The Effects of SJP-001 on Alcohol Hangover Severity: A Pilot Study



Abstract
1. Introduction
2. Methods
2.1. Subjects
2.2. Procedures
2.3. Assessment of Hangover Severity
2.4. Statistical Analysis
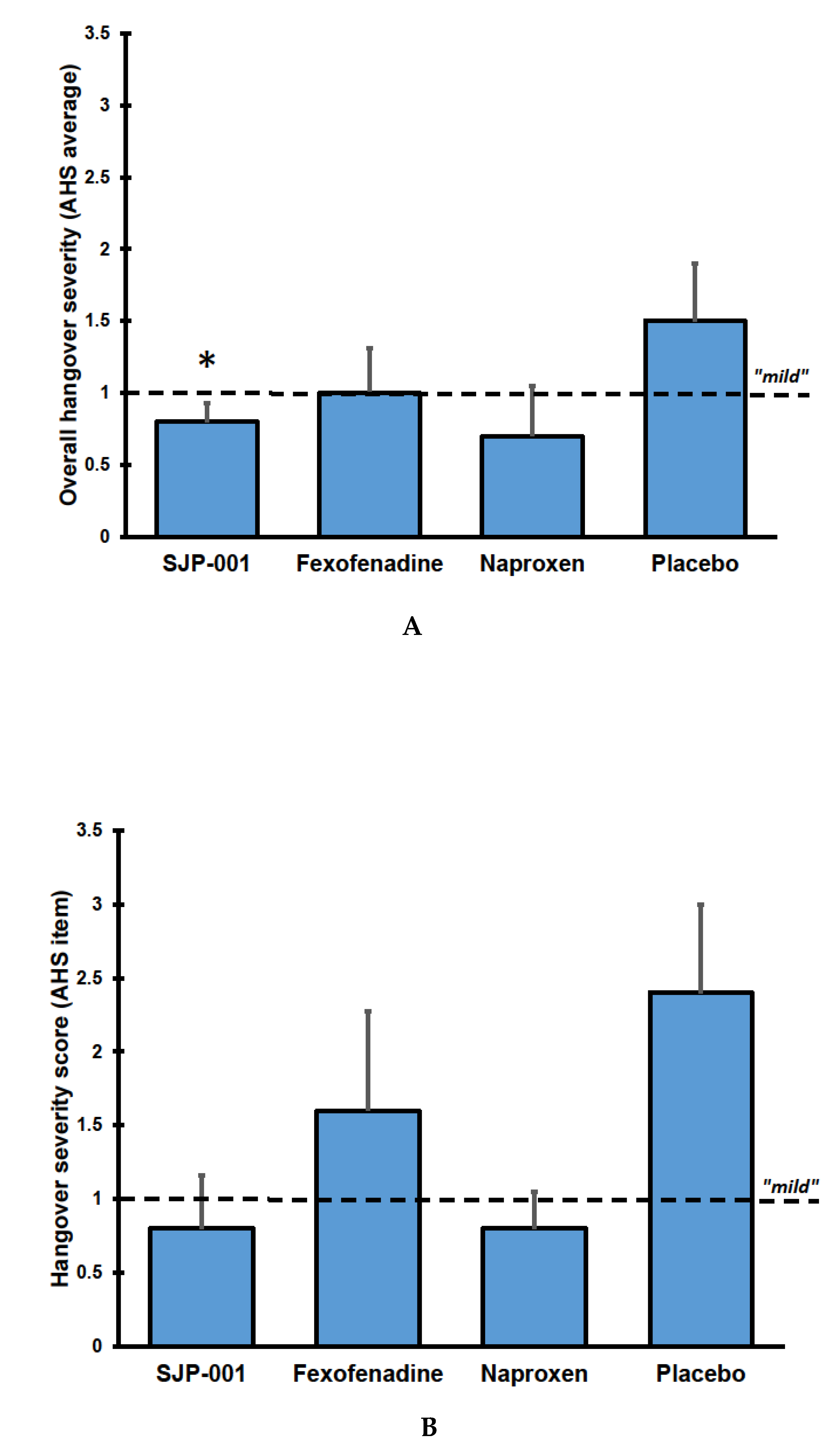
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Van Schrojenstein Lantman, M.; van de Loo, A.J.; Mackus, M.; Verster, J.C. Development of a definition for the alcohol hangover: Consumer descriptions and expert consensus. Curr. Drug Abus. Rev. 2016, 9, 148–154. [Google Scholar] [CrossRef]
- Verster, J.C.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. Updating the definition of the alcohol hangover. J. Clin. Med. 2020, 9, 823. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Kruisselbrink, L.D.; Slot, K.A.; Anogeianaki, A.; Adams, S.; Alford, C.; Arnoldy, L.; Ayre, E.; Balikji, S.; Benson, S.; et al. Sensitivity to experiencing alcohol hangovers: Reconsideration of the 0.11% blood alcohol concentration (BAC) threshold for having a hangover. J. Clin. Med. 2020, 9, 179. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Kruisselbrink, L.D.; Anogeianaki, A.; Alford, C.; Stock, A.K. Relationship of alcohol hangover and physical endurance performance: Walking the Samaria Gorge. J. Clin. Med. 2020, 9, 114. [Google Scholar] [CrossRef] [PubMed]
- Penning, R.; McKinney, A.; Verster, J.C. Alcohol hangover symptoms and their contribution to overall hangover severity. Alcohol Alcohol. 2012, 47, 248–252. [Google Scholar] [CrossRef]
- Van Schrojenstein Lantman, M.; Mackus, M.; van de Loo, A.J.A.E.; Verster, J.C. The impact of alcohol hangover symptoms on cognitive and physical functioning, and mood. Hum. Psychopharmacol. 2017, 32, e2623. [Google Scholar] [CrossRef]
- Gunn, C.; Mackus, M.; Griffin, C.; Munafò, M.R.; Adams, S. A systematic review of the next-day effects of heavy alcohol consumption on cognitive performance. Addiction 2018, 113, 2182–2193. [Google Scholar] [CrossRef]
- McKinney, A. A review of the next day effects of alcohol on subjective mood ratings. Curr. Drug Abus. Rev. 2010, 3, 88–91. [Google Scholar] [CrossRef]
- Frone, M.R. Employee psychoactive substance involvement: Historical context, key findings, and future directions. Annu. Rev. Organ. Psychol. Organ. Behav. 2019, 6, 273–297. [Google Scholar] [CrossRef]
- Verster, J.C. Alcohol hangover effects on driving and flying. Int. J. Disabil. Hum. Dev. 2007, 6, 361–367. [Google Scholar] [CrossRef]
- Verster, J.C.; Bervoets, A.C.; de Klerk, S.; Vreman, R.A.; Olivier, B.; Roth, T.; Brookhuis, K.A. Effects of alcohol hangover on simulated highway driving performance. Psychopharmacology 2014, 231, 2999–3008. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; van der Maarel, M.; McKinney, A.; Olivier, B.; de Haan, L. Driving during alcohol hangover among Dutch professional truck drivers. Traffic Inj. Prev. 2014, 15, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Sacks, J.J.; Gonzales, K.R.; Bouchery, E.E.; Tomedi, L.E.; Brewer, R.D. 2010 National and State Costs of Excessive Alcohol Consumption. Am. J. Prev. Med. 2015, 49, e73–e79. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, A. Financial Headache: The Cost of Workplace Hangovers and Intoxication to the UK Economy; Institute of Alcohol Studies: London, UK, 2019. [Google Scholar]
- Mackus, M.; van Schrojenstein Lantman, M.; van de Loo, A.J.A.E.; Nutt, D.J.; Verster, J.C. An effective hangover treatment: Friend or foe? Drug Sci. Policy Law 2017. [Google Scholar] [CrossRef]
- Pittler, M.H.; Verster, J.C.; Ernst, E. Interventions for preventing or treating alcohol hangover: Systematic review of randomized trials. Br. Med. J. 2005, 331, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; Penning, R. Treatment and prevention of alcohol hangover. Curr. Drug Abus. Rev. 2010, 3, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Jayawardena, R.; Thejani, T.; Ranasinghe, P.; Fernando, D.; Verster, J.C. Interventions for treatment and/or prevention of alcohol hangover: Systematic review. Hum. Psychopharmacol. 2017, 32, e2600. [Google Scholar] [CrossRef]
- Penning, R.; van Nuland, M.; Fliervoet, L.A.L.; Olivier, B.; Verster, J.C. The pathology of alcohol hangover. Curr. Drug Abus. Rev. 2010, 3, 68–75. [Google Scholar] [CrossRef]
- Tipple, C.T.; Benson, S.; Scholey, A. A review of the physiological factors associated with alcohol hangover. Curr. Drug Abus. Rev. 2016, 9, 93–98. [Google Scholar] [CrossRef]
- Palmer, E.; Tyacke, R.; Sastre, M.; Lingford-Hughes, A.; Nutt, D.; Ward, R.J. Alcohol Hangover: Underlying Biochemical, Inflammatory and Neurochemical Mechanisms. Alcohol Alcohol. 2019, 54, 196–203. [Google Scholar] [CrossRef]
- Van de Loo, A.J.A.E.; Mackus, M.; Korte-Bouws, G.A.H.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Urine ethanol concentration and alcohol hangover severity. Psychopharmacology 2017, 234, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Van de Loo, A.J.A.E.; Knipping, K.; Mackus, M.; Kraneveld, A.D.; Garssen, J.; Scholey, A.; Bruce, G.; Verster, J.C. Differential effects on acute saliva cytokine response following alcohol consumption and alcohol hangover: Preliminary results from two independent studies. Alcohol. Clin. Exp. Res. 2018, 42, 20A. [Google Scholar]
- Mackus, M.; van Schrojenstein Lantman, M.; van de Loo, A.J.A.E.; Brookhuis, K.A.; Kraneveld, A.D.; Garssen, J.; Verster, J.C. Alcohol metabolism in hangover sensitive versus hangover resistant social drinkers. Drug Alcohol Depend. 2018, 185, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Wiese, J.; McPherson, S.; Odden, M.C.; Shlipak, M.G. Effect of Opuntia ficus indica on symptoms of the alcohol hangover. Arch. Intern. Med. 2004, 164, 1334–1340. [Google Scholar] [CrossRef]
- Parantainen, J. Prostaglandins in alcohol intolerance and hangover. Drug Alcohol Depend. 1983, 11, 239–248. [Google Scholar] [CrossRef]
- Kaivola, S.; Parantainen, J.; Osterman, T.; Timonen, H. Hangover headache and prostaglandins: Prophylactic treatment with tolfenamic acid. Cephalalgia 1983, 3, 31–36. [Google Scholar] [CrossRef]
- Kim, D.J.; Kim, W.; Yoon, S.J.; Choi, B.M.; Kim, J.S.; Go, H.J.; Kim, Y.K.; Jeong, J. Effects of alcohol hangover on cytokine production in healthy subjects. Alcohol 2003, 31, 167–170. [Google Scholar] [CrossRef]
- Mandrekar, P.; Catalano, D.; Girouard, L.; Szabo, G. Human monocyte IL-10 production is increased by acute ethanol treatment. Cytokine 1996, 8, 567–577. [Google Scholar] [CrossRef]
- Szabo, G.; Mandrekar, P.; Girouard, L.; Catalano, D. Regulation of human monocyte functions by acute ethanol treatment: Decreased tumor necrosis factor-alpha, interleukin-1 beta and elevated interleukin-10, and transforming growth factor-beta production. Alcohol. Clin. Exp. Res. 1996, 20, 900–907. [Google Scholar] [CrossRef]
- Zimatkin, S.M.; Anichtchik, O.V. Alcohol-histamine interactions. Alcohol Alcohol. 1999, 34, 141–147. [Google Scholar] [CrossRef]
- Antonova, M.; Wienecke, T.; Olesen, J.; Ashina, M. Prostaglandins in migraine: Update. Curr. Opin. Neurol. 2013, 26, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Harmer, I.M.; Harris, K.E. Observations on the vascular reactions in man in response to histamine. Heart 1926, 13, 381–394. [Google Scholar]
- Worm, J.; Falkenberg, K.; Olesen, J. Histamine and migraine revisited: Mechanisms and possible drug targets. J. Headache Pain 2019, 20, 30. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration (FDA). Naproxyn (naproxen) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/017581s113,018164s063,020067s020lbl.pdf (accessed on 10 February 2020).
- Food and Drug Administration (FDA). Allegra (Fexofenadine Hydrochloride) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2003/20786se8-014,20872se8-011,20625se8-012_allegra_lbl.pdf (accessed on 10 February 2020).
- Brogden, R.N.; Heel, R.C.; Speight, T.M.; Avery, G.S. Naproxen up to date: A review of its pharmacological properties and therapeutic efficacy and use in rheumatic diseases and pain states. Drugs 1979, 18, 241–277. [Google Scholar] [CrossRef] [PubMed]
- Amichai, B.; Grunwald, M.H.; Brenner, L. Fexofenadine hydrochloride--a new anti-histaminic drug. IMAJ 2001, 3, 207–209. [Google Scholar] [PubMed]
- Ashenager, M.S.; Grgela, T.; Aragane, Y.; Kawada, A. Inhibition of cytokine-induced expression of T-cell cytokines by antihistamines. J. Investig. Allergol. Clin. Immunol. 2007, 17, 20–26. [Google Scholar]
- Rohsenow, D.J.; Howland, J.; Minsky, S.J.; Greece, J.; Almeida, A.; Roehrs, T.A. The acute hangover scale: A new measure of immediate hangover symptoms. Addict. Behav. 2007, 32, 1314–1320. [Google Scholar] [CrossRef]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: Recommendations for good practice. J. Eval. Clin. Pract. 2004, 10, 307–312. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1–10. [Google Scholar] [CrossRef]
- Lee, E.C.; Whitehead, A.L.; Jacques, R.M.; Julious, S.A. The statistical interpretation of pilot trials: Should significance thresholds be reconsidered? BMC Med. Res. Methodol. 2014, 14, 41. [Google Scholar] [CrossRef]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef] [PubMed]
- McGlothlin, A.E.; Lewis, R.J. Minimal clinically important difference: Defining what really matters to patients. JAMA 2014, 312, 1342–1343. [Google Scholar] [CrossRef] [PubMed]
- Verster, J.C.; van de Loo, A.J.A.E.; Benson, S.; Scholey, A.; Stock, A.-K. The assessment of overall hangover severity. J. Clin. Med. 2020, 9, 786. [Google Scholar] [CrossRef]
- Rohsenow, D.J.; Howland, J. The role of beverage congeners in hangover and other residual effects of alcohol intoxication: A review. Curr. Drug Abus. Rev. 2010, 3, 76–79. [Google Scholar] [CrossRef]
- Verster, J.C.; van de Loo, A.J.A.E.; Adams, S.; Stock, A.-K.; Benson, S.; Alford, C.; Scholey, A.; Bruce, G. Advantages and limitations of naturalistic study designs and their implementation in alcohol hangover research. J. Clin. Med. 2019, 8, 2160. [Google Scholar] [CrossRef]
- Webb, W.B.; Campbell, S.S. The first night effect revisited with age as variable. Waking Sleep. 1979, 3, 319–324. [Google Scholar]
- Le Bon, O.; Staner, L.; Hoffmann, G.; Dramaix, M.; San Sebastian, I.; Murphy, J.R.; Kentos, M.; Pelc, I.; Linkowski, P. The first-night effect may last more than one night. J. Psychiatr. Res. 2001, 35, 165–172. [Google Scholar] [CrossRef]
- Devenney, L.E.; Coyle, K.B.; Roth, T.; Verster, J.C. Sleep after heavy alcohol consumption and physical activity levels during alcohol hangover. J. Clin. Med. 2019, 8, 752. [Google Scholar] [CrossRef]
- Hogewoning, A.; van de Loo, A.J.A.E.; Mackus, M.; Raasveld, S.J.; de Zeeuw, R.; Bosma, E.R.; Bouwmeester, N.H.; Brookhuis, K.A.; Garssen, J.; Verster, J.C. Characteristics of social drinkers with and without a hangover after heavy alcohol consumption. Subst. Abus. Rehabil. 2016, 7, 161–167. [Google Scholar] [CrossRef]
- Penning, R.; McKinney, A.; Bus, L.D.; Olivier, B.; Slot, K.; Verster, J.C. Measurement of alcohol hangover severity: Development of the alcohol hangover severity scale (AHSS). Psychopharmacology 2013, 225, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Slutske, W.S.; Piasecki, T.M.; Hunt-Carter, E.E. Development and initial validation of the Hangover Symptoms Scale: Prevalence and correlates of hangover symptoms in college students. Alcohol. Clin. Exp. Res. 2003, 27, 1442–1450. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall | Subject 7 | Subject 8 | Subject 9 | Subject 12 | Subject 16 | |
|---|---|---|---|---|---|---|
| Sex (male/female) | 3/2 | Male | Male | Male | Female | Female |
| Age (years) | 35.2 (9.0) | 27 | 47 | 33 | 27 | 42 |
| Weight (lb) | 170.8 (13.7) | 169.4 | 192.6 | 172.8 | 162.4 | 156.6 |
| Height (in) | 67.4 (2.6) | 67.5 | 68.9 | 70.7 | 65.5 | 64.2 |
| BMI (kg/m2) | 26.4 (1.5) | 26.1 | 28.5 | 24.3 | 26.6 | 26.7 |
| Habitual bedtime 1 (h:min) | 23:12 (0:34) | 00:00 | 23:30 | 23:00 | 22:30 | 23:00 |
| Preferred alcohol type 2 | - | Rum | Mixed 3 | Mixed 4 | Rum | Vodka |
| Units alcohol for hangover 5 | 4.6 (1.1) | 3 | 6 | 5 | 4 | 5 |
| SJP-001 | Fexofenadine | Naproxen | Placebo | |
|---|---|---|---|---|
| Units of alcohol consumed | 4.6 (1.1) | 4.6 (1.1) | 4.6 (1.1) | 4.6 (1.1) |
| BrAC (3h) (%) | 0.064 (0.034) | 0.068 (0.026) | 0.053 (0.030) | 0.072 (0.038) |
| Total sleep time (min) | 412.0 (45.9) | 377.0 (66.3) | 406.0 (59.3) | 421.0 (44.2) |
| Number of nightly awakenings | 1.6 (1.1) | 2.0 (1.4) | 1.5 (1.9) | 1.6 (1.1) |
| Sleep onset latency (min) | 34.0 (18.5) | 52.0 (30.9) * | 45.0 (17.3) | 12.2 (11.3) |
| Time awake while in bed (min) | 29.4 (30.7) | 34.2 (38.8) | 13.0 (12.9) | 36.0 (38.7) |
| Sleep quality | 7.2 (1.5) | 4.8 (3.6) | 8.3 (1.0) | 7.8 (1.6) |
| Symptoms | SJP-001 | Fexofenadine | Naproxen | Placebo |
|---|---|---|---|---|
| Hangover | 0.8 (0.8) | 1.6 (1.5) | 0.8 (0.5) | 2.4 (1.3) |
| Thirsty | 2.4 (1.8) | 1.6 (1.1) | 1.5 (2.4) | 2.8 (2.4) |
| Tired | 2.2 (1.9) | 2.4 (2.1) | 1.8 (2.1) | 2.8 (1.6) |
| Headache | 0.4 (0.5) | 1.6 (1.5) | 0.3 (0.5) | 1.6 (2.5) |
| Dizziness/faintness | 0.0 (0.0) | 0.2 (0.4) | 1.0 (2.0) | 1.0 (1.2) |
| Loss of appetite | 0.4 (0.5) | 1.0 (1.7) | 0.3 (0.5) | 1.0 (0.7) |
| Stomachache | 0.8 (1.3) | 0.4 (0.9) | 0.3 (0.5) | 0.6 (0.5) |
| Nausea | 0.4 (0.9) | 0.2 (0.4) | 0.3 (0.5) | 1.0 (1.7) |
| Heart racing | 0.4 (0.5) | 0.2 (0.4) | 0.0 (0.0) | 0.2 (0.4) |
| Mean AHS score | 0.8 (0.3) * | 1.0 (0.7) | 0.7 (0.7) | 1.5 (0.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verster, J.C.; Dahl, T.A.; Scholey, A.; Iversen, J.M. The Effects of SJP-001 on Alcohol Hangover Severity: A Pilot Study. J. Clin. Med. 2020, 9, 932. https://doi.org/10.3390/jcm9040932
Verster JC, Dahl TA, Scholey A, Iversen JM. The Effects of SJP-001 on Alcohol Hangover Severity: A Pilot Study. Journal of Clinical Medicine. 2020; 9(4):932. https://doi.org/10.3390/jcm9040932
Chicago/Turabian StyleVerster, Joris C, Thomas A Dahl, Andrew Scholey, and Jacqueline M Iversen. 2020. "The Effects of SJP-001 on Alcohol Hangover Severity: A Pilot Study" Journal of Clinical Medicine 9, no. 4: 932. https://doi.org/10.3390/jcm9040932
APA StyleVerster, J. C., Dahl, T. A., Scholey, A., & Iversen, J. M. (2020). The Effects of SJP-001 on Alcohol Hangover Severity: A Pilot Study. Journal of Clinical Medicine, 9(4), 932. https://doi.org/10.3390/jcm9040932