Nuclear Magnetic Resonance Metabolomics Biomarkers for Identifying High Risk Patients with Extranodal Extension in Oral Squamous Cell Carcinoma



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Histopathology
2.2. Sample Preparation
2.3. NMR Experimental Protocols
2.4. Data Analysis
3. Results
3.1. Patient Demographics
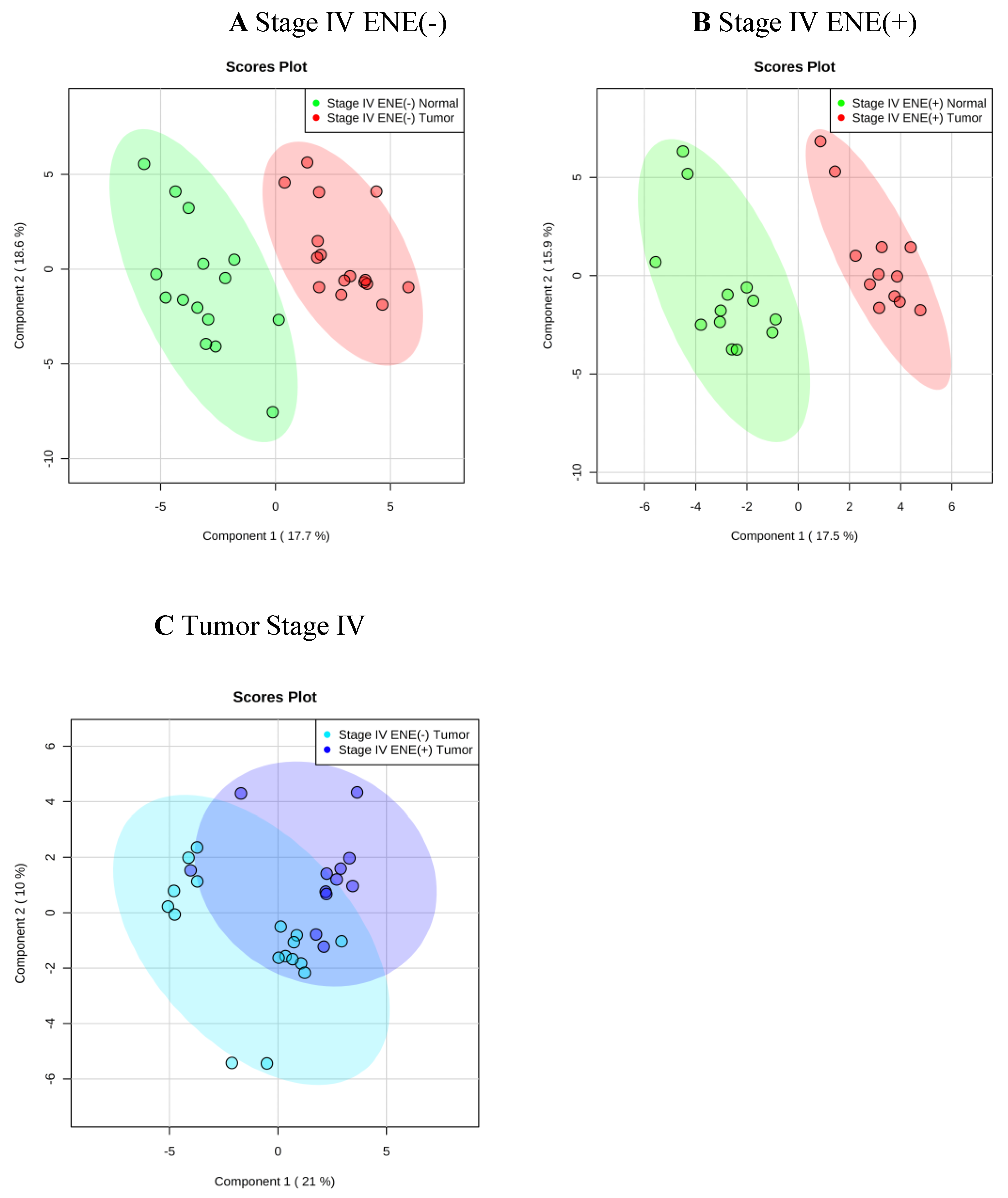
3.2. Metabolic Alteration in Tumor versus Adjacent Normal Tissue
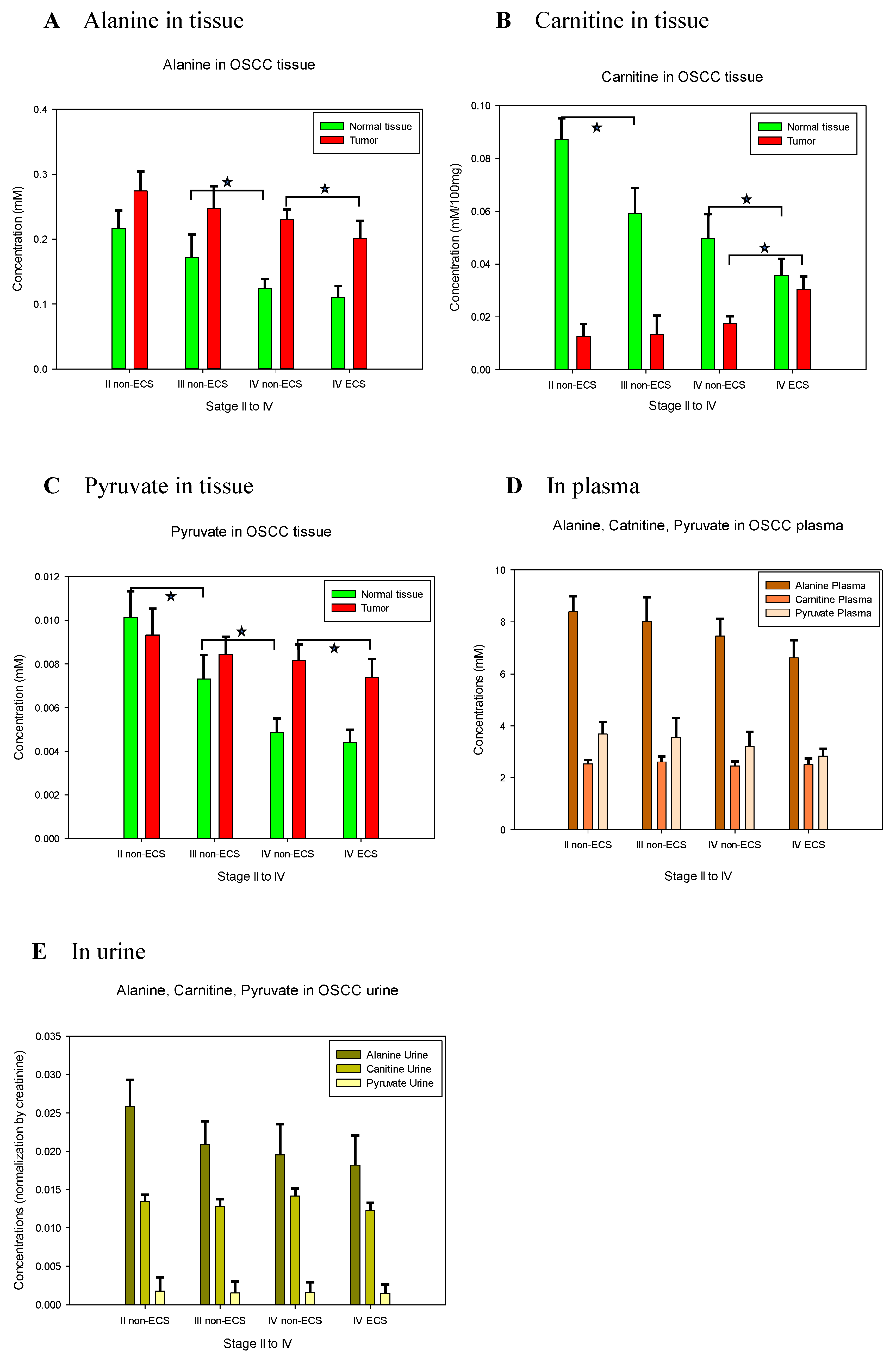
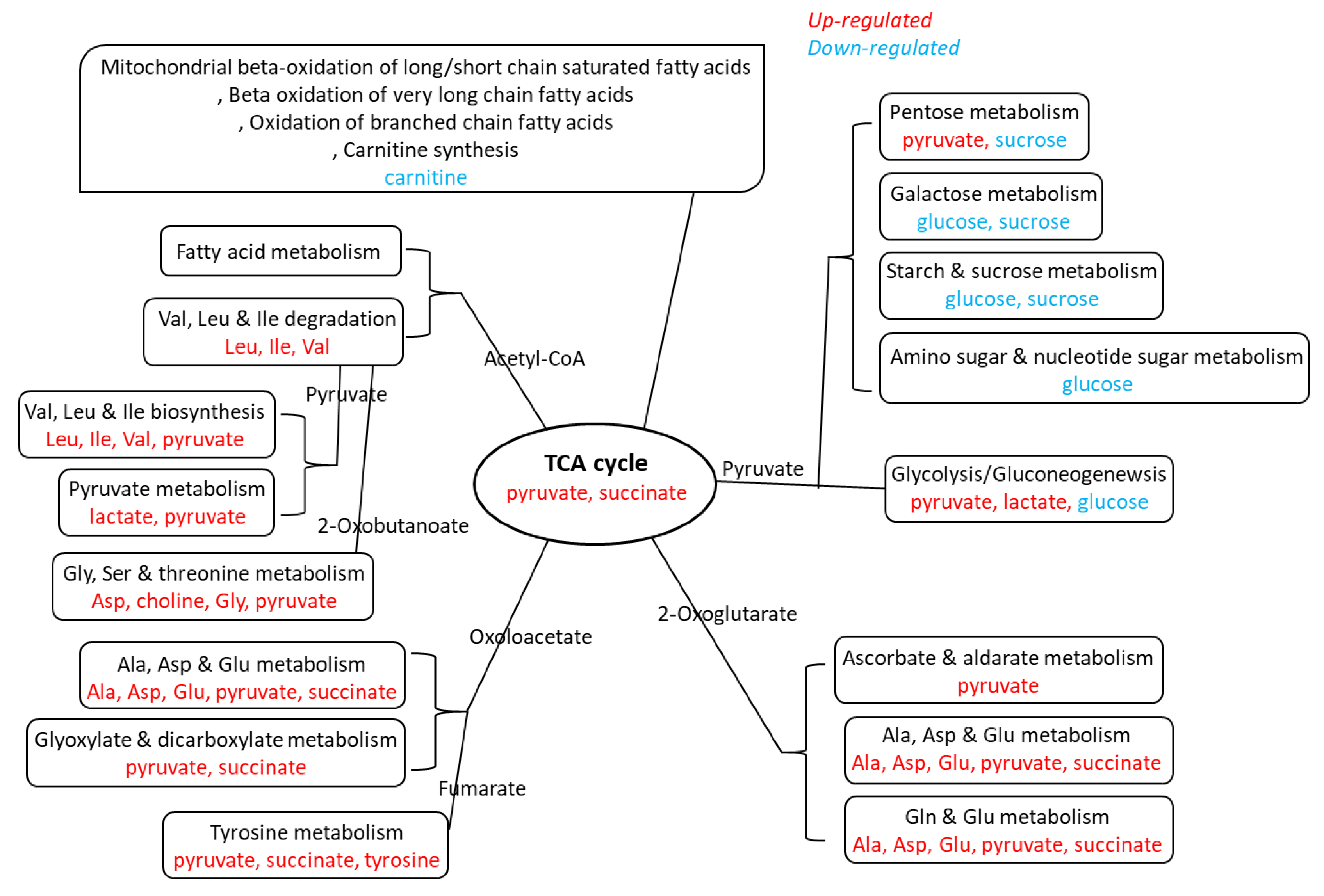
3.3. Metabolic Alteration in Tumor with ENE through Tandem Tissue, Plasma and Urine Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Taghavi, N.; Yazdi, I. Prognostic factors of survival rate in oral squamous cell carcinoma: Clinical, histologic, genetic and molecular concepts. Arch. Iran Med. 2015, 18, 314–319. [Google Scholar]
- Chang, C.C.; Lee, W.T.; Hsiao, J.R.; Ou, C.Y.; Huang, C.C.; Tsai, S.T.; Chen, K.C.; Huang, J.S.; Wong, T.Y.; Lai, Y.H.; et al. Oral hygiene and the overall survival of head and neck cancer patients. Cancer Med. 2019, 8, 1854–1864. [Google Scholar] [CrossRef] [PubMed]
- Vucicevic Boras, V.; Fucic, A.; Virag, M.; Gabric, D.; Blivajs, I.; Tomasovic-Loncaric, C.; Rakusic, Z.; Bisof, V.; Novere, N.L.; Vrdoljak, D.V. Significance of stroma in biology of oral squamous cell carcinoma. Tumori J. 2018, 104, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, N.; Thankappan, K.; Anand, A.; Balasubramanian, D.; Iyer, S. Implementing American Joint Committee on Cancer 8(th) edition for head-and-neck cancer in India: Context, feasibility, and practicality. Indian J. Cancer 2018, 55, 4–8. [Google Scholar] [PubMed]
- Michikawa, C.; Uzawa, N.; Sato, H.; Ohyama, Y.; Okada, N.; Amagasa, T. Epidermal growth factor receptor gene copy number aberration at the primary tumour is significantly associated with extracapsular spread in oral cancer. Br. J. Cancer 2011, 104, 850–855. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Suton, P.; Salaric, I.; Granic, M.; Mueller, D.; Luksic, I. Prognostic significance of extracapsular spread of lymph node metastasis from oral squamous cell carcinoma in the clinically negative neck. Int. J. Oral Maxillofac. Surg. 2017, 46, 669–675. [Google Scholar] [CrossRef]
- Mair, M.D.; Shetty, R.; Nair, D.; Mathur, Y.; Nair, S.; Deshmukh, A.; Thiagarajan, S.; Pantvaidya, G.; Lashkar, S.; Prabhash, K.; et al. Depth of invasion, size and number of metastatic nodes predicts extracapsular spread in early oral cancers with occult metastases. Oral Oncol. 2018, 81, 95–99. [Google Scholar] [CrossRef]
- Agarwal, J.P.; Kane, S.; Ghosh-Laskar, S.; Pilar, A.; Manik, V.; Oza, N.; Wagle, P.; Gupta, T.; Budrukkar, A.; Murthy, V.; et al. Extranodal extension in resected oral cavity squamous cell carcinoma: More to it than meets the eye. Laryngoscope 2019, 129, 1130–1136. [Google Scholar] [CrossRef]
- Mermod, M.; Tolstonog, G.; Simon, C.; Monnier, Y. Extracapsular spread in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol. 2016, 62, 60–71. [Google Scholar] [CrossRef]
- Evans, M.; Baddour, H.M., Jr.; Magliocca, K.R.; Müller, S.; Nannapaneni, S.; Chen, A.Y.; Kim, S.; Chen, Z.; Shin, D.M.; Wang, A.Y.; et al. Prognostic implications of peritumoral vasculature in head and neck cancer. Cancer Med. 2019, 8, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.T.; Chen, Y.F.; Lin, S.C.; Chang, K.W.; Li, W.C. Targeting Cellular Metabolism Modulates Head and Neck Oncogenesis. Int. J. Mol. Sci. 2019, 20, 3960. [Google Scholar] [CrossRef]
- Washio, J.; Takahashi, N. Metabolomic Studies of Oral Biofilm, Oral Cancer, and Beyond. Int. J. Mol. Sci. 2016, 17, 870. [Google Scholar] [CrossRef] [PubMed]
- Musharraf, S.G.; Shahid, N.; Naqvi, S.M.A.; Saleem, M.; Siddiqui, A.J.; Ali, A. Metabolite Profiling of Preneoplastic and Neoplastic Lesions of Oral Cavity Tissue Samples Revealed a Biomarker Pattern. Sci. Rep. 2016, 6, 38985. [Google Scholar] [CrossRef] [PubMed]
- Curry, J.; Tassone, P.; Gill, K.; Tuluc, M.; BarAd, V.; Mollaee, M.; Whitaker-Menezes, D.; Rodeck, U.; Luginbuhl, A.; Cognetti, D.; et al. Tumor Metabolism in the Microenvironment of Nodal Metastasis in Oral Squamous Cell Carcinoma. Otolaryngol. Head Neck Surg. 2017, 157, 798–807. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Yang, X.; Zhou, J.; Chen, S.; Li, X.; Jian, F.; Deng, P.; Li, W. Analysis of plasma metabolic biomarkers in the development of 4-nitroquinoline-1-oxide-induced oral carcinogenesis in rats. Oncol. Lett. 2015, 9, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Rivera, C.; Oliveira, A.K.; Costa, R.A.P.; De Rossi, T.; Leme, A.F.P. Prognostic biomarkers in oral squamous cell carcinoma: A systematic review. Oral Oncol. 2017, 72, 38–47. [Google Scholar] [CrossRef]
- Shin, J.M.; Kamarajan, P.; Fenno, J.C.; Rickard, A.H.; Kapila, Y.L. Metabolomics of Head and Neck Cancer: A Mini-Review. Front. Physiol. 2016, 7, 526. [Google Scholar] [CrossRef]
- Jiang, C.Y.; Yang, K.M.; Yang, L.; Miao, Z.X.; Wang, Y.H.; Zhu, H.B. A (1)H NMR-Based Metabonomic Investigation of Time-Related Metabolic Trajectories of the Plasma, Urine and Liver Extracts of Hyperlipidemic Hamsters. PLoS ONE 2013, 8, e66786. [Google Scholar] [CrossRef]
- Bag, S.; Banerjee, D.R.; Basak, A.; Das, A.K.; Pal, M.; Banerjee, R.; Paul, R.R.; Chatterjee, J. NMR ((1)H and (13)C) based signatures of abnormal choline metabolism in oral squamous cell carcinoma with no prominent Warburg effect. Biochem. Biophys. Res. Commun. 2015, 459, 574–578. [Google Scholar] [CrossRef]
- Gupta, A.; Gupta, S.; Mahdi, A.A. (1)H NMR-derived serum metabolomics of leukoplakia and squamous cell carcinoma. Clin. Chim. Acta 2015, 441, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Melone, M.A.B.; Valentino, A.; Margarucci, S.; Galderisi, U.; Giordano, A.; Peluso, G. The carnitine system and cancer metabolic plasticity. Cell Death Dis. 2018, 9, 228. [Google Scholar] [CrossRef] [PubMed]
- Corbet, C. Stem Cell Metabolism in Cancer and Healthy Tissues: Pyruvate in the Limelight. Front. Pharmacol. 2017, 8, 958. [Google Scholar] [CrossRef] [PubMed]
- Rauckhorst, A.J.; Taylor, E.B. Mitochondrial pyruvate carrier function and cancer metabolism. Curr. Opin. Genet. Dev. 2016, 38, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Le, A. Glutamine Metabolism in Cancer. Adv. Exp. Med. Biol. 2018, 1063, 13–32. [Google Scholar]
- Weinberg, J.M.; Bienholz, A.; Venkatachalam, M.A. The role of glycine in regulated cell death. Cell. Mol. Life Sci. 2016, 73, 2285–2308. [Google Scholar] [CrossRef]
- Brooks, G.A. The Science and Translation of Lactate Shuttle Theory. Cell Metab. 2018, 27, 757–785. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | Plasma | Urine | |||
|---|---|---|---|---|---|
| Normal | Tumor | ||||
| Patient Number | 110 | 37 | 36 | 44 | 98 |
| Stage I ENE(-) | 18 | -- | -- | 7 | 16 |
| Stage II ENE(-) | 25 | 5 | 4 | 15 | 23 |
| Stage III ENE(-) | 15 | 4 | 3 | 4 | 12 |
| Stage IV ENE(-) | 28 | 15 | 17 | 9 | 26 |
| Stage IV ENE(+) | 24 | 13 | 12 | 9 | 21 |
| Tumor | Area (cm)2 | Volume (cm)3 | Invasion Depth (cm) | Lymph Nodes (Number) with ENE | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| stage I ENE(-) | 1.3 | ± | 0.9 | 0.7 | ± | 0.9 | 0.45 | ± | 0.27 | -- | ||
| stage II ENE(-) | 5.0 | ± | 2.9 | 6.2 | ± | 5.7 | 1.06 | ± | 0.46 | -- | ||
| stage III ENE(-) | 8.7 | ± | 5.4 | 11.9 | ± | 10.2 | 1.06 | ± | 0.54 | -- | ||
| stage IV ENE(-) | 15.7 | ± | 10.1 | 47.3 | ± | 48.1 | 2.23 | ± | 1.45 | -- | ||
| stage IV ENE(+) | 17.9 | ± | 16.4 | 61.3 | ± | 83.7 | 2.38 | ± | 1.77 | 2.9 | ± | 2.5 |
| OSCC Tissue | Metabolites | VIP Score | Fold Change (Tumor/Normal) | p-Value (T-Test) | |
|---|---|---|---|---|---|
| Stage IV ENE(-) | Increased | Acetone | 1.40 | 2.08 | 0.003 |
| Adenosine | 1.10 | 3.28 | 0.030 | ||
| Alanine | 1.19 | 1.86 | 0.001 | ||
| Aspartate | 1.52 | 1.79 | 0.001 | ||
| Choline | 1.87 | 2.96 | 4.13 × 10−7 | ||
| Glutamate | 2.02 | 3.61 | 1.25 × 10−6 | ||
| Glycine | 1.92 | 3.78 | 0.001 | ||
| Guanosine | 1.70 | 2.90 | 1.81 × 10−4 | ||
| Isoleucine | 1.32 | 1.97 | 0.001 | ||
| Lactate | 0.94 | 1.01 | 0.032 | ||
| Leucine | 1.88 | 2.79 | 1.81 × 10−7 | ||
| Phenylalanine | 1.57 | 2.42 | 7.40 × 10−5 | ||
| Pyruvate | 0.89 | 1.67 | 0.035 | ||
| Succinate | 1.78 | 9.70 | 0.006 | ||
| Tyrosine | 1.57 | 1.89 | 8.14 × 10−5 | ||
| Valine | 1.83 | 2.55 | 1.23 × 10−7 | ||
| Decreased | Carnitine | 1.50 | 0.35 | 2.23 × 10−8 | |
| Glucose | 1.22 | 0.67 | 0.035 | ||
| Sucrose | 0.88 | 0.64 | 0.050 | ||
| Stage IV ENE(+) | Increased | Acetone | 0.97 | 1.26 | 0.044 |
| Alanine | 1.35 | 1.83 | 0.001 | ||
| Butyrate | 0.90 | 1.63 | 0.046 | ||
| Choline | 1.83 | 2.91 | 1.62 × 10−4 | ||
| Glutamate | 2.10 | 3.53 | 5.66 × 10−7 | ||
| Glutathione | 1.09 | 1.88 | 0.034 | ||
| Glycine | 2.85 | 6.79 | 3.67 × 10−6 | ||
| Isoleucine | 1.45 | 2.13 | 0.001 | ||
| Lactate | 1.41 | 1.90 | 4.04 × 10−5 | ||
| Leucine | 1.52 | 2.30 | 1.12 × 10−4 | ||
| O-Acetylcholine | 0.90 | 1.58 | 0.032 | ||
| Phenylalanine | 1.76 | 2.74 | 8.81 × 10−5 | ||
| Pyruvate | 0.98 | 1.68 | 0.036 | ||
| Tyrosine | 1.78 | 2.77 | 7.57 × 10−5 | ||
| Valine | 1.99 | 3.02 | 1.74 × 10−7 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.-K.; Lin, C.-Y.; Kang, C.-J.; Liao, C.-T.; Wang, W.-L.; Chiang, M.-H.; Yen, T.-C.; Lin, G. Nuclear Magnetic Resonance Metabolomics Biomarkers for Identifying High Risk Patients with Extranodal Extension in Oral Squamous Cell Carcinoma. J. Clin. Med. 2020, 9, 951. https://doi.org/10.3390/jcm9040951
Tsai C-K, Lin C-Y, Kang C-J, Liao C-T, Wang W-L, Chiang M-H, Yen T-C, Lin G. Nuclear Magnetic Resonance Metabolomics Biomarkers for Identifying High Risk Patients with Extranodal Extension in Oral Squamous Cell Carcinoma. Journal of Clinical Medicine. 2020; 9(4):951. https://doi.org/10.3390/jcm9040951
Chicago/Turabian StyleTsai, Cheng-Kun, Chien-Yu Lin, Chung-Jan Kang, Chun-Ta Liao, Wan-Ling Wang, Meng-Han Chiang, Tzu-Chen Yen, and Gigin Lin. 2020. "Nuclear Magnetic Resonance Metabolomics Biomarkers for Identifying High Risk Patients with Extranodal Extension in Oral Squamous Cell Carcinoma" Journal of Clinical Medicine 9, no. 4: 951. https://doi.org/10.3390/jcm9040951
APA StyleTsai, C.-K., Lin, C.-Y., Kang, C.-J., Liao, C.-T., Wang, W.-L., Chiang, M.-H., Yen, T.-C., & Lin, G. (2020). Nuclear Magnetic Resonance Metabolomics Biomarkers for Identifying High Risk Patients with Extranodal Extension in Oral Squamous Cell Carcinoma. Journal of Clinical Medicine, 9(4), 951. https://doi.org/10.3390/jcm9040951