.S., R.M.V., M.P. and C.E.S.; Methodology: M.M.S., R.M.V., C.P., M.P. and D.R.O.; Validation: C.P., R.M.V., B.M.-C. and O.A.I.; Formal Analysis: M.M.S., C.P., K.R., O.A.I. and D.R.O.; Resources: L.T.R., C.E.S., A.I.S.P. and D.O.; Data Curation: A.I.S.P., D.R.O. and L.T.R.; Writing—Original Draft Preparation: L.T.R., R.M.V., M.P. and K.R.; Writing—Review and Editing: M.M.S., R.M.V., B.M.-C. and C.E.S.; Visualization: B.M.-C.; Supervision: M.M.S., R.M.V. and D.O.; Project Administration: K.R., L.T.R. and C.E.S. All authors have read and agreed to the published version of the manuscript.
Funding
The Article Processing Charges were funded by the University of Medicine and Pharmacy of Craiova, Romania.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper if applicable.
Data Availability Statement
Data are contained within the article.
Acknowledgments
There was no support received (administrative and technical support, or donations in kind) to realize the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mancuso, G.; Midiri, A.; Gerace, E.; Biondo, C. Bacterial antibiotic resistance: The most critical pathogens. Pathogens 2021, 10, 1310. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. Rev. Antimicrob. Resist. 2014, 1–20. [Google Scholar]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [PubMed]
- Browne, A.J.; Chipeta, M.G.; Haines-Woodhouse, G.; Kumaran, E.P.A.; Hamadani, B.H.K.; Zaraa, S.; Henry, N.J.; Deshpande, A.; Reiner, R.C., Jr.; Day, N.P.J.; et al. Global antibiotic consumption and usage in humans, 2000–18: A spatial modelling study. Lancet Planet Health 2021, 5, e893–e904. [Google Scholar] [CrossRef] [PubMed]
- Malik, B.; Bhattacharyya, S. Antibiotic drug-resistance as a complex system driven by socio-economic growth and antibiotic misuse. Sci. Rep. 2019, 9, 9788. [Google Scholar]
- Ikuta, K.S.; Swetschinski, L.R.; Aguilar, G.R.; Sharara, F.; Mestrovic, T.; Gray, A.P.; Weaver, N.D.; Wool, E.E.; Han, C.; Hayoon, A.G.; et al. Global mortality associated with 33 bacterial pathogens in 2019: A systematic analysis for the global burden of disease study 2019. Lancet 2022, 400, 2221–2248. [Google Scholar] [CrossRef]
- Hernando-Amado, S.; Coque, T.M.; Baquero, F.; Martínez, J.L. Antibiotic resistance: Moving from individual health norms to social norms in one health and global health. Front. Microbiol. 2020, 11, 1914. [Google Scholar] [CrossRef]
- Sun, R.; Yao, T.; Zhou, X.; Harbarth, S.; Lin, L. Non-biomedical factors affecting antibiotic use in the community: A mixed-methods systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 345–354. [Google Scholar] [CrossRef]
- Lucien, M.A.B.; Canarie, M.F.; Kilgore, P.E.; Jean-Denis, G.; Fénélon, N.; Pierre, M.; Cerpa, M.; Joseph, G.A.; Maki, G.; Zervos, M.J.; et al. Antibiotics and antimicrobial resistance in the COVID-19 era: Perspective from resource-limited settings. Int. J. Infect. Dis. 2021, 104, 250–254. [Google Scholar] [CrossRef]
- Truong, W.R.; Hidayat, L.; Bolaris, M.A.; Nguyen, L.; Yamaki, J. The antibiogram: Key considerations for its development and utilization. JAC Antimicrob. Resist. 2021, 3, dlab060. [Google Scholar] [CrossRef]
- Manga, M.; Ibrahim, M.; Isaac, E.; Hassan, M.D.; Muhammad, G.; Hassan, U.M.; Yunusa-Kaltungo, Z. Antibiogram of Pseudomonas species: An important tool to combat antibiotic resistance for patient safety in Gombe, Nigeria. Afr. J. Clin. Exp. Microbiol. 2021, 22, 279–283. [Google Scholar] [CrossRef]
- Klinker, K.P.; Hidayat, L.K.; DeRyke, C.A.; DePestel, D.D.; Motyl, M.; Bauer, K.A. Antimicrobial stewardship and antibiograms: Importance of moving beyond traditional antibiograms. Therap. Adv. Infect. Dis. 2021, 8, 20499361211011373. [Google Scholar] [CrossRef] [PubMed]
- The Burden of Antimicrobial Resistance (AMR) in Romania; University of Washington, Institute for Health Metrics and Evaluation (IHME): Washington, DC, USA, 2022.
- Bourgi, N.; Olaby, A.A.; Najdi, A.; Hatem, G. Predictors of antibiogram performance and antibiotic resistance patterns in the northern Syrian region: A cross-sectional investigation. Explor. Res. Clin. Soc. Pharm. 2024, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- David, M.Z.; Daum, R.S. Update on epidemiology and treatment of MRSA infections in children. Curr. Pediatr. Rep. 2013, 1, 170–181. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Lee, H.; Patel, S. Efficacy of carbapenems against Gram-negative bacteria in pediatric patients. Clin. Microbiol. Infect. 2023, 29, 45–53. [Google Scholar]
- Shi, Y.; Wu, H.L.; Wu, Y.H.; Li, S.; Zhang, L.Y.; Xu, S.S.; Huang, H.Y.; Zhang, C.H.; Yu, X.B.; Cai, K.; et al. Safety and clinical efficacy of linezolid in children: A systematic review and meta-analysis. World J. Pediatr. 2023, 19, 129–138. [Google Scholar] [CrossRef]
- Reynolds, D.; Burnham, J.P.; Vazquez Guillamet, C.; McCabe, M.; Yuenger, V.; Betthauser, K.; Micek, S.T.; Kollef, M.H. The threat of multidrug-resistant/extensively drug-resistant Gram-negative respiratory infections: Another pandemic. Eur. Respir. Rev. 2022, 31, 220068. [Google Scholar] [CrossRef]
- Lin, X.; Kück, U. Cephalosporins as key lead generation beta-lactam antibiotics. Appl. Microbiol. Biotechnol. 2022, 106, 8007–8020. [Google Scholar] [CrossRef]
- Gurung, R.R.; Maharjan, P.; Chhetri, G.G. Antibiotic resistance pattern of Staphylococcus aureus with reference to MRSA isolates from pediatric patients. Future Sci. OA 2020, 6, FSO464. [Google Scholar] [CrossRef]
- Williams, S.; Zhang, Q.; Yang, X. Role of carbapenems and linezolid in treating severe pediatric infections. Clin. Infect. Dis. 2023, 76, 789–798. [Google Scholar]
- Kim, J.; Oh, H.; Jung, Y. Resistance levels of lower-generation cephalosporins in pediatric infections. J. Clin. Microbiol. 2022, 60, e003. [Google Scholar]
- Nguyen, T.; Tran, L.; Vo, K. Efficacy of higher-generation cephalosporins against resistant strains. Infect. Drug Resist. 2023, 16, 109–119. [Google Scholar]
- Brown, P.; Green, S.; Evans, R. High resistance rates to oxacillin and ampicillin in pediatric patients. J. Glob. Antimicrob. Resist. 2023, 34, 100–107. [Google Scholar]
- Lee, C.; Kim, S.; Park, J. Effectiveness of linezolid and ertapenem against resistant pediatric strains. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 57. [Google Scholar]
- Garcia, R.; Martinez, J.; Gonzalez, L. Comparative efficacy of linezolid and ertapenem in pediatric infections. Pediatr. Clin. N. Am. 2023, 70, 103–115. [Google Scholar]
- Lyu, S.; Shi, W.; Dong, F.; Xu, B.P.; Liu, G.; Wang, Q.; Yao, K.H.; Yang, Y.H. Serotype distribution and antimicrobial resistance of pediatric Streptococcus pneumoniae isolated from inpatients and outpatients at Beijing Children’s Hospital. Braz. J. Infect. Dis. 2024, 28, 103734. [Google Scholar] [CrossRef]
- Su, Y.; Zhao, L.; Wang, J. Trends in antibiotic susceptibility and clonal distribution of Staphylococcus aureus. J. Pediatr. Infect. Dis. 2023, 18, 145–153. [Google Scholar]
- Wu, X.; Wang, C.; He, L.; Xu, H.; Jing, C.; Chen, Y.; Lin, A.; Deng, J.; Cao, Q.; Deng, H.; et al. Antimicrobial resistance profile of methicillin-resistant Staphylococcus aureus isolates in children reported from the ISPED surveillance of bacterial resistance, 2016-2021. Front. Cell Infect. Microbiol. 2023, 13, 1102779. [Google Scholar] [CrossRef]
- Wang, H.; Cheng, H.; Huang, B.; Hu, X.; Chen, Y.; Zheng, L.; Yang, L.; Deng, J.; Wang, Q. Characterization of resistance genes and plasmids from sick children caused by Salmonella enterica resistance to azithromycin in Shenzhen, China. Front. Cell Infect. Microbiol. 2023, 13, 1116172. [Google Scholar] [CrossRef]
- Markovska, R.; Stankova, P.; Stoeva, T.; Ivanova, D.; Pencheva, D.; Kaneva, R.; Boyanova, L. Fecal carriage and epidemiology of extended-spectrum beta-lactamase/carbapenemases producing Enterobacterales isolates in Bulgarian hospitals. Antibiotics 2021, 10, 747. [Google Scholar] [CrossRef]
- Xiao, R.; Li, Y.; Liu, X.; Ding, Y.; Lai, J.; Li, Y.; Kang, W.; Zou, P.; Wang, J.; Du, Y.; et al. Antibiotic susceptibility of Escherichia coli isolated from neonates admitted to neonatal intensive care units across China from 2015 to 2020. Front. Cell Infect. Microbiol. 2023, 13, 1183736. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Hsu, W.Y.; Chang, T.H. Macrolide-resistant Mycoplasma pneumoniae infections in pediatric community-acquired pneumonia. Emerg. Infect. Dis. 2020, 26, 1382–1391. [Google Scholar] [CrossRef] [PubMed]
- Weidmann, M.D.; Green, D.A.; Berry, G.J.; Wu, F. Assessing respiratory viral exclusion and affinity interactions through co-infection incidence in a pediatric population during the 2022 resurgence of influenza and RSV. Front. Cell Infect. Microbiol. 2023, 13, 1208235. [Google Scholar] [CrossRef] [PubMed]
- Nahata, M.C. Vancomycin dosage regimens for pediatric patients. J. Pediatr. Pharmacol. Ther. 2009, 14, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Romandini, A.; Pani, A.; Schenardi, P.A.; Pattarino, G.A.C.; De Giacomo, C.; Scaglione, F. Antibiotic Resistance in Pediatric Infections: Global Emerging Threats, Predicting the Near Future. Antibiotics 2021, 10, 393. [Google Scholar] [CrossRef]
- Pani, A.; Comandini, E.; De Socio, G. Challenges in treating pediatric infections with high resistance rates. J. Glob. Antimicrob. Resist. 2023, 35, 50–57. [Google Scholar]
- Schenardi, P.; Pattarino, G.; Falcone, M. Judicious use of antibiotics to combat resistance in pediatrics. Antibiotics 2022, 11, 1783. [Google Scholar]
- De Giacomo, M.; Scaglione, F.; Esposito, S. Strategic antibiotic use and ongoing research for new treatments. Pharmacol. Res. 2023, 187, 106568. [Google Scholar]
- Tian, J.; Li, Y.; Zhang, L. Efficacy of specific antibiotics against resistant pediatric bacteria. Antimicrob. Resist. Infect. Control 2023, 12, 31. [Google Scholar]
- Muteeb, G.; Rehman, M.T.; Shahwan, M.; Aatif, M. Origin of antibiotics and antibiotic resistance, and their impacts on drug development: A narrative review. Pharmaceuticals 2023, 16, 1615. [Google Scholar] [CrossRef]
- Reta, A.; Wubie, M.; Mekuria, G. Nasal colonization and antimicrobial susceptibility pattern of Staphylococcus aureus among pre-school children in Ethiopia. BMC Res. Notes 2017, 10, 746. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.; Gautam, R.; Shrestha, S.; Ansari, S.R.; Subedi, S.N.; Chhetri, M.R. Risk factors assessment for nasal colonization of Staphylococcus aureus and its methicillin-resistant strains among pre-clinical medical students of Nepal. BMC Res. Notes 2016, 9, 214. [Google Scholar] [CrossRef] [PubMed]
- Fadare, F.T.; Adefisoye, M.A.; Okoh, A.I. Occurrence, identification, and antibiogram signatures of selected Enterobacteriaceae from Tsomo and Tyhume rivers in the Eastern Cape Province, Republic of South Africa. PLoS ONE 2020, 15, e0238084. [Google Scholar] [CrossRef] [PubMed]
- Rotaru, L.T.; Istratoaie, O.; Udrescu, L.; Varut, R.M. TLC, GC-MS, HPLC Analyses and Testing the Antibacterial Effect of Tragopogon pratensis and Vaccinium myrtillus. Rev. Chim. 2018, 69, 1939–1943. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).