Acute Kidney Injury Patterns Following Transplantation of Steatotic Liver Allografts

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Methods
3. Results
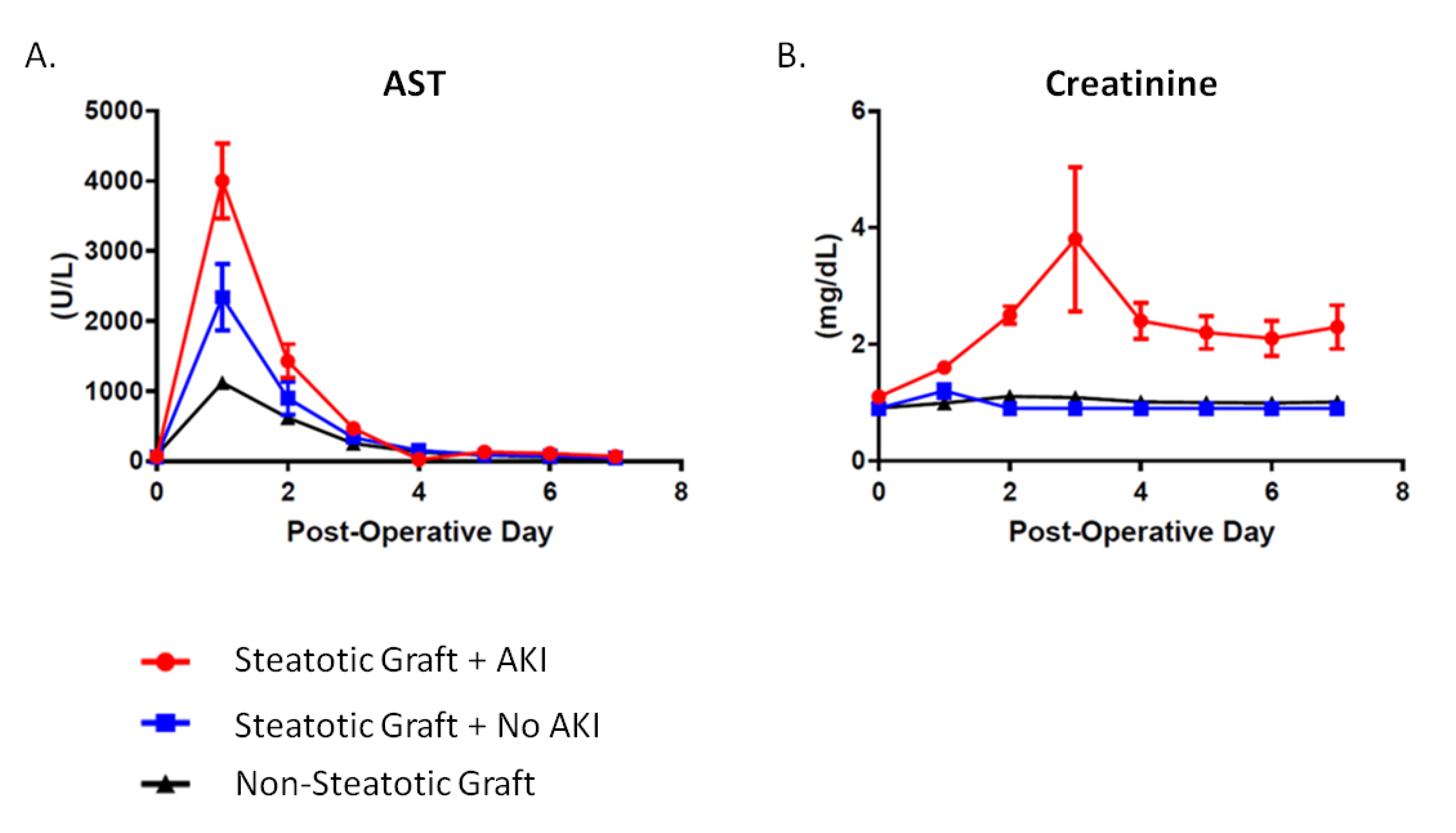
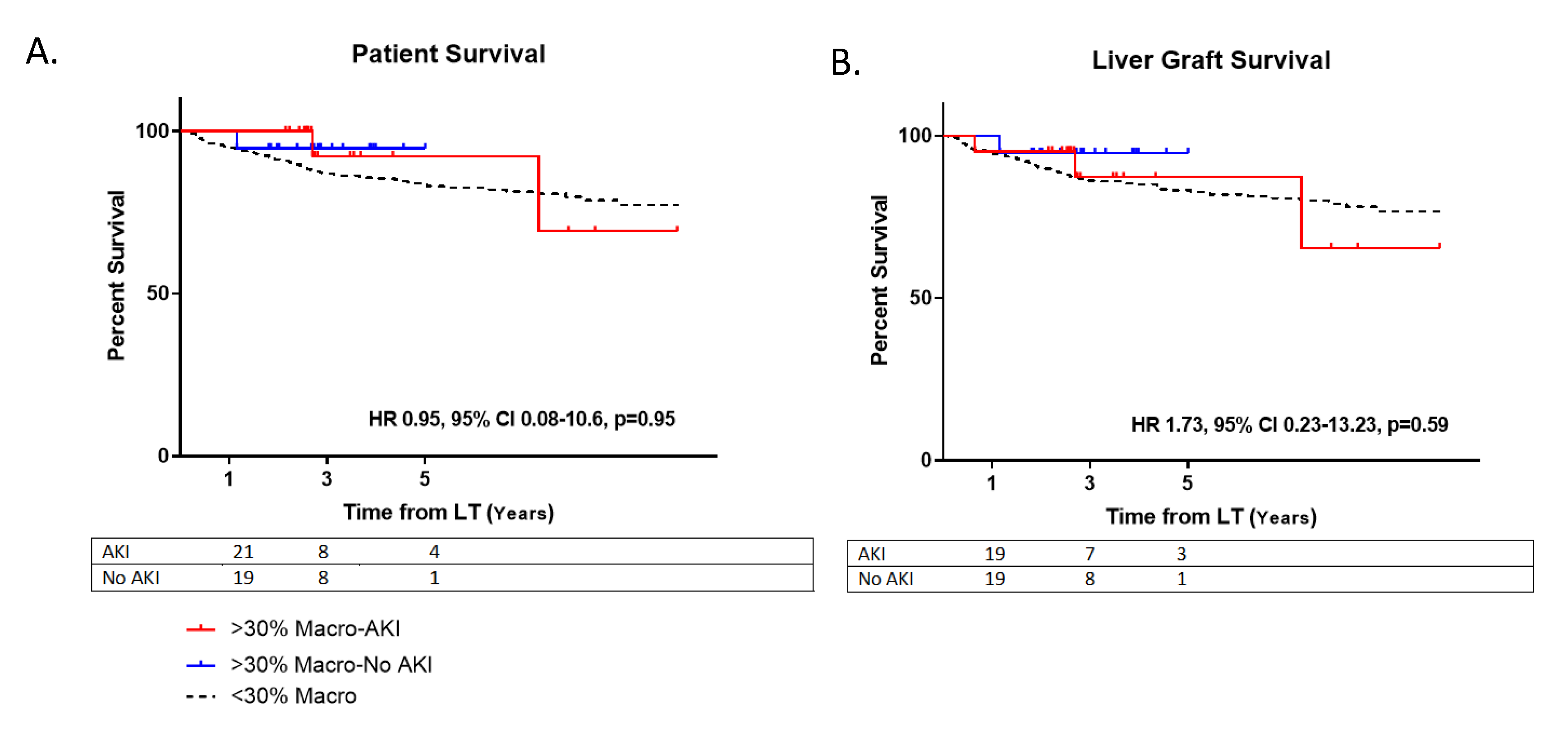
3.1. Postoperative Outcomes
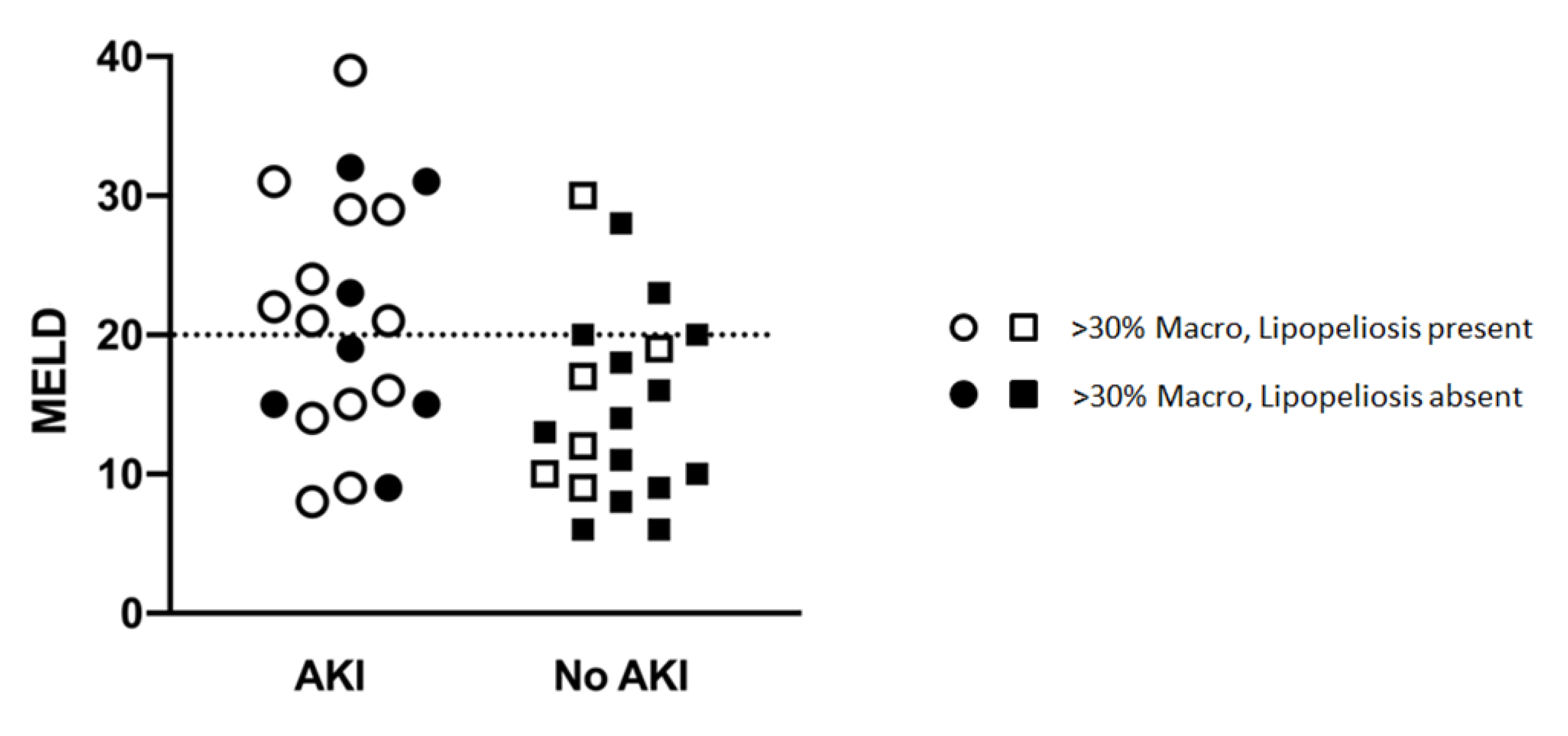
3.2. Moderately Steatotic Graft Subgroup Analysis
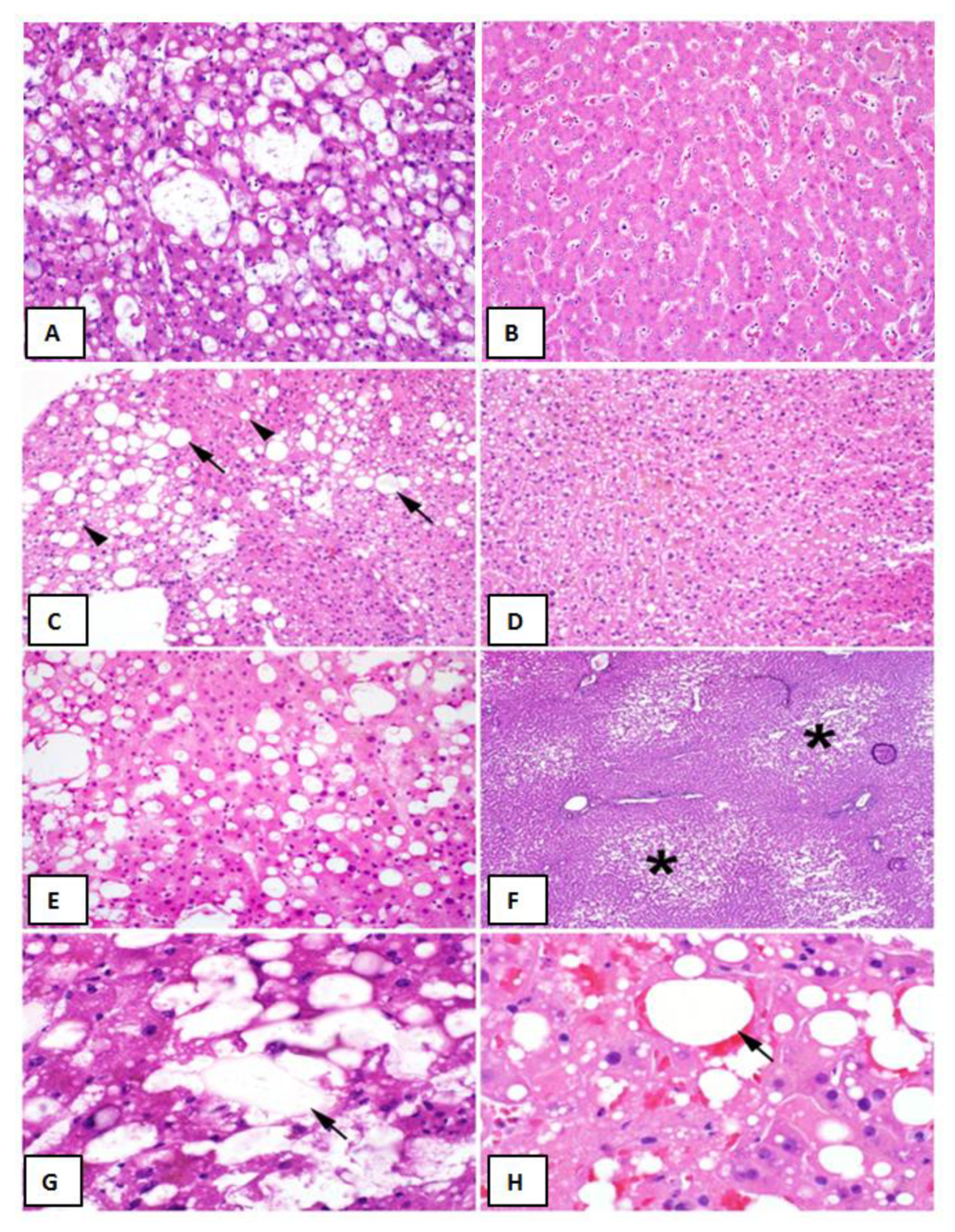
3.3. Liver Graft Biopsy Findings
4. Discussion
Author Contributions
Conflicts of Interest
References
- Verran, D.; Kusyk, T.; Painter, D.; Fisher, J.; Koorey, D.; Strasser, S.; Stewart, G.; McCaughan, G. Clinical experience gained from the use of 120 steatotic donor livers for orthotopic liver transplantation. Liver Transpl. 2003, 9, 500–505. [Google Scholar] [CrossRef]
- Selzner, M.; Clavien, P.A. Fatty liver in liver transplantation and surgery. Semin. Liver Dis. 2001, 21, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Lu, C.; Xu, C. Short-term and long-term outcomes of liver transplantation using moderately and severely steatotic donor livers: A systemic review. Medicine (Baltimore) 2018, 97, e12026. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, A.L.; Lao, O.B.; Dick, A.A.; Bakthavatsalam, R.; Halldorson, J.B.; Yeh, M.M.; Upton, M.P.; Reyes, J.D.; Perkins, J.D. The biopsied donor liver: Incorporating macrosteatosis into high-risk donor assessment. Liver Transpl. 2010, 16, 874–884. [Google Scholar] [CrossRef] [PubMed]
- Wadei, H.M.; Lee, D.D.; Croome, K.P.; Mai, M.L.; Golan, E.; Brotman, R.; Keaveny, A.P.; Taner, C.B. Early Allograft Dysfunction After Liver Transplantation Is Associated With Short- and Long-Term Kidney Function Impairment. Am. J. Transplant. 2016, 16, 850–859. [Google Scholar] [CrossRef]
- Fishbein, T.M.; Fiel, M.I.; Emre, S.; Cubukcu, O.; Guy, S.R.; Schwartz, M.E.; Miller, C.M.; Sheiner, P.A. Use of livers with microvesicular fat safely expands the donor pool. Transplantation 1997, 64, 248–251. [Google Scholar] [CrossRef]
- Croome, K.P.; Lee, D.D.; Croome, S.; Chadha, R.; Livingston, D.; Abader, P.; Keaveny, A.P.; Taner, C.B. The impact of postreperfusion syndrome during liver transplantation using livers with significant macrosteatosis. Am. J. Transpl. 2019, 19, 2550–2559. [Google Scholar] [CrossRef]
- McCormack, L.; Dutkowski, P.; El-Badry, A.M.; Clavien, P.A. Liver transplantation using fatty livers: Always feasible? J. Hepatol. 2011, 54, 1055–1062. [Google Scholar] [CrossRef]
- Hall, A.R.; Dhillon, A.P.; Green, A.C.; Ferrell, L.; Crawford, J.M.; Alves, V.; Balabaud, C.; Bhathal, P.; Bioulac-Sage, P.; Guido, M.; et al. Hepatic steatosis estimated microscopically versus digital image analysis. Liver Int. 2013, 33, 926–935. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; Zuckermann, A.; Macdonald, P.; Leprince, P.; Esmailian, F.; Luu, M.; Mancini, D.; Patel, J.; Razi, R.; Reichenspurner, H.; et al. Report from a consensus conference on primary graft dysfunction after cardiac transplantation. J. Heart Lung Transpl. 2014, 33, 327–340. [Google Scholar] [CrossRef]
- Doyle, M.M.; Vachharajani, N.; Wellen, J.R.; Anderson, C.D.; Lowell, J.A.; Shenoy, S.; Brunt, E.M.; Chapman, W.C. Short- and long-term outcomes after steatotic liver transplantation. Arch Surg. 2010, 145, 653–660. [Google Scholar] [CrossRef]
- Leithead, J.A.; Rajoriya, N.; Gunson, B.K.; Muiesan, P.; Ferguson, J.W. The evolving use of higher risk grafts is associated with an increased incidence of acute kidney injury after liver transplantation. J. Hepatol. 2014, 60, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Cabezuelo, J.B.; Ramirez, P.; Acosta, F.; Bueno, F.S.; Robles, R.; Pons, J.A.; Miras, M.; Munitiz, V.; Fernandez, J.A.; Lujan, J.; et al. Prognostic factors of early acute renal failure in liver transplantation. Transpl. Proc. 2002, 34, 254–255. [Google Scholar] [CrossRef]
- O’Riordan, A.; Wong, V.; McQuillan, R.; McCormick, P.A.; Hegarty, J.E.; Watson, A.J. Acute renal disease, as defined by the RIFLE criteria, post-liver transplantation. Am. J. Transpl. 2007, 7, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Leithead, J.A.; Armstrong, M.J.; Corbett, C.; Andrew, M.; Kothari, C.; Gunson, B.K.; Muiesan, P.; Ferguson, J.W. Hepatic ischemia reperfusion injury is associated with acute kidney injury following donation after brain death liver transplantation. Transpl. Int. 2013, 26, 1116–1125. [Google Scholar] [CrossRef]
- Ferrell, L.; Bass, N.; Roberts, J.; Ascher, N. Lipopeliosis: Fat induced sinusoidal dilation in transplanted liver mimicking peliosis hepatitis. J. Clin. Pathol. 1992, 45, 1109–1110. [Google Scholar] [CrossRef] [PubMed]
- Cha, I.; Bass, N.; Ferrell, L.D. Lipopeliosis: An Immunohistochemical and Clinicopathologic Study of Five Cases. Am. J. Surg. Pathol. 1994, 18, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, D.M.; Smith, M.L.; Seamans, D.P.; Giorgakis, E.; Gaitan, B.D.; Khurmi, N.; Aqel, B.A.; Reddy, K.S. Fatal diffuse pulmonary fat microemboli following reperfusion in orthotopic liver transplantation with the use of marginal steatotic allografts. Am. J. Transpl. 2019, 19, 2640–2645. [Google Scholar] [CrossRef]
- Shaikh, N. Emergency management of fat embolism syndrome. J. Emergencies Trauma Shock 2009, 2, 29–33. [Google Scholar] [CrossRef]
- Glossing, H.R.; Pellegrini, V.D. Fat embolism syndrome: A review of pathology and physiological basis of treatment. Clin. Orthop. Relat. Res. 1982, 165, 68–82. [Google Scholar]
- Baker, P.L.; Paxel, J.A.; Pettier, L.F. Free fatty acids, catecholamine and arterial hypoxia in patients with fat embolism. J. Trauma 1971, 11, 1026–1030. [Google Scholar] [CrossRef] [PubMed]
- Evarts, C.M. Diagnosis and treatment of fat embolism. JAMA 1965, 194, 899–901. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Steatotic Grafts (n = 40) | Non-Steatotic Grafts (n = 471) | p Value | |
|---|---|---|---|
| Pre-Liver Transplant | |||
| Steatosis (%) | 41.1 ± 15.8 | 3.8 ± 5.8 | <0.0001 |
| Recipient Age (years) | 57. 4 ± 9.7 | 56.0 ± 10.3 | 0.39 |
| Biologic MELD | 18.0 ± 8.3 | 16.1 ± 7.0 | 0.14 |
| Female | 9 (22.5%) | 155 (32.9%) | 0.18 |
| Indication for LT | 0.16 | ||
| Hepatitis C (HCV) | 6 (22.5%) | 55 (11.6%) | |
| Cholestatic | 5 (12.5%) | 53 (11.3%) | |
| Hepatocellular Carcinoma (HCC)/Other MELD Exception | 11 (27.5%) | 223 (47.3%) | |
| Alcohol-Related Liver Disease (ALD) | 8 (20.0%) | 46 (9.8%) | |
| Nonalcoholic Steatohepatitis (NASH) | 6 (15.0%) | 49 (10.4%) | |
| Other | 4 (10.0%) | 45 (9.6%) | |
| Pre-LT Creatinine (mg/dL) | 1.0 ± 0.3 | 0.9 ± 0.9 | 0.14 |
| Pre-LT eGFR | 57.7 ± 6.3 | 57.7 ± 6.6 | 0.97 |
| Post-Liver Transplant | |||
| Post-LT AKI | 21 (52.5%) | 79 (16.8%) | <0.0001 |
| Post-LT Temporary Dialysis | 4 (10.0%) | 5 (1.1%) | 0.003 |
| ICU LOS (days) | 2.0 ± 1.8 | 1.8 ± 2.6 | 0.62 |
| Total Hospital LOS (days) | 9.1 ± 10.3 | 9.9 ± 10.9 | 0.67 |
| One-Year Post-Liver Transplant | |||
| Creatinine (mg/dL) | 1.3 ± 0.3 | 1.3 ± 0.7 | 0.97 |
| eGFR (mL/min) | 53.1 ± 7.9 | 53.5 ± 10.1 | 0.70 |
| New Chronic Post-LT Dialysis | 0 (0.0%) | 2 (0.4%) | >0.99 |
| Post-LT AKI (n = 21) | No AKI (n = 19) | p Value | |
|---|---|---|---|
| Pre-Liver Transplant | |||
| Macrovesicular Steatosis (%) | 41.9 ± 15.7 | 40.3 ± 16.2 | 0.75 |
| Recipient Age (years) | 56.7 ± 8.3 | 58.3 ± 11.3 | 0.61 |
| Biologic MELD | 20.5 ± 8.9 | 15.3 ± 6.9 | 0.04 |
| Female | 3 (14.3%) | 6 (31.6%) | 0.43 |
| Indication for LT | 0.53 | ||
| HCV | 4 (19.0%) | 2 (10.5%) | |
| Cholestatic | 1 (4.8%) | 4 (21.1%) | |
| HCC/Other MELD Exception | 5 (23.8%) | 6 (31.6%) | |
| ALD | 4 (19.0%) | 4 (21.1%) | |
| NASH | 4 (19.0%) | 2 (10.5%) | |
| Other | 3 (14.3%) | 1 (5.3%) | |
| Total Hospital LOS (median) | 10.4 ± 13.5 (7.0) | 7.1 ± 4.1 (6.0) | 0.32 |
| One-Year Post-LT | |||
| Creatinine (mg/dL) | 1.3 ± 0.2 | 1.2 ± 0.4 | 0.27 |
| eGFR (mL/min) | 52.7 ± 6.9 | 53.6 ± 9.1 | 0.74 |
| Post-LT AKI (n = 21) | No AKI (n = 19) | p Value | |
|---|---|---|---|
| CIT (h) | 6.8 ± 2.1 | 6.1 ± 1.7 | 0.28 |
| EBL (mL) | 2157 ± 1649 | 1821 ± 1405 | 0.49 |
| Pre-Anhepatic | |||
| SBP (mmHg) | 111.2 ± 21.8 | 104.2 ± 14.5 | 0.25 |
| MAP | 75.1 ± 13.3 | 73.8 ± 13.6 | 0.76 |
| Inotrope Score | 4.1 ± 11.9 | 1.7 ± 6.9 | 0.45 |
| Anhepatic | |||
| SBP (mmHg) | 106.5 ± 15.4 | 104.4 ± 15.1 | 0.67 |
| MAP | 75.4 ± 11.0 | 76.7 ± 9.6 | 0.71 |
| Inotrope Score | 4.3 ± 11.9 | 2.6 ± 6.8 | 0.58 |
| Post Reperfusion | |||
| SBP (mmHg) | 95.6 ± 13.8 | 96.2 ± 7.9 | 0.87 |
| MAP | 67.0 ± 11.8 | 65.5 ± 9.8 | 0.69 |
| Inotrope Score | 19.5 ± 20.0 | 3.8 ± 4.4 | 0.03 |
| Post-LT AKI (n = 21) | No AKI (n = 19) | p Value | |
|---|---|---|---|
| Macrovesicular Steatosis | |||
| Large Droplet (%) | 69.2 ± 16.1 | 64.7 ± 16.9 | 0.41 |
| Small Droplet (%) | 30.8 ± 16.1 | 35.3 ± 16.9 | |
| Microvesicular Steatosis | 0 (0.0%) | 4 (21.1%) | 0.04 |
| Zonation | 14 (66.7%) | 11 (57.9%) | 0.75 |
| Inflammation | 5 (23.8%) | 6 (31.5%) | 0.73 |
| Ballooning | 2 (9.5%) | 3 (15.8%) | 0.65 |
| Mallory Hyaline | 0 (0.0%) | 0 (0.0%) | - |
| Lipopeliosis | 13 (61.9%) | 6 (31.6%) | 0.03 |
| Effect | Odds Ratio | 95% CI | p Value | |
|---|---|---|---|---|
| Donor Age | 0.93 | 0.87 | 0.99 | 0.02 |
| Lipopeliosis | 6.04 | 1.05 | 34.61 | 0.04 |
| Post-Reperfusion Systolic BP | 1.01 | 0.95 | 1.08 | 0.75 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jadlowiec, C.; Smith, M.; Neville, M.; Mao, S.; Abdelwahab, D.; Reddy, K.; Moss, A.; Aqel, B.; Taner, T. Acute Kidney Injury Patterns Following Transplantation of Steatotic Liver Allografts. J. Clin. Med. 2020, 9, 954. https://doi.org/10.3390/jcm9040954
Jadlowiec C, Smith M, Neville M, Mao S, Abdelwahab D, Reddy K, Moss A, Aqel B, Taner T. Acute Kidney Injury Patterns Following Transplantation of Steatotic Liver Allografts. Journal of Clinical Medicine. 2020; 9(4):954. https://doi.org/10.3390/jcm9040954
Chicago/Turabian StyleJadlowiec, Caroline, Maxwell Smith, Matthew Neville, Shennen Mao, Dina Abdelwahab, Kunam Reddy, Adyr Moss, Bashar Aqel, and Timucin Taner. 2020. "Acute Kidney Injury Patterns Following Transplantation of Steatotic Liver Allografts" Journal of Clinical Medicine 9, no. 4: 954. https://doi.org/10.3390/jcm9040954
APA StyleJadlowiec, C., Smith, M., Neville, M., Mao, S., Abdelwahab, D., Reddy, K., Moss, A., Aqel, B., & Taner, T. (2020). Acute Kidney Injury Patterns Following Transplantation of Steatotic Liver Allografts. Journal of Clinical Medicine, 9(4), 954. https://doi.org/10.3390/jcm9040954