Abstract
Advanced diagnostic technologies have made accurate and precise diagnosis of pathogens easy. Herein, we present a new diagnostic method, droplet digital PCR (ddPCR), to detect and quantify Acinetobacter baumannii in mini bronchoalveolar lavage (mini-BAL) samples. A. baumannii causes ventilator-associated pneumonia (VAP), a severe healthcare infection affecting patients’ lungs. VAP carries a high risk of morbidity and mortality, making its timely diagnosis crucial for prompt and effective management. Methodology. The assay performance was evaluated by comparing colonization data, quantitative culture results, and different generations of PCR (traditional PCR and Real-Time PCR—qPCR Taqman® and SYBR® Green). The ddPCR and qPCR Taqman® prove to be more sensitive than other molecular techniques. Reasonable analytical specificity was obtained with ddPCR, qPCR TaqMan®, and conventional PCR. However, qPCR SYBR® Green technology presented a low specificity, making the results questionable in clinical samples. DdPCR detected/quantified A. baumanni in more clinical samples than other methods (38.64% of the total samples). This emerging ddPCR technology offers promising advantages such as detection by more patients and direct quantification of pathogens without calibration curves.
1. Introduction
Nosocomial infections represent a major clinical challenge for diagnostic microbiology and significantly threaten public health safety. Acinetobacter baumannii is one of the highly reported pathogens associated with nosocomial infections, including ventilator-associated pneumonia (VAP), having an adaptive capacity to acquire and maintain multiple genetic elements encoding antimicrobial resistance determinants [1,2]. VAP mainly affects mechanically ventilated patients in intensive care units (ICUs). VAP develops at least 48 h after an endotracheal intubation or tracheostomy and is caused by pathogens not present or incubating during mechanical ventilation. VAP is characterized by progressive infiltrate signs of systemic infection, including elevated body temperature, altered blood cell count, and changes in sputum characteristics [3]. Recent reports of VAP infection show that the infection incidence ranges from 15% to 50% [4,5]. Thus, accurate and rapid identification of A. baumannii is critical for appropriate infection control in ICUs [6].
The conventional polymerase chain reaction (PCR) is commonly used for the detection of A. baumannii; however, it has some limitations, such as the requirement of an electrophoretic run on an agarose gel, absence of quantitative determination, and the use of harmful reagents such as ethidium bromide [7]. Real-time PCR (qPCR), also known as 2nd generation PCR, was developed in 1992 as an enhancement of conventional PCR and represents a significant advance in biotechnology for diagnosing infectious diseases [8]. However, its precision can be affected by amplification efficiency variations and inhibitor presence. Thus, the journey of PCR reached droplet digital PCR (ddPCR), one of the latest PCR techniques. ddPCR showed good efficiency in the detection of A. baumannii and K. pneumoniae in blood samples within 4 h, with a specificity of 100% [9]. Additionally, ddPCR has also proven to be efficient for diagnosing and quantifying Pneumocystis jerovecii in bronchoalveolar lavage fluid samples [10]. Clinically important pathogens, including Mycobacterium tuberculosis [11] and Staphylococcus aureus [12], are also successfully detected by ddPCR. The other potential applications of ddPCR are the identification of antimicrobial resistance genes in bacteria, confirmation of detection of SARS-CoV-2, expression levels of genes associated with the immunological synapse, and measurement of miRNA levels related to inflammation and aging [13].
ddPCR enables the precise detection and absolute quantification of nucleic acids, eliminating the requirement for a calibration curve [14]. The key to ddPCR’s enhanced performance lies in its ability to partition a sample into thousands to millions of separate reactions on microfluidic chips or within micro-droplets. These partitions are made at such a scale that each contains either a single or no copy of the target DNA or RNA molecule [9]. After PCR amplification, analyzing the proportion of partitions that yield a positive signal against the total number of partitions allows for directly calculating the absolute target nucleic acid quantity in the original sample. This calculation uses binomial Poisson statistics, enabling precise measurement of target copy numbers [15]. ddPCR showed promising results in the detection of A. baumannii [9]; therefore, we attempted to extend its diagnostic breadth towards the detection of VAP-associated A. baumannii, which is a life-threatening infection the timely diagnosis of which may reduce the mortality and morbidity rate.
This study aimed to develop a new ddPCR to detect and quantify A. baumannii in bronchoalveolar lavage samples from patients with VAP. In addition, we evaluated the performance of this assay by comparing quantitative culture results with those of different generations of PCR (traditional PCR, SYBR®, and Taqman®).
2. Results
2.1. Microbiological Analysis
A total of 44 microorganisms were isolated from mini-BAL samples. A. baumannii was the most prevalent, isolated from eight clinical specimens (18.2%) in quantitative culture. The second most recovered microorganism of the cases evaluated in this study was S. aureus (15.9%), followed by Pseudomonas aeruginosa (13.6%). All isolates of A. baumannii were resistant to all antimicrobials tested, except Polymyxin B. The mortality rate among the included patients was 20 (45.5%).
2.2. Analytical Sensitivity
The limit of detection for conventional PCR was 1.02 ng/µL (reference sample) or 2.00 ng/µL (clinical sample) (dilution 103). For SYBR®Green, the detection limit was 0.010 ng/µL or 20 pg (reference sample) or 0.020 ng/µL or 40 pg (clinical sample) (dilution 105). The limit of detection for TaqMan® qPCR and ddPCR was 0.0010 ng/µL or 2 pg (reference sample) or 0.0020 ng/µL or 4 pg (clinical sample) (dilution 106). Only the sigmoid curves were considered positive. We considered cutting off the 37 quantification cycle (Cq) for SYBR®Green and 35 for Taqman®. Table 1 shows the Cq of the reference A. baumannii ATCC 19606 and clinical sample dilutions close to the detection limit of both real-time PCR, values of absolute quantification by ddPCR, and its respective coefficient of variation (CV). Figure 1 presents the analytical sensitivity of ddPCR represented by serial dilution of A. baumannii ATCC 19606 type strain.

Table 1.
Amplification results of molecular assays by quantification cycle or absolute quantification belonging to the dilutions close to the limit of detection.
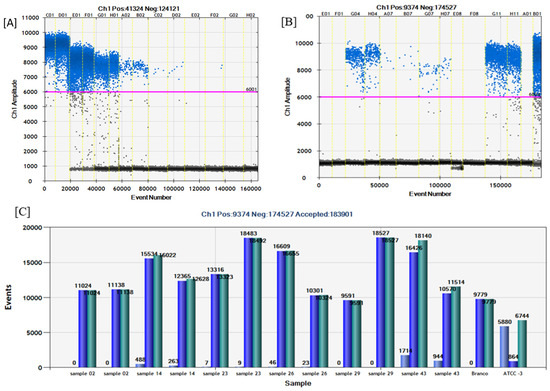
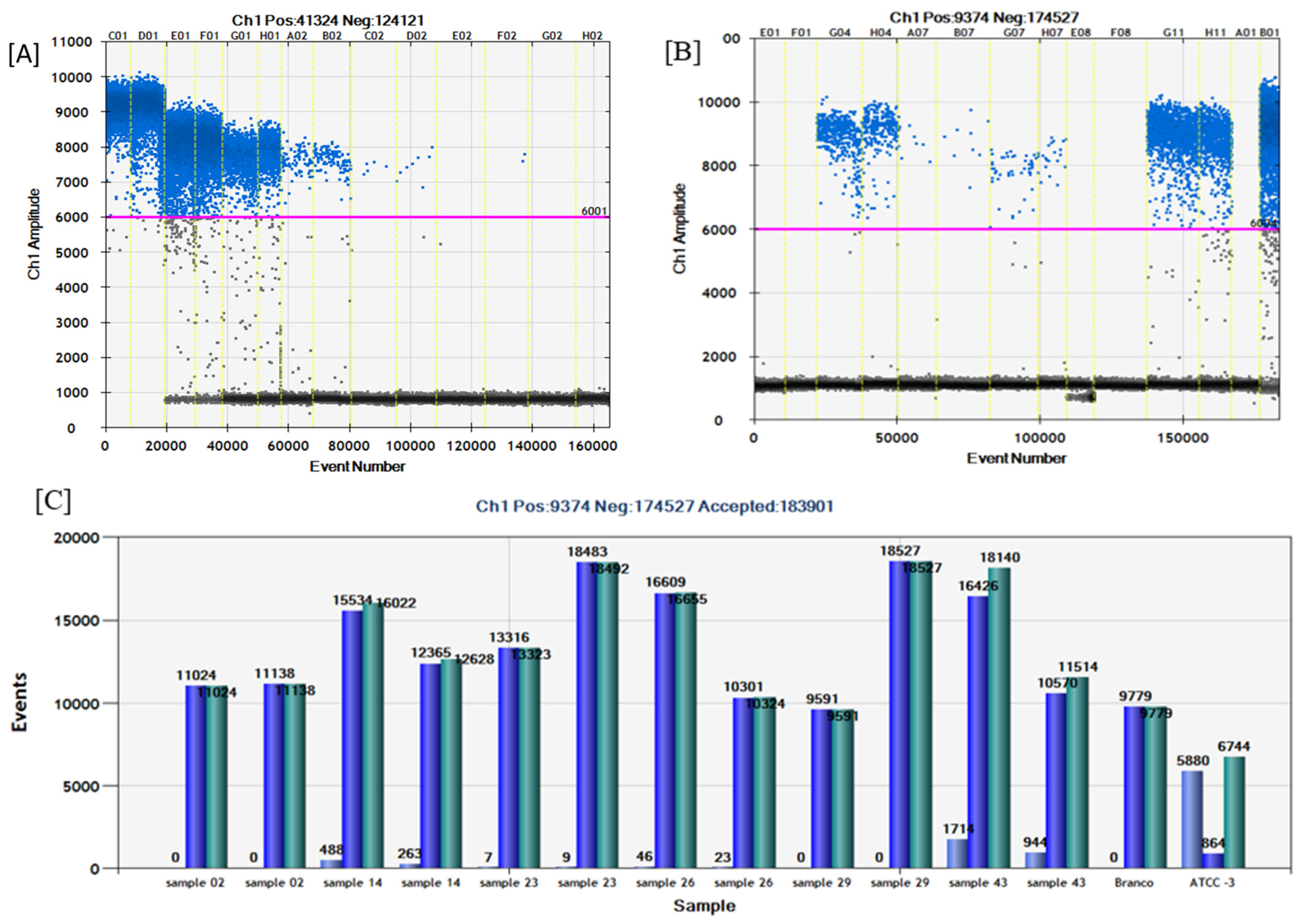
Figure 1.
(A) Analytical sensitivity of ddPCR using serial dilutions of A. baumanni ATCC 19606 (reference sample). C01–D01: 102. E01–F01: 103. G01–H01: 104. A02–B02: 105. C02–D02: 106. E02–F02: 107. G02–H02: 108. The blue droplets are considered positive, and the dark droplets are negative. Pink line: fluorescence amplitude cut-off. (B) ddPCR in clinical samples. A Fluorescence amplitude versus event number (total droplets). E01–F01: sample 02. G04–H04: sample 14. A07–B07: sample 23. G07–H07: sample 26. E08–F08: sample 29. G11–H11: sample 43. A01: no template control (NTC). B01: positive control A. baumanni ATCC 19606. The blue droplets are considered positive, and the dark droplets are negative. The pink line is the fluorescence amplitude cut-off (around 6000). (C) Number of total droplets (green), positive droplets (light blue), and negative droplets (dark blue) per sample.
2.3. Analytical Specificity
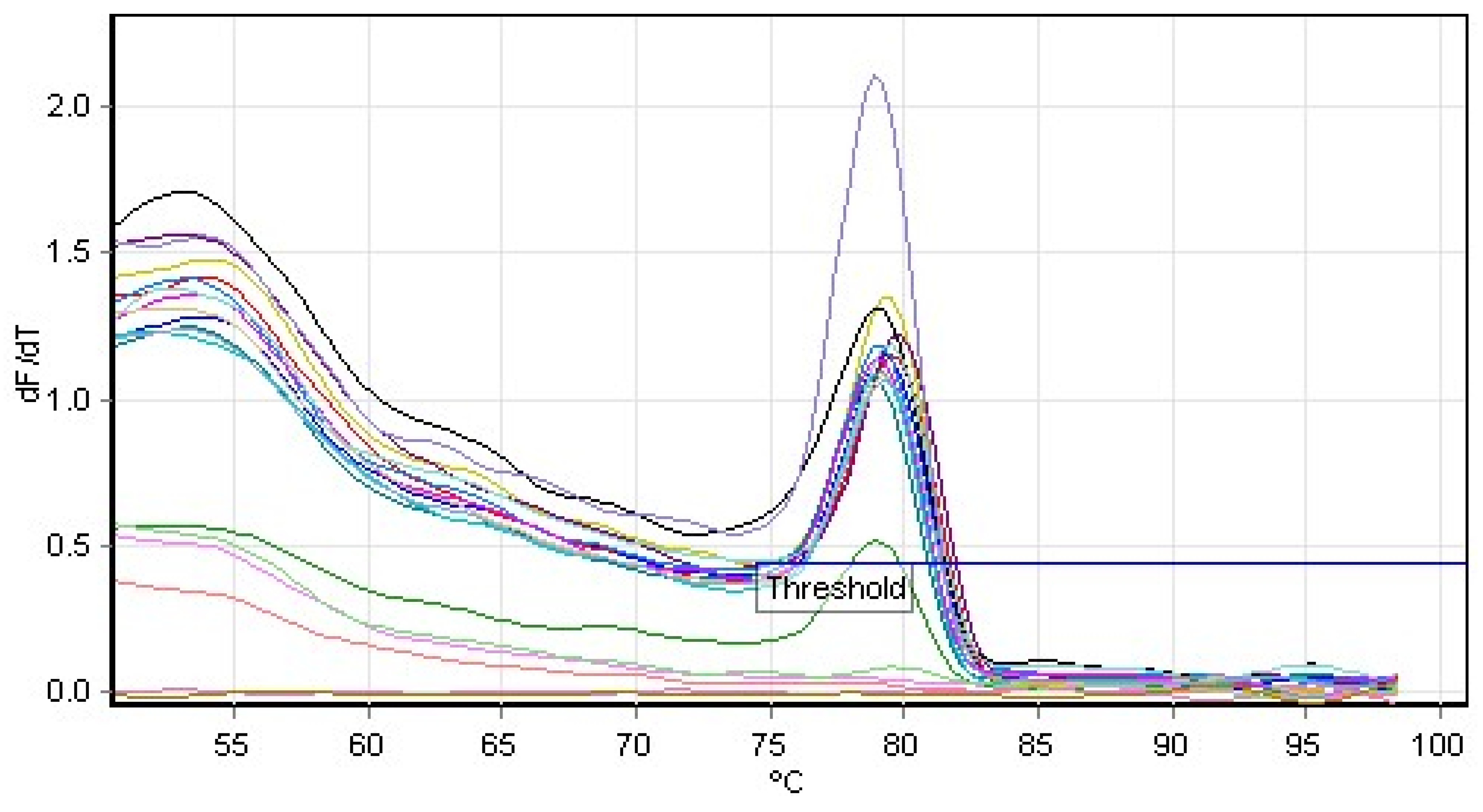
Conventional PCR demonstrated 100% specificity against the panel of bacteria tested; only A. baumannii was amplified, and no non-specific amplification was visualized against the tested target blaOXA-51. With respect to the SYBR® Green methodology, we verified the non-specific amplification of six bacteria (S. aureus ATCC 25923, Klebsiella pneumoniae ATCC 27799, Escherichia coli ATCC 25922, Staphylococcus epidermidis ATCC 29213, Pseudomonas aeruginosa ATCC 27853, and Klebsiella oxytoca 700324), through the existence o melting temperatures close to that of the positive control (A. baumannii ATCC 19606) used (Figure 2).
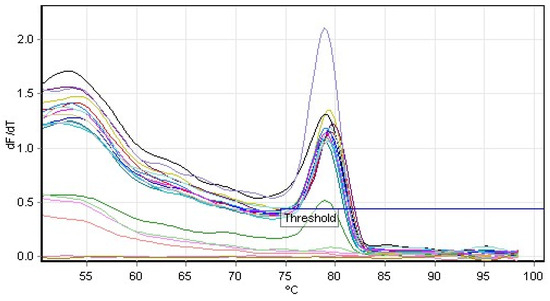
Figure 2.
Melting curve analysis of real-time PCR (SYBR)’s analytical specificity. The values of positive control peaks (fluorescence over time higher than 2) and some bacteria (S. aureus ATCC 25923, K. pneumoniae ATCC 27799, E. coli ATCC 25922, S. epidermidis 2ATCC 29213, P. aeruginosa ATCC 27853, and K. oxytoca 700324) were similar (around 79 °C).
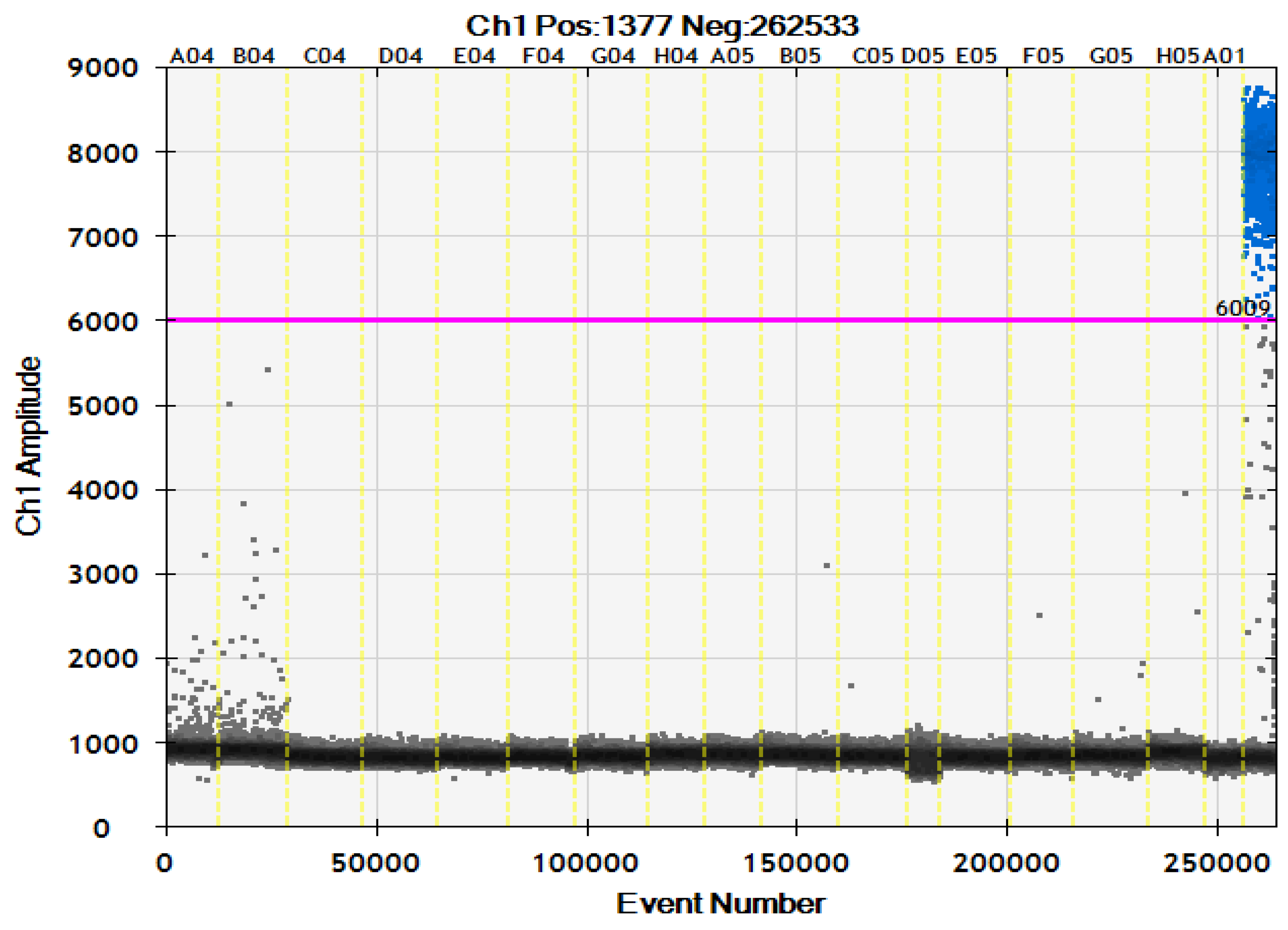
There was reasonable specificity of TaqMan® against the target tested; non-specific amplification was not detected, except for S. aureus ATCC 25923 with C.T. values of 22.77 and 22.27 (duplicates). The same results were found in the ddPCR specificity; no significant counting drops were observed about the positive control (A. baumannii ATCC 19606). S. aureus ATCC 25923 showed some droplets in ddPCR (fluorescence amplitude below 6000); however, the amplitude was lower than the positive control. In this sense, we used the fluorescence amplitude 6000 as a cut-off to distinguish between positive and negative droplets (Figure 3).
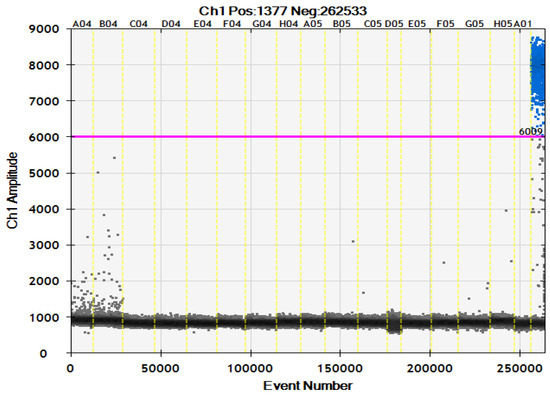
Figure 3.
Analytical specificity of ddPCR using the panel of bacteria A04–B04: S. aureus, C04–D04: P. aeruginosa, E04–F04: K. pneumoniae, G04–H04: E. coli, A05–B05: E. faecalis, C05–D05: K. oxytoca, E05–F05: E. faecium, G05–H05: S. epidermidis. A01: no template control (NTC). Last column: positive control A. baumanni ATCC 19606. The blue droplets are considered positive, and the dark droplets are negative. Pink line: fluorescence amplitude cut-off.
2.4. Comparison of Conventional PCR, Real-Time PCR (SYBR® Green and TaqMan®), and ddPCR on Detection of A. baumannii in Clinical Samples
Conventional PCR detected A. baumannii in 8 of 44 samples (18.18%) with a correlation of 69.44% (0.95 Confidence Interval, error 0.1183) between the traditional technique of PCR and quantitative culture). The SYBR®Green technique did not discriminate between negative and positive quantitative culture results and amplified all 44 samples with Cq 10.08 up to 34.19. Taqman® amplified 11 of 44 (25%) (correlation of 66.67% between Taqman PCR assay and quantitative culture with 0.95 confidence interval, error 0.1125). This assay showed Cq values higher than 35 in 24 samples; however, the amplification curves were not sigmoid. ddPCR showed 17 positive samples (38.64% of the total samples) with a correlation of 41.55% about the golden standard (0.95 confidence interval, error 0.1096).
Of the eight samples detected in the quantitative culture, Taqman® and ddPCR detected seven, and the conventional PCR detected six. One sample was detected in a quantitative culture but not in any molecular method (sample 5). Table 2 shows the molecular assays and quantitative culture evaluation results in clinical samples. Table 3 presents the quantity of detected and undetected samples by conventional PCR, Taqman, and ddPCR compared with quantitative culture.
Table 2.
Results of microbiological analysis and molecular assays (conventional PCR, SYBR®Green, TaqMan®, and ddPCR) in 44 mini-BAL samples.
Table 3.
Number of samples detected and undetected in conventional PCR, Taqman®, and ddPCR relative to quantitative culture.
In terms of a comparison of the ddPCR results versus conventional PCR and Taqman® in clinical samples, the ddPCR showed more positive results, and the correlation was better with Taqman® (69.23%, error 0.0921, 0.95 confidence interval) than conventional PCR (52.17%, error 0.1036 with 0.95 confidence interval) (Table 4).
Table 4.
Number of samples detected and undetected in ddPCR relative to conventional PCR and Taqman®.
3. Discussion
The criteria for diagnosing VAP are controversial, with various methodologies described in the literature for epidemiological surveillance and diagnosis [16,17]. Therefore, it is crucial to have consistent criteria and local data to accurately identify and manage VAP and its etiology.
Lower respiratory tract specimens (e.g., BAL, mini-BAL) are preferred for microbiological diagnosis of VAP, and detecting microorganisms in this sample can result in an effective and more accurate antimicrobial therapy [18]. In our study, the pathogen most frequently isolated in mini-BAL samples from 44 patients with VAP was A. baumannii, followed by S. aureus and P. aeruginosa. Similar results are reported in many studies that identify A. baumannii as a primary pathogen in VAP patients [19,20,21]. All isolates of A. baumannii exhibited resistance to the tested antimicrobials, except for Polymyxin B, indicating a high level of drug resistance consistent with previous reports [2,22]. This high drug resistance is associated with the presence of the carbapenemase gene blaOXA-51, which is responsible for the multi-drug resistance capacity of A. baumannii [23,24].
It is important to highlight that to evaluate colistin susceptibility, we chose the VITEK II system, even though broth microdilution is considered the gold standard as recommended by the joint CLSI-EUCAST Polymyxin Breakpoints Working Group. This decision was driven by the need for an efficient and rapid system capable of handling a large volume of samples in a practical and reliable manner, as our study was conducted primarily in a hospital routine laboratory. Recent studies have shown that VITEK II exhibits excellent categorical agreement with broth microdilution for most tested pathogens, including A. baumannii [25].
Currently, detection methods of A. baumannii include phenotypic characterization, which previously needed isolation, growth in culture medium, and incubation time [26]. In this context, rapid methods that can make the diagnosis quickly appear as alternatives in the scenario of ICUs. Molecular approaches to detect bacterial DNA in VAP have been used successfully, and recent studies use qPCR to diagnose VAP etiologic agents [27,28,29]. However, most studies explore other etiologic agents like S. aureus [28,30] and S. pneumoniae [31]. Moreover, ddPCR has yet to be studied and used for this purpose. This is the first study that used ddPCR to detect bacterial DNA in BAL from patients with VAP.
The analytical sensitivity of ddPCR showed a higher limit of detection (LOD) when compared with the two other PCR techniques (Conventional PCR and S.Y.B.R. qPCR). However, the analytical sensitivity of ddPCR was similar to the TaqMan qPCR; this similarity between ddPCR and TaqMan qPCR was also reported by Pinheiro de Oliveira et al. in the detection of the foot-and-mouth disease virus [32]. Our results indicated that ddPCR and TaqMan® possess high analytical sensitivity, capable of detecting very small amounts of DNA in mini-BAL and reference samples, with concentrations as low as 1 pg/µL and 2 pg/µL, respectively. ddPCR showed reasonable specificity for all the tested bacteria except S. aureus ATCC 25923, which demonstrated fluorescence amplitude below 6000. This result was essential to better determine the cut-off of the ddPCR.
We detected a low analytical specificity for SYBR® Green; this is a DNA intercalating agent, and the detection is monitored by fluorescence intensity over the cycles. It was suggested that this may be a significant drawback of the method since the dye is not specifically dye-bound to the double strand of target DNA [33], which may explain the non-specificity of the results. In the original work on these primers, Gadsby et al. [34] also used a probe in which a specificity step detected a positive signal only for A. baumanni DNA and did not detect amplification in any of the tested isolates found in the respiratory tract or commensals. The TaqMan system uses probes, which increase the sensitivity and specificity of the reaction; however, to obtain a quantitative result, the standard curve and the use of a reference gene for quantitative analysis by qPCR are essential to obtain reliable results [33,35,36,37].
Among the 44 mini-BAL samples from patients with VAP, ddPCR amplified 17 samples (38.64%), making it a more effective method for detecting positive samples compared to other molecular methods (conventional PCR and TaqMan) and culture techniques. ddPCR detected seven out of eight samples identified by culture, yielding a concordance rate of 41.55% with the quantitative culture results, because it detected bacteria in more samples. Notably, sample 5, which was identified by culture, was not detected by any of the PCR methods.
These results highlight the potential of ddPCR to replace traditional bacterial culture methods, providing a faster and equally reliable alternative for diagnosing VAP. ddPCR can rapidly and reliably confirm the involvement of A. baumannii in VAP, significantly reducing the diagnostic time by eliminating the need for bacterial culture growth. This expedited process allows for earlier intervention and more targeted treatment, potentially improving patient outcomes and reducing the duration of antibiotic therapy.
4. Materials and Methods
4.1. Criteria for Diagnosis of VAP
Ventilator-associated pneumonia (VAP) is diagnosed in patients with a pulmonary infection who have been on mechanical ventilation for at least 48 h. The diagnosis is confirmed when there is a new infiltrate or progression of a previously existing infiltrate on chest X-ray, in association with at least one of the following criteria:
- A mini-BAL culture showing a count of ≥104 CFU/mL;
- An axillary temperature of ≥38.3 °C;
- Total leukocytes of ≥109/L;
- Aspiration of purulent sputum through the orotracheal tube (OT) or tracheostomy; worsening of gas exchange, such as a PaO2/FiO2 ratio of less than 300;
- Increased need for supplemental oxygen or heightened ventilatory demand.
4.2. Sample Collection and Microbiological Analysis
Between January 2023 and December 2023, samples of mini-BAL were collected from 44 patients (23 men and 21 women, mean age 61 ± 19 years) with pneumonia associated with mechanical ventilation (VAP), admitted to an Intensive Care Center at Hospital das Clínicas/UFMG. The main comorbidities presented by these patients were arterial hypertension (22.72%), neoplasias (18.2%), and renal and hepatic insufficiency (11.4%). Before the sampling, the project was approved by the Teaching, Research, and Extension Directorate—DEPE—of Hospital das Clinicas and the Ethics and Research Committee.
Each mini-BAL sample obtained was homogenized and divided into five aliquots of approximately 2 ml using Eppendorf tubes. Direct microscopic analysis was performed using a smear, stained with Gram staining technique. The same aliquot was used for primary sowing in Tryptone Soya Agar (TSA-OXOID®) culture media for isolation of all pathogens and MacConkey (OXOID®) for isolation of Gram-negative rods. Using a 1 µL calibrated loop and after homogenization, the samples were cultured and incubated at 37 °C. The plates were evaluated for bacterial growth for 18–24 h; if there was growth, the number of colonies observed per mL on each plate was counted. The count was adjusted accordingly, given that the most widely accepted cut-off value in the literature is 104 CFU/mL.
- <10 colonies per plate <104 CFU/mL and, presumably, colonization.
- ≥10 colonies per plate ≥104 CFU/mL and should be interpreted as infectious disease.
Gram staining was performed for all colonies in order to confirm the purity of the isolated bacteria. To identify the isolated bacteria(s) grown, the VITEK® II system (BioMérieux®, Marcy-l'Étoil, France) was used employing cards (GN for Gram-negative and GP for Gram-positive) according to the manufacturer’s instructions. After identification by VITEK® II, three batches of inocula were preserved in cryotubes containing 1 mL of Brucella Broth (OXOID®, Basingstoke, UK) plus 10% sterile Glycerol and stored in a −80 °C freezer.
Antimicrobial susceptibility testing was performed by an automated microdilution VITEK® II (BioMérieux®) according to the recommendations of the Clinical and Laboratory Standards Institute [38]. Antimicrobials tested for A. baumannii were gentamicin (CN), ceftazidime (CAZ), Cefepime (FEP), ceftriaxone (CRO), imipenem (IPM), meropenem (MEM), Ampicillin/sulbactam (SAM), Piperacillin/Tazobactam (TZP), Ciprofloxacin (CIP), Colistin (COL), Tigecycline (TIG), Ampicillin (AMP), Cefuroxime (CRX), Cefuroxime Axetil (CRX), and Cefoxitin (CFO). Susceptibility to Polymyxin B (PB) was tested using the Etest ® (AB Biodisk, Solna, Sweden).
4.3. Nucleic Acid Extraction
DNA from the 44 mini-BAL was extracted using the QIAamp® DNA. Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s guidelines. The extracted DNA was kept in a freezer at −80 °C. The presence and integrity of the extracted DNA were assessed by electrophoresis on an agarose gel. The reference bacterial DNA was extracted according to Moreira [39]. Each sample was tested in triplicate to evaluate the analytical specificity of the molecular assay. All the extracted DNA was quantified in Nanodrop (Thermo, Waltham, MA, USA) using the purity ratios.
4.4. Conventional PCR Assay
The DNA extracted was amplified by standard PCR using a Mastercycler Nexus Gradient thermal cycler (Eppendorf®, Hamburg, Germany) and OXA-51-like β-lactamase (blaOXA-51-like) species-specific primers (Forward 5′-TAA TGC TTT GAT CGG CTT TG-3′ and Reverse 5′-TGG ATT GCA CTT CAT CTT GG-3′ [40]) that generate a fragment with 353 bp. The 25 μL reaction consisted of 12.5 μL 2× Master Mix (PROMEGA, Madison, WI, USA), 1 μL of primer forward (10 μM), 1 μL of primer reverse (10 μM), 2 μL of DNA (50 ng/μL), and 8.5 μL of ABD-type water. The PCR conditions were performed as follows: 1 cycle of 94 °C for 3 min; 35 cycles of 94 °C for 45 s, 60 °C for 40 s, and 72 °C for 50 s; and one cycle of 72 °C for 5 min. The amplified products were electrophoresed on a 1% agarose gel, stained with gelRed (Sigma, St. Louis, MO, USA), and visualized under UV light.
4.5. SYBR® Green qPCR Assay
qPCR was performed using Rotorgene Q (Qiagen) to amplify the blaOXA-51-like gene. Primers were designed to generate a 134 bp fragment, with the sequences Forward 5′-TTTAGCTCGTCGTATTGGACT-3′ and Reverse 5′-CCTCTTGCTGAGGAGTAATTTT-3′, as described by [34]. High-purity DNA was extracted using a Qiagen DNA extraction kit, and the concentration was determined using a NanoDrop spectrophotometer. The reaction mixture, with a total volume of 20 μL, included 12.5 μL of 2× SYBR® Green PCR Master Mix, 1 μL each of forward and reverse primers (both at 10 μM concentration), 1 μL of DNA template at a concentration of 20 ng/μL, and 4.5 μL of nuclease-free distilled water. Optimal annealing temperature was determined through gradient PCR. The standardized PCR protocol started with a 10 min denaturation step at 95 °C, followed by 40 cycles of 15 s at 95 °C for denaturation and 60 s at 60 °C for annealing and extension. Controls included no template controls (NTC) to check for contamination, positive controls to verify reaction functionality, and a standard curve generated using serial dilutions of a known concentration of the target gene to determine efficiency and quantify unknown samples. Each reaction was run in triplicate for accuracy. Data acquisition was performed using qPCR analysis software. The threshold was set in the exponential phase of amplification, and baseline correction was applied to remove background fluorescence. Efficiency was calculated from the standard curve, aiming for an efficiency range of 90–110% (slope of −3.1 to −3.6).
After the 40 cycles, a melting curve analysis was conducted by gradually increasing the temperature from 60 °C to 95 °C, with fluorescence measurements taken every 0.3 °C increment to assess amplification specificity. A single peak in the melting curve confirmed the specificity of the qPCR amplification for the blaOXA-51-like gene.
4.6. TaqMan® Real-Time PCR Assay (qPCR)
The oligonucleotides for TaqMan® qPCR targeting the blaOXA-51-like gene (89 bp) were designed using the Primer3 Plus program [41]. The amplification was performed using the CFX96 Touch Real-time PCR Detection System (Bio-Rad Laboratories, Hercules, CA, USA). The reaction mixture, with a total volume of 20 μL, consisted of 10 μL of QuantiTect® Probe Master Mix (Qiagen), 1 μL of probe (10 pmol) with the sequence 5′/56-FAM-CCTTGAGCA/ZEN/CCATAAGGCAACCAC/3IABKFQ-3′, 0.75 μL of forward primer (10 pmol) with the sequence 5′ CCTGCTTCGACCTTCAAAATG-3′, 0.75 μL of reverse primer (10 pmol) with the sequence 5′-TGCCCGTCCCACTTAAATAC-3′, 1 μL of MgCl2 (25 mM), 4.5 μL of nuclease-free water, and 2 μL of DNA template. The thermal cycling conditions were optimized as follows: initial denaturation at 95 °C for 10 min, followed by 45 cycles of 95 °C for 30 s and 60 °C for 60 s.
4.7. Droplet Digital PCR (ddPCR) Assay
The same oligonucleotides used in TaqMan® Real-time PCR were used in ddPCR. The genetic material extracted was quantified using the QX200™ Droplet Digital™ PCR System (Bio-Rad Laboratories) while following the manufacturers’ instructions. Briefly, the reaction was carried out using 10 μL ddPCR Supermix for probes, 0.6 μL probe (10 pmol), 2.16 μL of each forward and reverse primer (10 pmol), 7.08 μL of H2O and the 2 μL of DNA. After, 20 μL of the PCR reaction was placed into an 8-channel disposable droplet generation cartridge and 70 μL of droplet generation oil was added per well. Approximately 20,000 droplets were generated at each well by the QX200 droplet generator). After processing, the prepared droplet emulsion (40 μL) was further transferred to a skirted 96-well PCR plate (Eppendorf). The plate was heat-sealed with pierceable foil using the PX1™ PCR plate sealer (Bio-Rad). PCR amplification was carried out using a Px2 Thermal Cycler (Thermo Electron Corporation, Waltham, MA, USA). The reactions were first optimized in terms of the primer-annealing step (in the temperature range between 54 and 60 °C). The amplification conditions were as follows: 95 °C for 10 min; 40 cycles of 94 °C for 30 s and 58 °C for 60 s; and 1 cycle of 95 °C for 10 min. After amplification, the PCR plate was read by the QX200 droplet reader (Bio-Rad Laboratories) and analyzed by Quanta Soft droplet reader software, version 1.6.6.0320.
4.8. Analytical Sensitivity
To compare the sensitivity and accuracy among the three PCR generations, the DNA of 10 × 104 CFU/mL of A. baumannii ATCC 19606 type strain (1099 ng/μL) was extracted according to Moreira [13] and diluted by a factor of around 10 (101 to 1015). The detection limit was also defined using serial dilution of a clinical sample (10 × 104 CFU/mL–2002 ng/μL). Dilutions close to the limit were repeated in triplicate (real-time) or duplicate (ddPCR), and we considered the analytical sensitivity as the last dilution amplified or quantified in all replicates by the methods.
4.9. Analytical Specificity
To verify the analytical specificity of the three generations of PCR, a panel of eight reference bacteria that are commonly isolated species in quantitative culture in bronchoalveolar lavage samples from patients with ventilator-associated pneumonia was used: S. aureus ATCC 25923, K. pneumoniae ATCC 27799, Klebsiella oxytoca ATCC 700324, Enterococcus faecalis ATCC 29212, E. coli ATCC 25922, Enterobacter cloacae ATCC 700323, S. epidermidis ATCC 29213, and P. aeruginosa ATCC 27853. The four molecular methods were used in 44 mini-BAL DNA samples. The amplification or quantification (ddPCR) results were also compared with the results for A. baumannii in quantitative culture as the “golden standard”, in addition to the colonization data of the patients with A. baumannii at the time of collection.
4.10. Statistical Analysis
All statistical analyses were performed with the software package SPSS. version 19.0 (IBM, Armonk, NY, USA). Linear regression analysis of the calibration curves from real-time PCR was conducted using two different software platforms: Rotorgene Q Series Software version 2.1.0 for SYBR. green assays and Bio-Rad CFX Manager version 3.1 for Taqman assays. The values of the quantification cycle (Cq) obtained in analytical sensitivity were evaluated in triplicate (SYBR. and Taqman) or duplicate (ddPCR) for each test considering the coefficient of variation (CV). For ddPCR, the absolute concentration of each sample was automatically reported by QuantaSoft version 1.6.6.0320 software by calculating the ratio of the positive droplets over the total droplets combined with Poisson distribution. The error reported for a single well was the Poisson 95% confidence interval. The kappa statistic with quadratic weighting [42], available at http://vassarstats.net/kappa.html (accessed on 15 March 2024), was used to establish the correlation between the ddPCR and other molecular assay results with quantitative culture in clinical samples.
5. Conclusions
DdPCR and qPCR Taqman® showed better analytical sensitivity toward VAP associated with A. baumanni. However, ddPCR was more efficient than the other techniques in clinical samples, so it can be considered a promising molecular tool for VAP diagnosis to detect and estimate the bacterial load, mainly when absolute quantification is required. This work made a new tool available for the diagnosis of A. baumanni. Herein, we present ddPCR as an important diagnostic method for the detection of VAP-associated A. baumannii, having several exceptional features such as precision, high sensitivity and specificity, absolute quantification and quantification in a complex mixture, less vulnerability to inhibitors, and no requirement for post-amplification processing.
Author Contributions
Conceptualization, M.G.M. and A.G.G.O.; methodology, M.G.M., A.G.G.O., I.U.H., T.F.P.d.O. and V.A.N.J.; validation, M.G.M. and V.A.N.J.; formal analysis, T.F.P.d.O. and W.B.A.; investigation, I.U.H. and S.G.d.S.; resources, W.B.A.; data curation, A.G.G.O.; writing—original draft preparation, M.G.M.; writing—review and editing, I.U.H., T.F.P.d.O., A.A.F.J., V.A.N.J. and S.G.d.S.; visualization, A.A.F.J.; supervision, S.G.d.S.; project administration, S.G.d.S.; funding acquisition, W.B.A. All authors have read and agreed to the published version of the manuscript.
Funding
King Saud University, Saudi Arabia project number (RSP2024R332).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained within the article.
Acknowledgments
This work was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG), the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lee, C.R.; Lee, J.H.; Park, M.; Park, K.S.; Bae, I.L.K.; Kim, Y.B.; Cha, C.-J.; Jeong, B.C.; Lee, S.H. Biology of Acinetobacter baumannii: Pathogenesis, Antibiotic Resistance Mechanisms, and Prospective Treatment Options. Front. Cell. Infect. Microbiol. 2017, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Ciginskienė, A.; Dambrauskienė, A.; Rello, J.; Adukauskienė, D. Ventilator-Associated Pneumonia due to Drug-Resistant Acinetobacter baumannii: Risk Factors and Mortality Relation with Resistance Profiles, and Independent Predictors of In-Hospital Mortality. Medicina 2019, 55, 49. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, J.; Kinoshita, T.; Yamakawa, K.; Matsushima, A.; Nakamoto, N.; Hamasaki, T.F.S. Impact of Gram stain results on initial treatment selection in patients with ventilator-associated pneumonia: A retrospective analysis of two treatment algorithms. Crit. Care 2017, 21, 156. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, D.; Singh, D.; Loomba, P.; Kaur, A.; Tandon, M.; Bishnoi, I. Assessment of surgical risk factors in the development of ventilator-associated pneumonia in neurosurgical intensive care unit patients: Alarming observations. Neurol. India 2017, 65, 779–784. [Google Scholar] [CrossRef]
- Philippart, F.; Gaudry, S.; Quinquis, L.; Lau, N.; Ouanes, I.; Touati, S.; Nguyen, J.C.; Branger, C.; Faibis, F.; Mastouri, M.; et al. Randomized intubation with polyurethane or conical cuffs to prevent pneumonia in ventilated patients. Am. J. Respir. Crit. Care Med. 2015, 191, 637–645. [Google Scholar] [CrossRef]
- Haas, D.J.; Torres, D.A.C. Aplicações das técnicas de PCR no diagnóstico de doenças infecciosas dos animais. Rev. Científica Med. Veterinária 2016, 16, 26. [Google Scholar]
- Anbazhagan, D.; Mui, W.S.; Mansor, M.; Yan, G.O.S.; Yusof, M.Y.; Sekaran, S.D. Development of conventional and real-time multiplex PCR assays for the detection of nosocomial pathogens. Braz. J. Microbiol. 2011, 42, 448–458. [Google Scholar] [CrossRef]
- Zheng, Y.; Jin, J.; Shao, Z.; Liu, J.; Zhang, R.; Sun, R.; Hu, B. Development and clinical validation of a droplet digital PCR assay for detecting Acinetobacter baumannii and Klebsiella pneumoniae in patients with suspected bloodstream infections. Microbiology 2021, 10, e1247. [Google Scholar] [CrossRef]
- Jitmuang, A.; Nititammaluk, A.; Boonsong, T.; Sarasombath, P.T.; Sompradeekul, S.; Chayakulkeeree, M. A novel droplet digital polymerase chain reaction for diagnosis of Pneumocystis pneumonia (PCP)-a clinical performance study and survey of sulfamethoxazole-trimethoprim resistant mutations. J. Infect. 2021, 83, 701–708. [Google Scholar] [CrossRef]
- Yamamoto, M.; Ushio, R.; Watanabe, H.; Tachibana, T.; Tanaka, M.; Yokose, T.; Kaneko, T. Detection of Mycobacterium tuberculosis-derived DNA in circulating cell-free DNA from a patient with disseminated infection using digital PCR. Int. J. Infect. Dis. 2018, 66, 80–82. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, I.; Cajander, S.; Rasmussen, G.; Ennefors, T.; Mölling, P.; Strålin, K. High nuc DNA load in whole blood is associated with sepsis, mortality and immune dysregulation in Staphylococcus aureus bacteraemia. Infect. Dis. 2019, 51, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Merino, I.; de la Fuente, A.; Domínguez-Gil, M.; Eiros, J.M.; Tedim, A.P.; Bermejo-Martín, J.F. Digital PCR applications for the diagnosis and management of infection in critical care medicine. Crit. Care. Mar. 2022, 26, 63. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Farkas, K.; Hassard, F.; McDonald, J.E.; Malham, S.K.; Jones, D.L. Evaluation of Molecular Methods for the Detection and Quantification of Pathogen-Derived Nucleic Acids in Sediment. Front. Microbiol. 2017, 8, 53. [Google Scholar] [CrossRef]
- Ou, Y.; Cao, S.; Zhang, J.; Dong, W.; Yang, Z.; Yu, Z. Droplet microfluidics on analysis of pathogenic microbes for wastewater-based epidemiology. Trends Analyt. Chem. 2021, 143, 116333. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koenig, S.M.; Truwit, J.D. Ventilator-Associated Pneumonia: Diagnosis, Treatment, and Prevention. Clin. Microbiol. Rev. 2006, 19, 637–657. [Google Scholar] [CrossRef]
- Papazian, L.; Klompas, M.; Luyt, C. Ventilator-associated pneumonia in adults: A narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef]
- Berton, D.C.; Kalil, A.C.; Teixeira, P.J. Quantitative versus qualitative cultures of respiratory secretions for clinical outcomes in patients with ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2014, 10, CD006482. [Google Scholar] [CrossRef]
- Wałaszek, M.; Różańska, A.; Wałaszek, M.Z.; Wójkowska-Mach, J. Epidemiology of Ventilator-Associated Pneumonia, microbiological diagnostics and the length of antimicrobial treatment in the Polish Intensive Care Units in the years 2013–2015. BMC Infect. Dis. 2018, 18, 308. [Google Scholar] [CrossRef]
- Rose, D.D.; Pezzotti, P.; Fortunato, E.; Sordillo, P.; Gini, S.; Boros, S.; Meledandri, M.; Gallo, M.T.; Prignano, G.; Caccese, R.; et al. Clinical predictors and microbiology of ventilator-associated pneumonia in the intensive care unit: A retrospective analysis in six Italian hospitals. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1531–1539. [Google Scholar] [CrossRef]
- Sandiumenge, A.; Rello, J. Ventilator-associated pneumonia caused by E.S.K.A.P.E. organisms. Curr. Opin. Pulm. Med. 2012, 18, 187–193. [Google Scholar] [CrossRef]
- Denys, G.A.; Relich, R.F. Antibiotic resistance in nosocomial respiratory infections. Clin. Lab. Med. 2014, 34, 257–270. [Google Scholar] [CrossRef]
- Vázquez-López, R.; Solano-Gálvez, S.G.; Vignon-Whaley, J.J.J.; Vaamonde, J.A.A.; Alonzo, L.A.P.; Reséndiz, A.R.; Álvarez, M.M.; López, E.N.V.; Franyuti-Kelly, G.; Álvarez-Hernández, D.A.; et al. Acinetobacter baumannii Resistance: A Real Challenge for Clinicians. Antibiotics 2020, 9, 205. [Google Scholar] [CrossRef] [PubMed]
- Turton, J.F.; Woodford, N.; Glover, J.; Yarde, S.; Kaufmann, M.E.; Pitt, T.L. Identification of Acinetobacter baumannii by Detection of the blaOXA-51-like Carbapenemase Gene Intrinsic to This Species. J. Clin. Microbiol. 2006, 44, 2974–2976. [Google Scholar] [CrossRef] [PubMed]
- Wattal, C.; Goel, N.; Oberoi, J.K.; Datta, S.; Raveendran, R. Performance of three commercial assays for colistin susceptibility in clinical isolates and Mcr-1 carrying reference strain. Indian J. Med. Microbiol. 2019, 37, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, S.; Biswas, I.; Veeraraghavan, B. Accurate identification of clinically important Acinetobacter spp.: An update. Future Sci. 2019, 5, FSO395. [Google Scholar] [CrossRef] [PubMed]
- Schulte, B.; Eickmeyer, H.; Heininger, A.; Juretzek, S.; Karrasch, M.; Denis, O.; Roisin, S.; Pletz, M.W.; Klein, M.; Barth, S.; et al. Detection of pneumonia-associated pathogens using a prototype multiplexed pneumonia test in hospitalized patients with severe pneumonia. PLoS ONE 2014, 9, e110566. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Clavel, M.; Barraud, O.; Moucadel, V.; Meynier, F.; Karam, E.; Ploy, M.-C.; François, B. Molecular quantification of bacteria from respiratory samples in patients with suspected ventilator-associated pneumonia. Clin. Microbiol. Infect. 2016, 22, 812.e1–812.e7. [Google Scholar] [CrossRef]
- Mansour, M.G.E.; Albendary, S. Multiplex polymerase chain reaction: Could change diagnosis of Ventilator-associated pneumonia in pediatric critical care units to the fast track? Egypt. J. Med. Hum. Genet. 2018, 19, 135–139. [Google Scholar] [CrossRef]
- Kwon, S.J.; Jeon, T.; Seo, D.; Na, M.; Choi, E.G.; Son, J.W.; Yoo, E.H.; Park, C.G.; Lee, H.Y.; Kim, J.O.; et al. Quantitative PCR for Etiologic Diagnosis of Methicillin-Resistant Staphylococcus aureus Pneumonia in Intensive Care Unit. Tuberc. Respir. Dis. 2012, 72, 293–301. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sharifi, A.; Kavoosi, F.; Hosseini, S.M.J.; Mosavat, A.; Ahmadi, A. Prevalence of Streptococcus pneumoniae in Ventilator-Associated Pneumonia by Real-time PCR. Arch. Clin. Infect. Dis. 2019, 14, e86416. [Google Scholar] [CrossRef]
- Pinheiro-de-Oliveira, T.F.; Fonseca, A.A., Jr.; Camargos, M.F.; Laguardia-Nascimento, M.; de Oliveira, A.M.; Cottorello, A.C.P.; Goes-Neto, A.; Barbosa-Stancioli, E.F. Development of a droplet digital RT-PCR for the quantification of foot-and-mouth virus R.N.A. J. Virol. Methods 2018, 259, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Shieh, K.-J.; Chen, G.; Qiao, X.T.; Chuang, M.-Y. Application of Real-time Polymerase Chain Reaction (RT-PCR). J. Am. Sci. 2006, 2, 1–15. [Google Scholar]
- Gadsby, N.J.; McHugh, M.P.; Russell, C.D.; Mark, H.; Conway Morris, A.; Laurenson, I.F.; Hill, A.T.; Templeton, K.E. Development of two real-time multiplex PCR assays for the detection and quantification of eight key bacterial pathogens in lower respiratory tract infections. Clin. Microbiol. Infect. 2015, 21, 788.e1–788.e13. [Google Scholar] [CrossRef] [PubMed]
- Pfaffl, M.W. Quantification Strategies in Real-Time PCR; International University Line: La Jolla, CA, USA, 2004; Chapter 3; pp. 87–112. [Google Scholar]
- Wong, M.L.; Medrano, J.F. Real-time PCR for mRNA quantitation. BioTechniques 2005, 38, 75–85. [Google Scholar] [CrossRef]
- Bustin, S.A.; Benes, V.; Garson, G.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Disk and Dilution Susceptibility Tests for Bacteria Isolated from Animals; Second Informational Supplement. CLSI Document VET01-S2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2014; Volume 33, 70p. [Google Scholar]
- Moreira, M.G.; Camargo, C.H.; Vasconcellos, F.M.; Barreto, L.M.; Nobre, V.; Santos, S.G. Diversity of blaOXA-51 variants and its clonal complexes in multidrug-resistant Acinetobacter baumannii strains in patients with ventilator-associated pneumonia. J. Glob. Antimicrob. Resist. 2017, 9, 94–95. [Google Scholar] [CrossRef]
- Woodford, N.; Ellington, M.J.; Coelho, J.M.; Turton, J.F.; Ward, M.E.; Brown, S.; Amyes, S.G.; Livermore, D.M. Multiplex PCR for genes encoding prevalent O.X.A. carbapenemases in Acinetobacter spp. Int. J. Antimicrob. Agents 2006, 27, 351–353. [Google Scholar] [CrossRef]
- Untergasser, A.; Nijveen, H.; Rao, X.; Bisseling, T.; Geurts, R.; Leunissen, J.A.M. Primer3Plus, an enhanced web interface to Primer3. Nucleic Acids Res. 2007, 35, 71–74. [Google Scholar] [CrossRef]
- Cohen, J. Weighted kappa: Nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 1968, 70, 213–220. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).