Living-Donor Uterus Transplantation: Pre-, Intra-, and Postoperative Parameters Relevant to Surgical Success, Pregnancy, and Obstetrics with Live Births

 ,
, 
 ,
,  , ,
, ,  , , , , add
Show full author list
, , , , add
Show full author list
Abstract
1. Introduction
2. Material and Methods
2.1. Patients and Setting
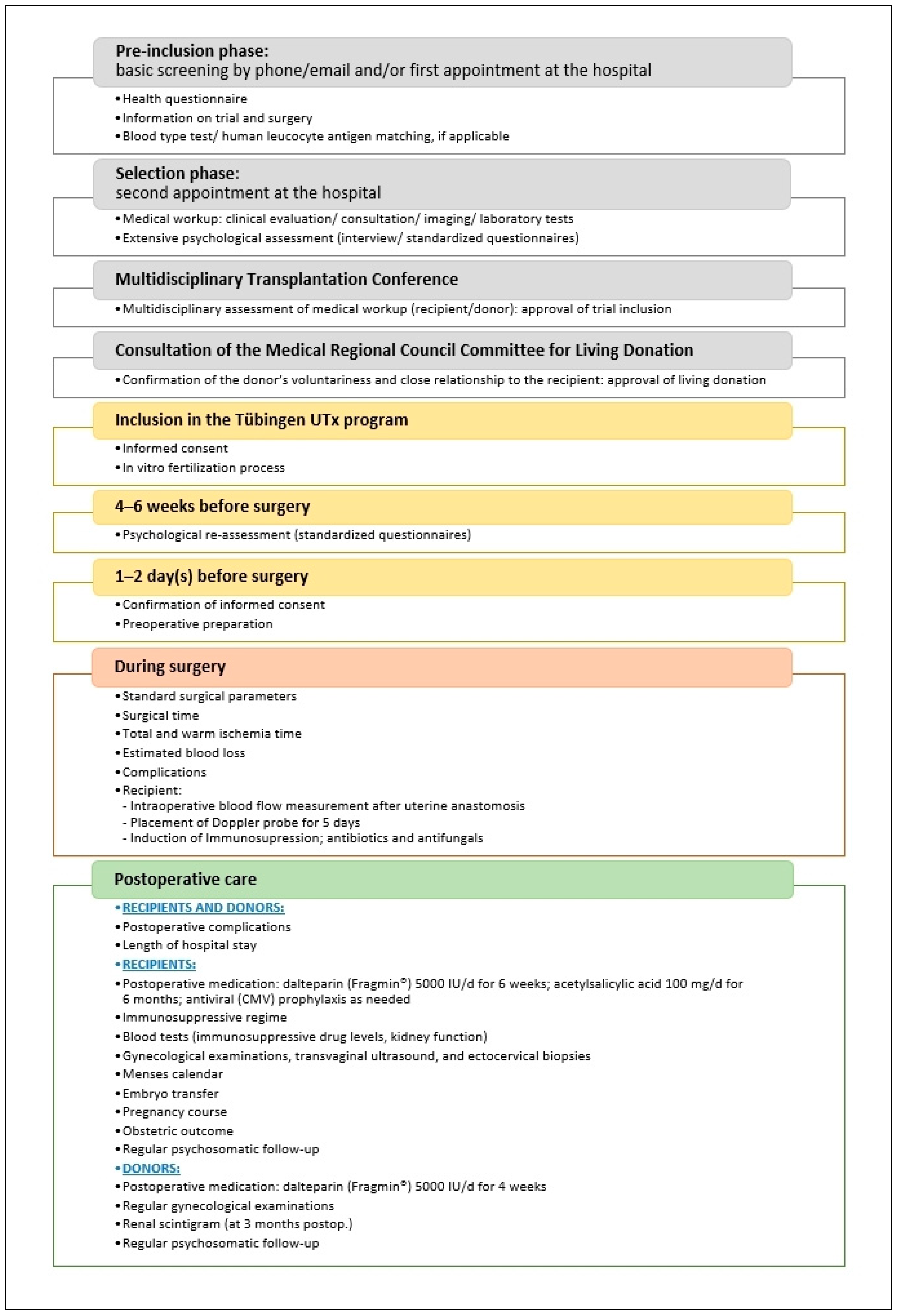
2.2. Design and Objective
2.3. Ethics
2.4. Surgical Technique
2.4.1. Donor Surgery
2.4.2. Recipient Surgery
2.5. Postoperative Immunosuppression
2.6. Data Collection and Analysis
3. Results
3.1. Recipient and Donor Clinical Characteristics at Baseline
3.2. Pre-, Intra-, and Postoperative Clinical Characteristics
3.2.1. Specific Preoperative Investigations and Procedures
- Uterus Evaluation
- 2
- Ovarian Stimulation and Oocyte Retrieval
3.2.2. Intraoperative Results, Vessels Used for Anastomosis, and Intraoperative Doppler Flow Assessments
3.2.3. Intra- and Postoperative Complications, Recovery, and Onset of Menstruation
3.2.4. Immunosuppression and Post-Transplantation Follow-up
3.2.5. Embryo Transfer and Postoperative Ovarian Restimulation
3.2.6. Pregnancy and Obstetric Outcome
3.3. Neonatal Findings and Postnatal Development
3.4. Postpartum Menstruation and Transplant Fate
4. Discussion
4.1. Intraoperative and Postoperative Complications
4.2. Rejection Episodes
4.3. ART Treatment
4.4. Antenatal Complications and Obstetric Outcomes
4.5. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ART | Assisted reproductive technology |
| ATG | Anti-thymocyte globulin |
| AUFI | Absolute uterine factor infertility |
| AZA | Azathioprine |
| BMI | Body mass index |
| bw | Body weight |
| C-D | Clavien-Dindo (classification) |
| CMV | Cytomegalovirus |
| CT | Computed tomography |
| D | Donor |
| DSA | Preformed donor-specific anti-HLA antibody |
| DUA | Deep uterine artery |
| DUV | Deep uterine vein |
| E/S | End to side (anastomosis) |
| EBL | Estimated blood loss |
| EIA | External iliac artery |
| EIV | External iliac vein |
| ET | Embryo transfer |
| HLA | Human leukocyte antigen |
| ICSI | Intracytoplasmic sperm injection |
| IIA | Internal iliac artery |
| IIV | Internal iliac vein |
| IS | Immunosuppression/immunosuppressive |
| ISUTx | International Society of Uterus Transplantation |
| IVF | In vitro fertilization |
| MMF | Mycophenolate mofetil |
| MPL | Missed pregnancy loss |
| MRA | Magnetic resonance angiography |
| MRKHS | Mayer–Rokitansky–Küster–Hauser syndrome |
| NA | Not applicable |
| OV | Ovarian vein |
| PN-2 | Pronuclear stage 2 |
| R | Recipient |
| r-hFSH | Recombinant human follicle-stimulating hormone |
| T1 MRKHS | Type 1 Mayer–Rokitansky–Küster–Hauser syndrome |
| TSE | T2-weighted turbo spin echo |
| UOV | Utero-ovarian vein |
| UTx | Uterus transplantation |
References
- Brännström, M. Introduction: Uterus transplantation. Fertil. Steril. 2019, 112, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Morcel, K.; Camborieux, L.; Guerrier, D. Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome. Orphanet J. Rare Dis. 2007, 2, 13. [Google Scholar] [CrossRef] [PubMed]
- Committee on Adolescent Health Care. ACOG Committee Opinion No. 728: Mullerian Agenesis: Diagnosis, Management, And Treatment. Obstet. Gynecol. 2018, 131, e35–e42. [Google Scholar] [CrossRef] [PubMed]
- Brucker, S.Y.; Rall, K.; Campo, R.; Oppelt, P.; Isaacson, K. Treatment of congenital malformations. Semin. Reprod. Med. 2011, 29, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Schöller, D.; Holting, M.; Stefanescu, D.; Burow, H.; Schönfisch, B.; Rall, K.; Taran, F.A.; Grimbizis, G.F.; Di Spiezio Sardo, A.; Brucker, S.Y. Female genital tract congenital malformations and the applicability of the ESHRE/ESGE classification: A systematic retrospective analysis of 920 patients. Arch. Gynecol. Obstet. 2018, 297, 1473–1481. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Gordts, S.; Di Spiezio Sardo, A.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.C.; Tanos, V.; Brolmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef]
- Bachmann, F.; Budde, K.; Gerland, M.; Wiechers, C.; Heyne, N.; Nadalin, S.; Brucker, S.; Bachmann, C. Pregnancy following kidney transplantation—Impact on mother and graft function and focus on childrens’ longitudinal development. BMC Pregnancy Childbirth 2019, 19, 376. [Google Scholar] [CrossRef]
- Wagner, A.; Brucker, S.Y.; Ueding, E.; Grober-Gratz, D.; Simoes, E.; Rall, K.; Kronenthaler, A.; Schaffeler, N.; Rieger, M.A. Treatment management during the adolescent transition period of girls and young women with Mayer-Rokitansky-Kuster-Hauser syndrome (MRKHS): A systematic literature review. Orphanet J. Rare Dis. 2016, 11, 152. [Google Scholar] [CrossRef]
- Bean, E.J.; Mazur, T.; Robinson, A.D. Mayer-Rokitansky-Kuster-Hauser syndrome: Sexuality, psychological effects, and quality of life. J. Pediatric Adolesc. Gynecol. 2009, 22, 339–346. [Google Scholar] [CrossRef]
- Järvholm, S.; Johannesson, L.; Brannström, M. Psychological aspects in pre-transplantation assessments of patients prior to entering the first uterus transplantation trial. Acta Obstet. Gynecol. Scand. 2015, 94, 1035–1038. [Google Scholar] [CrossRef]
- Rall, K.; Schickner, M.C.; Barresi, G.; Schonfisch, B.; Wallwiener, M.; Wallwiener, C.W.; Wallwiener, D.; Brucker, S.Y. Laparoscopically assisted neovaginoplasty in vaginal agenesis: A long-term outcome study in 240 patients. J. Pediatr. Adolesc. Gynecol. 2014, 27, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M.; Johannesson, L.; Dahm-Kähler, P.; Enskog, A.; Mölne, J.; Kvarnström, N.; Diaz-Garcia, C.; Hanafy, A.; Lundmark, C.; Marcickiewicz, J.; et al. First clinical uterus transplantation trial: A six-month report. Fertil. Steril. 2014, 101, 1228–1236. [Google Scholar] [CrossRef] [PubMed]
- Taran, F.A.; Schöller, D.; Rall, K.; Nadalin, S.; Königsrainer, A.; Henes, M.; Bösmüller, H.; Fend, F.; Nikolaou, K.; Notohamiprodjo, M.; et al. Screening and evaluation of potential recipients and donors for living donor uterus transplantation: Results from a single-center observational study. Fertil. Steril. 2019, 111, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Kölle, A.; Taran, F.A.; Rall, K.; Schöller, D.; Wallwiener, D.; Brucker, S.Y. Neovagina creation methods and their potential impact on subsequent uterus transplantation: A review. BJOG 2019, 126, 1328–1335. [Google Scholar] [CrossRef]
- Johannesson, L.; Kvarnström, N.; Molne, J.; Dahm-Kähler, P.; Enskog, A.; Diaz-Garcia, C.; Olausson, M.; Brännström, M. Uterus transplantation trial: 1-year outcome. Fertil. Steril. 2015, 103, 199–204. [Google Scholar] [CrossRef]
- Brucker, S.Y.; Taran, F.A.; Rall, K.; Schöller, D.; Dahm-Kähler, P.; Kvarnström, N.; Järvholm, S.; Nadalin, S.; Königsrainer, A.; Wallwiener, D.; et al. Experiences of a multistep process with medical and psychological interventions for patients with congenital uterine aplasia to achieve motherhood: The Gothenburg-Tubingen collaboration. Facts Views Vis Obgyn 2019, 11, 121–126. [Google Scholar]
- Brucker, S.Y.; Gegusch, M.; Zubke, W.; Rall, K.; Gauwerky, J.F.; Wallwiener, D. Neovagina creation in vaginal agenesis: Development of a new laparoscopic Vecchietti-based procedure and optimized instruments in a prospective comparative interventional study in 101 patients. Fertil. Steril. 2008, 90, 1940–1952. [Google Scholar] [CrossRef]
- Brucker, S.Y.; Rall, K.; Wallwiener, D. Laparoscopically assisted neovaginoplasty. In Nezhat’s video-assisted and robotic-assisted laparoscopy and hysteroscopy, 4th ed.; Nezhat, C., Nezhat, F.R., Nezhat, C., Eds.; Cambridge University Press: Cambridge, UK, 2013; pp. 426–432. [Google Scholar]
- Brucker, S.Y.; Brännström, M.; Taran, F.A.; Nadalin, S.; Königsrainer, A.; Rall, K.; Schöller, D.; Henes, M.; Bösmüller, H.; Fend, F.; et al. Selecting living donors for uterus transplantation: Lessons learned from two transplantations resulting in menstrual functionality and another attempt, aborted after organ retrieval. Arch. Gynecol. Obstet. 2018, 297, 675–684. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Chmel, R.; Novackova, M.; Janousek, L.; Matecha, J.; Pastor, Z.; Maluskova, J.; Cekal, M.; Kristek, J.; Olausson, M.; Fronek, J. Revaluation and lessons learned from the first 9 cases of a Czech uterus transplantation trial: Four deceased donor and 5 living donor uterus transplantations. Am. J. Transplant. 2019, 19, 855–864. [Google Scholar] [CrossRef]
- Kvarnström, N.; Järvholm, S.; Johannesson, L.; Dahm-Kähler, P.; Olausson, M.; Brännström, M. Live Donors of the Initial Observational Study of Uterus Transplantation-Psychological and Medical Follow-Up Until 1 Year After Surgery in the 9 Cases. Transplantation 2017, 101, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Ramani, A.; Testa, G.; Ghouri, Y.; Koon, E.C.; Di Salvo, M.; McKenna, G.J.; Bayer, J.; Marie Warren, A.; Wall, A.; Johannesson, L. DUETS (Dallas UtErus Transplant Study): Complete report of 6-month and initial 2-year outcomes following open donor hysterectomy. Clin. Transplant. 2020, 34, e13757. [Google Scholar] [CrossRef] [PubMed]
- Mölne, J.; Broecker, V.; Ekberg, J.; Nilsson, O.; Dahm-Kähler, P.; Brännström, M. Monitoring of Human Uterus Transplantation With Cervical Biopsies: A Provisional Scoring System for Rejection. Am. J. Transplant. 2017, 17, 1628–1636. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M. (Department of Obstetrics and Gynecology, Sahlgrenska Academy, University of Gothenburg, Göteborg, Sweden). Personal communication to S. Y. Brucker at the 2nd Congress of ISUTx. Cleveland, OH, USA, 2019.
- Clarke-Pearson, D.L.; Geller, E.J. Complications of hysterectomy. Obstet. Gynecol. 2013, 121, 654–673. [Google Scholar] [CrossRef]
- Fageeh, W.; Raffa, H.; Jabbad, H.; Marzouki, A. Transplantation of the human uterus. Int. J. Gynaecol. Obstet. 2002, 76, 245–251. [Google Scholar] [CrossRef]
- Oh, B.R.; Kwon, D.D.; Park, K.S.; Ryu, S.B.; Park, Y.I.; Presti, J.C., Jr. Late presentation of ureteral injury after laparoscopic surgery. Obstet. Gynecol. 2000, 95, 337–339. [Google Scholar] [CrossRef]
- Flyckt, R.; Falcone, T.; Quintini, C.; Perni, U.; Eghtesad, B.; Richards, E.G.; Farrell, R.M.; Hashimoto, K.; Miller, C.; Ricci, S.; et al. First birth from a deceased donor uterus in the United States: From severe graft rejection to successful cesarean delivery. Am. J. Obstet. Gynecol. 2020. [Google Scholar] [CrossRef]
- Blumenauer, V.; Czeromin, U.; Fehr, D.; Fiedler, K.; Gnoth, C.; Krüssel, J.S.; Kupka, M.S.; Ott, A.; Tandler-Schneider, A.D.I.R. Annual 2018. J. Reproduktionsmed. Endokrinol. 2019, 16, 272–311. [Google Scholar]
- Yaprak, M.; Doğru, V.; Sanhal, C.Y.; Özgür, K.; Erman, M. In Vitro Fertilization After Renal Transplantation: A Single-Center Experience. Transplant. Proc. 2019, 51, 1089–1092. [Google Scholar] [CrossRef]
- Norrman, E.; Bergh, C.; Wennerholm, U.B. Pregnancy outcome and long-term follow-up after in vitro fertilization in women with renal transplantation. Hum. Reprod. 2015, 30, 205–213. [Google Scholar] [CrossRef]
- Castellón, L.A.R.; Amador, M.I.G.; González, R.E.D.; Eduardo, M.S.J.; Díaz-García, C.; Kvarnström, N.; Bränström, M. The history behind successful uterine transplantation in humans. JBRA Assist. Reprod. 2017, 21, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M.; Bokström, H.; Dahm-Kähler, P.; Diaz-Garcia, C.; Ekberg, J.; Enskog, A.; Hagberg, H.; Johannesson, L.; Kvarnström, N.; Mölne, J.; et al. One uterus bridging three generations: First live birth after mother-to-daughter uterus transplantation. Fertil. Steril. 2016, 106, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Testa, G.; McKenna, G.J.; Gunby, R.T., Jr.; Anthony, T.; Koon, E.C.; Warren, A.M.; Putman, J.M.; Zhang, L.; dePrisco, G.; Mitchell, J.M.; et al. First live birth after uterus transplantation in the United States. Am. J. Transplant. 2018, 18, 1270–1274. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.P.; Saso, S.; Bracewell-Milnes, T.; Thum, M.Y.; Nicopoullos, J.; Diaz-Garcia, C.; Friend, P.; Ghaem-Maghami, S.; Testa, G.; Johannesson, L.; et al. Human uterine transplantation: A review of outcomes from the first 45 cases. BJOG 2019, 126, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Kallén, B.; Westgren, M.; Aberg, A.; Olausson, P.O. Pregnancy outcome after maternal organ transplantation in Sweden. BJOG 2005, 112, 904–909. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Recipient 1 | Recipient 3 | Recipient 4 | Recipient 5 | Donor 1 | Donor 3 | Donor 4 | Donor 5 | |
|---|---|---|---|---|---|---|---|---|
| Indication for UTx | T1 MRKHS | T1 MRKHS | T1 MRKHS | T1 MRKHS | NA | NA | NA | NA |
| Donor-Recipient relationship | Daughter | Daughter | Daughter | Sister | Mother | Mother | Mother | Sister |
| Age, years | 23 | 23 | 32 | 35 | 46 | 46 | 56 | 32 |
| Menopausal status | Pre- | Pre- | Pre- | Pre- | Pre- | Pre- | Post- | Pre- |
| BMI, kg/m² | 21.0 | 21.3 | 20.0 | 19.0 | 22.0 | 25.5 | 22.7 | 22.0 |
| Smoking, pack years | 0 | 5 | 0 | 0 | 0 | 5 | 0 | 0 |
| Preoperative abstinence from nicotine, months | NA | 12 | NA | NA | NA | 6 | NA | NA |
| Age at neovagina creation, years | 16 | Self-dilation | 18 | 19 | NA | NA | NA | NA |
| Neovaginal length, cm | 9 | 9 | 9–10 | 9–10 | NA | NA | NA | NA |
| Donor’s para at baseline (type of delivery) | NA | NA | NA | NA | 4 (all vaginal) | 2 (both vaginal) | 3 (1 cesarean, 2 vaginal) | 2 (both vaginal) |
| Donor’s age at delivery, years | NA | NA | NA | NA | 23 (Recipient 1), 24, 28, 30 | 22 (Recipient 3), 25 | 24 (Recipient 4), 27, 35 | 25, 27 |
| Birthweights of donors’ children, g | NA | NA | NA | NA | 3200, 3200, 3500, 3900 | 3600, 3800 | Unknown | 3085, 3460 |
| Fetal gestational age of donors’ children at delivery, weeks | NA | NA | NA | NA | 42 (all 4) | 40, 41 | 36, 41, 41 | 38, 40 |
| Blood group | A Rh− | A Rh− | O Rh+ | A Rh+ | A Rh+ | A Rh− | O Rh+ | A Rh+ |
| Preformed donor-specific anti-HLA antibody screen | No DSA | No DSA | No DSA | No DSA | — | — | — | — |
| HLA mismatches | 2/6 for HLA class I; 1/4 for class II | 0/6 for HLA class I; 2/4 for class II | 2/6 for HLA class I; 2/4 for class II | 4/6 for HLA class I; 2/4 for class II | — | — | — | — |
| HLA mismatches with potential father | None | Not tested | None | 2 repeated mismatches for HLA classes I and II | — | — | — | — |
| MRA: left/right uterine artery diameter, mm | NA | NA | NA | NA | 2.5/2.5 | 3/3.5 | 3/3 | 3/3 |
| MRA: left/right uterine vein diameter, mm | NA | NA | NA | NA | 2/2 | 4/2 | 4/5 | 3/5 |
| Donor 1/Recipient 1 | Donor 3/Recipient 3 | Donor 4/Recipient 4 | Donor 5/Recipient 5 | |
|---|---|---|---|---|
| Recipient oocytes fertilized and cryopreserved for IVF preoperatively | 10 | 6 + 2 (2 cycles of stimulation) | 17 | 14 |
| Recipient oocytes fertilized and cryopreserved for IVF; 2nd attempt, postoperative | 9 | 6 | NA | NA |
| UTx, month/year | 10/2016 | 06/2017 | 01/2019 | 10/2019 |
| Surgical time for donor/recipient, hours | 12.12/5.95 | 9.05/4.52 | 10.40/6.20 | 9.19/8.13 |
| Blood vessels used for anastomosis | Left side: – DUA (D) E/S onto EIA (R) – DUV (D) E/S onto EIV (R) Right side: – DUA (D) E/S onto EIA (R) – DUV (D) E/S onto EIV (R) | Left side: – DUA (D) E/S onto EIA (R) – DUV (D) E/S onto EIV (R) Right side: – DUA (D) E/S onto EIA (R) – OV (D) E/S onto EIV (R) with unilateral (right) ovariectomy | Left side: – DUA (D) E/S onto EIA (R) – DUV (D) and uterine branch of UOV (D), both E/S onto EIV (R) (UOV cranially from DUV) Right side: – DUA (D) E/S onto EIA (R) – DUV (D) E/S onto EIV (R) | Left side: – DUA (D) E/S onto EIA (R) – Uterine branch of UOV (D) with anastomosis onto DUV (D) onto EIV (R) Right side: – DUA (D) onto EIA(R) – DUV (D) and uterine branch of UOV (D) both E/S onto EIV (R) (UOV cranially from DUV) |
| Total ischemia time 1, min | 111 | 119 | 153 | 175 |
| Warm ischemia time 2, min | 63 | 77 | 86 | 83 |
| Estimated blood loss in donor/recipient, mL | 100/200 | 100/150 | 100/200 | 100/500 |
| Surgical complications in donor/recipient | None/None | None/None | None/None | None/Intraoperative reanastomosis of right DUV |
| Length of hospital stay of donor/recipient, days | 11/18 | 12/17 | 14/ 14 | 14/15 |
| Recipient’s first menstruation, weeks post UTx (only) | 6 | 6 | 3 | 5 |
| Graft rejection by recipient, treatment | None | 1 mild episode, successfully treated with 1 cortisone pulse over 3 days | 1 mild episode, successfully treated with 1 cortisone pulse over 3 days | None |
| Other postoperative events in donor/recipient | None/None | None/None | Donor: none/ Recipient: elevated liver enzymes confirmed hepatitis E, successful antiviral therapy; CMV infection, successfully treated with valganciclovir | None/None |
| Recipient pregnancies after UTx | 2; 1 missed pregnancy loss at gestation week 8 | 1 | NA | NA |
| Recipient deliveries after UTx | 1 | 1 | NA | NA |
| Recipient’s mode of delivery | Secondary cesarean section | Primary cesarean section | NA | NA |
| Time from incision to recipient’s delivery, min | 8 | 20 | NA | NA |
| Overall recipient surgery time for delivery, min | 59 | 70 | NA | NA |
| Recipient’s age at delivery, years | 26 | 25 | NA | NA |
| Gestational week + days at delivery | 35 + 1 after preterm prelabor rupture of membranes | 36 + 3, mild oligohydramnios | NA | NA |
| Placental histology | No pathology | No pathology | NA | NA |
| Explantation of the transplanted uterus | No | No | No | No |
| Baby Born to Recipient 1 | Baby Born to Recipient 3 | |
|---|---|---|
| Baby’s sex | Male | Male |
| Month/Year of birth | 05/2019 | 03/2019 |
| Presentation | Cephalic | Cephalic |
| Gestational age at birth, weeks + days | 35 + 1 | 36 + 3 |
| Birthweight, g (percentile) | 2180 (15th) | 2500 (15th) |
| Crown-heel length at birth, cm (percentile) | 45.0 (15th) | 47.0 (15th) |
| Head circumference at birth, cm (percentile) | 31.0 (8th) | 31.0 (< 3rd) |
| Neonatal health status | Healthy | Healthy |
| Apgar score at 1/5/10 min | 9/10/10 | 8/8/8 |
| Umbilical artery blood pH | 7.28 | 7.28 |
| Blood group | A Rh− | A Rh− |
| Diagnoses | Neonatal hypoglycemia and hypothermia | Respiratory maladaptation, CMV negative |
| Treatment | Early feeding, warming bed | CPAP |
| Bodyweight at hospital discharge, g (percentile) | 2376 (5th) | 2370 (4th) |
| Crown-heel length at hospital discharge, cm (percentile) | 45.0 (< 3rd) | 47.0 (8th) |
| Head circumference at hospital discharge, g (percentile) | 31.5 (< 3rd) | 31.0 (< 3rd) |
| Bodyweight at age 6 months, g (percentile) | 7270 (25th) | 8010 (48th) |
| Crown-heel length at age 6 months, cm (percentile) | 63 (5th) | 70 (52nd) |
| Head circumference at age 6 months, g (percentile) | 42 (12th) | 43.5 (50th) |
| Bodyweight at age 12 months, g (percentile) | 8995 (25th) | 9300 (27th) |
| Crown-heel length at age 12 months, cm (percentile) | 72.5 (11th) | 75 (50th) |
| Head circumference at age 12 months, g (percentile) | 47 (50th) | 46.5 (48th) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brucker, S.Y.; Strowitzki, T.; Taran, F.-A.; Rall, K.; Schöller, D.; Hoopmann, M.; Henes, M.; Guthoff, M.; Heyne, N.; Zipfel, S.; et al. Living-Donor Uterus Transplantation: Pre-, Intra-, and Postoperative Parameters Relevant to Surgical Success, Pregnancy, and Obstetrics with Live Births. J. Clin. Med. 2020, 9, 2485. https://doi.org/10.3390/jcm9082485
Brucker SY, Strowitzki T, Taran F-A, Rall K, Schöller D, Hoopmann M, Henes M, Guthoff M, Heyne N, Zipfel S, et al. Living-Donor Uterus Transplantation: Pre-, Intra-, and Postoperative Parameters Relevant to Surgical Success, Pregnancy, and Obstetrics with Live Births. Journal of Clinical Medicine. 2020; 9(8):2485. https://doi.org/10.3390/jcm9082485
Chicago/Turabian StyleBrucker, Sara Yvonne, Thomas Strowitzki, Florin-Andrei Taran, Katharina Rall, Dorit Schöller, Markus Hoopmann, Melanie Henes, Martina Guthoff, Nils Heyne, Stephan Zipfel, and et al. 2020. "Living-Donor Uterus Transplantation: Pre-, Intra-, and Postoperative Parameters Relevant to Surgical Success, Pregnancy, and Obstetrics with Live Births" Journal of Clinical Medicine 9, no. 8: 2485. https://doi.org/10.3390/jcm9082485
APA StyleBrucker, S. Y., Strowitzki, T., Taran, F.-A., Rall, K., Schöller, D., Hoopmann, M., Henes, M., Guthoff, M., Heyne, N., Zipfel, S., Schäffeler, N., Bösmüller, H., Fend, F., Rosenberger, P., Heim, E., Wiesing, U., Nikolaou, K., Fleischer, S., Bakchoul, T., ... Königsrainer, A. (2020). Living-Donor Uterus Transplantation: Pre-, Intra-, and Postoperative Parameters Relevant to Surgical Success, Pregnancy, and Obstetrics with Live Births. Journal of Clinical Medicine, 9(8), 2485. https://doi.org/10.3390/jcm9082485