Democratization of Point-of-Care Viral Biosensors: Bridging the Gap from Academia to the Clinic



Abstract
1. Introduction
2. Optical Methods
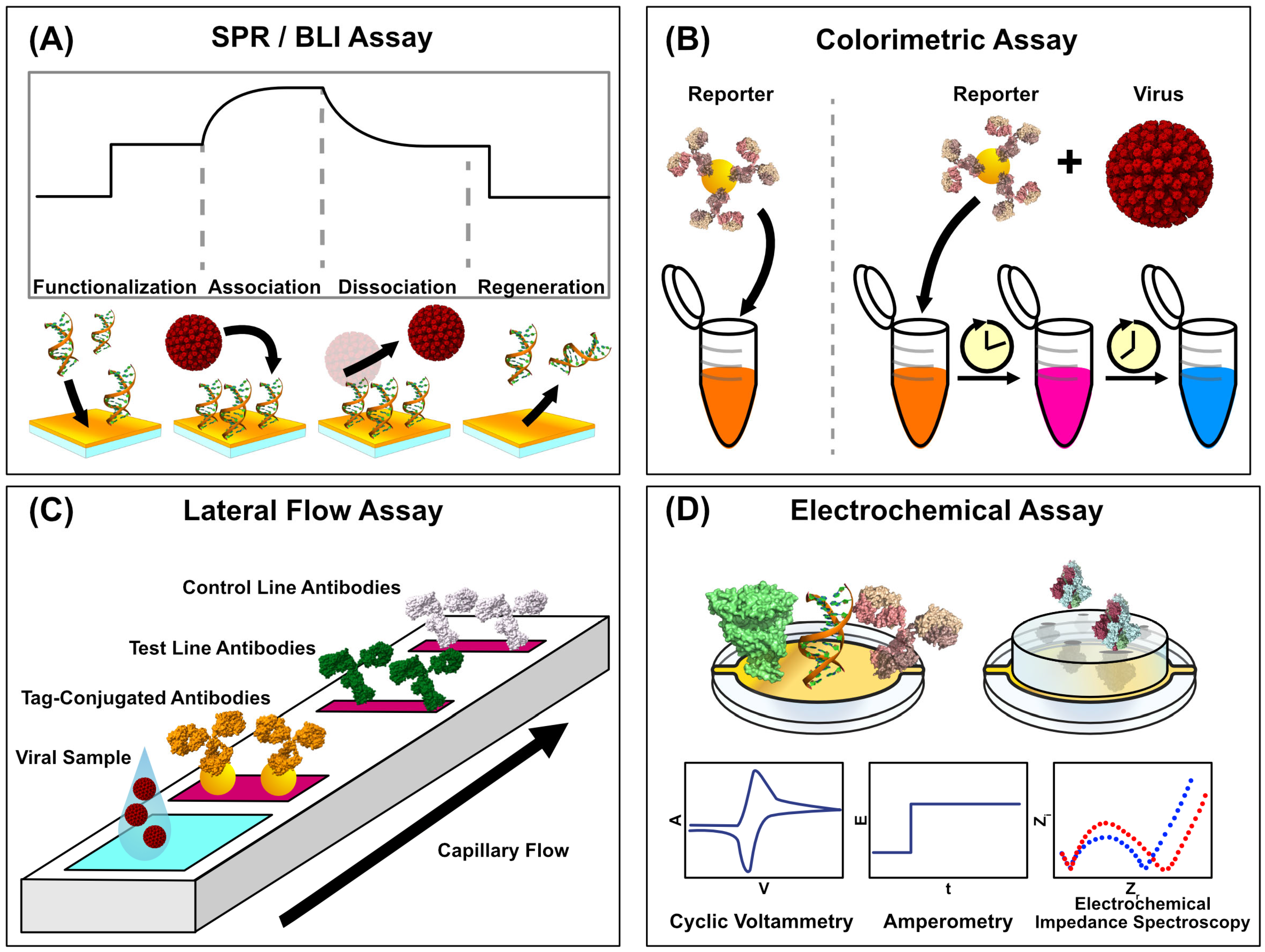
2.1. Surface Plasmon Resonance
2.2. Biolayer Interferometry
2.3. Colorimetric and Fluorescent Sensors
2.4. Non-Optical Methods
2.5. QCM
3. Comparing Approaches
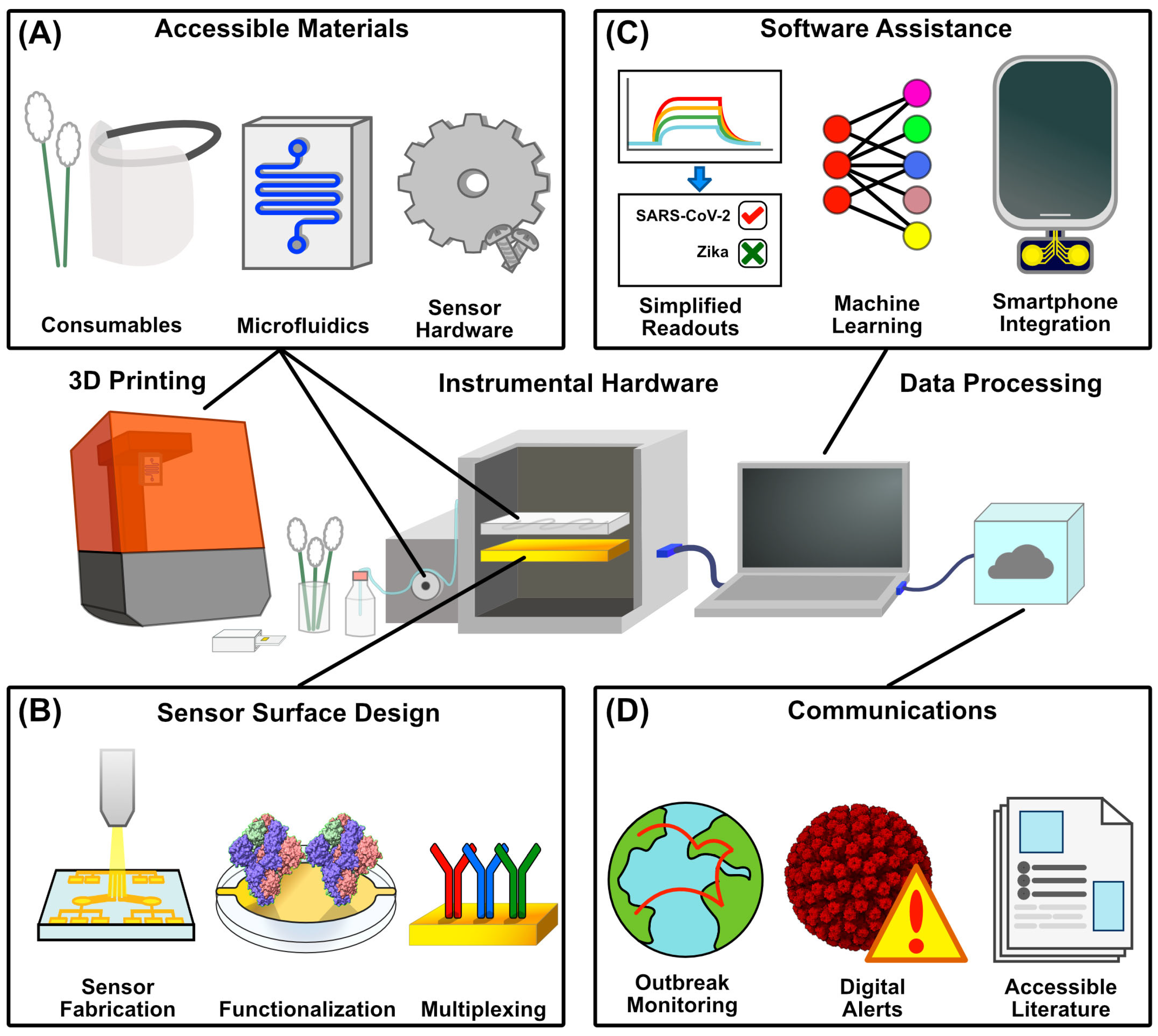
4. Diagnostic Development—Hardware and Software
4.1. Three-Dimensional Printing
4.2. Sensor Surface Fabrication
5. Software
6. Smartphone Apps
7. Democratizing Scientific Communications
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krammer, F.; Hermann, E.; Rasmussen, A.L. Highly Pathogenic Avian Influenza H5N1: History, Current Situation, and Outlook. J. Virol. 2025, 99, e02209-24. [Google Scholar] [CrossRef] [PubMed]
- Mylne, A.; Brady, O.J.; Huang, Z.; Pigott, D.M.; Golding, N.; Kraemer, M.U.G.; Hay, S.I. A Comprehensive Database of the Geographic Spread of Past Human Ebola Outbreaks. Sci. Data 2014, 1, 140042. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Ortiz, K.; Ansari, A.; Gershwin, M.E. The Zika Outbreak of the 21st Century. J. Autoimmun. 2016, 68, 1–13. [Google Scholar] [CrossRef]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Milind, T.; Mina, M.J.; Parker, R. Test Sensitivity Is Secondary to Frequency and Turnaround Time for COVID-19 Surveillance. medRxiv 2020. [Google Scholar] [CrossRef]
- Jean, S.; Burnham, C.-A.D.; Chapin, K.; Garner, O.B.; Pant Pai, N.; Turabelidze, G.; Butler-Wu, S. At-Home Testing for Infectious Diseases: The Laboratory Where You Live. Clin. Chem. 2022, 68, 19–26. [Google Scholar] [CrossRef]
- Marrazza, G.; Ramalingam, M.; Jaisankar, A.; Cheng, L.; Selvolini, G.; Vitale, I.A. Advancements and Emerging Technologies in Biosensors for Rapid and Accurate Virus Detection. TrAC Trends Anal. Chem. 2024, 172, 117609. [Google Scholar] [CrossRef]
- Otoo, J.A.; Schlappi, T.S. REASSURED Multiplex Diagnostics: A Critical Review and Forecast. Biosensors 2022, 12, 124. [Google Scholar] [CrossRef] [PubMed]
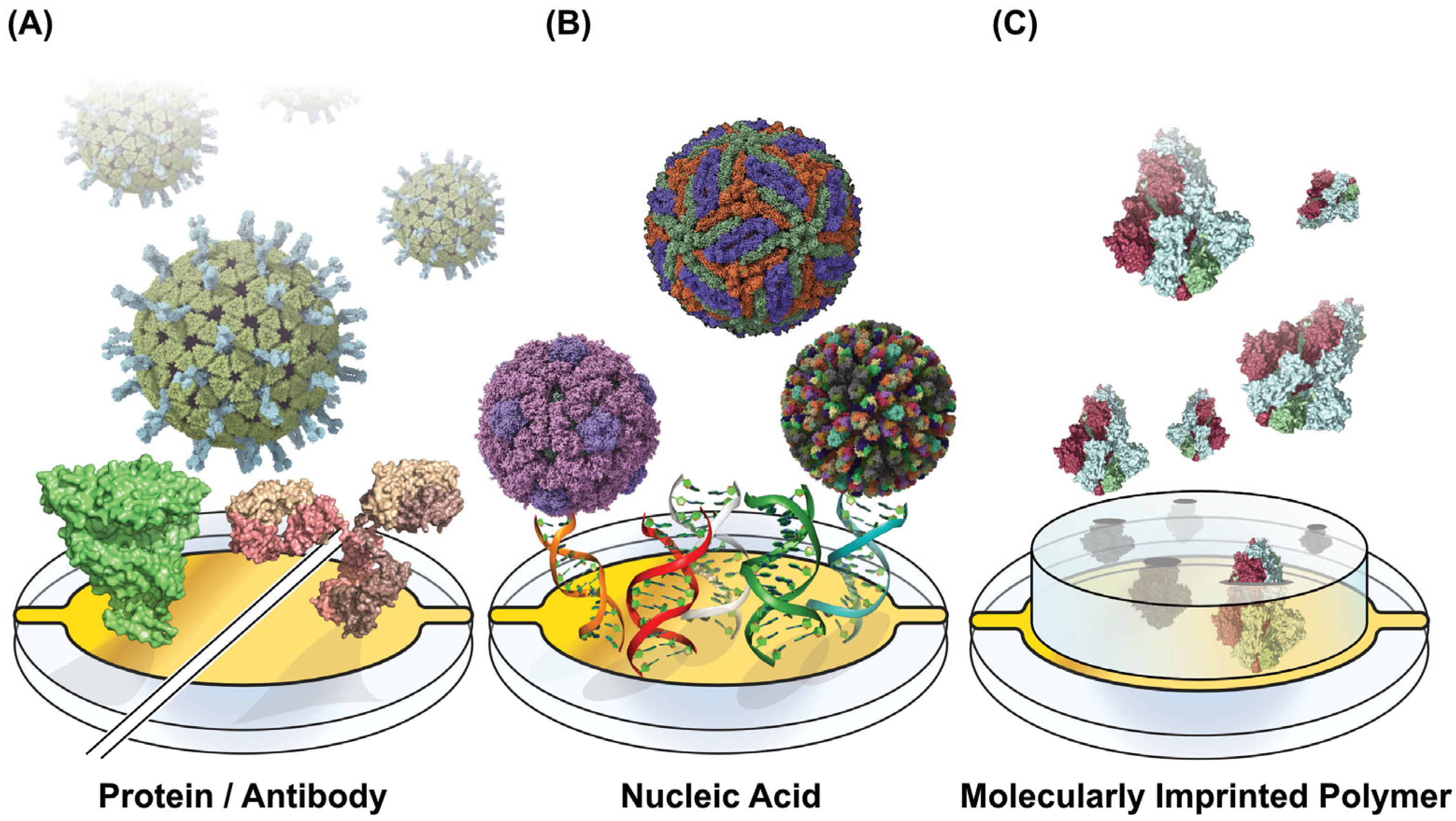
- Chambers, J.P.; Arulanandam, B.P.; Matta, L.L.; Weis, A.; Valdes, J.J. Biosensor Recognition Elements. Curr. Issues Mol. Biol. 2008, 10, 1–12. [Google Scholar]
- Thiviyanathan, V.; Gorenstein, D.G. Aptamers and the Next Generation of Diagnostic Reagents. Proteom. Clin. Appl. 2012, 6, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Karunakaran, R.; Keskin, M. Chapter 11—Biosensors: Components, Mechanisms, and Applications. In Analytical Techniques in Biosciences; Egbuna, C., Patrick-Iwuanyanwu, K.C., Shah, M.A., Ifemeje, J.C., Rasul, A., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 179–190. [Google Scholar] [CrossRef]
- Sajini, T.; Mathew, B. A Brief Overview of Molecularly Imprinted Polymers: Highlighting Computational Design, Nano and Photo-Responsive Imprinting. Talanta Open 2021, 4, 100072. [Google Scholar] [CrossRef]
- Wallace, S.; Kartau, M.; Kakkar, T.; Davis, C.; Szemiel, A.; Samardzhieva, I.; Vijayakrishnan, S.; Cole, S.; De Lorenzo, G.; Maillart, E.; et al. Multiplexed Biosensing of Proteins and Virions with Disposable Plasmonic Assays. ACS Sens. 2023, 8, 3338–3348. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, N.; Jolly, P.; Formisano, N.; Estrela, P. Introduction to Biosensors. Essays Biochem. 2016, 60, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Damborský, P.; Švitel, J.; Katrlík, J. Optical Biosensors. Essays Biochem. 2016, 60, 91–100. [Google Scholar] [CrossRef]
- Grieshaber, D.; MacKenzie, R.; Vörös, J.; Reimhult, E. Electrochemical Biosensors—Sensor Principles and Architectures. Sensors 2008, 8, 1400–1458. [Google Scholar] [CrossRef] [PubMed]
- Marx, K.A. Quartz Crystal Microbalance: A Useful Tool for Studying Thin Polymer Films and Complex Biomolecular Systems at the Solution−Surface Interface. Biomacromolecules 2003, 4, 1099–1120. [Google Scholar] [CrossRef]
- Mouro, J.; Pinto, R.; Paoletti, P.; Tiribilli, B. Microcantilever: Dynamical Response for Mass Sensing and Fluid Characterization. Sensors 2020, 21, 115. [Google Scholar] [CrossRef]
- Ramanathan, K.; Danielsson, B. Principles and Applications of Thermal Biosensors. Biosens. Bioelectron. 2001, 16, 417–423. [Google Scholar] [CrossRef]
- Chen, Y.-T.; Kolhatkar, A.G.; Zenasni, O.; Xu, S.; Lee, T.R. Biosensing Using Magnetic Particle Detection Techniques. Sensors 2017, 17, 2300. [Google Scholar] [CrossRef]
- Yang, C.-T.; Wu, L.; Bai, P.; Thierry, B. Investigation of Plasmonic Signal Enhancement Based on Long Range Surface Plasmon Resonance with Gold Nanoparticle Tags. J. Mater. Chem. C 2016, 4, 9897–9904. [Google Scholar] [CrossRef]
- Morales-Narváez, E.; Montón, H.; Fomicheva, A.; Merkoçi, A. Signal Enhancement in Antibody Microarrays Using Quantum Dots Nanocrystals: Application to Potential Alzheimer’s Disease Biomarker Screening. Anal. Chem. 2012, 84, 6821–6827. [Google Scholar] [CrossRef]
- Zhu, Z. An Overview of Carbon Nanotubes and Graphene for Biosensing Applications. Nanomicro Lett. 2017, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, P.; Lawrance, R.; Lu, Z.-Y.; Lin, H.-C.; Chan, Y.-H. Recent Progress in Dual/Multi-Modal Detection Modes for Improving Sensitivity and Specificity of Lateral Flow Immunoassays Applied for Point-of-Care Diagnostics. TrAC Trends Anal. Chem. 2024, 177, 117798. [Google Scholar] [CrossRef]
- Forssén, P.; Multia, E.; Samuelsson, J.; Andersson, M.; Aastrup, T.; Altun, S.; Wallinder, D.; Wallbing, L.; Liangsupree, T.; Riekkola, M.-L.; et al. Reliable Strategy for Analysis of Complex Biosensor Data. Anal. Chem. 2018, 90, 5366–5374. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Pandian, V.; Mauk, M.G.; Bau, H.H.; Cherry, S.; Tisi, L.C.; Liu, C. Smartphone-Based Mobile Detection Platform for Molecular Diagnostics and Spatiotemporal Disease Mapping. Anal. Chem. 2018, 90, 4823–4831. [Google Scholar] [CrossRef]
- Kadian, S.; Kumari, P.; Shukla, S.; Narayan, R. Recent Advancements in Machine Learning Enabled Portable and Wearable Biosensors. Talanta Open 2023, 8, 100267. [Google Scholar] [CrossRef]
- Sekhwama, M.; Mpofu, K.; Sivarasu, S.; Mthunzi-Kufa, P. Applications of Microfluidics in Biosensing. Discov. Appl. Sci. 2024, 6, 303. [Google Scholar] [CrossRef]
- Kulkarni, M.B.; Ayachit, N.H.; Aminabhavi, T.M. Biosensors and Microfluidic Biosensors: From Fabrication to Application. Biosensors 2022, 12, 543. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, M.; Jie, Z.; Tao, S. Nucleic Acid Testing of SARS-CoV-2: A Review of Current Methods, Challenges, and Prospects. Front. Microbiol. 2022, 13, 1074289. [Google Scholar] [CrossRef]
- Zhao, Y.; Qiu, J.; Jiang, P.; Wang, M.; Sun, M.; Fan, G.; Yang, N.; Huang, N.; Han, Y.; Han, L.; et al. RNA Extraction-Free Reduced Graphene Oxide-Based RT-LAMP Fluorescence Assay for Highly Sensitive SARS-CoV-2 Detection. Talanta 2024, 277, 126413. [Google Scholar] [CrossRef]
- Teymouri, M.; Mollazadeh, S.; Mortazavi, H.; Naderi Ghale-noie, Z.; Keyvani, V.; Aghababaei, F.; Hamblin, M.R.; Abbaszadeh-Goudarzi, G.; Pourghadamyari, H.; Hashemian, S.M.R.; et al. Recent Advances and Challenges of RT-PCR Tests for the Diagnosis of COVID-19. Pathol. Res. Pract. 2021, 221, 153443. [Google Scholar] [CrossRef]
- Fowler, V.L.; Armson, B.; Gonzales, J.L.; Wise, E.L.; Howson, E.L.A.; Vincent-Mistiaen, Z.; Fouch, S.; Maltby, C.J.; Grippon, S.; Munro, S.; et al. A Highly Effective Reverse-Transcription Loop-Mediated Isothermal Amplification (RT-LAMP) Assay for the Rapid Detection of SARS-CoV-2 Infection. J. Infect. 2021, 82, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, S.; Vázquez-Villegas, P.; Rito-Palomares, M.; Martinez-Chapa, S.O. Advantages, Disadvantages and Modifications of Conventional ELISA. In Enzyme-Linked Immunosorbent Assay (ELISA): From A to Z; Hosseini, S., Vázquez-Villegas, P., Rito-Palomares, M., Martinez-Chapa, S.O., Eds.; Springer: Singapore, 2018; pp. 67–115. [Google Scholar] [CrossRef]
- Heidt, B.; Siqueira, W.F.; Eersels, K.; Diliën, H.; van Grinsven, B.; Fujiwara, R.T.; Cleij, T.J. Point of Care Diagnostics in Resource-Limited Settings: A Review of the Present and Future of PoC in Its Most Needed Environment. Biosensors 2020, 10, 133. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, K.; Melendez, J.H.; Gaydos, C.A.; Wang, T.-H. Bridging the gap between development of point-of-care nucleic acid testing and patient care for sexually transmitted infections. Lab Chip 2022, 22, 476–511. [Google Scholar] [CrossRef] [PubMed]
- Ledgerwood-Lee, M.; Hubenko, A.; Ray, P.; Theriault, Y.; Brickner, H.; Vazquez, L.F.; Schooley, R.; Carlin, A.; Clark, A.; Garretson, A.; et al. A User-Centered Service Model for Accelerating COVID-19 Diagnostic Innovation: The RADx- Rad Dx Core Approach. IEEE Open J. Eng. Med. Biol. 2025, 6, 472–479. [Google Scholar] [CrossRef]
- RADx® Tech|National Institute of Biomedical Imaging and Bioengineering. Available online: https://www.nibib.nih.gov/programs/radx-tech-program (accessed on 18 June 2025).
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.-F.; et al. Infectious Disease in an Era of Global Change. Nat. Rev. Microbiol. 2022, 20, 193–205. [Google Scholar] [CrossRef]
- Meng, E.C.; Goddard, T.D.; Pettersen, E.F.; Couch, G.S.; Pearson, Z.J.; Morris, J.H.; Ferrin, T.E. UCSF ChimeraX: Tools for Structure Building and Analysis. Protein Sci. 2023, 32, e4792. [Google Scholar] [CrossRef]
- Nguyen, H.H.; Park, J.; Kang, S.; Kim, M. Surface Plasmon Resonance: A Versatile Technique for Biosensor Applications. Sensors 2015, 15, 10481–10510. [Google Scholar] [CrossRef]
- Abbas, A.; Linman, M.J.; Cheng, Q. Sensitivity Comparison of Surface Plasmon Resonance and Plasmon-Waveguide Resonance Biosensors. Sens. Actuators B Chem. 2011, 156, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Liu, X.; Shi, S.; Huang, R.; Su, R.; Qi, W.; He, Z. Design and Mechanisms of Antifouling Materials for Surface Plasmon Resonance Sensors. Acta Biomater. 2016, 40, 100–118. [Google Scholar] [CrossRef]
- Riedel, T.; Rodriguez-Emmenegger, C.; de los Santos Pereira, A.; Bědajánková, A.; Jinoch, P.; Boltovets, P.M.; Brynda, E. Diagnosis of Epstein–Barr Virus Infection in Clinical Serum Samples by an SPR Biosensor Assay. Biosens. Bioelectron. 2014, 55, 278–284. [Google Scholar] [CrossRef]
- Florschütz, K.; Schröter, A.; Schmieder, S.; Chen, W.; Schweizer, P.; Sonntag, F.; Danz, N.; Baronian, K.; Kunze, G. ‘Phytochip’: On-Chip Detection of Phytopathogenic RNA Viruses by a New Surface Plasmon Resonance Platform. J. Virol. Methods 2013, 189, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Yano, T.; Kajisa, T.; Ono, M.; Miyasaka, Y.; Hasegawa, Y.; Saito, A.; Otsuka, K.; Sakane, A.; Sasaki, T.; Yasutomo, K.; et al. Ultrasensitive Detection of SARS-CoV-2 Nucleocapsid Protein Using Large Gold Nanoparticle-Enhanced Surface Plasmon Resonance. Sci. Rep. 2022, 12, 1060. [Google Scholar] [CrossRef] [PubMed]
- Tombelli, S.; Minunni, M.; Luzi, E.; Mascini, M. Aptamer-Based Biosensors for the Detection of HIV-1 Tat Protein. Bioelectrochemistry 2005, 67, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Kan, L.; Duan, F.; He, L.; Wang, M.; Cui, J.; Zhang, Z.; Zhang, Z. Surface Plasmon Resonance Aptasensor Based on Niobium Carbide MXene Quantum Dots for Nucleocapsid of SARS-CoV-2 Detection. Microchim. Acta 2021, 188, 316. [Google Scholar] [CrossRef]
- P4SPR 2.0. Affinite Instruments. Available online: https://www.affiniteinstruments.com/p4spr-2-0 (accessed on 22 April 2025).
- Dong, T.; Han, C.; Jiang, M.; Zhang, T.; Kang, Q.; Wang, P.; Zhou, F. A Four-Channel Surface Plasmon Resonance Sensor Functionalized Online for Simultaneous Detections of Anti-SARS-CoV-2 Antibody, Free Viral Particles, and Neutralized Viral Particles. ACS Sens. 2022, 7, 3560–3570. [Google Scholar] [CrossRef]
- Meet OpenSPR|Benchtop SPR Instrument|Nicoya. Available online: https://nicoyalife.com/products/spr-instruments/openspr/ (accessed on 22 April 2025).
- NanoSPR—Devices and Glass Plates for Surface Plasmon Resonance. Available online: https://nanospr.com/ (accessed on 22 April 2025).
- Choudhary, S.; Altintas, Z. Development of a Point-of-Care SPR Sensor for the Diagnosis of Acute Myocardial Infarction. Biosensors 2023, 13, 229. [Google Scholar] [CrossRef]
- Murali, S.; Rustandi, R.R.; Zheng, X.; Payne, A.; Shang, L. Applications of Surface Plasmon Resonance and Biolayer Interferometry for Virus–Ligand Binding. Viruses 2022, 14, 717. [Google Scholar] [CrossRef]
- Jug, A.; Bratkovič, T.; Ilaš, J. Biolayer Interferometry and Its Applications in Drug Discovery and Development. TrAC Trends Anal. Chem. 2024, 176, 117741. [Google Scholar] [CrossRef]
- Guo, Z.; Wilson, J.R.; York, I.A.; Stevens, J. Biosensor-Based Epitope Mapping of Antibodies Targeting the Hemagglutinin and Neuraminidase of Influenza A Virus. J. Immunol. Methods 2018, 461, 23–29. [Google Scholar] [CrossRef]
- Lu, W.; Du, W.; Somovilla, V.J.; Yu, G.; Haksar, D.; de Vries, E.; Boons, G.-J.; de Vries, R.P.; de Haan, C.A.M.; Pieters, R.J. Enhanced Inhibition of Influenza A Virus Adhesion by Di- and Trivalent Hemagglutinin Inhibitors. J. Med. Chem. 2019, 62, 6398–6404. [Google Scholar] [CrossRef]
- Wei, X.; Du, W.; Duca, M.; Yu, G.; de Vries, E.; de Haan, C.A.M.; Pieters, R.J. Preventing Influenza A Virus Infection by Mixed Inhibition of Neuraminidase and Hemagglutinin by Divalent Inhibitors. J. Med. Chem. 2022, 65, 7312–7323. [Google Scholar] [CrossRef] [PubMed]
- Poolsup, S.; Zaripov, E.; Hüttmann, N.; Minic, Z.; Artyushenko, P.V.; Shchugoreva, I.A.; Tomilin, F.N.; Kichkailo, A.S.; Berezovski, M.V. Discovery of DNA Aptamers Targeting SARS-CoV-2 Nucleocapsid Protein and Protein-Binding Epitopes for Label-Free COVID-19 Diagnostics. Mol. Ther. Nucleic Acids 2023, 31, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Dzimianski, J.V.; Lorig-Roach, N.; O’Rourke, S.M.; Alexander, D.L.; Kimmey, J.M.; DuBois, R.M. Rapid and Sensitive Detection of SARS-CoV-2 Antibodies by Biolayer Interferometry. Sci. Rep. 2020, 10, 21738. [Google Scholar] [CrossRef] [PubMed]
- Daaboul, G.G.; Freedman, D.S.; Scherr, S.M.; Carter, E.; Rosca, A.; Bernstein, D.; Mire, C.E.; Agans, K.N.; Hoenen, T.; Geisbert, T.W.; et al. Enhanced Light Microscopy Visualization of Virus Particles from Zika Virus to Filamentous Ebolaviruses. PLoS ONE 2017, 12, e0179728. [Google Scholar] [CrossRef]
- Daaboul, G.G.; Lopez, C.A.; Chinnala, J.; Goldberg, B.B.; Connor, J.H.; Ünlü, M.S. Digital Sensing and Sizing of Vesicular Stomatitis Virus Pseudotypes in Complex Media: A Model for Ebola and Marburg Detection. ACS Nano 2014, 8, 6047–6055. [Google Scholar] [CrossRef]
- Daaboul, G.G.; Yurt, A.; Zhang, X.; Hwang, G.M.; Goldberg, B.B.; Ünlü, M.S. High-Throughput Detection and Sizing of Individual Low-Index Nanoparticles and Viruses for Pathogen Identification. Nano Lett. 2010, 10, 4727–4731. [Google Scholar] [CrossRef]
- Aslan, M.; Seymour, E.; Brickner, H.; Clark, A.E.; Celebi, I.; Townsend, M.B.; Satheshkumar, P.S.; Riley, M.; Carlin, A.F.; Ünlü, M.S.; et al. A Label-Free Optical Biosensor-Based Point-of-Care Test for the Rapid Detection of Monkeypox Virus. Biosens. Bioelectron. 2025, 269, 116932. [Google Scholar] [CrossRef]
- Wang, X.; Shang, X.; Huang, X. Next-Generation Pathogen Diagnosis with CRISPR/Cas-Based Detection Methods. Emerg. Microbes Infect. 2020, 9, 1682–1691. [Google Scholar] [CrossRef]
- Kaminski, M.M.; Abudayyeh, O.O.; Gootenberg, J.S.; Zhang, F.; Collins, J.J. CRISPR-Based Diagnostics. Nat. Biomed. Eng. 2021, 5, 643–656. [Google Scholar] [CrossRef]
- Wang, X.; Xiong, E.; Tian, T.; Cheng, M.; Lin, W.; Wang, H.; Zhang, G.; Sun, J.; Zhou, X. Clustered Regularly Interspaced Short Palindromic Repeats/Cas9-Mediated Lateral Flow Nucleic Acid Assay. ACS Nano 2020, 14, 2497–2508. [Google Scholar] [CrossRef]
- Weerathunge, P.; Ramanathan, R.; Torok, V.A.; Hodgson, K.; Xu, Y.; Goodacre, R.; Behera, B.K.; Bansal, V. Ultrasensitive Colorimetric Detection of Murine Norovirus Using NanoZyme Aptasensor. Anal. Chem. 2019, 91, 3270–3276. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Gupta, P.; Wang, S.; Melnykov, A.; Jiang, Q.; Seth, A.; Wang, Z.; Morrissey, J.J.; George, I.; Gandra, S.; et al. Ultrasensitive Lateral-Flow Assays via Plasmonically Active Antibody-Conjugated Fluorescent Nanoparticles. Nat. Biomed. Eng. 2023, 7, 1556–1570. [Google Scholar] [CrossRef] [PubMed]
- Gugliandolo, G.; Pilato, G.; Donato, N. Compact System for Colorimetric Sensor Arrays Characterization Based on Computer Screen Photo-Assisted Technology. Electronics 2021, 10, 2587. [Google Scholar] [CrossRef]
- Kim, H.; Jang, H.; Song, J.; Lee, S.M.; Lee, S.; Kwon, H.-J.; Kim, S.; Kang, T.; Park, H.G. A CRISPR/Cas12 Trans-Cleavage Reporter Enabling Label-Free Colorimetric Detection of SARS-CoV-2 and Its Variants. Biosens. Bioelectron. 2024, 251, 116102. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Tellez, J.; Ramirez-Montes, S.; Ferreira, T.A.; Santos, E.M.; Rodriguez, J.A. Application of Voltammetric Sensors for Pathogen Bacteria Detection: A Review. Chemosensors 2022, 10, 424. [Google Scholar] [CrossRef]
- Hammond, J.L.; Formisano, N.; Estrela, P.; Carrara, S.; Tkac, J. Electrochemical Biosensors and Nanobiosensors. Essays Biochem. 2016, 60, 69–80. [Google Scholar] [CrossRef]
- Jarosińska, E.; Zambrowska, Z.; Witkowska Nery, E. Methods of Protection of Electrochemical Sensors against Biofouling in Cell Culture Applications. ACS Omega 2024, 9, 4572–4580. [Google Scholar] [CrossRef]
- Zamani, M.; Robson, J.M.; Fan, A.; Bono, M.S., Jr.; Furst, A.L.; Klapperich, C.M. Electrochemical Strategy for Low-Cost Viral Detection. ACS Cent. Sci. 2021, 7, 963–972. [Google Scholar] [CrossRef]
- Huang, K.-J.; Li, J.; Liu, Y.-M.; Cao, X.; Yu, S.; Yu, M. Disposable Immunoassay for Hepatitis B Surface Antigen Based on a Graphene Paste Electrode Functionalized with Gold Nanoparticles and a Nafion-Cysteine Conjugate. Microchim. Acta 2012, 177, 419–426. [Google Scholar] [CrossRef]
- Salahandish, R.; Jalali, P.; Tabrizi, H.O.; Hyun, J.E.; Haghayegh, F.; Khalghollah, M.; Zare, A.; Berenger, B.M.; Niu, Y.D.; Ghafar-Zadeh, E.; et al. A Compact, Low-Cost, and Binary Sensing (BiSense) Platform for Noise-Free and Self-Validated Impedimetric Detection of COVID-19 Infected Patients. Biosens. Bioelectron. 2022, 213, 114459. [Google Scholar] [CrossRef]
- de Lima, L.F.; Ferreira, A.L.; Ranjan, I.; Collman, R.G.; de Araujo, W.R.; de la Fuente-Nunez, C. A Bacterial Cellulose-Based and Low-Cost Electrochemical Biosensor for Ultrasensitive Detection of SARS-CoV-2. Cell Rep. Phys. Sci. 2023, 4, 101476. [Google Scholar] [CrossRef] [PubMed]
- Szydlowska, B.M.; Pola, C.C.; Cai, Z.; Chaney, L.E.; Hui, J.; Sheets, R.; Carpenter, J.; Dean, D.; Claussen, J.C.; Gomes, C.L.; et al. Biolayer-Interferometry-Guided Functionalization of Screen-Printed Graphene for Label-Free Electrochemical Virus Detection. ACS Appl. Mater. Interfaces 2024, 16, 25169–25180. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Liu, F.; Xie, W.; Zhou, T.-C.; OuYang, J.; Jin, L.; Li, H.; Zhao, C.-Y.; Zhang, L.; Wei, J.; et al. Ultrasensitive Supersandwich-Type Electrochemical Sensor for SARS-CoV-2 from the Infected COVID-19 Patients Using a Smartphone. Sens. Actuators B Chem. 2021, 327, 128899. [Google Scholar] [CrossRef]
- Torrente-Rodríguez, R.M.; Lukas, H.; Tu, J.; Min, J.; Yang, Y.; Xu, C.; Rossiter, H.B.; Gao, W. SARS-CoV-2 RapidPlex: A Graphene-Based Multiplexed Telemedicine Platform for Rapid and Low-Cost COVID-19 Diagnosis and Monitoring. Matter 2020, 3, 1981–1998. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.J.; Han, M.; Desroches, P.E.; Manasa, C.S.; Dennaoui, J.; Quigley, A.F.; Kapsa, R.M.I.; Moulton, S.E.; Guijt, R.M.; Greene, G.W.; et al. Antifouling Strategies for Electrochemical Biosensing: Mechanisms and Performance toward Point of Care Based Diagnostic Applications. ACS Sens. 2021, 6, 1482–1507. [Google Scholar] [CrossRef]
- Kamsong, W.; Primpray, V.; Pasakon, P.; Sriprachuabwong, C.; Pakapongpan, S.; Mensing, J.P.; Wisitsoraat, A.; Tuantranont, A.; Karuwan, C. Highly Sensitive and Disposable Screen-Printed Ionic Liquid/Graphene Based Electrochemical Sensors. Electrochem. Commun. 2022, 135, 107209. [Google Scholar] [CrossRef]
- Dixon, M.C. Quartz Crystal Microbalance with Dissipation Monitoring: Enabling Real-Time Characterization of Biological Materials and Their Interactions. J. Biomol. Tech. 2008, 19, 151–158. [Google Scholar]
- Uttenthaler, E.; Kößlinger, C.; Drost, S. Quartz Crystal Biosensor for Detection of the African Swine Fever Disease. Anal. Chim. Acta 1998, 362, 91–100. [Google Scholar] [CrossRef]
- Nilsson, P.H.; Al-Majdoub, M.; Ibrahim, A.; Aseel, O.; Suriyanarayanan, S.; Andersson, L.; Fostock, S.; Aastrup, T.; Tjernberg, I.; Rydén, I.; et al. Quartz Crystal Microbalance Platform for SARS-CoV-2 Immuno-Diagnostics. Int. J. Mol. Sci. 2023, 24, 16705. [Google Scholar] [CrossRef]
- Ly, T.N.; Park, S.; Park, S.J. Detection of HIV-1 Antigen by Quartz Crystal Microbalance Using Gold Nanoparticles. Sens. Actuators B Chem. 2016, 237, 452–458. [Google Scholar] [CrossRef]
- Makaraviciute, A.; Ruzgas, T.; Ramanavicius, A.; Ramanaviciene, A. A QCM-D Study of Reduced Antibody Fragments Immobilized on Planar Gold and Gold Nanoparticle Modified Sensor Surfaces. Key Eng. Mater. 2014, 605, 340–343. [Google Scholar] [CrossRef]
- Owen, T.W.; Al-Kaysi, R.O.; Bardeen, C.J.; Cheng, Q. Microgravimetric Immunosensor for Direct Detection of Aerosolized Influenza A Virus Particles. Sens. Actuators B Chem. 2007, 126, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Jenik, M.; Schirhagl, R.; Schirk, C.; Hayden, O.; Lieberzeit, P.; Blaas, D.; Paul, G.; Dickert, F.L. Sensing Picornaviruses Using Molecular Imprinting Techniques on a Quartz Crystal Microbalance. Anal. Chem. 2009, 81, 5320–5326. [Google Scholar] [CrossRef]
- Tai, D.-F.; Lin, C.-Y.; Wu, T.-Z.; Chen, L.-K. Recognition of Dengue Virus Protein Using Epitope-Mediated Molecularly Imprinted Film. Anal. Chem. 2005, 77, 5140–5143. [Google Scholar] [CrossRef]
- Shen, H.; Zhou, T.; Hu, J. A High-Throughput QCM Chip Configuration for the Study of Living Cells and Cell-Drug Interactions. Anal. Bioanal. Chem. 2017, 409, 6463–6473. [Google Scholar] [CrossRef]
- Liu, Y.; Zhan, L.; Qin, Z.; Sackrison, J.; Bischof, J.C. Ultrasensitive and Highly Specific Lateral Flow Assays for Point-of-Care Diagnosis. ACS Nano 2021, 15, 3593–3611. [Google Scholar] [CrossRef]
- Bukasov, R.; Dossym, D.; Filchakova, O. Detection of RNA Viruses from Influenza and HIV to Ebola and SARS-CoV-2: A Review. Anal. Methods 2021, 13, 34–55. [Google Scholar] [CrossRef]
- Iqbal, B.N.; Arunasalam, S.; Divarathna, M.V.M.; Jabeer, A.; Sirisena, P.; Senaratne, T.; Muthugala, R.; Noordeen, F. Diagnostic Utility and Validation of a Newly Developed Real Time Loop Mediated Isothermal Amplification Method for the Detection of SARS CoV-2 Infection. J. Clin. Virol. Plus 2022, 2, 100081. [Google Scholar] [CrossRef]
- Hoffmann, E.d.R.; Balzan, L.d.R.; Inamine, E.; Pancotto, L.R.; Gaboardi, G.; Cantarelli, V.V. Performance of Reverse Transcription Loop-Mediated Isothermal Amplification (RT-LAMP) Targeting the RNA Polymerase Gene for the Direct Detection of SARS-CoV2 in Nasopharyngeal Swabs. Int. J. Mol. Sci. 2023, 24, 13056. [Google Scholar] [CrossRef]
- Kuang, Y.; Tan, W.; Hu, C.; Dai, Z.; Bai, L.; Wang, J.; Liao, H.; Chen, H.; He, R.; Zhu, P.; et al. Diagnosis Value of Targeted and Metagenomic Sequencing in Respiratory Tract Infection. Front. Cell. Infect. Microbiol. 2024, 14, 1498512. [Google Scholar] [CrossRef]
- SPR Instruments. Available online: https://www.sprpages.nl/spr-instruments (accessed on 18 June 2025).
- Aziz, A.; Asif, M.; Ashraf, G.; Farooq, U.; Yang, Q.; Wang, S. Trends in Biosensing Platforms for SARS-CoV-2 Detection: A Critical Appraisal against Standard Detection Tools. Curr. Opin. Colloid. Interface Sci. 2021, 52, 101418. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.L.; Scott, I.M.; McMurry, J.L. Optical Biosensing: Kinetics of Protein A-IGG Binding Using Biolayer Interferometry. Biochem. Mol. Biol. Educ. 2010, 38, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Afzal, A.; Mujahid, A.; Schirhagl, R.; Bajwa, S.Z.; Latif, U.; Feroz, S. Gravimetric Viral Diagnostics: QCM Based Biosensors for Early Detection of Viruses. Chemosensors 2017, 5, 7. [Google Scholar] [CrossRef]
- Su, R.; Wang, F.; McAlpine, M.C. 3D Printed Microfluidics: Advances in Strategies, Integration, and Applications. Lab Chip 2023, 23, 1279–1299. [Google Scholar] [CrossRef]
- Three-Dimensional Direct Laser Writing of PEGda Hydrogel Microstructures with Low Threshold Power Using a Green Laser Beam. Available online: https://www.light-am.com/en/article/doi/10.37188/lam.2021.003 (accessed on 22 April 2025).
- Jin, Y.; Xiong, P.; Xu, T.; Wang, J. Time-Efficient Fabrication Method for 3D-Printed Microfluidic Devices. Sci. Rep. 2022, 12, 1233. [Google Scholar] [CrossRef]
- Guttridge, C.; Shannon, A.; O’Sullivan, A.; O’Sullivan, K.J.; O’Sullivan, L.W. Biocompatible 3D Printing Resins for Medical Applications: A Review of Marketed Intended Use, Biocompatibility Certification, and Post-Processing Guidance. Ann. 3D Print. Med. 2022, 5, 100044. [Google Scholar] [CrossRef]
- Poskus, M.D.; Wang, T.; Deng, Y.; Borcherding, S.; Atkinson, J.; Zervantonakis, I.K. Fabrication of 3D-Printed Molds for Polydimethylsiloxane-Based Microfluidic Devices Using a Liquid Crystal Display-Based Vat Photopolymerization Process: Printing Quality, Drug Response and 3D Invasion Cell Culture Assays. Microsyst. Nanoeng. 2023, 9, 140. [Google Scholar] [CrossRef]
- Vaidya, N.; Solgaard, O. 3D Printed Optics with Nanometer Scale Surface Roughness. Microsyst. Nanoeng. 2018, 4, 18. [Google Scholar] [CrossRef]
- Shanmugam, A.; Usmani, M.; Mayberry, A.; Perkins, D.L.; Holcomb, D.E. Imaging Systems and Algorithms to Analyze Biological Samples in Real-Time Using Mobile Phone Microscopy. PLoS ONE 2018, 13, e0193797. [Google Scholar] [CrossRef]
- Ali, M.A.; Zhang, G.F.; Hu, C.; Yuan, B.; Jahan, S.; Kitsios, G.D.; Morris, A.; Gao, S.-J.; Panat, R. Ultrarapid and Ultrasensitive Detection of SARS-CoV-2 Antibodies in COVID-19 Patients via a 3D-printed Nanomaterial-based Biosensing Platform. J. Med. Virol. 2022, 94, 5808–5826. [Google Scholar] [CrossRef]
- Sharma, P.; Hasan Mohd, R.; Yardim, A.; Celik, E.G.; Timur, S.; Abdin, M.Z.; Narang, J. Next-Generation Point-of-Care Diagnostics: Silver Nanoparticle-Enhanced 3D-Printed Multiplex Electrochemical Biosensor for Detecting Dengue and Chikungunya Viruses. ACS Appl. Bio Mater. 2025, 8, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Krejcova, L.; Nejdl, L.; Rodrigo, M.A.M.; Zurek, M.; Matousek, M.; Hynek, D.; Zitka, O.; Kopel, P.; Adam, V.; Kizek, R. 3D Printed Chip for Electrochemical Detection of Influenza Virus Labeled with CdS Quantum Dots. Biosens. Bioelectron. 2014, 54, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Karamzadeh, V.; Sohrabi-Kashani, A.; Shen, M.; Juncker, D. Digital Manufacturing of Functional Ready-to-Use Microfluidic Systems. Adv. Mater. 2023, 35, 2303867. [Google Scholar] [CrossRef] [PubMed]
- Armijo, P.R.; Markin, N.W.; Nguyen, S.; Ho, D.H.; Horseman, T.S.; Lisco, S.J.; Schiller, A.M. 3D Printing of Face Shields to Meet the Immediate Need for PPE in an Anesthesiology Department during the COVID-19 Pandemic. Am. J. Infect. Control 2021, 49, 302–308. [Google Scholar] [CrossRef]
- Prototyping Rapid Diagnostics for COVID-19 with 3D Printing. Formlabs. Available online: https://formlabs.com/covid-19-response/covid-19-rapid-diagnostics/?srsltid=AfmBOoq2JMJEfdWqop-UvUqu4hrgqFwz8Ngiu-GrmlGGl162dFemATCz (accessed on 22 April 2025).
- Ford, J.; Goldstein, T.; Trahan, S.; Neuwirth, A.; Tatoris, K.; Decker, S. A 3D-Printed Nasopharyngeal Swab for COVID-19 Diagnostic Testing. 3D Print. Med. 2020, 6, 21. [Google Scholar] [CrossRef]
- Goswami, M.; Yadav, A.K.; Chauhan, V.; Singh, N.; Kumar, S.; Das, A.; Yadav, V.; Mandal, A.; Tiwari, J.K.; Siddiqui, H.; et al. Facile Development of Graphene-Based Air Filters Mounted on a 3D Printed Mask for COVID-19. J. Sci. Adv. Mater. Devices 2021, 6, 407–414. [Google Scholar] [CrossRef]
- Naz, S.A.; Huynh, V.T.; Doeven, E.H.; Adams, S.; Kouzani, A.; Guijt, R.M. Closed-Loop Control Systems for Pumps Used in Portable Analytical Systems. J. Chromatogr. A 2023, 1695, 463931. [Google Scholar] [CrossRef]
- Moya Muñoz, G.G.; Brix, O.; Klocke, P.; Harris, P.D.; Luna Piedra, J.R.; Wendler, N.D.; Lerner, E.; Zijlstra, N.; Cordes, T. Single-Molecule Detection and Super-Resolution Imaging with a Portable and Adaptable 3D-Printed Microscopy Platform (Brick-MIC). Sci. Adv. 2024, 10, eado3427. [Google Scholar] [CrossRef]
- Mendoza-Gallegos, R.A.; Rios, A.; Garcia-Cordero, J.L. An Affordable and Portable Thermocycler for Real-Time PCR Made of 3D-Printed Parts and Off-the-Shelf Electronics. Anal. Chem. 2018, 90, 5563–5568. [Google Scholar] [CrossRef]
- Sheu, S.C.; Kijamnajsuk, P.; Chan, C.K.; Chen, J.J. A 3D-Printed Oscillatory Polymerase Chain Reaction System Using a Single Heater. Appl. Therm. Eng. 2024, 239, 122201. [Google Scholar] [CrossRef]
- Torres Fredes, I.P.; Cortés-Adasme, E.N.; Barrientos, B.A.; Real, J.P.; Gomez, C.G.; Palma, S.D.; Kogan, M.J.; Real, D.A. 3D-Printed Plasmonic Nanocomposites: VAT Photopolymerization for Photothermal-Controlled Drug Release. Pharmaceuticals 2024, 17, 1453. [Google Scholar] [CrossRef] [PubMed]
- Horst, R.J.; Katzourakis, A.; Mei, B.T.; de Beer, S. Design and Validation of a Low-Cost Open-Source Impedance Based Quartz Crystal Microbalance for Electrochemical Research. HardwareX 2022, 12, e00374. [Google Scholar] [CrossRef] [PubMed]
- Glasco, D.L.; Elhassan, M.M.; McLeod, W.T.; Bell, J.G. Nonenzymatic Detection of Glucose Using 3D Printed Carbon Electrodes in Human Saliva. ECS Sens. Plus 2024, 3, 020602. [Google Scholar] [CrossRef]
- Lee, J.W.; Sim, S.J.; Cho, S.M.; Lee, J. Characterization of a Self-Assembled Monolayer of Thiol on a Gold Surface and the Fabrication of a Biosensor Chip Based on Surface Plasmon Resonance for Detecting Anti-GAD Antibody. Biosens. Bioelectron. 2005, 20, 1422–1427. [Google Scholar] [CrossRef]
- Nakamoto, K.; Kurita, R.; Niwa, O.; Fujii, T.; Nishida, M. Development of a Mass-Producible on-Chip Plasmonic Nanohole Array Biosensor. Nanoscale 2011, 3, 5067–5075. [Google Scholar] [CrossRef]
- Wang, Z.; Wilkop, T.; Han, J.H.; Dong, Y.; Linman, M.J.; Cheng, Q. Development of Air-Stable, Supported Membrane Arrays with Photolithography for Study of Phosphoinositide−Protein Interactions Using Surface Plasmon Resonance Imaging. Anal. Chem. 2008, 80, 6397–6404. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X. Microfluidics-Based Plasmonic Biosensing System Based on Patterned Plasmonic Nanostructure Arrays. Micromachines 2021, 12, 826. [Google Scholar] [CrossRef]
- Sun, S.; Zhao, Y.; Hao, Y.; Xue, P.; Guo, X.; Zhang, W.; Zhang, C.; Zhang, Q.; Zhou, W.; Ong, H.C.; et al. Rapid, Sensitive and Multiplexed Detection of SARS-CoV-2 Viral Nucleic Acids Enabled by Phase-Based Surface Plasmon Resonance of Metallic Gratings. Biomed. Opt. Express 2024, 15, 5215–5226. [Google Scholar] [CrossRef]
- Pardee, K.; Green, A.A.; Takahashi, M.K.; Braff, D.; Lambert, G.; Lee, J.W.; Ferrante, T.; Ma, D.; Donghia, N.; Fan, M.; et al. Rapid, Low-Cost Detection of Zika Virus Using Programmable Biomolecular Components. Cell 2016, 165, 1255–1266. [Google Scholar] [CrossRef]
- Crapnell, R.D.; Banks, C.E. Electroanalytical Overview: Screen-Printed Electrochemical Sensing Platforms. ChemElectroChem 2024, 11, e202400370. [Google Scholar] [CrossRef]
- Inam, A.K.M.S.; Costa Angeli, M.A.; Shkodra, B.; Douaki, A.; Avancini, E.; Magagnin, L.; Petti, L.; Lugli, P. Flexible Screen-Printed Electrochemical Sensors Functionalized with Electrodeposited Copper for Nitrate Detection in Water. ACS Omega 2021, 6, 33523–33532. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Cao, J.; Ding, H.; Liu, C.; Neilson, J.; Li, Z.; Kinloch, I.A.; Derby, B. Screen-Printing of a Highly Conductive Graphene Ink for Flexible Printed Electronics. ACS Appl. Mater. Interfaces 2019, 11, 32225–32234. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Kim, K.-W.; Kwon, J.H.; Kim, J.K.; Kim, S.H.; Moon, H.C. Direct Ink Writing of PEDOT:PSS Inks for Flexible Micro-Supercapacitors. J. Ind. Eng. Chem. 2023, 123, 272–277. [Google Scholar] [CrossRef]
- Fernandes, I.J.; Aroche, A.F.; Schuck, A.; Lamberty, P.; Peter, C.R.; Hasenkamp, W.; Rocha, T.L.A.C. Silver Nanoparticle Conductive Inks: Synthesis, Characterization, and Fabrication of Inkjet-Printed Flexible Electrodes. Sci. Rep. 2020, 10, 8878. [Google Scholar] [CrossRef]
- Sher, M.; Faheem, A.; Asghar, W.; Cinti, S. Nano-Engineered Screen-Printed Electrodes: A Dynamic Tool for Detection of Viruses. TrAC Trends Anal. Chem. 2021, 143, 116374. [Google Scholar] [CrossRef]
- Sestaioni, D.; Giurlani, W.; Ciacci, G.; Camagni, V.; Palladino, P.; Barucci, A.; Scarano, S. Sustainable and Effective Reconditioning of SPR Gold Chips Functionalized with Molecularly Imprinted Polynorepinephrine. Anal. Chim. Acta 2024, 1321, 343037. [Google Scholar] [CrossRef]
- Kimple, A.J.; Muller, R.E.; Siderovski, D.P.; Willard, F.S. A Capture Coupling Method for the Covalent Immobilization of Hexahistidine Tagged Proteins for Surface Plasmon Resonance. Methods Mol. Biol. 2010, 627, 91–100. [Google Scholar] [CrossRef]
- Auer, S.; Azizi, L.; Faschinger, F.; Blazevic, V.; Vesikari, T.; Gruber, H.J.; Hytönen, V.P. Stable Immobilisation of His-Tagged Proteins on BLI Biosensor Surface Using Cobalt. Sens. Actuators B Chem. 2017, 243, 104–113. [Google Scholar] [CrossRef]
- Mantena, S.; Pillai, P.P.; Petros, B.A.; Welch, N.L.; Myhrvold, C.; Sabeti, P.C.; Metsky, H.C. Model-Directed Generation of Artificial CRISPR–Cas13a Guide RNA Sequences Improves Nucleic Acid Detection. Nat. Biotechnol. 2024, 1–8. [Google Scholar] [CrossRef]
- Khan, S.; Singh, Y.V.; Singh, P.; Singh, R.S. An Optimized Artificial Intelligence System Using IoT Biosensors Networking for Healthcare Problems. Comput. Intell. Neurosci. 2022, 2022, 2206573. [Google Scholar] [CrossRef]
- Padhi, A.; Agarwal, A.; Saxena, S.K.; Katoch, C.D.S. Transforming Clinical Virology with AI, Machine Learning and Deep Learning: A Comprehensive Review and Outlook. Virusdisease 2023, 34, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, J.; Mohebbi, M.H.; Patel, R.S.; Brammer, L.; Smolinski, M.S.; Brilliant, L. Detecting Influenza Epidemics Using Search Engine Query Data. Nature 2009, 457, 1012–1014. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Sheng, D.; Zhou, Z.; Wu, Y. AI Hallucination: Towards a Comprehensive Classification of Distorted Information in Artificial Intelligence-Generated Content. Humanit. Soc. Sci. Commun. 2024, 11, 1278. [Google Scholar] [CrossRef]
- Zens, M.; Brammertz, A.; Herpich, J.; Südkamp, N.; Hinterseer, M. App-Based Tracking of Self-Reported COVID-19 Symptoms: Analysis of Questionnaire Data. J. Med. Internet Res. 2020, 22, e21956. [Google Scholar] [CrossRef]
- Çelik Ertuğrul, D.; Çelik Ulusoy, D. A Knowledge-Based Self-Pre-Diagnosis System to Predict Covid-19 in Smartphone Users Using Personal Data and Observed Symptoms. Expert. Syst. 2022, 39, e12716. [Google Scholar] [CrossRef]
- Aborode, A.T.; Adesola, R.O.; Scott, G.Y.; Arthur-Hayford, E.; Otorkpa, O.J.; Kwaku, S.D.; Elebesunu, E.E.; Nibokun, E.O.; Aruorivwooghene, I.J.; Bakre, A.A.; et al. Bringing Lab to the Field: Exploring Innovations in Point-of-Care Diagnostics for the Rapid Detection and Management of Tropical Diseases in Resource-Limited Settings. Adv. Biomark. Sci. Technol. 2025, 7, 28–43. [Google Scholar] [CrossRef]
- Chen, H.-C. A Systematic Review of the Barcoding Strategy That Contributes to COVID-19 Diagnostics at a Population Level. Front. Mol. Biosci. 2023, 10, 1141534. [Google Scholar] [CrossRef]
- Farrell, L. Automated Digital Notification of COVID-19 Diagnoses Through Text and Email Messaging—North Carolina, December 2020–January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1603–1607. [Google Scholar] [CrossRef]
- Ding, X.; Yin, K.; Li, Z.; Lalla, R.V.; Ballesteros, E.; Sfeir, M.M.; Liu, C. Ultrasensitive and Visual Detection of SARS-CoV-2 Using All-in-One Dual CRISPR-Cas12a Assay. Nat. Commun. 2020, 11, 4711. [Google Scholar] [CrossRef]
- Martín-Sierra, C.; Chavez, M.T.; Escobedo, P.; García-Cabrera, V.; López-Delgado, F.J.; Guardia-Monteagudo, J.J.; Ruiz-García, I.; Erenas, M.M.; Sanchez-Martin, R.M.; Capitán-Vallvey, L.F.; et al. SARS-CoV-2 Viral RNA Detection Using the Novel CoVradar Device Associated with the CoVreader Smartphone App. Biosens. Bioelectron. 2023, 230, 115268. [Google Scholar] [CrossRef]
- Wu, K.; Chugh, V.K.; Girolamo, A.d.; Liu, J.; Saha, R.; Su, D.; Krishna, V.D.; Nair, A.; Davies, W.; Wang, A.Y.; et al. Portable Magnetic Particle Spectrometer (MPS) for Future Rapid and Wash-Free Bioassays. ACS Appl. Mater. Interfaces 2021, 13, 7966–7976. [Google Scholar] [CrossRef] [PubMed]
- Pennisi, I.; Cavuto, M.L.; Miglietta, L.; Malpartida-Cardenas, K.; Stringer, O.W.; Mantikas, K.-T.; Reid, R.; Frise, R.; Moser, N.; Randell, P.; et al. Rapid, Portable, and Electricity-Free Sample Extraction Method for Enhanced Molecular Diagnostics in Resource-Limited Settings. Anal. Chem. 2024, 96, 11181–11188. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Sha, Z.; Huang, S.; Yin, C.; Wan, L.; Li, J.; Ling, J.; Wu, C.; Dai, L. An Open Source, PCR Based, Point-of-Care Testing Platform. Sci. Rep. 2025, 15, 12025. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Mandujano, G.; Grünberg, R.; Zhang, Y.; Bi, C.; Guzmán-Vega, F.J.; Shuaib, M.; Gorchakov, R.V.; Xu, J.; Tehseen, M.; Takahashi, M.; et al. An Open-Source, Automated, and Cost-Effective Platform for COVID-19 Diagnosis and Rapid Portable Genomic Surveillance Using Nanopore Sequencing. Sci. Rep. 2023, 13, 20349. [Google Scholar] [CrossRef]
- Moukarzel, G.; Wang, Y.; Xin, W.; Hofmann, C.; Joshi, A.; Loughney, J.W.; Bowman, A. Automation of Biochemical Assays Using an Open-Sourced, Inexpensive Robotic Liquid Handler. SLAS Technol. 2024, 29, 100205. [Google Scholar] [CrossRef]
- 3D Printing: Overview, Impacts, and the Federal Role. Available online: https://www.congress.gov/crs-product/R45852 (accessed on 18 June 2025).
- Peters, H.P. Gap between Science and Media Revisited: Scientists as Public Communicators. Proc. Natl. Acad. Sci. USA 2013, 110 (Suppl. 3), 14102–14109. [Google Scholar] [CrossRef]
- Dankel, M.; Lambert, M. Abstracts for a Wider Audience: Promoting Linguistic Diversity in JBI Evidence Synthesis. JBI Evid. Synth. 2023, 21, 833. [Google Scholar] [CrossRef]
- How to Make Your Research Accessible. Author Services. Available online: https://authorservices.taylorandfrancis.com/publishing-your-research/writing-your-paper/how-to-make-your-research-accessible/ (accessed on 23 April 2025).
- Stack Whitney, K.; Perrone, J.; Bahlai, C.A. Open Access Journals Lack Image Accessibility Guidelines. Quant. Sci. Stud. 2025, 6, 46–62. [Google Scholar] [CrossRef]
- Shailes, S. Plain-Language Summaries of Research: Something for Everyone. eLife 2017, 6, e25411. [Google Scholar] [CrossRef]
- Sedgwick, C.; Belmonte, L.; Margolis, A.; Shafer, P.O.; Pitterle, J.; Gidal, B.E. Extending the Reach of Science—Talk in Plain Language. Epilepsy Behav. Rep. 2021, 16, 100493. [Google Scholar] [CrossRef]
- Viruses: Instructions for Authors. Available online: https://www.mdpi.com/journal/viruses/instructions (accessed on 23 April 2025).
- Highlights of Journal Articles|Elsevier. Available online: https://www.elsevier.com/researcher/author/tools-and-resources/highlights (accessed on 23 April 2025).
- Bredbenner, K.; Simon, S.M. Video Abstracts and Plain Language Summaries Are More Effective than Graphical Abstracts and Published Abstracts. PLoS ONE 2019, 14, e0224697. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Method | Sensitivity | Cost | Complexity | Portability | Clinical/POC Applicability | References |
|---|---|---|---|---|---|---|
| Lateral Flow Assay | + | ++++ | ++++ | ++++ | ++++ | [92,93] |
| RT-PCR | +++ | + | + | + | ++++ | [92,93] |
| ELISA | ++ | ++ | ++ | + | ++++ | [92,93] |
| RT-LAMP | ++ | +++ | +++ | +++ | +++ | [93,94,95] |
| NGS | ++++ | + | + | + | +++ | [96] |
| Plasmonic/SPR | ++++ | + | + | + | ++ | [97,98] |
| BLI | +++ | ++ | + | + | ++ | [59,99] |
| QCM | ++ | ++ | ++ | +++ | + | [100] |
| Electrochemical | ++ | ++ | ++ | +++ | ++ | [74,77,98] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Zant, W.; Ray, P. Democratization of Point-of-Care Viral Biosensors: Bridging the Gap from Academia to the Clinic. Biosensors 2025, 15, 436. https://doi.org/10.3390/bios15070436
Van Zant W, Ray P. Democratization of Point-of-Care Viral Biosensors: Bridging the Gap from Academia to the Clinic. Biosensors. 2025; 15(7):436. https://doi.org/10.3390/bios15070436
Chicago/Turabian StyleVan Zant, Westley, and Partha Ray. 2025. "Democratization of Point-of-Care Viral Biosensors: Bridging the Gap from Academia to the Clinic" Biosensors 15, no. 7: 436. https://doi.org/10.3390/bios15070436
APA StyleVan Zant, W., & Ray, P. (2025). Democratization of Point-of-Care Viral Biosensors: Bridging the Gap from Academia to the Clinic. Biosensors, 15(7), 436. https://doi.org/10.3390/bios15070436