Prevalence and Associated Factors of Nocturnal Eating Behavior and Sleep-Related Eating Disorder-Like Behavior in Japanese Young Adults: Results of an Internet Survey Using Munich Parasomnia Screening

 , , and
, , and
Abstract
1. Introduction
2. Experimental Section
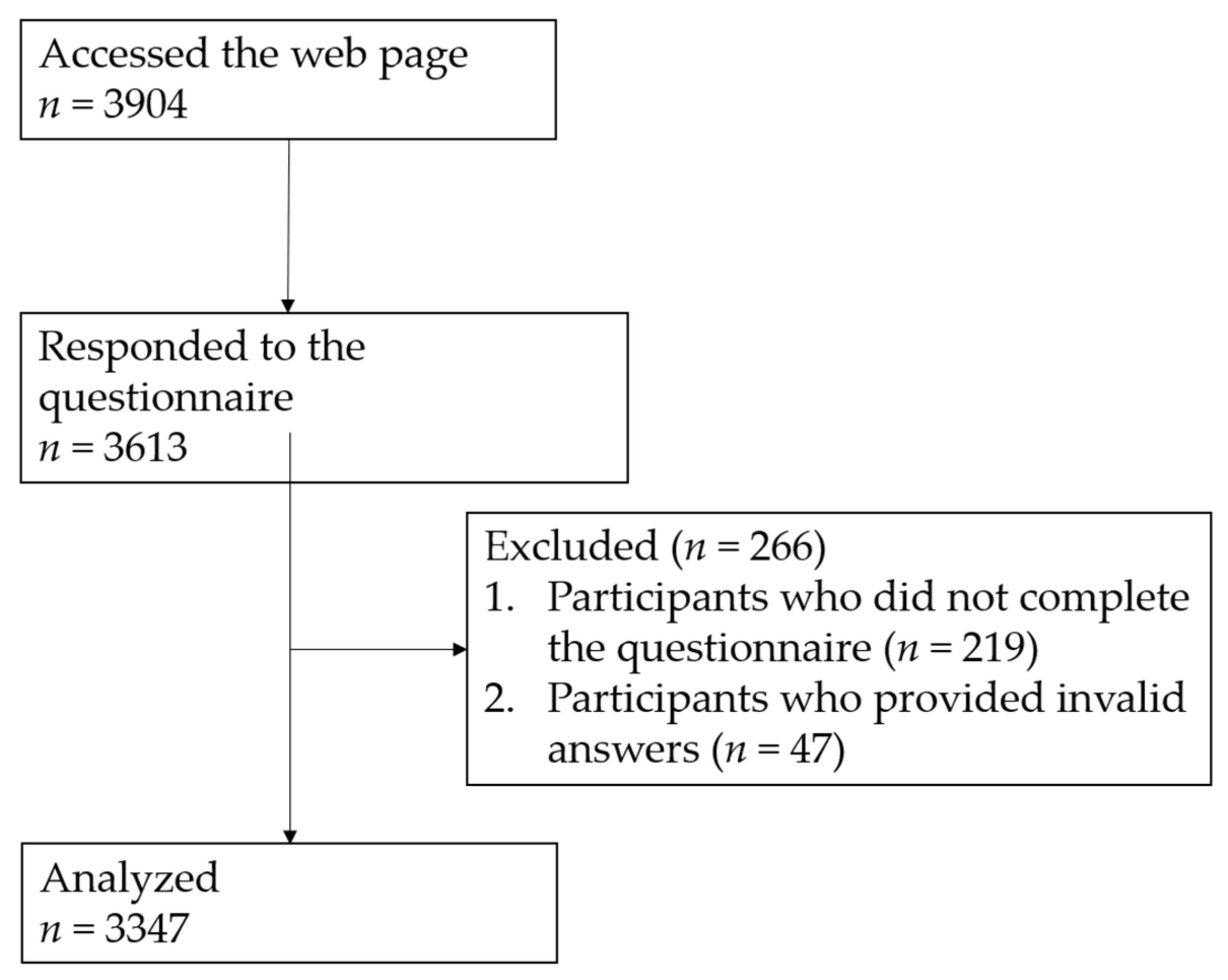
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Allison, K.C.; Lundgren, J.D.; O’Reardon, J.P.; Geliebter, A.; Gluck, M.E.; Vinai, P.; Mitchell, J.E.; Schenck, C.H.; Howell, M.J.; Crow, S.J.; et al. Proposed diagnostic criteria for night eating syndrome. Int. J. Eat. Disord. 2010, 43, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Schenck, C.H.; Mahowald, M.W. Review of nocturnal sleep-related eating disorders. Int. J. Eat. Disord. 1994, 15, 343–356. [Google Scholar] [CrossRef] [PubMed]
- Winkelman, J.W. Clinical and polysomnographic features of sleep-related eating disorder. J. Clin. Psychiatry 1998, 59, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Schenck, C.H.; Hurwitz, T.D.; O’Connor, K.A.; Mahowald, M.W. Additional Categories of Sleep-Related Eating Disorders and the Current Status of Treatment. Sleep 1993, 16, 457–466. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders (ICSD-3), 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Vinai, P.; Ferri, R.; Ferini-Strambi, L.; Cardetti, S.; Anelli, M.; Vallauri, P.; Ferrato, N.; Zucconi, M.; Carpegna, G.; Manconi, M. Defining the borders between Sleep-Related Eating Disorder and Night Eating Syndrome. Sleep Med. 2012, 13, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y. Sleep-related eating disorder and its associated conditions. Psychiatry Clin. Neurosci. 2015, 69, 309–320. [Google Scholar] [CrossRef]
- Birketvedt, G.S.; Florholmen, J.; Sundsfjord, J.; Østerud, B.; Dinges, D.; Bilker, W.; Stunkard, A. Behavioral and neuroendocrine characteristics of the night-eating syndrome. JAMA 1999, 282, 657–663. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Grace, W.J.; Wolff, H.G. The night-eating syndrome; a pattern of food intake among certain obese patients. Am. J. Med. 1955, 19, 78–86. [Google Scholar] [CrossRef]
- Boston, R.C.; Moate, P.; Allison, K.C.; Lundgren, J.D.; Stunkard, A.J. Modeling circadian rhythms of food intake by means of parametric deconvolution: Results from studies of the night eating syndrome. Am. J. Clin. Nutr. 2008, 87, 1672–1677. [Google Scholar] [CrossRef]
- Goel, N.; Stunkard, A.J.; Rogers, N.; Van Dongen, H.P.; Allison, K.C.; O’Reardon, J.P.; Ahima, R.S.; Cummings, D.E.; Heo, M.; Dinges, D.F. Circadian rhythm profiles in women with night eating syndrome. J. Boil. Rhythm. 2009, 24, 85–94. [Google Scholar] [CrossRef]
- Vetrugno, R.; Manconi, M.; Ferini-Strambi, L.; Provini, F.; Plazzi, G.; Montagna, P. Nocturnal eating: Sleep-related eating disorder or night eating syndrome? A videopolysomnographic study. Sleep 2006, 29, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Fulda, S.; Hornyak, M.; Muller, K.; Černý, L.; Beitinger, P.A.; Wetter, T.C. Development and validation of the Munich Parasomnia Screening (MUPS). Somnologie Schlafforsch. Schlafmed. 2008, 12, 56–65. [Google Scholar] [CrossRef]
- Komada, Y.; Breugelmans, R.; Fulda, S.; Nakano, S.; Watanabe, A.; Noda, C.; Nishida, S.; Inoue, Y. Japanese version of the Munich Parasomnia Screening: Translation and linguistic validation of a screening instrument for parasomnias and nocturnal behaviors. Neuropsychiatr. Dis. Treat. 2015, 11, 2953–2958. [Google Scholar] [CrossRef] [PubMed]
- Morita, Y.; Sasai-Sakuma, T.; Asaoka, S.; Inoue, Y. The impact of a delayed sleep-wake schedule on depression is greater in women-A web-based cross-sectional study in Japanese young adults. Chrono Int. 2015, 32, 952–958. [Google Scholar]
- Asaoka, S.; Komada, Y.; Aritake, S.; Morita, Y.; Fukuda, K.; Inoue, Y. Effect of delayed sleep phase during university life on the daytime functioning in work life after graduation. Sleep Med. 2014, 15, 1155–1158. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. Neuroimaging 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. Neuroimaging 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Simonelli, G.; Dudley, K.A.; Weng, J.; Gallo, L.C.; Perreira, K.; Shah, N.A.; Alcantara, C.; Zee, P.C.; Ramos, A.R.; Llabre, M.M.; et al. Neighborhood Factors as Predictors of Poor Sleep in the Sueño Ancillary Study of the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Sleep 2016, 40, 025. [Google Scholar]
- Milano, W.; De Rosa, M.; Milano, L.; Capasso, A. Night eating syndrome: An overview. J. Pharm. Pharmacol. 2011, 64, 2–10. [Google Scholar] [CrossRef]
- Petrov, M.E.; Howard, G.; Grandner, M.A.; Kleindorfer, D.; Molano, J.R.; Howard, V.J. Sleep duration and risk of incident stroke by age, sex, and race. Neurol. 2018, 91, 1702–1709. [Google Scholar] [CrossRef]
- Kaneita, Y.; Ohida, T.; Uchiyama, M.; Takemura, S.; Kawahara, K.; Yokoyama, E.; Miyake, T.; Harano, S.; Suzuki, K.; Fujita, T. The relationship between depression and sleep disturbances: A Japanese nationwide general population survey. J. Clin. Psychiatry 2006, 67, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Molina, S.M.; Joshi, K.G. A Case of Zaleplon-Induced Amnestic Sleep-Related Eating Disorder. J. Clin. Psychiatry 2010, 71, 210–211. [Google Scholar] [CrossRef] [PubMed]
- Najjar, M. Zolpidem and Amnestic Sleep Related Eating Disorder. J. Clin. Sleep Med. 2007, 3, 637–638. [Google Scholar] [CrossRef] [PubMed]
- Nzwalo, H.; Ferreira, L.; Peralta, R.; Bentes, C. Sleep-related eating disorder secondary to zolpidem. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.M.; Shin, H.W. Zolpidem Induced Sleep-related Eating and Complex Behaviors in a Patient with Obstructive Sleep Apnea and Restless Legs Syndrome. Clin. Psychopharmacol. Neurosci. 2016, 14, 299–301. [Google Scholar] [CrossRef] [PubMed]
- Yun, C.H.; Ji, K.H. Zolpidem-induced sleep-related eating disorder. J. Neurol. Sci. 2010, 288, 200–201. [Google Scholar] [CrossRef]
- Kim, H.K.; Kwon, J.T.; Baek, J.; Park, D.S.; Yang, K.I. Zolpidem-Induced Compulsive Evening Eating Behavior. Clin. Neuropharmacol. 2013, 36, 173–174. [Google Scholar] [CrossRef]
- Paton, C. Benzodiazepines and disinhibition: A review. Psychiatr. Bull. 2002, 26, 460–462. [Google Scholar] [CrossRef]
- Olson, L.G. Hypnotic hazards: Adverse effects of zolpidem and other z-drugs. Aust. Prescr. 2008, 31, 146–149. [Google Scholar] [CrossRef]
- Yahia, N.; Brown, C.; Potter, S.; Szymanski, H.; Smith, K.; Pringle, L.; Herman, C.P.; Uribe, M.; Fu, Z.; Chung, M.; et al. Night eating syndrome and its association with weight status, physical activity, eating habits, smoking status, and sleep patterns among college students. Eat. Weight. Disord. Stud. Anorexia Bulim. Obes. 2017, 22, 421–433. [Google Scholar] [CrossRef]
- Ceru-Bjork, C.; Andersson, I.; Rossner, S. Night eating and nocturnal eating-two different or similar syndromes among obese patients? J. Int. Assoc. Study Obes. 2001, 25, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, C.V.; Turco, R.M.; Sunday, S.R.; Halmi, K.A. Smoking and body image concerns in adolescent girls. Int. J. Eat. Disord. 1998, 24, 429–433. [Google Scholar] [CrossRef]
- Bulik, C.M.; Epstein, L.H.; McKee, M.; Kaye, W. Drug use in women with bulimia and anorexia nervosa. NIDA Res. Monogr. 1990, 105, 462–463. [Google Scholar] [CrossRef]
- Haug, N.A.; Heinberg, L.J.; Guarda, A.S. Cigarette smoking and its relationship to other substance use among eating disordered inpatients. Eat. Weight. Disord. Stud. Anorexia, Bulim. Obes. 2001, 6, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Anzengruber, D.; Klump, K.L.; Thornton, L.; Brandt, H.; Crawford, S.; Fichter, M.; Halmi, K.A.; Johnson, C.; Kaplan, A.; LaVia, M.; et al. Smoking in eating disorders. Eat. Behav. 2006, 7, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Tu, C.Y.; Tseng, M.C.M.; Chang, C.H. Night eating syndrome in patients with eating disorders: Is night eating syndrome distinct from bulimia nervosa? J. Formos. Med Assoc. 2019, 118, 1038–1046. [Google Scholar] [CrossRef]
- Varghese, R.; De Castro, J.R.; Liendo, C.; Schenck, C.H. Two Cases of Sleep-Related Eating Disorder Responding Promptly to Low-Dose Sertraline Therapy. J. Clin. Sleep Med. 2018, 14, 1805–1808. [Google Scholar] [CrossRef]
- Provini, F.; Vetrugno, R.; Montagna, P. Sleep-related smoking syndrome. Sleep Med. 2008, 9, 903–905. [Google Scholar] [CrossRef]
- Striegel-Moore, R.H.; Bulik, C.M.; Weissman, R.S. Risk factors for eating disorders. Am. Psychol. 2007, 62, 181–198. [Google Scholar] [CrossRef]
- Hoek, H.W. Incidence, prevalence and mortality of anorexia nervosa and other eating disorders. Curr. Opin. Psychiatry 2006, 19, 389–394. [Google Scholar] [CrossRef]
- Hudson, J.I.; Hiripi, E.; Pope, H.G.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Boil. Psychiatry 2006, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Aronoff, N.J.; Geliebter, A.; Zammit, G. Gender and Body Mass Index as Related to the Night-Eating Syndrome in Obese Outpatients. J. Am. Diet. Assoc. 2001, 101, 102–104. [Google Scholar] [CrossRef]
- Tholin, S.; Lindroos, A.; Tynelius, P.; Åkerstedt, T.; Stunkard, A.J.; Bulik, C.M.; Rasmussen, F. Prevalence of Night Eating in Obese and Nonobese Twins. Obes. 2009, 17, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; Franko, D.L.; Thompson, D.; Affenito, S.; Kraemer, H.C.; Weissman, R.S. Night Eating: Prevalence and Demographic Correlates*. Obes. 2006, 14, 139–147. [Google Scholar] [CrossRef]
- Grilo, C.M.; Masheb, R.M. Night-time eating in men and women with binge eating disorder. Behav. Res. Ther. 2004, 42, 397–407. [Google Scholar] [CrossRef]
- Winkelman, J.W. Efficacy and tolerability of open-label topiramate in the treatment of sleep-related eating disorder: A retrospective case series. J. Clin. Psychiatry 2006, 67, 1729–1734. [Google Scholar] [CrossRef]
- Schenck, C.H.; Hurwitz, T.D.; Bundlie, S.R.; Mahowald, M.W. Sleep-Related Eating Disorders: Polysomnographic Correlates of a Heterogeneous Syndrome Distinct from Daytime Eating Disorders. Sleep 1991, 14, 419–431. [Google Scholar] [CrossRef]
- O’Reardon, J.P.; Ringel, B.L.; Dinges, D.F.; Allison, K.C.; Rogers, N.; Martino, N.S.; Stunkard, A.J. Circadian Eating and Sleeping Patterns in the Night Eating Syndrome. Obes. Res. 2004, 12, 1789–1796. [Google Scholar] [CrossRef]
- Mendoza, J.; Clesse, D.; Pévet, P.; Challet, E. Food-reward signalling in the suprachiasmatic clock. J. Neurochem. 2010, 112, 1489–1499. [Google Scholar] [CrossRef]
- McCune, A.M.; Lundgren, J.D. Bright light therapy for the treatment of night eating syndrome: A pilot study. Psychiatry Res. Neuroimaging 2015, 229, 577–579. [Google Scholar] [CrossRef]
- Milano, W.; De Rosa, M.; Milano, L.; Capasso, A. Agomelatine Efficacy in the Night Eating Syndrome. Case Rep. Med. 2013, 2013, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Milano, W.; De Rosa, M.; Milano, L.; Riccio, A.; Sanseverino, B.; Capasso, A. Successful Treatment with Agomelatine in NES: A Series of Five Cases. Open Neurol. J. 2013, 7, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Cain, N.; Gradisar, M. Electronic media use and sleep in school-aged children and adolescents: A review. Sleep Med. 2010, 11, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Do, Y.K.; Shin, E.; Bautista, M.A.; Foo, K. The associations between self-reported sleep duration and adolescent health outcomes: What is the role of time spent on Internet use? Sleep Med. 2013, 14, 195–200. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total (n = 3347) | Nocturnal Eating Behavior (n = 160) | Sleep-Related Eating Disorder-Like Behavior (n = 73) |
|---|---|---|---|
| Age, mean (SD), year | 22.9 (1.8) | 22.9 (1.8) | 22.8 (1.7) |
| Sex (percent male) | 45.3 | 36.3 | 46.6 |
| Body mass index, mean (SD), kg/m2 | 21.1 (3.6) | 21.5 (4.4) | 22.2 (4.4) |
| Current smoker (%) | 10.5 | 20.0 | 21.9 |
| Regular alcohol consumption (%) | 35.1 | 34.4 | 47.9 |
| Living alone (%) | 34.1 | 35.0 | 35.6 |
| Use of hypnotic medication (three or more times per week) (%) | 2.8 | 13.1 | 12.3 |
| Previous and/or current sleepwalking (%) | 8.5 | 35.0 | 71.2 |
| Typical sleep duration, mean (SD), hours | 6.8 (1.4) | 6.9 (1.6) | 7.0 (1.7) |
| Midpoint on weekdays, mean (SD), time | 4:22 (1:40) | 4:41 (1:51) | 4:17 (1:33) |
| Pittsburgh Sleep Quality Index score, mean (SD), points | 5.5 (2.7) | 7.6 (3.1) | 7.2 (3.3) |
| Predictor | Univariate Relative Risk (95% Confidence Interval) 1 | p | Multivariate Relative Risk (95% Confidence Interval) 1 | p | |
|---|---|---|---|---|---|
| Age (years) | 3347 | n.s. | n.s. | ||
| Sex | |||||
| Male | 1517 | ||||
| Female | 1830 | 1.485 (1.068–2.065) | <0.05 | 1.560 (1.103–2.206) | <0.05 |
| Body mass index (kg/m2) | |||||
| <25 | 3016 | ||||
| 25–29 | 247 | n.s. | n.s. | ||
| ≥30 | 84 | 2.484 (1.219–5.062) | <0.05 | n.s. | |
| Living alone | |||||
| No | 2204 | ||||
| Yes | 1143 | n.s. | n.s. | ||
| Current smoker | |||||
| No | 2995 | ||||
| Yes | 352 | 2.240 (1.495–3.356) | <0.001 | 1.980 (1.286–3.047) | <0.01 |
| Regular alcohol consumption | |||||
| No | 2172 | ||||
| Yes | 1175 | n.s. | n.s. | ||
| Use of hypnotic medication (three or more times per week) | |||||
| No | 3253 | ||||
| Yes | 94 | 6.445 (3.854–10.778) | <0.001 | 4.054 (2.306–7.129) | <0.001 |
| Previous and/or current sleepwalking | |||||
| No | 3062 | ||||
| Yes | 285 | 6.955 (4.894–9.886) | <0.001 | 6.249 (4.335–9.009) | <0.001 |
| Typical sleep duration (hours) | |||||
| ≥6 | 2723 | ||||
| <6 | 624 | 1.539 (1.067–2.219) | <0.05 | n.s. | |
| Sleep-wake schedule2 | |||||
| Not delayed | 1438 | ||||
| Delayed | 1909 | 1.507 (1.078–2.107) | <0.05 | 1.478 (1.042–2.096) | <0.05 |
| Pittsburgh Sleep Quality Index score (points) | |||||
| <6 | 1827 | ||||
| ≥6 | 1520 | 2.690 (1.915–3.779) | <0.001 | 1.871 (1.304–2.684) | <0.01 |
| Predictor | Univariate Relative Risk (95% Confidence Interval) 1 | p | Multivariate Relative Risk (95% Confidence interval) 1 | p | |
|---|---|---|---|---|---|
| Age (years) | 3347 | n.s. | n.s. | ||
| Sex | |||||
| Male | 1517 | ||||
| Female | 1830 | n.s. | n.s. | ||
| Body mass index (kg/m2) | |||||
| <25 | 3016 | ||||
| 25–29 | 247 | 2.115 (1.068–4.188) | <0.05 | n.s. | |
| ≥30 | 84 | n.s. | n.s. | ||
| Living alone | |||||
| No | 2204 | ||||
| Yes | 1143 | n.s. | n.s. | ||
| Current smoker | |||||
| No | 2995 | ||||
| Yes | 352 | 2.454 (1.394–4.322) | <0.01 | 1.998 (1.072–3.724) | <0.05 |
| Regular alcohol consumption | |||||
| No | 2172 | ||||
| Yes | 1175 | 1.724 (1.083–2.744) | <0.05 | n.s. | |
| Use of hypnotic medication (three or more times per week) | |||||
| No | 3253 | ||||
| Yes | 94 | 5.276 (2.542–10.951) | <0.001 | 3.750 (1.606–8.755) | <0.01 |
| Previous and/or current sleepwalking | |||||
| No | 3062 | ||||
| Yes | 285 | 32.318 (19.137–54.576) | <0.001 | 30.113 (17.764–51.044) | <0.001 |
| Typical sleep duration (hours) | |||||
| ≥6 | 2723 | ||||
| <6 | 624 | n.s. | n.s. | ||
| Sleep-wake schedule2 | |||||
| Not delayed | 1438 | ||||
| Delayed | 1909 | n.s. | n.s. | ||
| Pittsburgh Sleep Quality Index (points) | |||||
| <6 | 1827 | ||||
| ≥6 | 1520 | 1.848 (1.151–2.969) | <0.05 | n.s. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsui, K.; Komada, Y.; Nishimura, K.; Kuriyama, K.; Inoue, Y. Prevalence and Associated Factors of Nocturnal Eating Behavior and Sleep-Related Eating Disorder-Like Behavior in Japanese Young Adults: Results of an Internet Survey Using Munich Parasomnia Screening. J. Clin. Med. 2020, 9, 1243. https://doi.org/10.3390/jcm9041243
Matsui K, Komada Y, Nishimura K, Kuriyama K, Inoue Y. Prevalence and Associated Factors of Nocturnal Eating Behavior and Sleep-Related Eating Disorder-Like Behavior in Japanese Young Adults: Results of an Internet Survey Using Munich Parasomnia Screening. Journal of Clinical Medicine. 2020; 9(4):1243. https://doi.org/10.3390/jcm9041243
Chicago/Turabian StyleMatsui, Kentaro, Yoko Komada, Katsuji Nishimura, Kenichi Kuriyama, and Yuichi Inoue. 2020. "Prevalence and Associated Factors of Nocturnal Eating Behavior and Sleep-Related Eating Disorder-Like Behavior in Japanese Young Adults: Results of an Internet Survey Using Munich Parasomnia Screening" Journal of Clinical Medicine 9, no. 4: 1243. https://doi.org/10.3390/jcm9041243
APA StyleMatsui, K., Komada, Y., Nishimura, K., Kuriyama, K., & Inoue, Y. (2020). Prevalence and Associated Factors of Nocturnal Eating Behavior and Sleep-Related Eating Disorder-Like Behavior in Japanese Young Adults: Results of an Internet Survey Using Munich Parasomnia Screening. Journal of Clinical Medicine, 9(4), 1243. https://doi.org/10.3390/jcm9041243