
Predicting Extended-Spectrum Beta-Lactamase and Carbapenem Resistance in Enterobacteriaceae Bacteremia: A Diagnostic Model Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Results
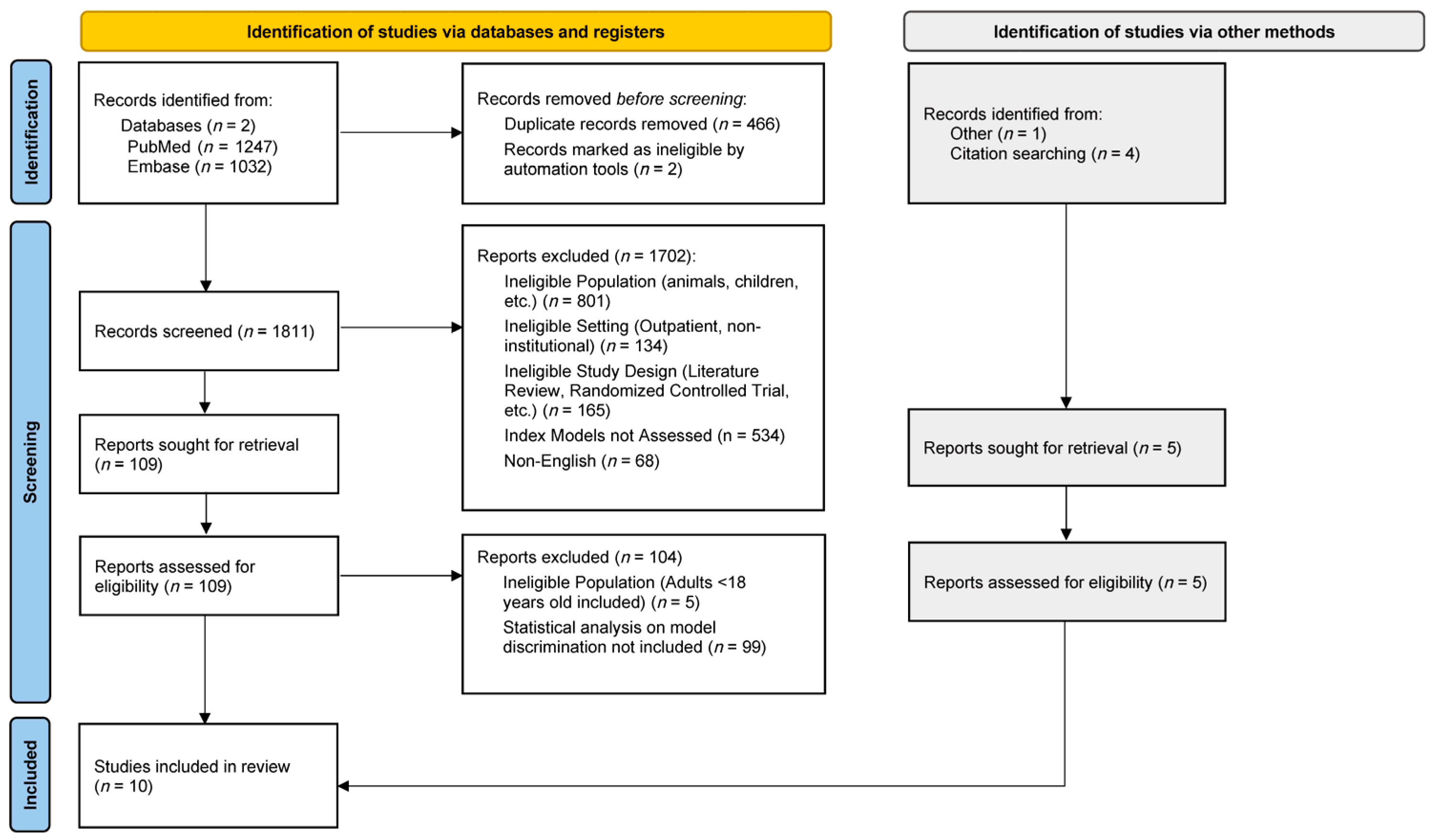
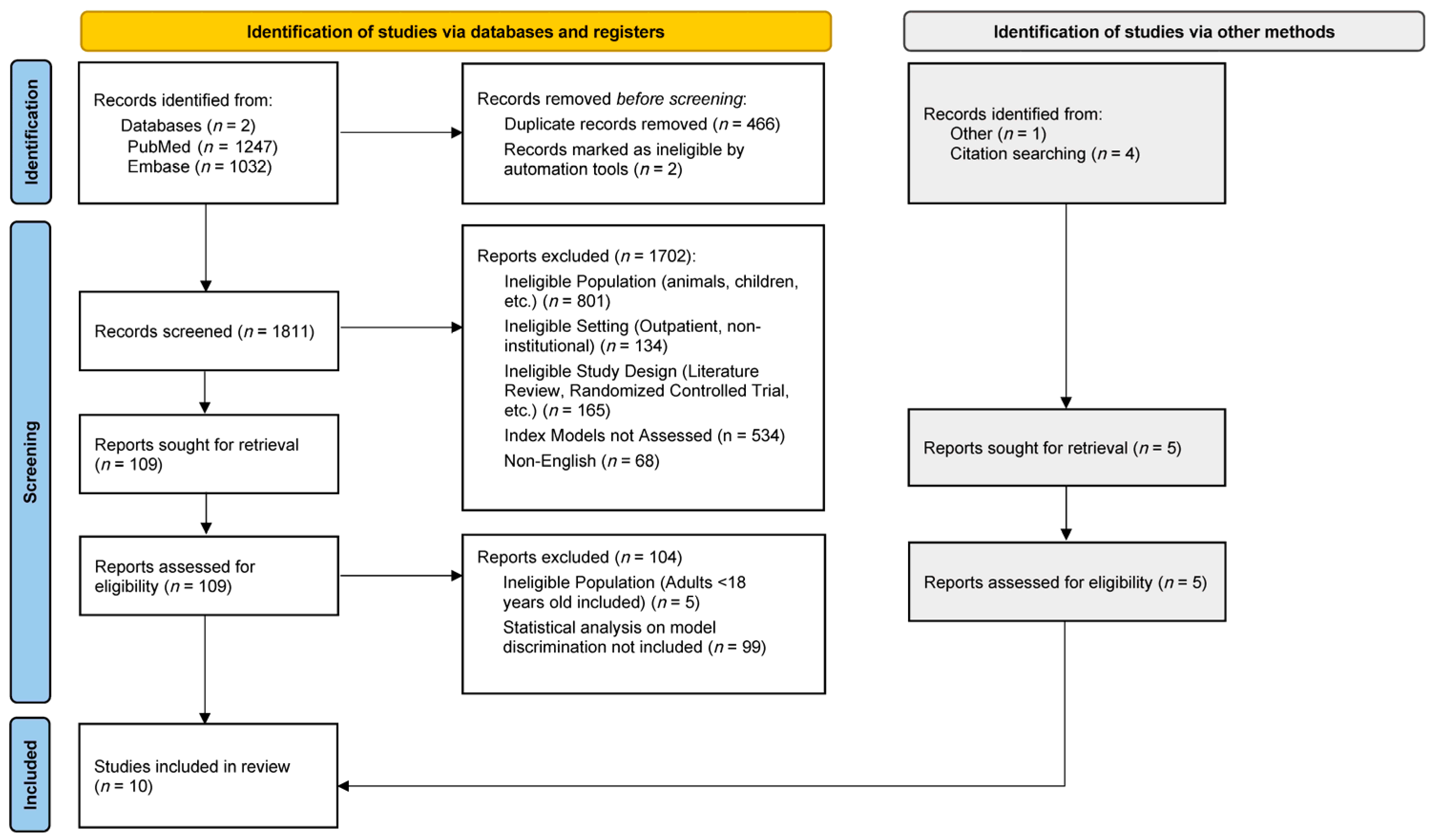
2.1. Study Selection
2.2. Study and Model Characteristics
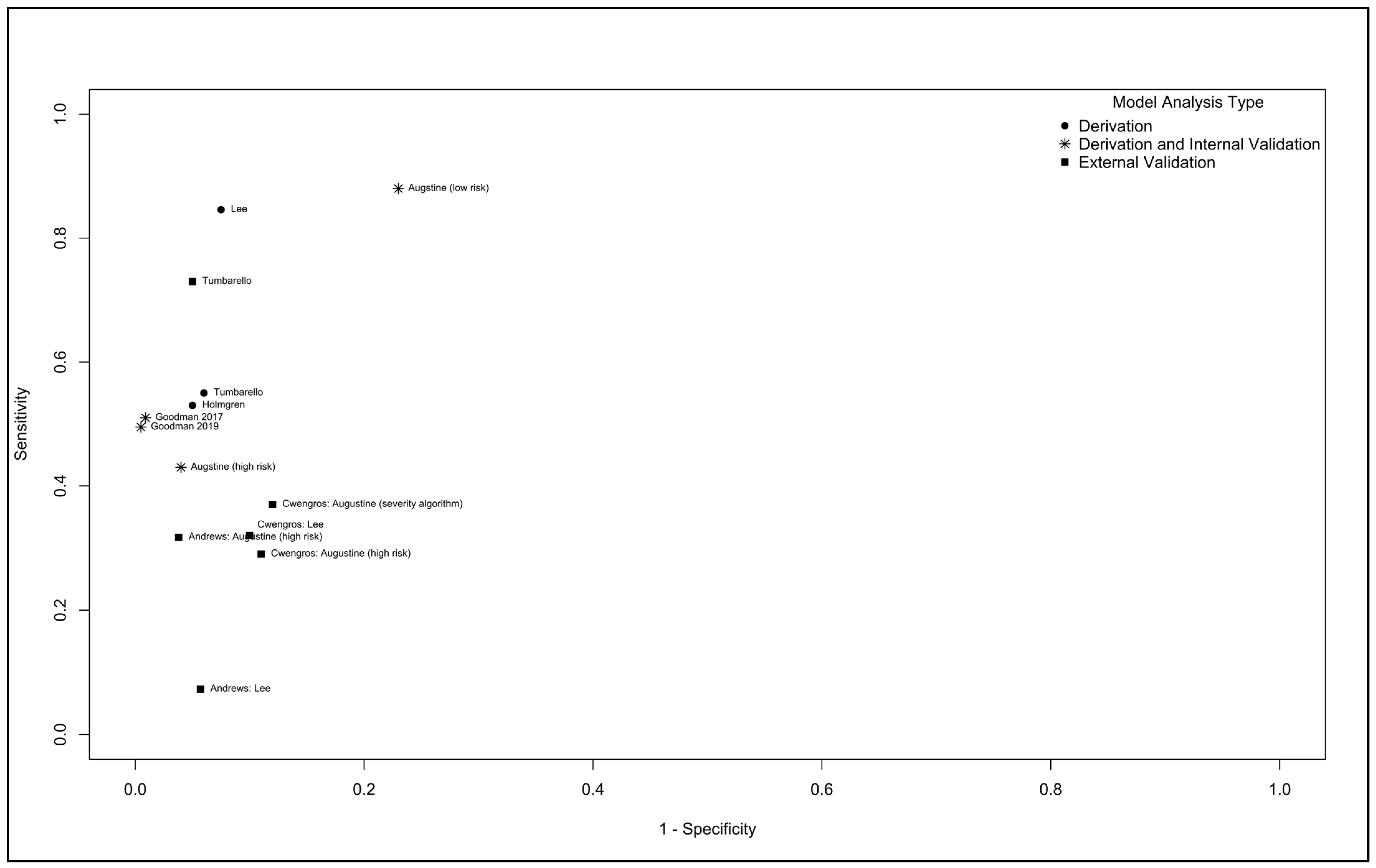
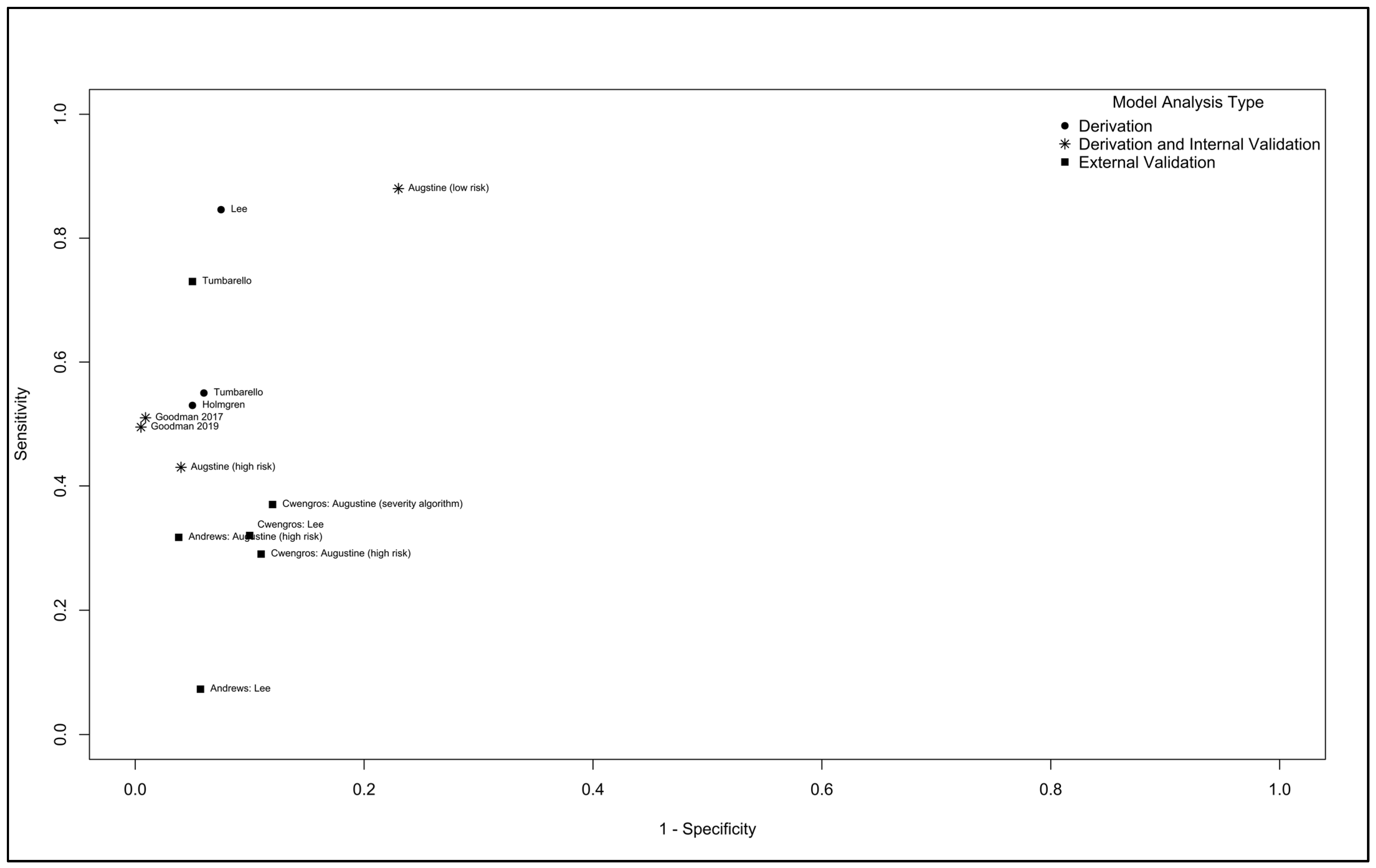
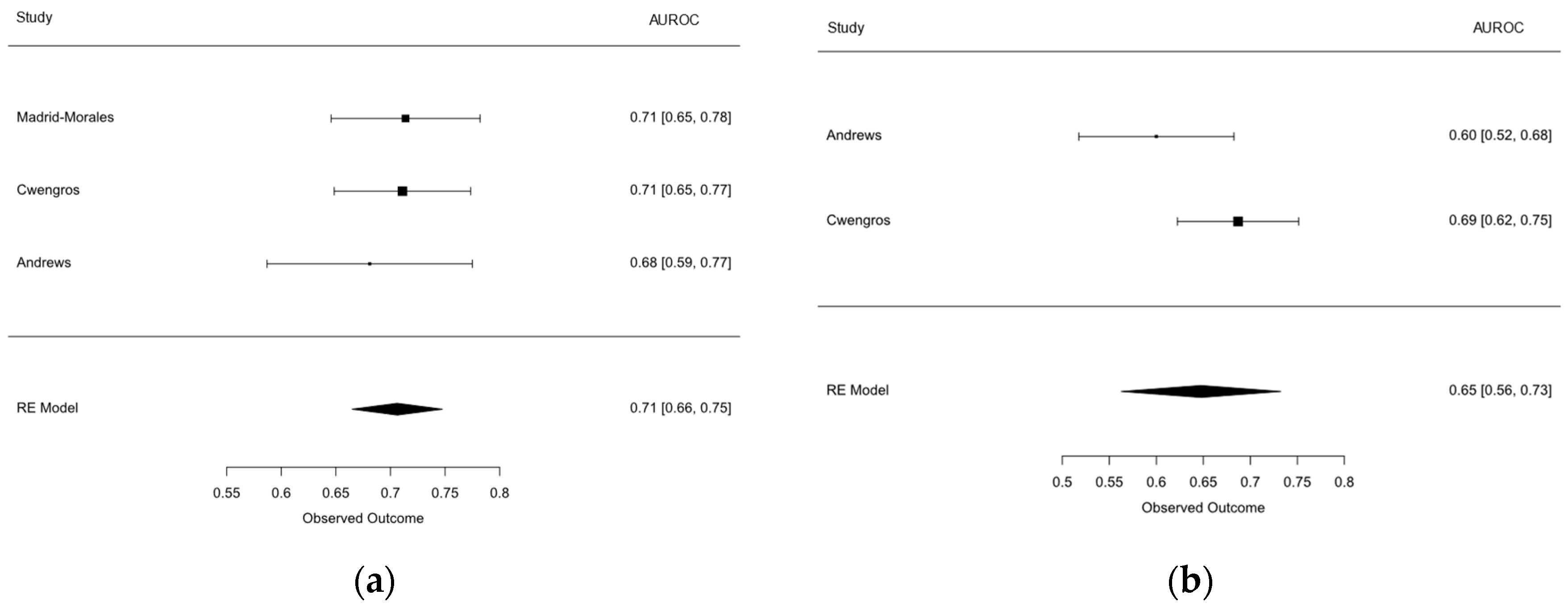
2.3. Results of Model Performance in Individual and Pooled Studies
2.4. Clinical Utility
3. Discussion
4. Materials and Methods
4.1. Study Selection
4.2. Data Extraction
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- CDC. Antibiotic Resistance Threats in the United States; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2019.
- van Duin, D.; Paterson, D.L. Multidrug-Resistant Bacteria in the Community: An Update. Infect. Dis. Clin. N. Am. 2020, 34, 709–722. [Google Scholar] [CrossRef]
- Serwecińska, L. Antimicrobials and Antibiotic-Resistant Bacteria: A Risk to the Environment and to Public Health. Water 2020, 12, 3313. [Google Scholar] [CrossRef]
- Cizman, M.; Plankar Srovin, T. Antibiotic consumption and resistance of gram-negative pathogens (collateral damage). GMS Infect. Dis. 2018, 6, Doc05. [Google Scholar] [CrossRef]
- Smith, R.A.; M’Ikanatha N, M.; Read, A.F. Antibiotic resistance: A primer and call to action. Health Commun. 2015, 30, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Baena, Z.R.; Giannella, M.; Manissero, D.; Rodríguez-Baño, J.; Viale, P.; Lopes, S.; Wilson, K.; McCool, R.; Longshaw, C. Risk factors for carbapenem-resistant Gram-negative bacterial infections: A systematic review. Clin. Microbiol. Infect. 2021, 27, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Lodise, T.P.; Zhao, Q.; Fahrbach, K.; Gillard, P.J.; Martin, A. A systematic review of the association between delayed appropriate therapy and mortality among patients hospitalized with infections due to Klebsiella pneumoniae or Escherichia coli: How long is too long? BMC Infect. Dis. 2018, 18, 625. [Google Scholar] [CrossRef]
- Li, C.; Claeys, K.C.; Justo, J.A.; Heil, E.L. Heil. No Crystal Ball? Using Risk Factors and Scoring Systems ot Predict Extended-Spectrum Beta-Lactamase Producing Enterobacterales (ESBL-E) and Carbapenem-Resistant Enterobacterales (CRE) Infections. Curr. Infect. Dis. Rep. 2022, 24, 147–158. [Google Scholar] [CrossRef]
- Andrews, S.R.; Timbrook, T.T.; Fisher, M.A.; Tritle, B.J. Evaluation of a Rapid Diagnostic Test and Scoring Tools for Predicting Ceftriaxone Resistance in Enterobacterales Bloodstream Infections. In Proceedings of the IDWeek 2023, Boston, MA, USA, 11–15 October 2023. [Google Scholar]
- Augustine, M.R.; Testerman, T.L.; Justo, J.A.; Bookstaver, P.B.; Kohn, J.; Albrecht, H.; Al-Hasan, M.N. Clinical Risk Score for Prediction of Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae in Bloodstream Isolates. Infect. Control Hosp. Epidemiol. 2017, 38, 266–272. [Google Scholar] [CrossRef]
- Cwengros, L.N.; Mynatt, R.P.; Timbrook, T.T.; Mitchell, R.; Salimnia, H.; Lephart, P.; Pogue, J.M. Minimizing Time to Optimal Antimicrobial Therapy for Enterobacteriaceae Bloodstream Infections: A Retrospective, Hypothetical Application of Predictive Scoring Tools vs Rapid Diagnostics Tests. Open Forum Infect. Dis. 2020, 7, ofaa278. [Google Scholar] [CrossRef]
- Goodman, K.E.; Lessler, J.; Cosgrove, S.E.; Harris, A.D.; Lautenbach, E.; Han, J.H.; Milstone, A.M.; Massey, C.J.; Tamma, P.D.; Antibacterial Resistance Leadership, G. A Clinical Decision Tree to Predict Whether a Bacteremic Patient Is Infected with an Extended-Spectrum β-Lactamase-Producing Organism. Clin. Infect. Dis. 2016, 63, 896–903. [Google Scholar] [CrossRef]
- Goodman, K.E.; Lessler, J.; Harris, A.D.; Milstone, A.M.; Tamma, P.D. A methodological comparison of risk scores versus decision trees for predicting drug-resistant infections: A case study using extended-spectrum beta-lactamase (ESBL) bacteremia. Infect. Control Hosp. Epidemiol. 2019, 40, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, A.; Ljung, A.; Bremell, D. An easy-to-use scoring system for predicting bacteraemia with third-generation cephalosporin-resistant Enterobacterales in a low-resistance setting. Infect. Dis. 2020, 52, 242–248. [Google Scholar] [CrossRef]
- Lee, C.H.; Chu, F.Y.; Hsieh, C.C.; Hong, M.Y.; Chi, C.H.; Ko, W.C.; Lee, C.C. A simple scoring algorithm predicting extended-spectrum β-lactamase producers in adults with community-onset monomicrobial Enterobacteriaceae bacteremia: Matters of frequent emergency department users. Medicine 2017, 96, e6648. [Google Scholar] [CrossRef]
- Madrid-Morales, J.; Sharma, A.; Reveles, K.; Velez-Mejia, C.; Hopkins, T.; Yang, L.; Walter, E.; Cadena, J. Validation of Available Extended-Spectrum-Beta-Lactamase Clinical Scoring Models in Predicting Drug Resistance in Patients with Enteric Gram-Negative Bacteremia Treated at South Texas Veterans Health Care System. Antimicrob. Agents Chemother. 2021, 65. [Google Scholar] [CrossRef] [PubMed]
- Tumbarello, M.; Trecarichi, E.M.; Bassetti, M.; De Rosa, F.G.; Spanu, T.; Di Meco, E.; Losito, A.R.; Parisini, A.; Pagani, N.; Cauda, R. Identifying patients harboring extended-spectrum-beta-lactamase-producing Enterobacteriaceae on hospital admission: Derivation and validation of a scoring system. Antimicrob. Agents Chemother. 2011, 55, 3485–3490. [Google Scholar] [CrossRef]
- Weston, G.; Jahufar, F.; Sharma, N.; Su, C.; Bellin, E.; Ostrowsky, B. Derivation of a Model to Guide Empiric Therapy for Carbapenem-Resistant Klebsiella pneumoniae Bloodstream Infection in an Endemic Area. Open Forum Infect. Dis. 2020, 7, ofaa070. [Google Scholar] [CrossRef] [PubMed]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Siontis, G.C.; Tzoulaki, I.; Castaldi, P.J.; Ioannidis, J.P. External validation of new risk prediction models is infrequent and reveals worse prognostic discrimination. J. Clin. Epidemiol. 2015, 68, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Debray, T.P.; Vergouwe, Y.; Koffijberg, H.; Nieboer, D.; Steyerberg, E.W.; Moons, K.G. A new framework to enhance the interpretation of external validation studies of clinical prediction models. J. Clin. Epidemiol. 2015, 68, 279–289. [Google Scholar] [CrossRef]
- Ramspek, C.L.; Jager, K.J.; Dekker, F.W.; Zoccali, C.; van Diepen, M. External validation of prognostic models: What, why, how, when and where? Clin. Kidney J. 2021, 14, 49–58. [Google Scholar] [CrossRef]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. J. Clin. Epidemiol. 2015, 68, 134–143. [Google Scholar] [CrossRef]
- Pate, A.; Riley, R.D.; Collins, G.S.; van Smeden, M.; Van Calster, B.; Ensor, J.; Martin, G.P. Minimum sample size for developing a multivariable prediction model using multinomial logistic regression. Stat. Methods Med. Res. 2023, 32, 555–571. [Google Scholar] [CrossRef] [PubMed]
- Snell, K.I.E.; Archer, L.; Ensor, J.; Bonnett, L.J.; Debray, T.P.A.; Phillips, B.; Collins, G.S.; Riley, R.D. External validation of clinical prediction models: Simulation-based sample size calculations were more reliable than rules-of-thumb. J. Clin. Epidemiol. 2021, 135, 79–89. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Vergouwe, Y. Towards better clinical prediction models: Seven steps for development and an ABCD for validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef] [PubMed]
- Haimerl, B.J.; Encinas, R.; Justo, J.A.; Kohn, J.; Bookstaver, P.B.; Winders, H.R.; Al-Hasan, M.N. Optimization of Empirical Antimicrobial Therapy in Enterobacterales Bloodstream Infection Using the Extended-Spectrum Beta-Lactamase Prediction Score. Antibiotics 2023, 12, 1003. [Google Scholar] [CrossRef] [PubMed]
- Pogue, J.M.; Heil, E.L. The Clinical Impact of a Negative Molecular beta-Lactamase Gene Test for Enterobacteriaceae: Let’s Not Let Perfect Be the Enemy of Really Good. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed]
- Pogue, J.M.; Heil, E.L.; Lephart, P.; Johnson, J.K.; Mynatt, R.P.; Salimnia, H.; Claeys, K.C. An Antibiotic Stewardship Program Blueprint for Optimizing Verigene BC-GN within an Institution: A Tale of Two Cities. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2023 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. Clin. Infect. Dis. 2023, ciad428. [Google Scholar] [CrossRef]
- Lagace-Wiens, P.R.; Adam, H.J.; Karlowsky, J.A.; Nichol, K.A.; Pang, P.F.; Guenther, J.; Webb, A.A.; Miller, C.; Alfa, M.J. Identification of blood culture isolates directly from positive blood cultures by use of matrix-assisted laser desorption ionization-time of flight mass spectrometry and a commercial extraction system: Analysis of performance, cost, and turnaround time. J. Clin. Microbiol. 2012, 50, 3324–3328. [Google Scholar] [CrossRef]
- Idelevich, E.A.; Schule, I.; Grunastel, B.; Wullenweber, J.; Peters, G.; Becker, K. Rapid identification of microorganisms from positive blood cultures by MALDI-TOF mass spectrometry subsequent to very short-term incubation on solid medium. Clin. Microbiol. Infect. 2014, 20, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- MacFadden, D.R.; Coburn, B.; Shah, N.; Robicsek, A.; Savage, R.; Elligsen, M.; Daneman, N. Decision-support models for empiric antibiotic selection in Gram-negative bloodstream infections. Clin. Microbiol. Infect. 2019, 25, 108.e1–108.e7. [Google Scholar] [CrossRef]
- Lodise, T.P.; Bonine, N.G.; Ye, J.M.; Folse, H.J.; Gillard, P. Development of a bedside tool to predict the probability of drug-resistant pathogens among hospitalized adult patients with gram-negative infections. BMC Infect. Dis. 2019, 19, 718. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Wolff, R.F.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S. PROBAST: A Tool to Assess Risk of Bias and Applicability of Prediction Model Studies: Explanation and Elaboration. Ann. Intern. Med. 2019, 170, W1–W33. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Kengne, A.P.; Grobbee, D.E.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Woodward, M. Risk prediction models: II. External validation, model updating, and impact assessment. Heart 2012, 98, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Snell, K.I.E.; Levis, B.; Damen, J.A.A.; Dhiman, P.; Debray, T.P.A.; Hooft, L.; Reitsma, J.B.; Moons, K.G.M.; Collins, G.S.; Riley, R.D. Transparent reporting of multivariable prediction models for individual prognosis or diagnosis: Checklist for systematic reviews and meta-analyses (TRIPOD-SRMA). BMJ 2023, 381, e073538. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; de Groot, J.A.; Bouwmeester, W.; Vergouwe, Y.; Mallett, S.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: The CHARMS checklist. PLoS Med. 2014, 11, e1001744. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Damen, J.A.A.; Moons, K.G.M.; van Smeden, M.; Hooft, L. How to conduct a systematic review and meta-analysis of prognostic model studies. Clin. Microbiol. Infect. 2023, 29, 434–440. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses inRwith themetaforPackage. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country | Design | Model Type | Sample Size | Resistance Type | Resistance Incidence |
|---|---|---|---|---|---|---|
| Andrews 2023 [9] | USA | Retrospective cohort | External validation of Lee 2017 and Augustine 2017 | 356 | ESBL | 11.5% |
| Augustine 2017 [10] | USA | Retrospective cohort | Derivation and internal validation | 910 | ESBL | 4.6% |
| Cwengros 2020 [11] | USA | Retrospective cohort | External validation of Lee 2017 and Augustine 2017 | 451 | ESBL | 16% |
| Goodman 2016 [12] | USA | Retrospective cohort | Derivation and internal validation | 1288 | ESBL | 15% |
| Goodman 2019 [13] | USA | Retrospective cohort | Derivation and internal validation | 1288 | ESBL | 15% |
| Holmgren 2020 [14] | Sweden | Retrospective cohort | Derivation | 625 | ESBL | 9% |
| Lee 2017 [15] | Taiwan | Retrospective cohort | Derivation | 1141 | ESBL | 5.7% |
| Madrid-Morales 2021 [16] | USA | Retrospective cohort | External validation of Augustine, 2017; Goodman, 2016 and 2019; and Tumbarello, 2011 | 145 | ESBL | 13.8% |
| Tumbarello 2011 [17] | Italy | Retrospective case–control | Derivation and external validation | 339; 510 | ESBL | 33.3%; 20% |
| Weston 2020 [18] | USA | Retrospective case–control | Derivation and internal validation | 341 | CRE | NA |
| Study | Demographics | Hospitalization/Admission History | Medical History | Procedure/Intervention History | Medication Use History | Other |
|---|---|---|---|---|---|---|
| Augustine 2017 [10] | - | - | ESBL-E infection or colonization | GI/GU procedure | Number of prior BL/FQ courses | - |
| Goodman 2016 [12] | Age, ≥43 years | Hospitalization in ESBL high-burden region | ESBL-E infection or colonization, chronic indwelling vascular hardware | - | Days of antibiotic exposure | |
| Goodman 2019 [13] | - | Hospital care abroad, prior hospitalization | COPD, emphysema, ventilator dependence, indwelling hardware, MDRO colonization or infection | - | Weeks of antibiotic exposure | Source of infection |
| Hömgren 2019 [14] | - | Hospital care abroad | ESBL-E infection or colonization | - | - | - |
| Lee 2017 [15] | - | Prior hospitalization, recent ED visits | Urological diseases, diabetes mellitus | Invasive procedure | Antibiotic exposure | Nursing home residents |
| Tumbarello 2011 [17] | Age, ≥70 years | Recent hospitalization, admission from healthcare | Charlson comorbidity index, urinary catheterization | - | Previous therapy with β-lactams and/or fluoroquinolones | - |
| Weston 2020 [18] | - | Admitted >3 days | Prior CRE culture, liver disease, mechanical ventilation | - | Proton pump inhibitor, antibiotic exposure | Admission from SNF, no prior culture |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timbrook, T.T.; Fowler, M.J. Predicting Extended-Spectrum Beta-Lactamase and Carbapenem Resistance in Enterobacteriaceae Bacteremia: A Diagnostic Model Systematic Review and Meta-Analysis. Antibiotics 2023, 12, 1452. https://doi.org/10.3390/antibiotics12091452
Timbrook TT, Fowler MJ. Predicting Extended-Spectrum Beta-Lactamase and Carbapenem Resistance in Enterobacteriaceae Bacteremia: A Diagnostic Model Systematic Review and Meta-Analysis. Antibiotics. 2023; 12(9):1452. https://doi.org/10.3390/antibiotics12091452
Chicago/Turabian StyleTimbrook, Tristan T., and McKenna J. Fowler. 2023. "Predicting Extended-Spectrum Beta-Lactamase and Carbapenem Resistance in Enterobacteriaceae Bacteremia: A Diagnostic Model Systematic Review and Meta-Analysis" Antibiotics 12, no. 9: 1452. https://doi.org/10.3390/antibiotics12091452
APA StyleTimbrook, T. T., & Fowler, M. J. (2023). Predicting Extended-Spectrum Beta-Lactamase and Carbapenem Resistance in Enterobacteriaceae Bacteremia: A Diagnostic Model Systematic Review and Meta-Analysis. Antibiotics, 12(9), 1452. https://doi.org/10.3390/antibiotics12091452