

Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan

 , ,
, ,
Abstract
1. Introduction
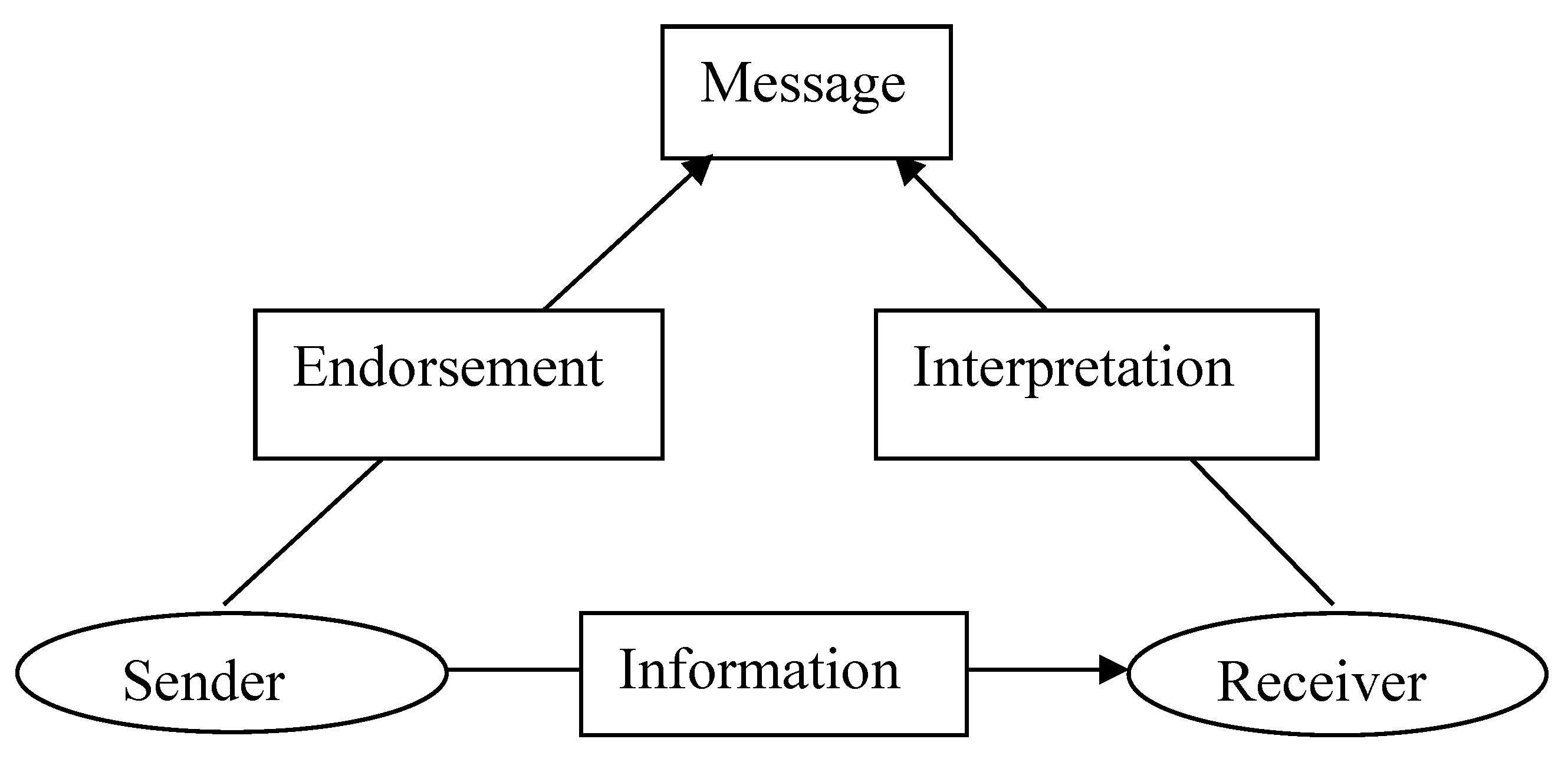
Theories and Conceptual Framework
2. Methods
2.1. Simulated Clients
2.2. Communication Skills Assessment
2.3. Pilot Study
2.4. Documentation of Feedback
2.5. Study Setting
2.6. Pharmacy Selection
2.7. Scenarios
Scenario 1
Scenario 2
2.8. Ethical Considerations
2.9. Data Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, S.; Kim, D.; Choi, H.J.; Chang, M.J. A comparison of patients’ and pharmacists’ satisfaction with medication counseling provided by community pharmacies: A cross-sectional survey. BMC Health Serv. Res. 2016, 16, 131. [Google Scholar] [CrossRef]
- Kashour, T.S.; Joury, A.; Alotaibi, A.M.; Althagafi, M.; Almufleh, A.S.; Hersi, A.; Thalib, L. Quality of assessment and counselling offered by community pharmacists and medication sale without prescription to patients presenting with acute cardiac symptoms: A simulated client study. Eur. J. Clin. Pharm. 2015, 72, 321–328. [Google Scholar] [CrossRef]
- Berger, K.; Eickhoff, C.; Schulz, M. Counseling quality in community pharmacies: Implementation of the pseudo customer methodology in Germany. J. Clin. Pharm. Ther. 2005, 30, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.T.; Roque, F.; Gonzalez, C.; Soares, S.; Figueiras, A.; Herdeiro, M.T. Improving Antibiotic Use through Educational Interventions. Microbial Pathogens and Strategies For Combating Them: Science, Technology and Education. Available online: www.formatex.info/microbiology4/vol3/1706-1714.pdf (accessed on 12 February 2023).
- Palaian, S.; Prabhu, M.; Shankar, P.R. Patient counseling by pharmacist—A focus on chronic illness. Pak. J. Pharm. Sci. 2006, 19, 65–72. [Google Scholar] [PubMed]
- Okumura, L.M.; Rotta, I.; Correr, C.J. Assessment of pharmacist-led patient counseling in randomized controlled trials: A systematic review. Pharm. Weekbl. 2014, 36, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Alaqeel, S.; Abanmy, N.O. Counseling practices in community pharmacies in Riyadh, Saudi Arabia: A cross-sectional study. BMC Health Serv. Res. 2015, 15, 557. [Google Scholar] [CrossRef]
- Hussain, A.; Ibrahim, M.I.M. Medication counselling and dispensing practices at community pharmacies: A comparative cross sectional study from Pakistan. Pharm. Weekbl. 2011, 33, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Al Aqeel, S.; Abanmy, N.; Alshaya, H.; AlMeshari, A. Interventions for improving pharmacist-led patient counselling in the community setting: A systematic review. Syst. Rev. 2018, 7, 1–13. [Google Scholar] [CrossRef]
- Kheir, N. Pharmacy Practice in Qatar. Elsevier Inc. Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000125 (accessed on 12 February 2023).
- Medication Errors Cause Half a Million Deaths in Pakistan, Say Pharmacists. Available online: https://www.dawn.com/news/1362951 (accessed on 12 February 2023).
- Del Arco, A.; Tortajada, B.; de la Torre, J.; Olalla, J.; Padra, J.L.; Montiel, N.; García-Alegría, J. Results of a counselling programme in antibiotic treatment in a secondary hospital. Rev. Esp. Quimioter. 2011, 24, 96–98. [Google Scholar] [PubMed]
- WHO 2014. The Role of Pharmacist in Encouraging Prudent Use of Antibiotics and Averting Antimicrobial Resistance: A Review Ofpol-Icy and Experience. Available online: http://apps.who.int/medicinedocs/en/m/abstract/Js22244en/ (accessed on 12 February 2023).
- Bradley, J.; Langford, A.M. Morris. Is it time to stop counselling patients to “finish the course of antibiotics”? Can. Pharm. J. 2017, 150, 349–350. [Google Scholar]
- Pai, M.P.; Momary, K.M.; Rodvold, K.A. Antibiotic drug interactions. Med. Clin. N. Am. 2006, 90, 1223–1255. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.H.; Coombes, I. Mortality from common drug interactions systems, knowledge and clinical reasoning to optimise prescribing. Intern. Med. J. 2014, 44, 621–622. [Google Scholar] [CrossRef]
- Ashdown, H.F.; Räisänen, U.; Wang, K.; Ziebland, S.; Harnden, A. Prescribing antibiotics to ‘at-risk’ children with influenza-like illness in primary care: Qualitative study. BMJ Open 2016, 6, e011497. [Google Scholar] [CrossRef] [PubMed]
- Beckett, C.; Harbarth, S.; Huttner, B. Special considerations of antibiotic prescription in the geriatric population. Clin. Microbiol. Infect. 2015, 21, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Ansari, J. Drug Interaction and Pharmacist. J. Young -Pharm. 2010, 2, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.M.; Masood, I.; Yousaf, M.; Saleem, H.; Ye, D.; Fang, Y. Pattern of medication selling and self-medication practices: A study from Punjab, Pakistan. PLoS ONE 2018, 13, e0194240. [Google Scholar] [CrossRef]
- Babar, Z.D.; Jamshed, S. Social pharmacy strengthening clinical pharmacy: Why pharmaceutical policy research is needed in Paki-stan? Pharm. World Sci. 2008, 30, 617–619. [Google Scholar] [CrossRef]
- Hussain, A.; Malik, M.; Toklu, H.Z. A literature review: Pharmaceutical care an evolving role at community pharmacies in Pakistan. Pharmacol. Pharm. 2013, 4, 425–630. [Google Scholar] [CrossRef]
- Khalid, L.; Mahsood, N.; Ali, I. The public health problem of OTC antibiotics in developing nations. Res. Soc. Adm. Pharm. 2016, 12, 801–802. [Google Scholar] [CrossRef]
- Rabbani, F.; Cheema, F.H.; Talati, N.; Siddiqui, S.; Syed, S.; Bashir, S.; Zuberi, L.Z.; Shamim, A.; Mumtaz, Q. Behind the counter: Pharmacies and dispensing patterns of pharmacy attendants in Karachi. J. Pak. Med. Assoc. 2001, 51, 149–153. [Google Scholar] [PubMed]
- Tully, M.P.; Beckman-Gyllenstrand, A.; Bernsten, C.B. Factors predicting poor counselling about prescription medicines in Swedish community pharmacies. Patient Educ. Couns. 2011, 83, 3–6. [Google Scholar] [CrossRef]
- Shah, B.; Chewning, B. Conceptualizing and measuring pharmacist-patient communication: A review of published studies. Res. Soc. Adm. Pharm. 2006, 2, 153–185. [Google Scholar] [CrossRef] [PubMed]
- Puspitasari, H.P.; Aslani, P.; Krass, I. A review of counseling practices on prescription medicines in community pharmacies. Res. Soc. Adm. Pharm. 2009, 5, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M. The role of communication skills: Developing patient-centred practice in community pharmacies. Chronic III 2004, 8, 10–14. [Google Scholar]
- Watson, M.C.; Norris, P.; Granas, A.G. A systematic review of the use of simulated patients and pharmacy practice research. Int. J. Pharm. Pr. 2006, 14, 83–93. [Google Scholar] [CrossRef]
- Specialized Healthcare & Medical Education Department (SHMED). Available online: http://health.punjab.gov.pk/ (accessed on 12 February 2023).
- Raosoft Inc. RaoSoft Sample Size Calculator. 2004. Available online: http://www.raosoft.com/samplesize.html (accessed on 1 June 2020).
- Adepu, R.; Nagavi, B. Attitudes and behaviors of practicing community pharmacists towards patient counselling. Indian J. Pharm. Sci. 2009, 71, 285–289. [Google Scholar] [CrossRef]
- Offor, I.; Enato, E. Patients’ Assessment of Pharmacists’ Medication Counseling in a Psychiatric Hospital in Nigeria. Trop. J. Pharm. Res. 2011, 10, 507–516. [Google Scholar] [CrossRef]
- Ibrahim, M.I.; Palaian, S.; Al-Sulaiti, F.; El-Shami, S. Evaluating community pharmacy practice in Qatar using simulated patient method: Acute gastroenteritis management. Pharm. Pract. 2016, 14, 1–8. [Google Scholar] [CrossRef]
- Horvat, N.; Koder, M.; Kos, M. Using the Simulated Patient Methodology to Assess Paracetamol-Related Counselling for Headache. PLoS ONE 2012, 7, e52510. [Google Scholar] [CrossRef]
- Chua, S.S.; Ramachandran, C.D.; Paraidathathu, T.T. Response of community pharmacists to the presentation of back pain: A simulated patient study. Int. J. Pharm. Pract. 2006, 14, 171–178. [Google Scholar] [CrossRef]
- Kline, J.M.; Wietholter, J.P.; Kline, V.T.; Confer, J. Pediatric Antibiotic Use: A focused review of Fluoroquinolones and Tetracyclines. US Pharm. 2012, 37, 59. Available online: https://www.uspharmacist.com/article/pediatric-antibiotic-use-a-focused-review-of-fluoroquinolones-and-tetracyclines (accessed on 12 February 2023).
- Masters, K.P.; Carr, B.M. Survey of pharmacists and physicians on drug interactions between combined oral contraceptives and broad-spectrum antibiotics. Pharm. Pract. 2009, 7, 139–144. [Google Scholar] [CrossRef]
- Weller, T.M.A.; Jamieson, C.E. The expanding role of the antibiotic pharmacist. J. Antimicrob. Chemother. 2004, 54, 295–298. [Google Scholar] [CrossRef]
- Alfadl, A.A.; Musaad, A.A.; Alhassun, S. Evaluation of medication counseling practice at community pharmacies in Qassim region, Saudi Arabia. Saudi Pharm. J. 2018, 26, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; McCombs, J.S.; Cheng, R.A.; Johnson, K.A. Pharmacist time requirements for counseling in an outpatient pharmacy. Am. J. Health Pharm. 2002, 59, 2346–2355. [Google Scholar] [CrossRef] [PubMed]
- Anwar, K.; Antibiotic Resistance: It’s Bug-ging. The Express Tribune. 26 April 2015. Available online: https://tribune.com.pk/story/874147/antibiotic-resistance-its-bug-ging/ (accessed on 12 February 2023).
- Tips for Proper Storage of Medications (TPSM). Available online: https://www.opatoday.com/medication-storage-tips (accessed on 12 February 2023).
- WHO 2003, Guidelines for the Storage of Essential Medicines and Other Health Commodities. Available online: http://apps.who.int/medicinedocs/en/d/Js4885e/6.5.html (accessed on 12 February 2023).
- Hawke, K.L.; McGuire, T.; Ranmuthugala, G.; Van Driel, M.L. What do consumers want to know about antibiotics? Analysis of a medicines call centre database. Fam. Pract. 2015, 33, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ayalew, M. Medication Counseling Practice in Ethiopia: A Systematic Review. J. Basic Clin. Pharm. 2017, 8, 1–5. [Google Scholar]
- Ejeta, F.; Feyisa, D.; Kebede, O.; Aferu, T.; Siraj, J.; Feyissa, D.; Wodajo, E.; Tamiru, A. Medication Counseling Practices in Medicine Retail Outlets Found in Bench Sheko Zone, Southern Nations, Nationalities, and Peoples’ Region, South West Ethiopia. Pragmatic Obs. Res. 2021, 12, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.K.; Edelman, A.; Jensen, J. Patient satisfaction and the impact of written material about postpartum contraceptive decisions. Am. J. Obstet. Gynecol. 2003, 188, 1202–1204. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Category | Scenario 1 (n = 554) | Scenario 2 (n = 465) | Overall % |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Class of pharmacy (Number of the sale counters reported by SCs) | 1 | 334 (60.3) | 287 (61.7) | 61 |
| 2–5 | 204 (36.8) | 164 (35.3) | 36.1 | |
| >5 | 16 (2.9) | 14 (3.0) | 2.9 | |
| Number of employees at the time of visit as reported by SCs | 1–5 | 389 (70.2) | 335 (72.1) | 71.2 |
| 6–10 | 156 (28.1) | 125 (26.8) | 27.5 | |
| >10 | 9 (1.6) | 5 (1.1) | 1.4 | |
| Gender of pharmacy retailers (contacted) | Male | 554 (100.0) | 465 (100.0) | 100.0 |
| Female | 0 (0.0) | 0 (0.0) | 0.0 | |
| Age of contacted retailer (years), estimated by SC | <25 | 19 (3.4) | 21 (4.5) | 3.9 |
| 25–35 | 164 (29.6) | 153 (32.9) | 31.3 | |
| 36–45 | 112 (20.2) | 140 (30.1) | 25.2 | |
| 46–55 | 202 (36.5) | 123 (26.5) | 31.5 | |
| >55 | 57 (10.3) | 28 (6.0) | 8.2 | |
| Day of the visit | Monday | 38 (6.8) | 65 (13.9) | 10.4 |
| Tuesday | 59 (10.6) | 42 (9.0) | 9.8 | |
| Wednesday | 110 (19.8) | 86 (18.5) | 19.1 | |
| Thursday | 79 (14.2) | 32 (6.9) | 10.6 | |
| Friday | 58 (10.5) | 101 (21.7) | 16.1 | |
| Saturday | 66 (11.9) | 70 (15.2) | 13.6 | |
| Sunday | 144 (25.9) | 69 (14.8) | 20.4 | |
| Time of visit | 8:00–12:00 | 146 (26.4) | 167 (35.9) | 31.1 |
| 12:00–14:00 | 35 (6.3) | 67(14.4) | 10.4 | |
| 14:00–22:00 | 373 (67.3) | 231 (49.7) | 58.5 | |
| Number of waiting customers | 0–5 | 361 (65.2) | 338 (72.7) | 68.9 |
| 6–10 | 184 (33.2) | 120 (25.8) | 29.5 | |
| >10 | 9 (1.6) | 7 (1.5) | 1.6 | |
| Waiting time (mints) | 1–5 | 224 (40.4) | 232 (49.9) | 45.2 |
| >5 | 330 (59.6) | 233 (50.1) | 54.8 | |
| Total time of conversation (talk about medication) (mints) | ≤2 | 311 (56.1) | 284 (61.0) | 58.6 |
| 3–5 | 234 (42.2) | 175 (37.6) | 39.9 | |
| >5 | 9 (1.7) | 6 (1.3) | 1.5 | |
| Privacy during conversation | Full provided | 1 (0.2) | 0 (0.0) | 0.09 |
| Semi provided | 17 (3.1) | 4 (0.9) | 2.0 | |
| Not provided | 536 (96.7) | 461 (99.1) | 97.9 |
| Response | Scenario 1 (n = 554) n (%) | Scenario 2 (n = 465) n (%) | Overall % | |
|---|---|---|---|---|
| Counseling without demand | 2 (0.3) | 32 (6.8) | 3.6 | |
| On demand counseling | Provided | 256 (46.2) | 204 (43.8) | 45 |
| Questioning and advised to contact a doctor | 179 (32.3) | 184 (39.5) | 35.9 | |
| Directly advised to contact a doctor | 117 (21.1) | 45 (9.6) | 15.4 | |
| Questions Asked | Scenario 1 (n = 437) n (%) | Scenario 2 (n = 420) n (%) | Overall % |
|---|---|---|---|
| Duration of disease or therapy | 301 (68.8) | 97 (23.0) | 45.9 |
| Whether had taken medicine before | 195 (44.6) | 161 (38.3) | 45.5 |
| Why the medicine was prescribed | - | 91 (21.6) | 21.6 *1 |
| Any co-morbidity or its treatment? | 287 (65.6) | 81 (19.2) | 42.4 |
| Any allergy to medicine in history? | 79 (18.0) | 55 (13.0) | 15.5 |
| Do you know how to take medicine? | 15 (3.4) | 76 (18.0) | 10.7 |
| You want to ask anything else? | 3 (0.7) | 18 (4.2) | 2.5 |
| Information Provided | Scenario 1 (n = 258) n (%) | Scenario 2 (n = 236) n (%) | Overall% |
|---|---|---|---|
| The name of the medicine discussed | - | 13 (5.5) | 5.5 *1 |
| Drug storage | 0 (0.0) | 0 (0.0) | 0.0 |
| How to take the medication (e.g., with/before/after meal) | 7 (2.7) | 12 (5.1) | 3.9 |
| Discussed root of drug administration | 0 (0.0) | 9 (3.8) | 1.9 |
| Dose of therapy | 219 (84.9) | 185 (78.4) | 81.6 |
| Duration of therapy | 107 (41.4) | 173 (73.3) | 57.4 |
| Possible side effects of therapy | 2 (0.8) | 3 (1.3) | 1.1 |
| Possible drug-drug interaction | 4 (1.5) | 3 (1.3) | 1.4 |
| Life style modification or dietary instruction | 113 (43.8) | 153 (64.8) | 54.3 |
| Any other special warnings or precautions about medication | 4 (1.5) | 3 (1.3) | 1.4 |
| Non compliance to medication and its effect | 0 (0.0) | 0 (0.0) | 0.0 |
| Effect of medicine withdrawal | 0(0.0) | 0(0.0) | 0.0 |
| Other medication during this therapy | 0 (0.0) | 0 (0.0) | 0.0 |
| Reinsured that client understand all instructions | 49 (18.9) | 16 (6.8) | 12.8 |
| Advice to change medication | 4 (1.5) | 3 (1.2) | 1.4 |
| Skill Used | Scenario 1 (n = 258) | Scenario 2 (n = 236) | Overall (n = 494) |
|---|---|---|---|
| Eye contact | 2.3 ± 0.4 | 2.2 ± 0.5 | 2.25 ± 0.4 |
| Attention to customer | 2.5 ± 0.4 | 2.3 ± 0.4 | 2.4 ± 0.4 |
| Engagement of customer | 2.2 ± 0.3 | 2.2 ± 0.3 | 2.2 ± 0.3 |
| Non-verbal expressions used | 1.4 ± 0.2 | 1.4 ± 0.3 | 1.4 ± 0.2 |
| Provided written information | 1.1 ± 0.3 | 1.1 ± 0.4 | 1.1 ± 0.3 |
| Factors | Scenario 1 | Scenario 2 |
|---|---|---|
| Number of employees at the time of visit | 0.294 | 0.387 |
| Age of pharmacy retailer (contacted) | 0.013 | 0.656 |
| Day of visit | 0.178 | 0.614 |
| Time of visit | 0.627 | 0.952 |
| Number of waiting customers | 0.834 | 0.043 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, M.M.; Rasool, M.F.; Alanazi, M.; Alharby, T.N.; Alanazi, J.; Huwaimel, B. Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan. Antibiotics 2023, 12, 931. https://doi.org/10.3390/antibiotics12050931
Aziz MM, Rasool MF, Alanazi M, Alharby TN, Alanazi J, Huwaimel B. Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan. Antibiotics. 2023; 12(5):931. https://doi.org/10.3390/antibiotics12050931
Chicago/Turabian StyleAziz, Muhammad Majid, Muhammad Fawad Rasool, Muteb Alanazi, Tareq Nafea Alharby, Jowaher Alanazi, and Bader Huwaimel. 2023. "Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan" Antibiotics 12, no. 5: 931. https://doi.org/10.3390/antibiotics12050931
APA StyleAziz, M. M., Rasool, M. F., Alanazi, M., Alharby, T. N., Alanazi, J., & Huwaimel, B. (2023). Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan. Antibiotics, 12(5), 931. https://doi.org/10.3390/antibiotics12050931