
Respect for Religiosity: Review of Faith Integration in Health and Wellbeing Interventions with Muslim Minorities


Abstract
:1. Introduction
2. Methods
What are the characteristics of mosque- and/or Muslim faith-based community welfare interventions in countries with Muslim minority populations?
2.1. Eligibility Criteria
2.2. Search Strategy
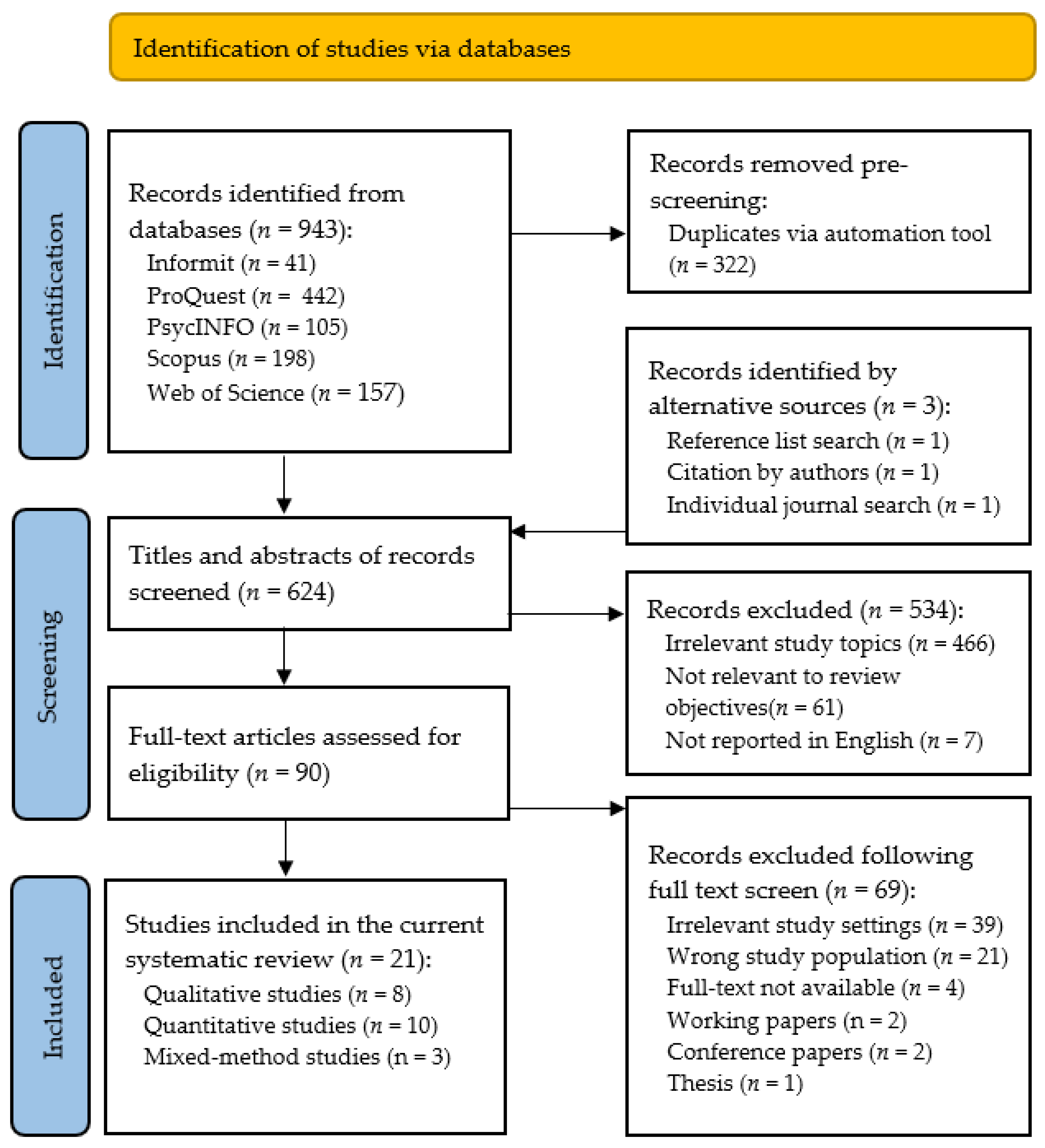
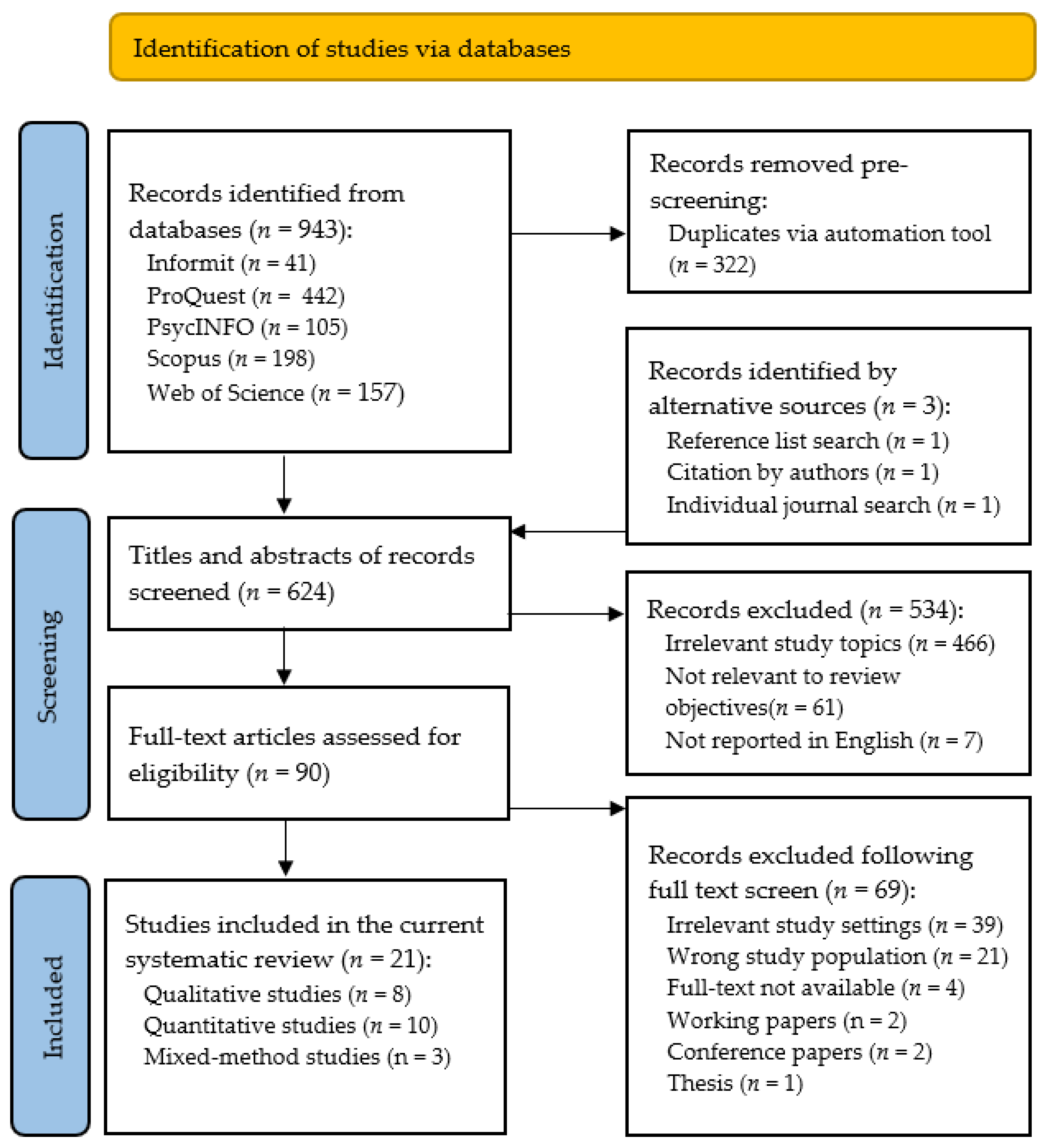
2.3. Study Selection
2.4. Risk of Bias Assessment
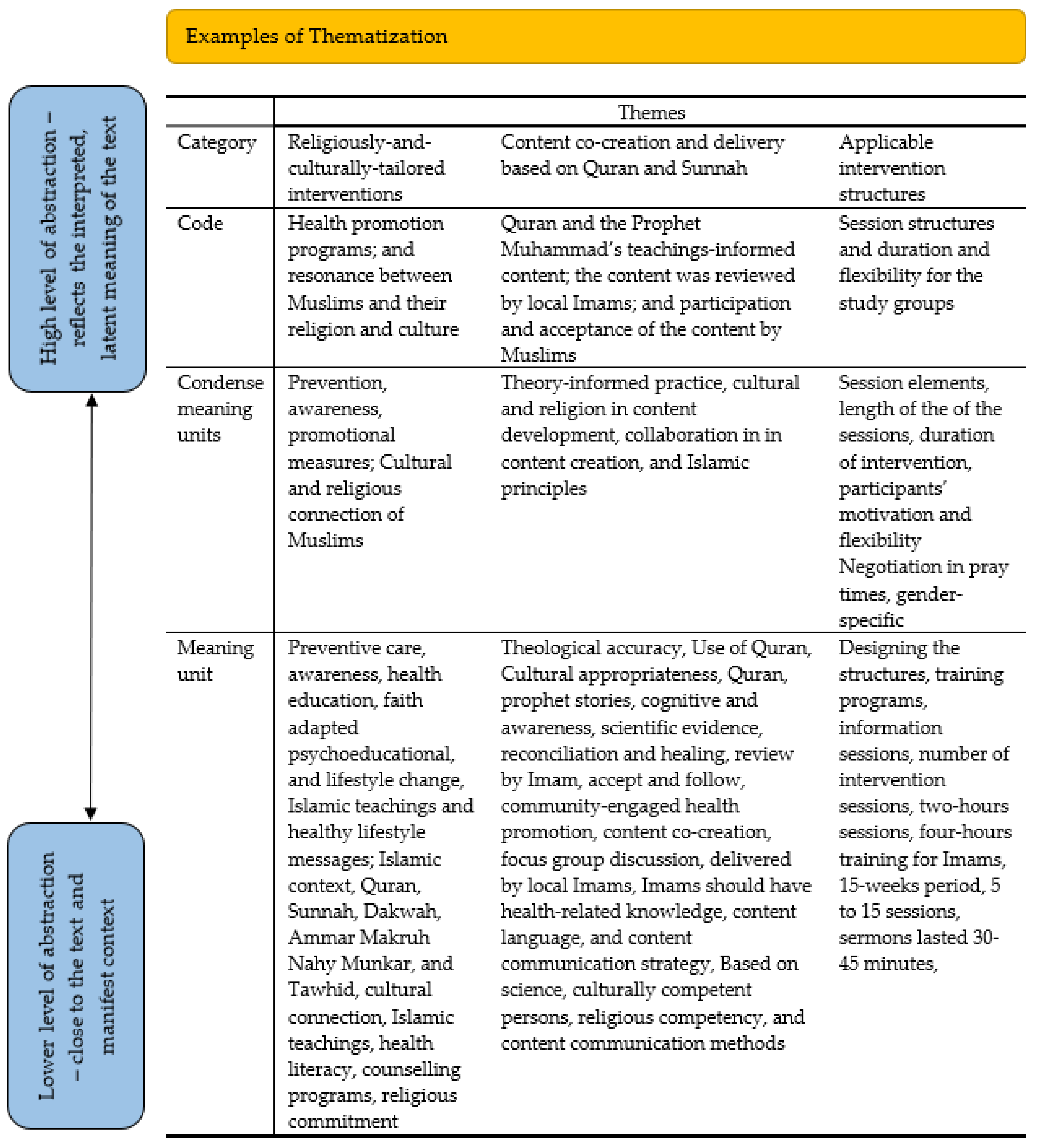
2.5. Synthesis and Analysis of Results
3. Results
3.1. The Study Characteristics
3.2. The Interventions: Nature and Features
3.3. Religiously Tailored Interventions
3.4. Content Co-Creation and Delivery Based on the Quran and Sunnah
3.5. Applicable Intervention Structures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Abdulwasi, Munira, Meena Bhardwaj, Yuka Nakamura, Maha Zawi, Jennifer Price, Paula Harvey, and Ananya Tina Banerjee. 2018. An ecological exploration of facilitators to participation in a mosque-based physical activity program for South Asian Muslim women. Journal of Physical Activity and Health 15: 671–78. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ras, Wahiba, Ali Gheith, and Francine Cournos. 2008. The Imam’s Role in Mental Health Promotion: A Study at 22 Mosques in New York City’s Muslim Community. Journal of Muslim Mental Health 3: 155–76. [Google Scholar] [CrossRef]
- Akers, Jo, Raquel Aguiar-Ibáñez, and Ali Baba-Akbari Sari. 2009. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care, 3rd ed. York: Centre for Reviews and Dissemination, University of York. [Google Scholar]
- Al-Rumayyan, Ahmed, Hamoud Alqarni, Bader S. Almanna, Naif Althonayan, Mohammed Alhalafi, and Nawaf Alomary. 2020. Utilization of Complementary Medicine by Pediatric Neurology Patients and Their Families in Saudi Arabia. Curēus (Palo Alto, CA) 12: e7960. [Google Scholar] [CrossRef]
- Al Haq, M. Ashraf, Nor Azlina Binti Abd Wahab, Hj Abdullah Abd Ghani, and Nor Hayati Ahmad. 2016. Islamic Prayer, Spirituality and Productivity: An Exploratory Conceptual Analysis. Al-Iqtishad: Jurnal Ilmu Ekonomi Syariah 8: 271–86. [Google Scholar] [CrossRef]
- Amri, Saara, and Fred Bemak. 2013. Mental health help-seeking behaviors of Muslim immigrants in the United States: Overcoming social stigma and cultural mistrust. Journal of Muslim Mental Health 7. [Google Scholar] [CrossRef] [Green Version]
- Asadzandi, Minoo. 2017. Sound Heart: Spiritual Nursing Care Model from Religious Viewpoint. Journal of Religion and Health 56: 2063–75. [Google Scholar] [CrossRef] [PubMed]
- Asadzandi, Minoo. 2020. An Islamic Religious Spiritual Health Training Model for Patients. Journal of Religion and Health 59: 173–87. [Google Scholar] [CrossRef] [PubMed]
- Bader, Anglika, Doris Musshauser, Filiz Sahin, Hayriye Bezirkan, and Margarethe Hochleitner. 2006. The Mosque Campaign: A cardiovascular prevention program for female Turkish immigrants. Wiener Klinische Wochenschrift 118: 217–23. [Google Scholar] [CrossRef]
- Banerjee, Ananya Tina, Mireille Landry, Maha Zawi, Debbie Childerhose, Neil Stephens, Ammara Shafique, and Jennifer Price. 2017. A pilot examination of a mosque-based physical activity intervention for South Asian Muslim women in Ontario, Canada. Journal of Immigrant and Minority Health 19: 349–57. [Google Scholar] [CrossRef]
- Basil, H. Aboul-Enein. 2016. Health-Promoting Verses as mentioned in the Holy Quran. Journal of Religion and Health 55: 821–29. [Google Scholar] [CrossRef]
- Bosire, Edna N., Lindile Cele, Xola Potelwa, Allison Cho, and Emily Mendenhall. 2021. God, Church water and spirituality: Perspectives on health and healing in Soweto, South Africa. Global Public Health, 1–14. [Google Scholar] [CrossRef]
- Braun, Virginia, and Victoria Clarke. 2013. Successful Qualitative Research: A Practical Guide for Beginners. London: Sage. [Google Scholar]
- Chaudhary, Anila, Niccolo Dosto, Rachel Hill, Maiju Lehmijoki-Gardner, Phyllis Sharp, W. Daniel Hale, and Panagis Galiatsatos. 2019. Community Intervention for Syrian Refugees in Baltimore City: The Lay Health Educator Program at a Local Mosque. Journal of Religion and Health 58: 1687–97. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Dar, Michal, and Samira Obeid. 2017. Islamic Religious Leaders in Israel as Social Agents for Change on Health-Related Issues. Journal of Religion and Health 56: 2285–96. [Google Scholar] [CrossRef]
- Colic-Peisker, Val. 2009. Visibility, settlement success and life satisfaction in three refugee communities in Australia. Ethnicities 9: 175–99. [Google Scholar] [CrossRef]
- Darko, Natalie, Helen Dallosso, Michelle Hadjiconstantinou, Kerry Hulley, Kamlesh Khunti, and Melanie Davies. 2020. Qualitative evaluation of A Safer Ramadan, a structured education programme that addresses the safer observance of Ramadan for Muslims with Type 2 diabetes. Diabetes Research and Clinical Practice 160: 107979. [Google Scholar] [CrossRef] [PubMed]
- Delbridge, Robyn, Loretta Garvey, Jessica L. Mackelprang, Nicole Cassar, Emily Ward-Pahl, Mikaela Egan, and Anne Williams. 2021. Working at a cultural interface: Co-creating Aboriginal health curriculum for health professions. Higher Education Research and Development, 1–16. [Google Scholar] [CrossRef]
- Duman, Mesude, Yeter Durgun Ozan, and Özlem Doğan Yüksekol. 2021. Relationship between the religious attitudes of women with gynecologic cancer and mental adjustment to cancer. Palliat Support Care 19: 62–68. [Google Scholar] [CrossRef]
- El-Seedi, Hesham R., Shaden A. M. Khalifa, Nermeen Yosri, Alfi Khatib, Lei Chen, Aamer Saeed, Thomas Efferth, and Rob Verpoorte. 2019. Plants mentioned in the Islamic Scriptures (Holy Qur’ân and Ahadith): Traditional uses and medicinal importance in contemporary times. Journal of Ethnopharmacology 243: 112007. [Google Scholar] [CrossRef]
- Erlingsson, Christen, and Petra Brysiewicz. 2017. A hands-on guide to doing content analysis. African Journal of Emergency Medicine 7: 93–99. [Google Scholar] [CrossRef]
- Gardner, Timothy M., Christian U. Krägeloh, and Marcus A. Henning. 2014. Religious coping, stress, and quality of life of Muslim university students in New Zealand. Mental Health, Religion & Culture 17: 327–38. [Google Scholar] [CrossRef]
- Ghafournia, Nafiseh. 2017. Muslim women and domestic violence: Developing a framework for social work practice. Journal of Religion & Spirituality in Social Work: Social Thought 36: 146–63. [Google Scholar] [CrossRef]
- Grace, Clare, Reha Begum, Syed Subhani, Peter Kopelman, and Trisha Greenhalgh. 2008. Prevention of type 2 diabetes in British Bangladeshis: Qualitative study of community, religious, and professional perspectives. British Medical Journal 337: 1094–97. [Google Scholar] [CrossRef] [Green Version]
- Hardan-Khalil, Kholoud. 2020. Factors Affecting Health-Promoting Lifestyle Behaviors Among Arab American Women. Journal of Transcultural Nursing 31: 267–75. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, Neda, Maryam Marzban, Bernadette Sebar, and Neil Harris. 2020. Religious Identity and Psychological Well-Being Among Middle-Eastern Migrants in Australia: The Mediating Role of Perceived Social Support, Social Connectedness, and Perceived Discrimination. Psychology of Religion and Spirituality 12: 475–86. [Google Scholar] [CrossRef]
- Hassan, Ahmed N., Heba Ragheb, Arfeen Malick, Zainib Abdullah, Yusra Ahmad, Nadiya Sunderji, and Farah Islam. 2021. Inspiring Muslim minds: Evaluating a spiritually adapted psycho-educational program on addiction to overcome stigma in Canadian Muslim communities. Community Mental Health Journal 57: 644–54. [Google Scholar] [CrossRef] [PubMed]
- Hong, Quan Nha, Pierre Pluye, Sergi Fàbregues, Gillian Bartlett, Felicity Boardman, Margaret Cargo, Pierre Dagenais, Marie-Pierre Gagnon, Frances Griffiths, and Belinda Nicolau. 2018. Mixed methods appraisal tool (MMAT), version 2018. Registration of Copyright 1148552: 10. [Google Scholar]
- Illueca, Marta, and Benjamin R. Doolittle. 2020. The Use of Prayer in the Management of Pain: A Systematic Review. Journal of Religion and Health 59: 681–99. [Google Scholar] [CrossRef]
- Islam, Nadia S, Darius Tandon, Runi Mukherji, Michael Tanner, Krittika Ghosh, Gulnahar Alam, Mamnunal Haq, Mariano Jose Rey, and Chau Trinh-Shevrin. 2012. Understanding Barriers to and Facilitators of Diabetes Control and Prevention in the New York City Bangladeshi Community: A Mixed-Methods Approach. American Journal of Public Health 102: 486–90. [Google Scholar] [CrossRef]
- Islam, Farah, Nazilla Khanlou, Alison Macpherson, and Hala Tamim. 2018a. Mental Health Consultation Among Ontario’s Immigrant Populations. Community Mental Health Journal 54: 579–89. [Google Scholar] [CrossRef]
- Islam, Nadia S., Laura C. Wyatt, Md Taher, Lindsey Riley, S. Darius Tandon, Michael Tanner, B. Runi Mukherji, and Chau Trinh-Shevrin. 2018b. A Culturally Tailored Community Health Worker Intervention Leads to Improvement in Patient-Centered Outcomes for Immigrant Patients With Type 2 Diabetes. Clinical Diabetes 36: 100. [Google Scholar] [CrossRef] [Green Version]
- Jawaid, Hena. 2020. Assessing Perception of Patients and Physicians Regarding Spirituality in Karachi, Pakistan: A Pilot Study. Permanente Journal 24. [Google Scholar] [CrossRef]
- Jepson, Ruth G., Fiona M. Harris, Stephen Platt, and Carol Tannahill. 2010. The effectiveness of interventions to change six health behaviours: A review of reviews. BMC Public Health 10: 1–16. [Google Scholar] [CrossRef] [Green Version]
- Jongen, Crystal Sky, Janya McCalman, and Roxanne Gwendalyn Bainbridge. 2017. The implementation and evaluation of health promotion services and programs to improve cultural competency: A systematic scoping review. Frontiers in Public Health 5: 24. [Google Scholar] [CrossRef] [Green Version]
- Jozaghi, Ehsan, Muhammad Asadullah, and Azim Dahya. 2016. The role of Muslim faith-based programs in transforming the lives of people suffering with mental health and addiction problems. Journal of Substance Use 21: 587–93. [Google Scholar] [CrossRef]
- Khan, Shamsul, and Mahjabeen Ahmad. 2014. The case for Muslim aged care in the west. Journal of Religion, Spirituality & Aging 26: 281–99. [Google Scholar] [CrossRef]
- King, Rebecca, Sahil Warsi, Amanda Amos, Sundes Shah, Ghazala Mir, Aziz Sheikh, and Kamran Siddiqi. 2017. Involving mosques in health promotion programmes: A qualitative exploration of the MCLASS intervention on smoking in the home. Health Education Research 32: 293–305. [Google Scholar] [CrossRef]
- Koenig, Harold G., Terrence D. Hill, Steven Pirutinsky, and David H Rosmarin. 2021. Commentary on “does spirituality or religion positively affect mental health”? The International Journal for the Psychology of Religion 31: 27–44. [Google Scholar] [CrossRef]
- Koenig, Harold G., and Saad Al Shohaib. 2014. Health and Well-Being in Islamic Societies: Background, Research, and Applications, 2014th ed. Cham: Springer International Publishing AG, vol. 9783319058733. [Google Scholar]
- Koerner, Catherine, and Soma Pillay. 2020. Policy, Practice, and Legislative Matters. In Governance and Multiculturalism: The White Elephand of Social Construction and Cultural Identities. Cham: Palgrave Macmillan, pp. 221–69. [Google Scholar]
- Kongsuwan, Waraporn, and Warangkana Chatchawet. 2019. Effect of nursing intervention integrating an Islamic praying program on labor pain and pain behaviors in primiparous Muslim women. Iranian Journal of Nursing and Midwifery Research 24: 220–26. [Google Scholar] [CrossRef]
- Lewinson, Lesline P., Wilfred McSherry, and Peter Kevern. 2018. “Enablement”—Spirituality Engagement in Pre-Registration Nurse Education and Practice: A Grounded Theory Investigation. Religions 9: 356. [Google Scholar] [CrossRef] [Green Version]
- Marinescu, Lluiza G., Denise Sharify, James Krieger, Brian E. Saelens, Jeniffer Calleja, and Ayaan Aden. 2013. Be Active Together: Supporting Physical Activity in Public Housing Communities Through Women-Only Programs. Progress in Community Health Partnerships-Research Education and Action 7: 57–66. [Google Scholar] [CrossRef] [PubMed]
- Maynard, Maria, Graham Baker, and Seeromanie Harding. 2017. Exploring childhood obesity prevention among diverse ethnic groups in schools and places of worship: Recruitment, acceptability and feasibility of data collection and intervention components. Preventive Medicine Reports 6: 130–36. [Google Scholar] [CrossRef] [PubMed]
- McCoy, John, Anna Kirova, and W. Andy Knight. 2016. Gauging social integration among Canadian Muslims: A sense of belonging in an age of anxiety. Canadian Ethnic Studies 48: 21–52. [Google Scholar] [CrossRef]
- McLaren, Helen J., and Tejaswini Vishwanath Patil. 2016. Manipulative silences and the politics of representation of boat children in Australian print media. Continuum: Journal of Media & Cultural Studies 30: 602–12. [Google Scholar] [CrossRef]
- McLaren, Helen J., and Nismah Qonita. 2020. Indonesia’s Orphanage Trade: Islamic Philanthropy’s Good Intentions, Some Not So Good Outcomes. Religions 11: 1. [Google Scholar] [CrossRef] [Green Version]
- Mehmood, Azhar, Suliman Khan, Sajid Khan, Saeed Ahmed, Ashaq Ali, Mengzhou Xue, Liaqat Ali, Muhammad Hamza, Anum munir, Saad ur Rehman, and et al. 2021. In silico analysis of quranic and prophetic medicinals plants for the treatment of infectious viral diseases including corona virus. Saudi Journal of Biological Sciences 28: 3137–51. [Google Scholar] [CrossRef] [PubMed]
- Meyer, Claudia, Rajna Ogrin, Hamzah Al-Zubaidi, Arti Appannah, Sally McMillan, Elizabeth Barrett, and Colette Browning. 2017. Diversity training for community aged care workers: An interdisciplinary meta-narrative review. Educational Gerontology 43: 365–78. [Google Scholar] [CrossRef]
- Minas, Harry, Ritsuko Kakuma, Lay San Too, Hamza Vayani, Sharon Orapeleng, Rita Prasad-Ildes, Greg Turner, Nicholas Procter, and Daryl Oehm. 2013. Mental health research and evaluation in multicultural Australia: Developing a culture of inclusion. International Journal of Mental Health Systems 7: 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munsoor, Mohamed Safiullah, and Hannah Safiullah Munsoor. 2017. Well-being and the worshipper: A scientific perspective of selected contemplative practices in Islam. Humanomics 33: 163–88. [Google Scholar] [CrossRef]
- Nagle, John. 2016. Multiculturalism’s Double-Bind: Creating Inclusivity, Cosmopolitanism and Difference. London: Routledge. [Google Scholar]
- Novita, Rice, Mustakim, and Febi Nur Salisah. 2021. Determination of the relationship pattern of association topic on Al-Qur’an using FP-Growth Algorithms. IOP Conference Series. Materials Science and Engineering 1088: 12020. [Google Scholar] [CrossRef]
- Padela, Aasim I., Sana Malik, Milkie Vu, Michael Quinn, and Monica Peek. 2018a. Developing religiously-tailored health messages for behavioral change: Introducing the reframe, reprioritize, and reform (“3R”) model. Social Science and Medicine 204: 92–99. [Google Scholar] [CrossRef]
- Padela, Aasim I., Sana Malik, and Nadia Ahmed. 2018b. Acceptability of Friday sermons as a modality for health promotion and education. Journal of Immigrant and Minority Health 20: 1075–84. [Google Scholar] [CrossRef] [PubMed]
- Padela, Aasim I., Sana Malik, Akila Ally Syeda, Michael Quinn, Stephen Hall, and Monica Peek. 2018c. Reducing Muslim Mammography Disparities: Outcomes From a Religiously Tailored Mosque-Based Intervention. Health Education and Behavior 45: 1025–35. [Google Scholar] [CrossRef]
- Padela, Aasim I., Sana Malik, Hena Din, Stephen Hall, and Michael Quinn. 2019. Changing Mammography-Related Beliefs Among American Muslim Women: Findings from a Religiously-Tailored Mosque-Based Intervention. Journal of Immigrant and Minority Health 21: 1325–33. [Google Scholar] [CrossRef]
- Page, Matthew J., David Moher, Patrick M. Bossuyt, Isabelle Boutron, Tammy C. Hoffmann, Cynthia D. Mulrow, Larissa Shamseer, Jennifer M. Tetzlaff, Elie A. Akl, Sue E. Brennan, and et al. 2021. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 372: n160. [Google Scholar] [CrossRef] [PubMed]
- Palmer Kelly, Elizabeth, Madison Hyer, Nicolette Payne, and Timothy M. Pawlik. 2020. Does spiritual and religious orientation impact the clinical practice of healthcare providers? Journal of Interprofessional Care 34: 520–27. [Google Scholar] [CrossRef] [PubMed]
- Parati, Graziella. 2017. Transitive spaces. In Migrant Writers and Urban Space in Italy. Edited by Graziella Parati. Cham: Springer, pp. 37–85. [Google Scholar]
- Pasyar, Nilofar, Masoume Rambod, and Mostafa Jowkar. 2020. The Effect of Peer Support on Hope Among Patients Under Hemodialysis. International Journal of Nephrology and Renovascular Disease 13: 37–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patil, Tejaswini Vishwanath, and Helen Jacqueline McLaren. 2019. Australian Media and Islamophobia: Representations of Asylum Seeker Children. Religions 10: 501. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, Jane, Hong Li, Maybelline Martez, and Tim Gillespie. 2018. The Role of Religious Behavior in Health Self-Management: A Community-Based Participatory Research Study. Religions 9: 357. [Google Scholar] [CrossRef] [Green Version]
- Powers-James, Catherine, Adriana Alvarez, Kathrin Milbury, Andrea Barbo, Katherine Daunov, Gabriel Lopez, Lorenzo Cohen, Marvin O. Delgado-Guay, Olufunmilayo I. Olopade, and Richard T. Lee. 2020. The Influence of Spirituality and Religiosity on US Oncologists’ Personal Use of and Clinical Practices Regarding Complementary and Alternative Medicine. Integrative Cancer Therapies 19. [Google Scholar] [CrossRef]
- Ragsdale, Judith R., Mohammad Othman, Ruby Khoury, Christopher E. Dandoy, Karen Geiger-Behm, Mark Mueller, Eyad Mussallam, and Stella M. Davies. 2018. Islam, The Holy Qur’an, and Medical Decision-Making: The Experience of Middle Eastern Muslim Families with Children Undergoing Bone Marrow Transplantation in the United States. Journal of Pastoral Care & Counseling 72: 180–89. [Google Scholar] [CrossRef]
- Rambod, Masoume, Farkhondeh Sharif, Zahra Molazem, and Kate Khair. 2019. Spirituality Experiences in Hemophilia Patients: A Phenomenological Study. Journal of Religion and Health 58: 992–1002. [Google Scholar] [CrossRef]
- Rambod, Masoume, Nilofar Pasyar, and Mahsa Mokhtarizadeh. 2020. Psychosocial, Spiritual, and Biomedical Predictors of Hope in Hemodialysis Patients. International Journal of Nephrology and Renovascular Disease 13: 163–69. [Google Scholar] [CrossRef]
- Rossato, Lucas, Ana M. Ullán, and Fabio Scorsolini-Comin. 2021. Profile of scientific production on religiosity and spirituality in coping with childhood cancer. Archive for the Psychology of Religion. [Google Scholar] [CrossRef]
- Salma, Jordana, and Bukola Salami. 2020. “Growing Old is not for the Weak of Heart”: Social isolation and loneliness in Muslim immigrant older adults in Canada. Health & Social Care in the Community 28: 615–23. [Google Scholar] [CrossRef]
- Sena Lomba Vasconcelos, Ana Paula, Alessandra Lamas Granero Lucchetti, Ana Paula Rodrigues Cavalcanti, Simone Regina Souza da Silva Conde, Lidia Maria Goncalves, Filipe Rodrigues do Nascimento, Ana Claudia Santos Chazan, Rubens Lene Carvalho Tavares, Oscarina da Silva Ezequiel, and Giancarlo Lucchetti. 2020. Religiosity and Spirituality of Resident Physicians and Implications for Clinical Practice-the SBRAMER Multicenter Study. Journal of General Internal Medicine 35: 3613–19. [Google Scholar] [CrossRef] [PubMed]
- Siddique, Ifran, and Douglas A. Mitchell. 2013. The impact of a community-based health education programme on oral cancer risk factor awareness among a Gujarati community. British Dental Journal 215. [Google Scholar] [CrossRef] [PubMed]
- Sohail, Malik Muhammad, Qaisar Khalid Mahmood, Falak Sher, Muhammad Saud, Siti Mas’udah, and Rachmah Ida. 2020. Coping Through Religiosity, Spirituality and Social Support Among Muslim Chronic Hepatitis Patients. Journal of Religion and Health 59: 3126–40. [Google Scholar] [CrossRef] [PubMed]
- Thunström, Linda, Chian Jones Ritten, Christopher Bastian, Elizabeth Minton, and Dayana Zhappassova. 2021. Trust and Trustworthiness of Christians, Muslims, and Atheists/Agnostics in the United States. Journal for the Scientific Study of Religion 60: 147–79. [Google Scholar] [CrossRef]
- Tse, Tina. 2002. Islamic Community Worker Training Program for the Management of Depression. The Australian e-Journal for the Advancement of Mental Health 1: 121–27. [Google Scholar] [CrossRef]
- Vu, Milkie, Hadiyah Muhammad, Monica E. Peek, and Aasim I. Padela. 2018. Muslim women’s perspectives on designing mosque-based women’s health interventions-An exploratory qualitative study. Women & Health 58: 334–46. [Google Scholar] [CrossRef]
- Whittemore, Robin, and Kathleen Knafl. 2005. The integrative review: Updated methodology. Journal of Advanced Nursing 52: 546–53. [Google Scholar] [CrossRef] [PubMed]
- Widianingsih, Ida, Helen Jaqueline McLaren, and Janet McIntyre-Mills. 2018. Decentralization, Participatory Planning, and the Anthropocene in Indonesia, with a Case Example of the Berugak Dese, Lombok, Indonesia. In Balancing Individualism and Collectivism: Social and Environmental Justice. Edited by Janet McIntyre-Mills, Norma Romm and Yvonne Corcoran-Nantes. Cham: Springer International Publishing, pp. 271–84. [Google Scholar]
- Zoellner, Lori, Belinda Graham, Elizabeth Marks, Norah Feeny, Jacob Bentley, Anna Franklin, and Diana Lang. 2018. Islamic Trauma Healing: Initial Feasibility and Pilot Data. Societies 8: 47. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Authors, Year and Country | Study Aims | Methods and Samples | Contexts and Methodology | Overview of Interventions and Religiosity Considerations |
| Abdulwasi et al. (2018), Canada | Investigate factors associated with South Asian women’s decisions to engage in physical exercise programs. | Descriptive qualitative study, purposive sampling. Semi-structured interviews, women (n = 12), 100% Muslim. | Mosque-based health promotion activity. Ecological framework informed the intervention. | Delivery of a women’s exercise program via a mosque partnership with a cardiovascular health initiative at a women’s hospital, and a diabetes prevention program at a health center. Islamic teachings enabled women to understand caring for one’s own body as consistent with religious world views, with physical exercise as a form of worship when integrating with teachings in the Quran. Integration included sex-segregation, modest clothing, no physical activity during religious fasting. Activity types required approval of mosque council members. |
| Bader et al. (2006), Austria | Measure outcomes of a cardiovascular health prevention activity to Turkish immigrant women. | Three cross-sectional studies yearly, purposive sampling. Surveys, women (n = 2446), 100% Muslim. | Mosque-based health prevention program. Ethnocentric orientation as the center of intervention design. | A cardiovascular health promotion activity (lecture and Turkish-language print materials) for women was delivered in 28 mosques during an annual mosque campaign on women’s health. Mosque was chosen upon identifying importance of it as a socio-political center for the Turkish community. Fliers were distributed by religious leaders to men at Friday prayer, to give to the wives, as a form of approval. Permission from head of each mosque for use of facility. |
| Banerjee et al. (2017), Canada | Evaluate the effectiveness of a healthy lifestyle program for South Asian women. | Participatory action research, purposive sampling. Pre-post surveys, women (n = 19), 100% Muslim. | Mosque-based health promotion program. Religiously tailored intervention approach. | Physical activity program of 24 weeks duration to 62 women, comprised of cardiovascular exercise and strength training. Evening classes minimized disruption to usual mosque activities and the women’s filial responsibilities. Activities approved by the mosque council members were walking, resistance training, relaxation, and chair exercises. Permission to use the Sisters prayer room. |
| Chaudhary et al. (2019), USA | Evaluate lay educator training for delivery of health promotion to Syrian refugees. | Prospective cohort study, purposive sampling. Surveys, women (n = 17), men (n = 1), 100% Muslim. | Mosque-based lay educator program. Religiously tailored peer-development for health promotion. | Six-week lay educator training in health and healthcare. Lay educators then disseminated information to 99 individuals over 24 months. Imam nominated people to become lay educators, the health topics and advised on religious sensitivities when promoting lifestyle modifications and mental health interventions. |
| Darko et al. (2020), United Kingdom | Evaluate the outcomes of a diabetes health care training program, “A Safer Ramadan program”. | Qualitative study, purposive sampling. Focus groups (n = 2), women (n = 6), men (n = 6); stakeholder interviews (n = 13), 100% Muslim. | Community based program. Health promotion program. | Training of healthcare professionals (GPs and nurses), community awareness program to 80 participants and patient self-management program, focused on implications for Muslims with type 2 diabetes during Ramadan, and referral service. Co-production with religious and community leaders. Pilot assessed by religious leaders for religiosity. As champions, leaders attended group sessions with community members on type 2 diabetics to express disapproval of fasting. |
| Grace et al. (2008), United Kingdom | Explore perceptions about healthy lifestyles in diabetes prevention, among a Bangladeshi community. | Qualitative study, purposive sampling. 17 focus groups, women (n = 77), men (n = 52); interviews, women (n = 6), men (n = 2), 100% Muslim. | Community center based. Pure research with dual purpose of health promotion. | Focus groups with lay people, Islamic scholars and religious leaders and health professionals. Resonance between healthy lifestyle (diet and exercise) and Islamic teachings were agreed by both religious leaders and lay participants. Lifestyle leading to ill health, physical or mental, accorded with Islam to care for oneself to enable fulfilling responsibilities to their families. |
| Hassan et al. (2021), Canada | Evaluate a spiritually adapted psycho-educational program on substance use for adults. | Convergent mixed method design, purposive sampling. Surveys and focus-groups, 100% Muslim (n = 93). | Mosque-based psycho-educational. Spiritually adapted health promotion program. | One 90-min seminar on substance use and mental health delivered at 9 mosques by Muslim medical and allied health professionals of various racial backgrounds. Facilitators dressed in visible markers of being Muslim (i.e., hijab) to elicit cultural respect of groups and communities. Scientific content was simplified and linked Islamic content, based on reading of the Quran and Hadith, and used to educate about prevalence, stigma and support. |
| Islam et al. (2012), USA | Explain outcomes of health promotion program on knowledge about diabetes risk among a Bangladeshi community. | Mixed-method research, purposive sampling. Surveys and focus groups, 100% Muslim (surveys, n = 169; focus groups, n = 47). | Community centers, health worker-led health promotion program. | Focus groups with members of New York City’s Bangladeshi community on health beliefs and behaviours related to diabetes prevention or management. Facilitators integrated the concept of niyom [rules and routine for life] to reinforce Muslim religious commitment to engage in healthy lifestyles. |
| Islam et al. (2018b), USA | Explain outcomes of a health promotion activity focused on type-2 diabetes to Bangladeshis. | Randomized control trial, random sampling. Surveys, 100% Muslim (n = 336; study group, n = 176; control group, n = 160). | Clinic and community settings, health promotion program. Community health worker led intervention. | Intervention group participated in five, two-hourly group-based educational sessions monthly, and two 90-min one-on-one sessions with a community health worker. Acknowledges lifestyles associated with religious norms but does not report religiosity in design or application. |
| Jozaghi et al. (2016), Canada | Explore impact of a psychosocial intervention for youth and prisoners at risk of substance use and mental ill-health. | Qualitative study, purposive sampling. In-depth interviews, 100% Muslim (n = 8). | Community centers, health promotion program. Empowerment approach with members of the community. | Mentorship, guidance and counselling program for young Muslims struggling with substance use, behavioral and mental health challenges. Integrated religious precepts to set up a foundation in which to promote harm reduction and promote mental health rehabilitation as being relevant to Islam, and to break down stigma associated with substance use and mental illness. |
| King et al. (2017), United Kingdom | Explain outcomes of health education intervention on second-hand smoke exposure among children. | Randomized controlled trial, random sampling. Interviews and focus groups with households (n = 74), 100% Muslim. | Seven religious institutions (6 Mosques & 1 school), health promotion program. | Key information on smoking and second-hand smoke, and promotion of smoke free homes delivered in sermons and school assemblies. Educational package developed with Muslim religious teachers, and information, practical exercises and guidance situated in the Islamic context. |
| Marinescu et al. (2013), USA | Evaluate health promotion activity, specifically physical activity interventions with women. | Community-based participatory research, purposive sampling. Focus groups, 100% Muslim (n = 239). | Community centers, gender specific health promotion program. Religiously tailored. | Physical activity and exercise classes for women-only at community centers for 10 weeks per season, including swimming. Religious considerations allowed women to exit classes for 10–15 min for prayer time if during class time. Respects that mixed-gender physical activity is not religiously acceptable in some Muslim communities. |
| Maynard et al. (2017), United Kingdom | Explains delivery of health promotion activity to ethnic minorities, focused on childhood obesity. | Quasi-experimental study, purposive sampling. Survey (n = 81), 16% Muslim (n = 13) | Places of worship (n = 6, Mosque n = 2) and six schools health promotion program. Child-focused intervention. | Health promotion focused on childhood obesity prevention; reduction of energy dense foods and increase of physical activity, in a once-off session that also included a physical activity. Building of relationships with faith organizations was required to garner support of faith-based communities, but religiosity specific to Muslim communities was not reported. |
| Padela et al. (2018c), USA | Explain outcomes of a group education program on women’s mammography intention. | Quantitative, purposive sampling. Surveys, 100% Muslim (n = 58) | Mosque-based, health promotion program. Theory of planned behaviour. | Constitution of program was two classes, of 7.5 h each, led by peer educators and guest lecturers who conveyed learning to women about breast care and Islamic teachings about health. Messages were religiously tailored to overcome belief barrier, delivered in multiple ways across the sessions. Facilitated discussions by experts integrated health-related and religious teachings. |
| Padela et al. (2018b), USA | Assess community response to mosque-based health promotion during sermons. | Cross-sectional study, purposive sampling. Surveys, 100% Muslim (n = 233). | Mosque-based health sermon at two mosques. Religiously tailored sermons as the intervention. | Two 30–45-min sermons were delivered at Friday prayer and designed to impart promotion information. Sermon development, setting and choice of giver were informed by focus group discussion. Content reviewed by Imams for accuracy and acceptability based on Sunni theology and law. Imams trained to deliver to script, with integration of own language and examples. |
| Padela et al. (2018a), USA | Describe a conceptual model for the delivery of religious tailored health promotion messages. | Qualitative study, purposive sampling. Surveys, focus groups and interviews, 100% Muslim (n = 240). | Conceptual model for Muslim health promotion. Model developed based on social cognitive theories. | Developed a conceptual model to translate behavioral theory into actionable processes for crafting religiously tailored health messages, involving three approaches: reframing, reprioritizing and reforming. Used religious constructs to resolve barriers based on beliefs acquired, then drew on religious teachings and theoretical stances to reform alternative messages about healthy lifestyle behaviours. |
| Padela et al. (2019), USA | Evaluate a religiously tailored intervention to promote uptake of breast cancer screening among women. | Qualitative study, purposive sampling. Focus groups (n = 13), Interviews (n = 19), 100% Muslim. | Community consultation and mosque-based health promotion. Religious tailored social cognitive theory. | Analysis of facilitator and barrier beliefs, having positive or negative influences, upon mammography intention, using guest lectures and facilitated discussion, two-session workshop over two half-days. Use of religion to reframe health, health access and healing are understood in juxtaposition to faith-based ideas around modesty. Imams and mosque staff formed part of project advisory group. |
| Siddique and Mitchell (2013), United Kingdom | Measure impact of a community-based health education to increase oral cancer risk awareness. | Participatory action research design, purposive sampling. Survey, 100% Muslim (n = 96). | Community based oral care health promotion. Education and awareness program. | Short lectures, poster presentations and workshops were delivered by trained dental and medical practitioners. Increased awareness of associations between tobacco, alcohol, other substances with stigma and health seeking barriers. Acknowledged religious prohibition as a factor of nondisclosure of alcohol, tobacco and other substance use. No information on religiosity in program design or delivery was provided. |
| Tse (2002), Australia | Evaluate a training of bilingual community workers to support women with depression. | Qualitative study, purposive sampling. Summative questionnaire, 100% Muslim (n = 20, 16 completers). | Religiously informed training program. Training program for community health workers. | Muslim community workers were trained 3 h per week for 15 weeks to support women with depression; training in communication, interviewing, assessment, networking, facilitation, depression and suicide, postnatal depression, and therapeutic intervention. Based on perspectives that workers from Islamic backgrounds would achieve more effective outcomes in their religio-cultural support to Muslim women. |
| Vu et al. (2018), USA | Explore women’s views on mosque-based health promotion on women’s health. | Qualitative study, purposive sampling. Interviews, 100% Muslim (n = 19). | Mosque-based, health promotion program. Imam and Muslim-peer led education. | Focus group discussions on the modality, content and delivery of mosque-based health promotion to women, including characteristics of role of Imam and peer educators. Imams with health-related knowledge to lead sermons and Muslim women/health workers to -lead classes to promote women’s health. |
| Zoellner et al. (2018), USA | Examine trauma healing intervention targeted at asylum seekers and refugees. | Mixed-methods, purposive sampling. Survey (n = 39); focus group (n = 13), 100% Muslim. | Mosques-based trauma intervention. Islamic trauma needs assessment; and, pilot trauma therapy group. | Consisting of two studies, study 1 community needs assessment informed design of study 2 pilot of trauma healing intervention groups delivered over two sessions each of 4 h duration. Integrated prophet narratives, Islamic principles on reconciliation and healing, and cognitive and trauma exposure principals, and group discussion on trauma healing. Groups and leaders separated by gender. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McLaren, H.; Patmisari, E.; Hamiduzzaman, M.; Jones, M.; Taylor, R. Respect for Religiosity: Review of Faith Integration in Health and Wellbeing Interventions with Muslim Minorities. Religions 2021, 12, 692. https://doi.org/10.3390/rel12090692
McLaren H, Patmisari E, Hamiduzzaman M, Jones M, Taylor R. Respect for Religiosity: Review of Faith Integration in Health and Wellbeing Interventions with Muslim Minorities. Religions. 2021; 12(9):692. https://doi.org/10.3390/rel12090692
Chicago/Turabian StyleMcLaren, Helen, Emi Patmisari, Mohammad Hamiduzzaman, Michelle Jones, and Renee Taylor. 2021. "Respect for Religiosity: Review of Faith Integration in Health and Wellbeing Interventions with Muslim Minorities" Religions 12, no. 9: 692. https://doi.org/10.3390/rel12090692
APA StyleMcLaren, H., Patmisari, E., Hamiduzzaman, M., Jones, M., & Taylor, R. (2021). Respect for Religiosity: Review of Faith Integration in Health and Wellbeing Interventions with Muslim Minorities. Religions, 12(9), 692. https://doi.org/10.3390/rel12090692