Twenty Years of Cerebral Ultrasound Perfusion Imaging—Is the Best yet to Come?


Abstract
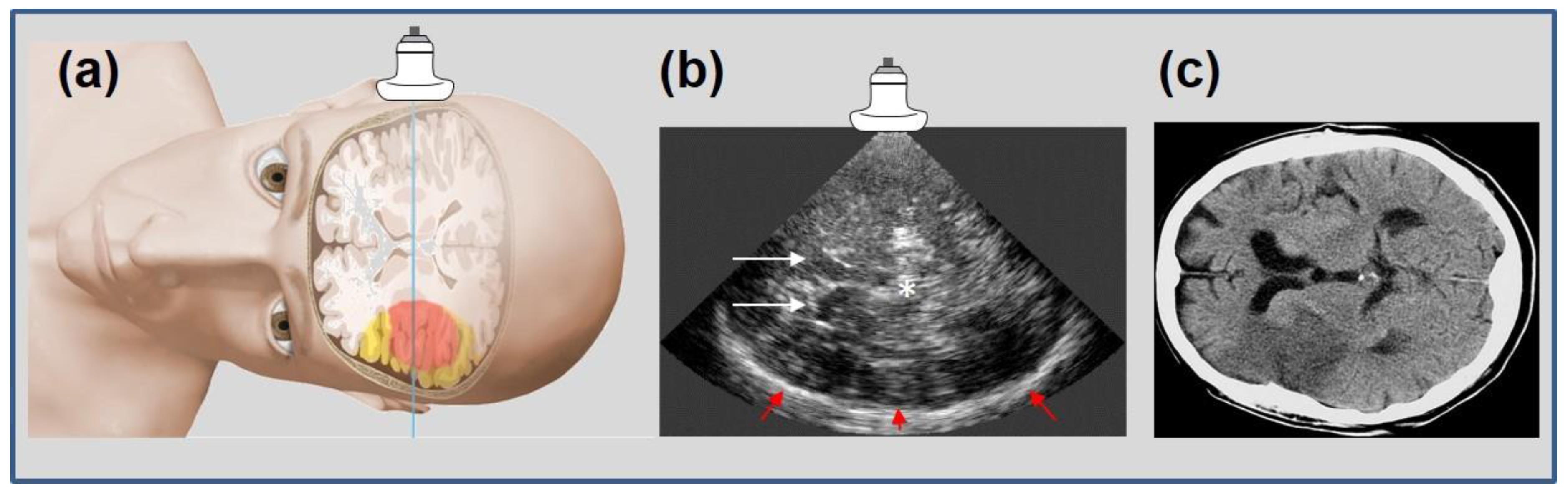
1. Introduction: Cerebral Ultrasound Perfusion Imaging (UPI), First Clinical Applications
2. Technical Aspects
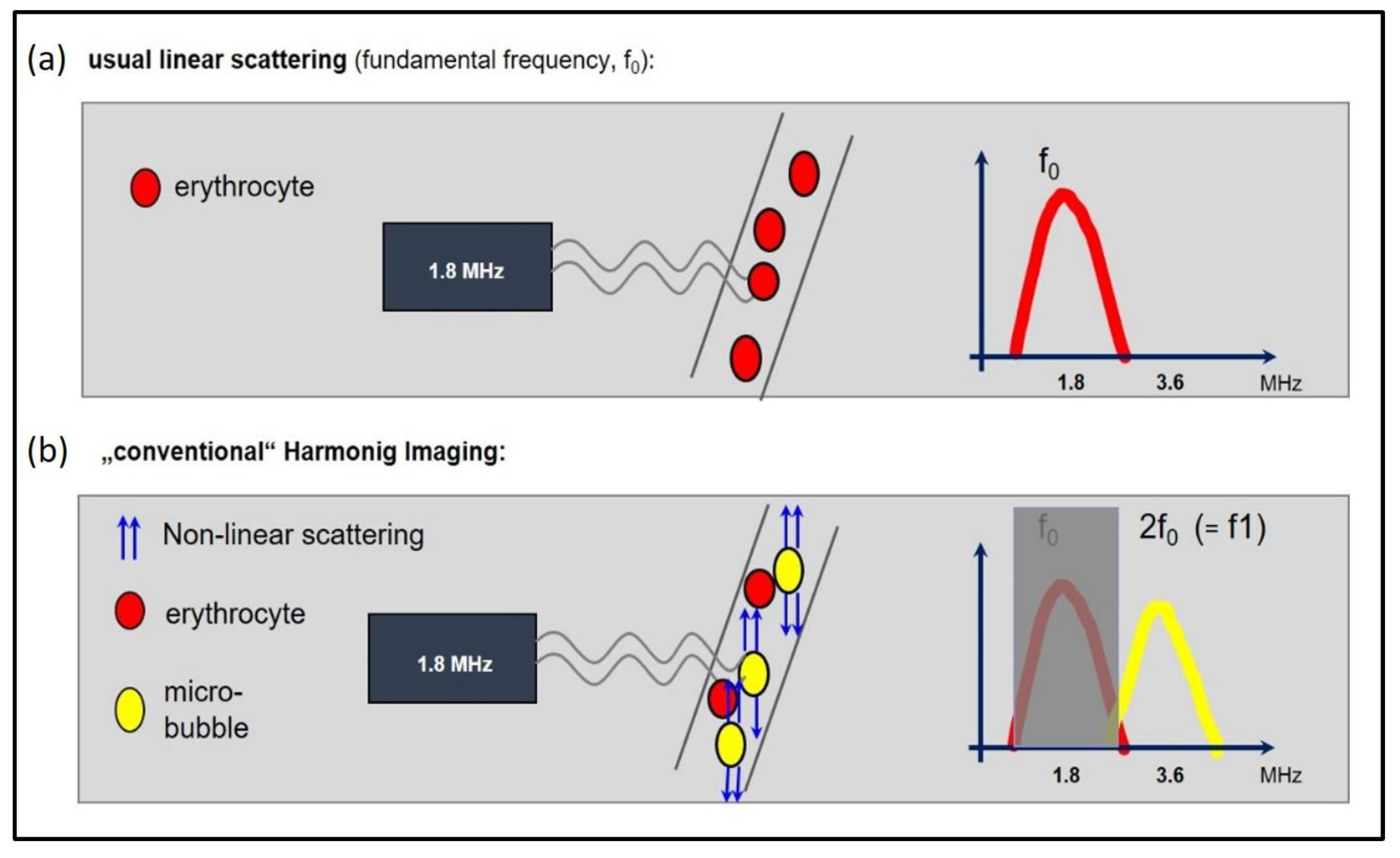
2.1. Microbubbles and Harmonic Imaging
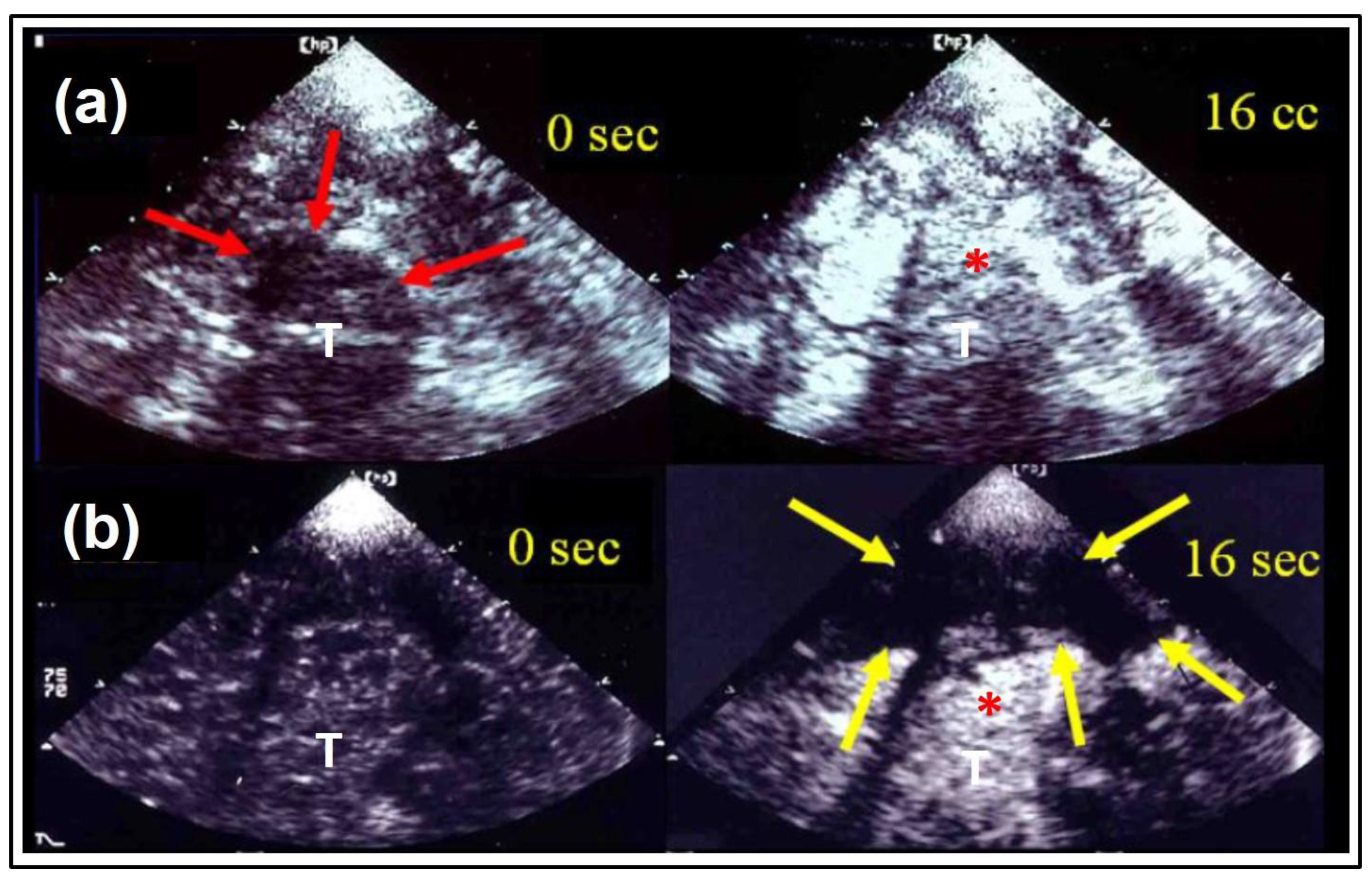
2.1.1. “Non-Destructive Imaging Modes”:
2.1.2. “Destructive Imaging modes”:
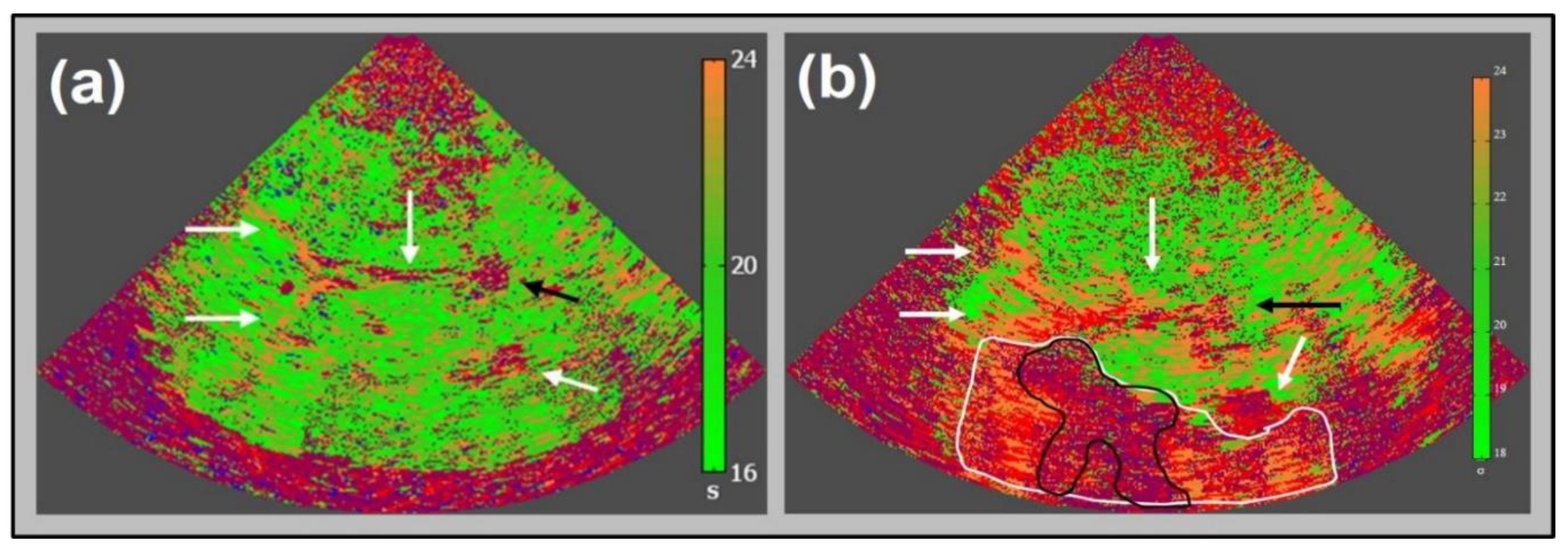
2.2. Data Acquisition and Processing
3. Validation to Standard Imaging
4. Clinical Applications up to Date and Future Indications
5. Restrictions of the Method and Safety Considerations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Postert, T.; Muhs, A.; Meves, S.; Federlein, J.; Przuntek, H.; Büttner, T. Transient response harmonic imaging: An ultrasound technique related to brain perfusion. Stroke 1998, 29, 1901–1907. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Postert, T.; Federlein, J.; Weber, S.; Przuntek, H.; Büttner, T. Second harmonic imaging in acute middle cerebral artery infarction: Preliminary results. Stroke 1999, 30, 1702–1706. [Google Scholar] [CrossRef]
- Firschke, C.; Lindner, J.R.; Wie, K.; Goodman, N.C.; Skyba, D.M.; Kaul, S. Myocardial perfusion imaging in the setting of coronary artery stenosis and acute myocardial infarction using venous injection of a second generation echocardiographic contrast agent. Circulation 1997, 96, 959–967. [Google Scholar] [PubMed]
- Federlein, J.; Postert, T.; Meves, S.; Weber, S.; Przuntek, H.; Büttner, T. Ultrasonic evaluation of pathological brain perfusion in acute stroke using second harmonic imaging. J. Neurol. Neurosurg. Psychiatry 2000, 69, 616–622. [Google Scholar] [CrossRef][Green Version]
- Wiesmann, M.; Meyer, K.; Albers, T.; Seidel, G. Parametric imaging with contrast-enhanced ultrasound in acute ischemic stroke. Stroke 2004, 35, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Seidel, G.; Meyer-Wiethe, K.; Berdien, G.; Hollstein, D.; Toth, D.; Aach, T. Ultrasound perfusion imaging in acute middle cerebral artery infarction predicts outcome. Stroke 2004, 35, 1107–1111. [Google Scholar] [CrossRef]
- Postert, T.; Hoppe, P.; Federlein, J.; Helbeck, S.; Ermert, H.; Przuntek, H.; Büttner, T.; Wilkening, W. Contrast agent specific imaging modes for the ultrasonic assessment of parenchymal cerebral echo contrast enhancement. J. Cereb. Blood Flow. Metab. 2000, 20, 1709–1716. [Google Scholar] [CrossRef]
- Eyding, J.; Krogias, C.; Wilkening, W.; Meves, S.; Ermert, H.; Postert, T. Parameters of cerebral perfusion in phase inversion harmonic imaging (PIHI) ultrasound examinations. Ultrasound. Med. Biol. 2003, 29, 1379–1385. [Google Scholar] [CrossRef]
- Eyding, J.; Wilkening, W.; Reckhardt, M.; Schmid, G.; Meves, S.; Ermert, H.; Przuntek, H.; Postert, T. Contrast Burst Depletion Imaging (CODIM): A new imaging procedure and analysis method for semi-quantitative ultrasonic perfusion imaging. Stroke 2003, 34, 77–83. [Google Scholar] [CrossRef]
- Kern, R.; Perren, F.; Schoeneberger, K.; Gass, A.; Hennerici, M.; Meairs, S. Ultrasound microbubble destruction imaging in acute middle cerebral artey stroke. Stroke 2004, 35, 1665–1670. [Google Scholar] [CrossRef]
- Krogias, C.; Postert, T.; Wilkening, W.; Meves, S.; Przuntek, H.; Eyding, J. Semiquantitative analysis of ultrasonic cerebral perfusion imaging. Ultrasound Med. Biol. 2005, 31, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Eyding, J.; Schöllhammer, M.; Eyding, D.; Wilkening, W.; Meves, S.; Schröder, A.; Przuntek, H.; Krogias, C.; Postert, T. Contrast-enhanced ultrasonic parametric perfusion imaging detects tissue at risk in acute stroke. J. Cereb. Blood Flow. Metab. 2006, 26, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Reitmeir, R.; Eyding, J.; Oertel, M.F.; Wiest, R.; Gralla, J.; Fischer, U.; Giquel, P.Y.; Weber, S.; Raabe, A.; Mattle, H.P.; et al. Is ultrasound perfusion imaging capable of detecting mismatch? A proof of- concept study in acute stroke patients. J. Cereb. Blood Flow. Metab. 2017, 37, 1517–1526. [Google Scholar] [CrossRef] [PubMed]
- Vinke, E.J.; Kortenbout, J.; Eyding, J.; Slump, C.H.; van der Hoeven, J.G.; de Korte, C.L.; Hoedemaekers, C.W.E. Potential of contrast enhanced ultrasound as a bedside monitoring technique of cerebral perfusion: A systematic review. Ultrasound Med. Biol. 2017, 43, 2751–2757. [Google Scholar] [CrossRef]
- Eyding, J.; Wilkening, W.; Postert, T. Brain perfusion and ultrasonic imaging techniques. Eur. J. Ultrasound. 2002, 16, 91–104. [Google Scholar] [CrossRef]
- Paefgen, V.; Doleschel, D.; Kiessling, F. Evolution of contrast agents for ultrasound imaging and ultrasound-mediated drug delivery. Front. Pharmacol. 2015, 6, 197. [Google Scholar] [CrossRef]
- Meves, S.H.; Wilkening, W.; Thies, T.; Eyding, J.; Holscher, T.; Finger, M.; Schmid, G.; Ermert, H.; Postert, T. Ruhr Center of Competence for Medical Engineering. Comparison between echo contrast agent specific imaging modes and perfusion-weighted magnetic resonance imaging for the assessment of brain perfusion. Stroke 2002, 33, 2433–2437. [Google Scholar] [CrossRef]
- Kern, R.; Diels, A.; Pettenpohl, J.; Kablau, M.; Brade, J.; Hennerici, M.G.; Meairs, S. Real-time ultrasound brain perfusion imaging with analysis of microbubble replenishment in acute MCAstroke. J. Cereb. Blood Flow. Metab. 2011, 31, 1716–1724. [Google Scholar] [CrossRef]
- Eyding, J.; Reitmair, R.; Oertel, M.; Fischer, U.; Wiest, R.; Gralla, J.; Raabe, A.; Zubak, I.; Z’Graggen, W.; Beck, J. Ultrasonic quantification of cerebral perfusion in acute arterial occlusive stroke-a comparative challenge of the refill- and the bolus-kinetics approach. PLoS ONE 2019, 14, e0220171. [Google Scholar] [CrossRef]
- Piscaglia, F.; Nolsøe, C.; Dietrich, C.F.; Cosgrove, D.O.; Gilja, O.H.; Bachmann Nielsen, M.; Albrecht, T.; Barozzi, L.; Bertolotto, M.; Catalano, O.; et al. The EFSUMB Guidelines and Recommendations on the Clinical Practice of Contrast Enhanced Ultrasound (CEUS). Update 2011 on non-hepatic applications. Ultraschall Med. 2012, 33, 33–59. [Google Scholar] [CrossRef]
- Nolte, C.H.; Gruss, J.; Steinbrink, J.; Jungehulsing, G.J.; Brunecker, P.; Hopt, A.M.; Schreiber, S.J. Ultrasound Perfusion Imaging of Small Stroke Involving the Thalamus. Ultraschall Med. 2008, 29, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Krogias, C.; Henneböhl, C.; Geier, B.; Hansen, C.; Hummel, T.; Meves, S.H.; Lukas, C.; Eyding, J. Transcranial ultrasound perfusion imaging and perfusion-MRI–a pilot study on the evaluation of cerebral perfusion in severe carotid artery stenosis. Ultrasound Med. Biol. 2010, 36, 1973–1980. [Google Scholar] [CrossRef] [PubMed]
- Krogias, C.; Meves, S.H.; Hansen, C.; Mönnings, P.; Eyding, J. Ultrasound Perfusion Imaging of the brain–Routine and novel applications. Uncommon cases and review of the literature. J. Neuroimaging 2011, 21, 255–258. [Google Scholar] [CrossRef]
- Herzberg, M.; Boy, S.; Hölscher, T.; Ertl, M.; Zimmermann, M.; Ittner, K.P.; Pemmerl, J.; Pels, H.; Bogdahn, U.; Schlachetzki, F. Prehospital stroke diagnostics based on neurological examination and transcranial ultrasound. Crit. Ultrasound. J. 2014, 6, 3. [Google Scholar] [CrossRef]
- Lima, F.O.; Mont’Alverne, F.J.A.; Bandeira, D.; Nogueira, R.G. Pre-hospital assessment of large vessel occlusion strokes: Implications for modeling and planning stroke systems of care. Front. Neurol. 2019, 10, 955. [Google Scholar] [CrossRef] [PubMed]
- Fuhrer, H.; Reinhard, M.; Niesen, W.D. Paradigm change? Cardiac output better associates with cerebral perfusion than blood pressure in ischemic stroke. Front. Neurol. 2017, 8, 706. [Google Scholar] [CrossRef]
- Seidel, G.; Kaps, M.; Dorndorf, W. Transcranial color-coded duplex sonography of intracerebral hematomas in adults. Stroke 1993, 24, 1519–1527. [Google Scholar] [CrossRef]
- Fainardi, E.; Borrelli, M.; Saletti, A.; Schivalocchi, R.; Azzini, C.; Cavallo, M.; Ceruti, S.; Tamarozzi, R.; Chieregato, A. CT perfusion mapping of hemodynamic disturbances associated to acute spontaneous intracerebral hemorrhage. Neuroradiology 2008, 50, 729–740. [Google Scholar] [CrossRef]
- Kern, R.; Kablau, M.; Sallustio, F.; Fatar, M.; Stroick, M.; Hennerici, M.G.; Meairs, S. Improved detection of intracerebral hemorrhage with transcranial ultrasound perfusion imaging. Cerebrovasc. Dis. 2008, 26, 277–283. [Google Scholar] [CrossRef]
- Niesen, W.; Schläger, A.; Reinhard, M.; Fuhrer, H. Transcranial sonography to differentiate primary intracerebral hemorrhage from cerebral infarction with hemorrhagic transformation. J. Neuroimaging 2018, 28, 370–373. [Google Scholar] [CrossRef]
- Harrer, J.U.; Hornen, S.; Oertel, M.F.; Stracke, C.P.; Klötzsch, C. Comparison of perfusion harmonic imaging and perfusion mr imaging for the assessment of microvascular characteristics in brain tumors. Ultraschall. Med. 2008, 29, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Harrer, J.U.; Mayfrank, L.; Mull, M.; Klötzsch, C. Second harmonic imaging: A new ultrasound technique to assess human brain tumour perfusion. J. Neurol. Neurosurg. Psychiatry 2003, 74, 333–338. [Google Scholar] [CrossRef]
- Harrer, J.U.; Möller-Hartmann, W.; Oertel, M.F.; Klötzsch, C. Perfusion imaging of high-grade gliomas: A comparison between contrast harmonic and magnetic resonance imaging. Technical note. J. Neurosurg. 2004, 101, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.F.; He, W.; Lin, S.; Han, B.; Zee, C.S. Using Real-Time Fusion Imaging Constructed from Contrast-Enhanced Ultrasonography and Magnetic Resonance Imaging for High-Grade Glioma in Neurosurgery. World Neurosurg. 2019, 125, e98–e109. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, G.M.; Ius, T.; Menna, G.; La Rocca, G.; Battistella, C.; Rapisarda, A.; Mazzucchi, E.; Pignotti, F.; Alexandre, A.; Marchese, E.; et al. “Dark corridors” in 5-ALA resection of high-grade gliomas: Combining fluorescence-guided surgery and contrast-enhanced ultrasonography to better explore the surgical field. J. Neurosurg. Sci. 2019, 63, 688–696. [Google Scholar] [CrossRef]
- Nagelhus Hernes, T.A.; Lindseth, F.; Selbekk, T.; Wollf, A.; Solberg, O.V.; Harg, E.; Rygh, O.M.; Tangen, G.A.; Rasmussen, I.; Augdal, S.; et al. Computer-assisted 3D ultrasound-guided neurosurgery: Technological contributions, including multimodal registration and advanced display, demonstrating future perspectives. Int. J. Med. Robot 2006, 2, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, I.A., Jr.; Lindseth, F.; Rygh, O.M.; Berntsen, E.M.; Selbekk, T.; Xu, J.; Nagelhus Hernes, T.A.; Harg, E.; Håberg, A.; Unsgaard, G. Functional neuronavigation combined with intra-operative 3D ultrasound: Initial experiences during surgical resections close to eloquent brain areas and future directions in automatic brain shift compensation of preoperative data. Acta Neurochir. (Wien) 2007, 149, 365–378. [Google Scholar] [CrossRef]
- Lassau, N.; Chami, L.; Chebil, M.; Benatsou, B.; Bidault, S.; Girard, E.; Abboud, G.; Roche, A. Dynamic contrast-enhanced ultrasonography (DCE-US) and anti-angiogenic treatments. Discov. Med. 2011, 11, 18–24. [Google Scholar]
- Solbiati, L.; Ierace, T.; Tonolini, M.; Cova, L. Guidance and monitoring of radiofrequency liver tumor ablation with contrast-enhanced ultrasound. Eur. J. Radiol. 2004, 51, S19–S23. [Google Scholar] [CrossRef]
- Prada, F.; Perin, A.; Martegani, A.; Aiani, L.; Solbiati, L.; Lamperti, M.; Casali, C.; Legnani, F.; Mattei, L.; Saladino, A.; et al. Intraoperative contrast-enhanced ultrasound for brain tumor surgery. Neurosurgery 2014, 74, 542–552. [Google Scholar] [CrossRef]
- Engelhardt, M.; Hansen, C.; Eyding, J.; Wilkening, W.; Brenke, C.; Krogias, C.; Scholz, M.; Harders, A.; Ermert, H.; Schmieder, K. Feasibility of contrast-enhanced sonography during resection of cerebral tumours: Initial results of a prospective study. Ultrasound. Med. Biol. 2007, 33, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Vicenzini, E.; Delfini, R.; Magri, F.; Puccinelli, F.; Altieri, M.; Santoro, A.; Giannoni, M.F.; Bozzao, L.; Di Piero, V.; Lenzi, G.L. Semiquantitative human cerebral perfusion assessment with ultrasound in brain space-occupying lesions: Preliminary data. J. Ultrasound. Med. 2008, 27, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Daffertshofer, M.; Gass, A.; Ringleb, P.; Sitzer, M.; Sliwka, U.; Els, T.; Sedlaczek, O.; Koroshetz, W.J.; Hennerici, M.G. Transcranial lowfrequency ultrasound-mediated thrombolysis in brain ischemia: Increased risk of hemorrhage with combined ultrasound and tissue plasminogen activator: Results of a phase II clinical trial. Stroke 2005, 36, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Reinhard, M.; Hetzel, A.; Kruger, S.; Kretzer, S.; Talazko, J.; Ziyeh, S.; Weber, J.; Els, T. Blood-brain barrier disruption by low-frequency ultrasound. Stroke 2006, 37, 1546–1548. [Google Scholar] [CrossRef]
- Jungehulsing, G.J.; Brunecker, P.; Nolte, C.H.; Fiebach, J.B.; Kunze, C.; Doepp, F.; Villringer, A.; Schreiber, S.J. Diagnostic transcranial ultrasound perfusion-imaging at 2.5 MHz does not affect the blood–brain barrier. Ultrasound Med. Biol. 2008, 34, 147–150. [Google Scholar] [CrossRef]
- Harrer, J.U.; Eyding, J.; Ritter, M.; Schminke, U.; Schulte-Altedorneburg, G.; Köhrmann, M.; Nedelmann, M.; Schlachetzki, F. The potential of neurosonography in neurological emergency and intensive care medicine: Basic principles, vascular stroke diagnostics, and monitoring of stroke-specific therapy-part 1. Ultraschall. Med. 2012, 33, 218–235. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | First Approved | Gas | Shell Material | Producer/Distributor |
|---|---|---|---|---|
| Levovist® | 1993, withdrawn | Air | Galactose microparticles | Schering AG, Berlin, DE |
| Optison® | 1998 | Octafluoropropane, C3F8 | Cross-linked serum albumin | GE healthcare, Buckinghamshire, UK |
| SonoVue® | 2001 | Sulphurhexafluoride, SF6 | Phospholipid | Bracco diagnostics, Milano, Italy |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eyding, J.; Fung, C.; Niesen, W.-D.; Krogias, C. Twenty Years of Cerebral Ultrasound Perfusion Imaging—Is the Best yet to Come? J. Clin. Med. 2020, 9, 816. https://doi.org/10.3390/jcm9030816
Eyding J, Fung C, Niesen W-D, Krogias C. Twenty Years of Cerebral Ultrasound Perfusion Imaging—Is the Best yet to Come? Journal of Clinical Medicine. 2020; 9(3):816. https://doi.org/10.3390/jcm9030816
Chicago/Turabian StyleEyding, Jens, Christian Fung, Wolf-Dirk Niesen, and Christos Krogias. 2020. "Twenty Years of Cerebral Ultrasound Perfusion Imaging—Is the Best yet to Come?" Journal of Clinical Medicine 9, no. 3: 816. https://doi.org/10.3390/jcm9030816
APA StyleEyding, J., Fung, C., Niesen, W.-D., & Krogias, C. (2020). Twenty Years of Cerebral Ultrasound Perfusion Imaging—Is the Best yet to Come? Journal of Clinical Medicine, 9(3), 816. https://doi.org/10.3390/jcm9030816