Shunt-Induced Hepatic Encephalopathy in TIPS: Current Approaches and Clinical Challenges



Abstract
1. Background
2. Pathogenesis and Molecular Mechanisms
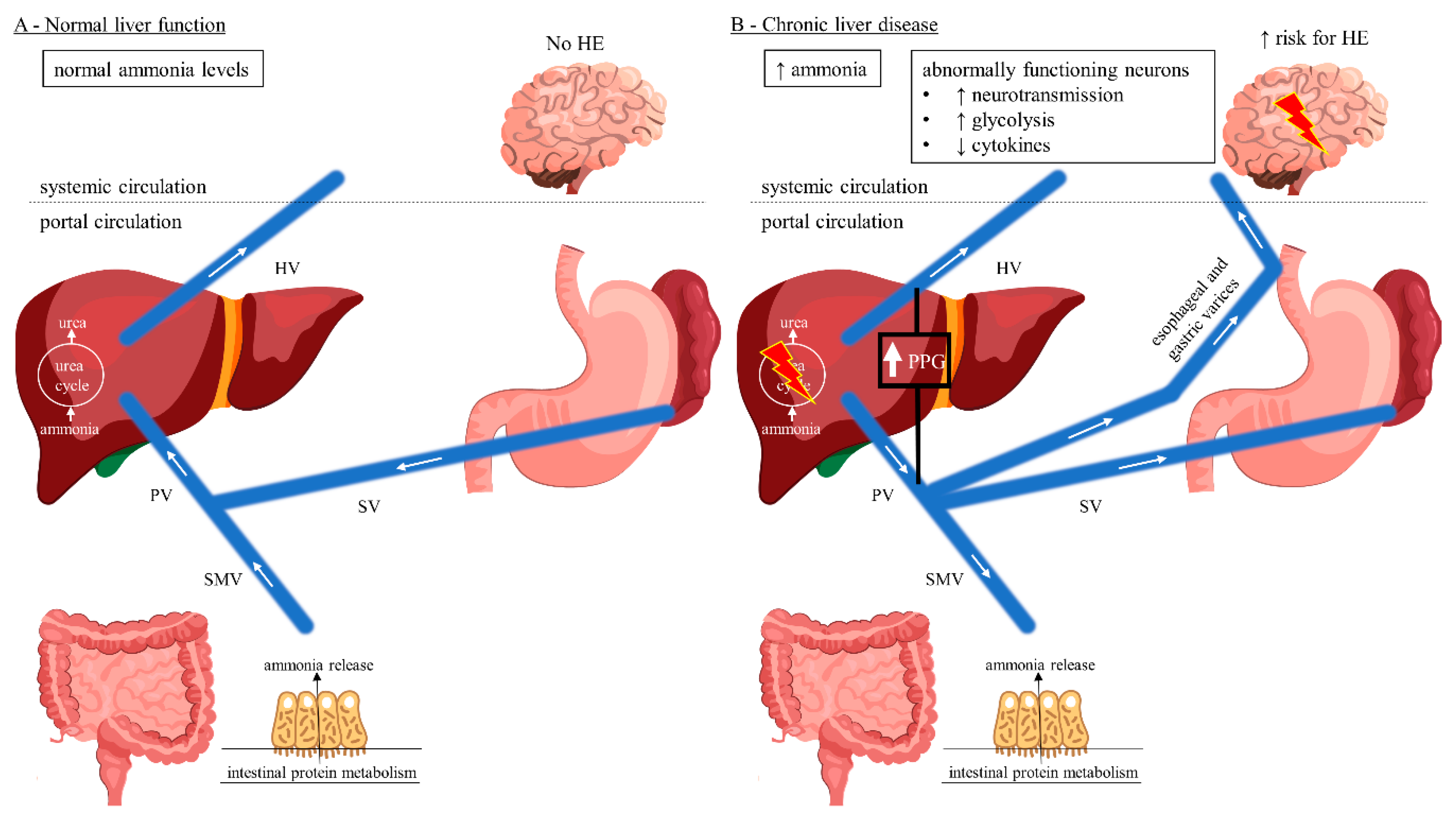
2.1. Ammonia Homeostasis in Normal Liver Function and Hepatic Failure
2.2. Cerebral Ammonia Metabolism
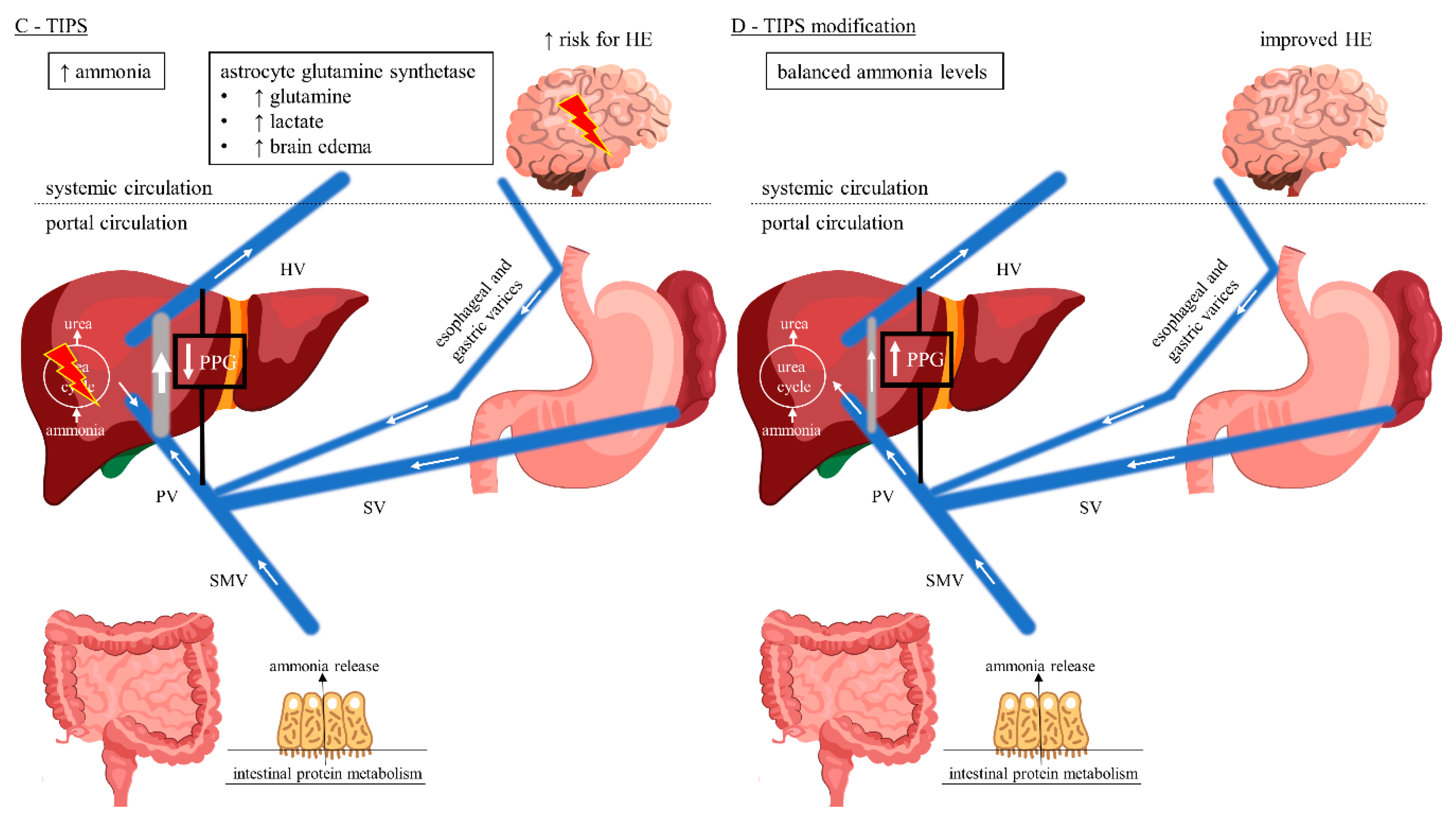
2.3. Ammonia Homeostasis among TIPS Patients
2.4. Additional Mechanisms Underlying HE
3. Epidemiology and Clinical Presentation
- (1)
- According to the underlying cause, HE is subdivided into type A (due to reduced detoxification performance of the liver in acute liver failure), type B (if the hepatic detoxification function is bypassed by portosystemic bypass or shunt) and type C (by combining the mechanisms mentioned above in cirrhosis) [25,54,55].
- (2)
- Clinical effects range from mild confusion to coma and are commonly graded by the West Haven Criteria [14,54]:
- Grade 0 (minimal)—normal state of consciousness, objectifiable only by neuropsychiatric tests;
- Grade 1—slight mental slowdown, disturbed fine motor skills;
- Grade 2—increased fatigue, apathy, flapping tremor/asterixis, ataxia, slurred speech;
- Grade 3—somnolence, marked disorientation, rigor, stupor;
- Grade 4—coma.
- (3)
- (4)
- In the event of overt HE occurrence, triggering factors such as constipation, infections, gastrointestinal bleeding, electrolyte imbalance, diuretic over dosage or taking benzodiazepines, analgesics or hypnotics must always be cared for [25,54,55]. In the absence of precipitating factors, HE is considered to be spontaneous [54,55].
4. Risk Factors of HE in Cirrhosis and Following Tips
4.1. Risk Factors in Cirrhosis
4.2. Risk Factors Following TIPS
5. Shunt Diameter and HE
6. Management and Outcome of Post-Tips HE
7. Summary
Funding
Conflicts of Interest
References
- Hung, M.L.; Lee, E.W. Role of Transjugular Intrahepatic Portosystemic Shunt in the Management of Portal Hypertension: Review and Update of the Literature. Clin. Liver Dis. 2019, 23, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.W.; Sood, A.; Jacobson, I.M.; Brown, R.S. Transjugular intrahepatic portosystemic shunt for refractory ascites: An analysis of the literature on efficacy, morbidity, and mortality. Am. J. Gastroenterol. 2003, 98, 2521–2527. [Google Scholar] [CrossRef] [PubMed]
- Perry, B.C.; Kwan, S.W. Portosystemic Shunts: Stable Utilization and Improved Outcomes, Two Decades after the Transjugular Intrahepatic Portosystemic Shunt. J. Am. Coll. Radiol. 2015, 12, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Bureau, C.; Thabut, D.; Oberti, F.; Dharancy, S.; Carbonell, N.; Bouvier, A.; Mathurin, P.; Otal, P.; Cabarrou, P.; Péron, J.M.; et al. Transjugular Intrahepatic Portosystemic Shunts With Covered Stents Increase Transplant-Free Survival of Patients With Cirrhosis and Recurrent Ascites. Gastroenterology 2017, 152, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Horhat, A.; Bureau, C.; Thabut, D.; Rudler, M. Transjugular intrahepatic portosystemic shunt in patients with cirrhosis: Indications and post-transjugular intrahepatic portosystemic shunt complications in 2020. United Eur. Gastroenterol. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Casadaban, L.C.; Parvinian, A.; Minocha, J.; Lakhoo, J.; Grant, C.W.; Ray, C.E.; Knuttinen, M.G.; Bui, J.T.; Gaba, R.C. Clearing the Confusion over Hepatic Encephalopathy After TIPS Creation: Incidence, Prognostic Factors, and Clinical Outcomes. Dig. Dis. Sci. 2015, 60, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Fonio, P.; Discalzi, A.; Calandri, M.; Breatta, A.D.; Bergamasco, L.; Martini, S.; Ottobrelli, A.; Righi, D.; Gandini, G. Incidence of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt (TIPS) according to its severity and temporal grading classification. La Radiologia Medica 2017, 122, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Hadjihambi, A.; Arias, N.; Sheikh, M.; Jalan, R. Hepatic encephalopathy: A critical current review. Hepatol. Int. 2018, 12, 135–147. [Google Scholar] [CrossRef]
- Wijdicks, E.F.M. Hepatic Encephalopathy. N. Engl. J. Med. 2016, 375, 1660–1670. [Google Scholar] [CrossRef]
- Butterworth, R.F. Hepatic Encephalopathy in Cirrhosis: Pathology and Pathophysiology. Drugs 2019, 79, 17–21. [Google Scholar] [CrossRef]
- Jaffe, A.; Lim, J.K.; Jakab, S.S. Pathophysiology of Hepatic Encephalopathy. Clin. Liver Dis. 2020, 24, 175–188. [Google Scholar] [CrossRef] [PubMed]
- Weir, V.; Reddy, K.R. Nonpharmacologic Management of Hepatic Encephalopathy: An update. Clin. Liver Dis. 2020, 24, 243–261. [Google Scholar] [CrossRef] [PubMed]
- American Association for the Study of Liver Diseases; European Association for the Study of the Liver. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef] [PubMed]
- Weissenborn, K. Hepatic Encephalopathy: Definition, Clinical Grading and Diagnostic Principles. Drugs 2019, 79, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Sharma, B.C. Management of Overt Hepatic Encephalopathy. J. Clin. Exp. Hepatol. 2015, 5, S82–S87. [Google Scholar] [CrossRef]
- Waghray, A.; Waghray, N.; Mullen, K. Management of Covert Hepatic Encephalopathy. J. Clin. Exp. Hepatol. 2015, 5, S75–S81. [Google Scholar] [CrossRef]
- Mahpour, N.Y.; Pioppo-Phelan, L.; Reja, M.; Tawadros, A.; Rustgi, V.K. Pharmacologic Management of Hepatic Encephalopathy. Clin. Liver Dis. 2020, 24, 231–242. [Google Scholar] [CrossRef]
- Pereira, K.; Carrion, A.F.; Salsamendi, J.; Doshi, M.H.; Baker, R.; Kably, I. Endovascular Management of Refractory Hepatic Encephalopathy Complication of Transjugular Intrahepatic Portosystemic Shunt (TIPS): Comprehensive Review and Clinical Practice Algorithm. Cardiovasc. Interv. Radiol. 2016, 39, 170–182. [Google Scholar] [CrossRef]
- Rowley, M.W.; Choi, M.; Chen, S.; Hirsch, K.; Seetharam, A.B. Refractory Hepatic Encephalopathy After Elective Transjugular Intrahepatic Portosystemic Shunt: Risk Factors and Outcomes with Revision. Cardiovasc. Interv. Radiol. 2018, 41, 1765–1772. [Google Scholar] [CrossRef]
- De Keyzer, B.; Nevens, F.; Laenen, A.; Heye, S.; Laleman, W.; Verslype, C.; Van Der Merwe, S.; Maleux, G. Percutaneous shunt reduction for the management of TIPS-induced acute liver decompensation: A follow-up study. Ann. Hepatol. 2016, 15, 911–917. [Google Scholar]
- Taylor, A.G.; Kolli, K.P.; Kerlan, R.K. Techniques for Transjugular Intrahepatic Portosystemic Shunt Reduction and Occlusion. Tech. Vasc. Interv. Radiol. 2016, 19, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Vizzutti, F.; Schepis, F.; Arena, U.; Fanelli, F.; Gitto, S.; Aspite, S.; Turco, L.; Dragoni, G.; Laffi, G.; Marra, F. Transjugular intrahepatic portosystemic shunt (TIPS): Current indications and strategies to improve the outcomes. Intern. Emerg. Med. 2020, 15, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Coronado, W.M.; Ju, C.; Bullen, J.; Kapoor, B. Predictors of Occurrence and Risk of Hepatic Encephalopathy after TIPS Creation: A 15-Year Experience. Cardiovasc. Interv. Radiol. 2020, 43, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Dariushnia, S.R.; Haskal, Z.J.; Midia, M.; Martin, L.G.; Walker, T.G.; Kalva, S.P.; Clark, T.W.I.; Ganguli, S.; Krishnamurthy, V.; Saiter, C.K.; et al. Quality Improvement Guidelines for Transjugular Intrahepatic Portosystemic Shunts. J. Vasc. Interv. Radiol. 2016, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Elsaid, M.I.; Rustgi, V.K. Epidemiology of Hepatic Encephalopathy. Clin. Liver Dis. 2020, 24, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Lattanzi, B.; Torrisi, S.; Greco, F.; Farcomeni, A.; Gioia, S.; Merli, M.; Riggio, O. Sarcopenia Is Risk Factor for Development of Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt Placement. Clin. Gastroenterol. Hepatol. 2017, 15, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Qi, X.; Yang, Z.; Yin, Z.; Nie, Y.; Yuan, S.; Wu, K.; Han, G.; Fan, D. Predictors of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt in cirrhotic patients: A systematic review. J. Gastroenterol. Hepatol. 2011, 26, 943–951. [Google Scholar] [CrossRef]
- Jayakumar, A.R.; Norenberg, M.D. Hyperammonemia in Hepatic Encephalopathy. J. Clin. Exp. Hepatol. 2018, 8, 272–280. [Google Scholar] [CrossRef]
- Jayakumar, A.R.; Norenberg, M.D. Aberrant Brain Bile Acid Signaling and Cholesterol Accumulation: A New Look at Mechanisms in Hepatic Encephalopathy. Cell. Mol. Gastroenterol. Hepatol. 2018, 6, 119–120. [Google Scholar] [CrossRef]
- Pereira, K.; Carrion, A.F.; Martin, P.; Vaheesan, K.; Salsamendi, J.; Doshi, M.; Yrizarry, J.M. Current diagnosis and management of post-transjugular intrahepatic portosystemic shunt refractory hepatic encephalopathy. Liver Int. 2015, 35, 2487–2494. [Google Scholar] [CrossRef]
- Sheasgreen, C.; Lu, L.; Patel, A. Pathophysiology, diagnosis, and management of hepatic encephalopathy. Inflammopharmacology 2014, 22, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, A.R.; Norenberg, M.D. Glutamine Synthetase: Role in Neurological Disorders. Adv. Neurobiol. 2016, 13, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Desjardins, P.; Du, T.; Jiang, W.; Peng, L.; Butterworth, R.F. Pathogenesis of hepatic encephalopathy and brain edema in acute liver failure: Role of glutamine redefined. Neurochem. Int. 2012, 60, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Liotta, E.M.; Kimberly, W.T. Cerebral edema and liver disease: Classic perspectives and contemporary hypotheses on mechanism. Neurosci. Lett. 2020, 721, 134818. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.J.; Zhong, J.; Lu, G.M. Multimodality MR Imaging Findings of Low-Grade Brain Edema in Hepatic Encephalopathy. Am. J. Neuroradiol. 2013, 34, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Frederick, R.T. Current Concepts in the Pathophysiology and Management of Hepatic Encephalopathy. Gastroenterol. Hepatol. 2011, 7, 222–233. [Google Scholar]
- Tranah, T.H.; Paolino, A.; Shawcross, D.L. Pathophysiological mechanisms of hepatic encephalopathy. Clin. Liver Dis. 2015, 5, 59–63. [Google Scholar] [CrossRef]
- Riggio, O.; Nardelli, S.; Moscucci, F.; Pasquale, C.; Ridola, L.; Merli, M. Hepatic Encephalopathy After Transjugular Intrahepatic Portosystemic Shunt. Clin. Liver Dis. 2012, 16, 133–146. [Google Scholar] [CrossRef]
- Tsien, C.; Shah, S.N.; McCullough, A.J.; Dasarathy, S. Reversal of sarcopenia predicts survival after a transjugular intrahepatic portosystemic stent. Eur. J. Gastroenterol. Hepatol. 2013, 25, 85–93. [Google Scholar] [CrossRef]
- Dasarathy, J.; Alkhouri, N.; Dasarathy, D. Changes in body composition after transjugular intrahepatic portosystemic stent in cirrhosis: A critical review of literature. Liver Int. 2011, 31, 1250–1258. [Google Scholar] [CrossRef]
- Ong, J.P.; Aggarwal, A.; Krieger, D.; Easley, K.A.; Karafa, M.T.; Van Lente, F.; Arroliga, A.C.; Mullen, K.D. Correlation between ammonia levels and the severity of hepatic encephalopathy. Am. J. Med. 2003, 114, 188–193. [Google Scholar] [CrossRef]
- Kundra, A.; Jain, A.; Banga, A.; Bajaj, G.; Kar, P. Evaluation of plasma ammonia levels in patients with acute liver failure and chronic liver disease and its correlation with the severity of hepatic encephalopathy and clinical features of raised intracranial tension. Clin. Biochem. 2005, 38, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Sun, Q.; Sun, X.; Chen, D.; Wei, C.; Yu, X.; Liu, C.; Li, Y.; Li, J. Activation of GABAA Receptors in Colon Epithelium Exacerbates Acute Colitis. Front. Immunol. 2018, 9, 987. [Google Scholar] [CrossRef] [PubMed]
- Häussinger, D.; Sies, H. Hepatic encephalopathy: Clinical aspects and pathogenetic concept. Arch. Biochem. Biophys. 2013, 536, 97–100. [Google Scholar] [CrossRef]
- Grønbæk, L.; Watson, H.; Vilstrup, H.; Jepsen, P. Benzodiazepines and risk for hepatic encephalopathy in patients with cirrhosis and ascites. United Eur. Gastroenterol. J. 2018, 6, 407–412. [Google Scholar] [CrossRef]
- Ahboucha, S.; Gamrani, H.; Baker, G. GABAergic neurosteroids: The “endogenous benzodiazepines” of acute liver failure. Neurochem. Int. 2012, 60, 707–714. [Google Scholar] [CrossRef]
- Manzhalii, E.; Virchenko, O.; Falalyeyeva, T.; Moiseienko, V.; Nykula, T.; Kondratiuk, V.; Savchuk, O.; Beregova, T.; Stremmel, W. Hepatic Encephalopathy Aggravated by Systemic Inflammation. Dig. Dis. 2019, 37, 509–517. [Google Scholar] [CrossRef]
- Gluud, L.L.; Dam, G.; Les, I.; Marchesini, G.; Borre, M.; Aagaard, N.K.; Vilstrup, H. Branched-chain amino acids for people with hepatic encephalopathy. Cochrane Database Syst. Rev. 2017, 5, CD001939. [Google Scholar] [CrossRef]
- Dam, G.; Keiding, S.; Munk, O.L.; Ott, P.; Buhl, M.; Vilstrup, H.; Bak, L.K.; Waagepetersen, H.S.; Schousboe, A.; Møller, N.; et al. Branched-chain amino acids increase arterial blood ammonia in spite of enhanced intrinsic muscle ammonia metabolism in patients with cirrhosis and healthy subjects. Am. J. Physiol. Liver Physiol. 2011, 301, G269–G277. [Google Scholar] [CrossRef]
- Holecek, M. Ammonia and amino acid profiles in liver cirrhosis: Effects of variables leading to hepatic encephalopathy. Nutrition 2015, 31, 14–20. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Taniguchi, E.; Sata, M. Effects of Oral Branched-Chain Amino Acids on Hepatic Encephalopathy and Outcome in Patients with Liver Cirrhosis. Nutr. Clin. Pract. 2013, 28, 580–588. [Google Scholar] [CrossRef] [PubMed]
- Mandiga, P.; Foris, L.A.; Kassim, G.; Bollu, P.C. Hepatic Encephalopathy; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Acharya, C.; Bajaj, J.S. Current Management of Hepatic Encephalopathy. Am. J. Gastroenterol. 2018, 113, 1600–1612. [Google Scholar] [CrossRef] [PubMed]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study Of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef] [PubMed]
- Dharel, N.; Bajaj, J.S. Definition and Nomenclature of Hepatic Encephalopathy. J. Clin. Exp. Hepatol. 2015, 5, S37–S41. [Google Scholar] [CrossRef] [PubMed]
- Butterworth, R.F.; Norenberg, M.D.; Felipo, V.; Ferenci, P.; Albrecht, J.; Blei, A.T.; Members of the ISHEN Commision on Experimental Models of HE. Experimental models of hepatic encephalopathy: ISHEN guidelines. Liver Int. 2009, 29, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Cordoba, J.; Mullen, K.D.; Amodio, P.; Shawcross, D.L.; Butterworth, R.F.; Morgan, M.Y. Review article: The design of clinical trials in hepatic encephalopathy—An International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN) consensus statement. Aliment. Pharmacol. Ther. 2011, 33, 739–747. [Google Scholar] [CrossRef]
- Jepsen, P.; Watson, H.; Andersen, P.K.; Vilstrup, H. Diabetes as a risk factor for hepatic encephalopathy in cirrhosis patients. J. Hepatol. 2015, 63, 1133–1138. [Google Scholar] [CrossRef]
- Riggio, O.; Amodio, P.; Farcomeni, A.; Merli, M.; Nardelli, S.; Pasquale, C.; Pentassuglio, I.; Gioia, S.; Onori, E.; Piazza, N.; et al. A Model for Predicting Development of Overt Hepatic Encephalopathy in Patients with Cirrhosis. Clin. Gastroenterol. Hepatol. 2015, 13, 1346–1352. [Google Scholar] [CrossRef]
- Ruiz-Margáin, A.; Macías-Rodríguez, R.U.; Ampuero, J.; Cubero, F.J.; Chi-Cervera, L.; Ríos-Torres, S.L.; Duarte-Rojo, A.; Espinosa-Cuevas, Á.; Romero-Gómez, M.; Torre, A. Low phase angle is associated with the development of hepatic encephalopathy in patients with cirrhosis. World J. Gastroenterol. 2016, 22, 10064–10070. [Google Scholar] [CrossRef]
- Tapper, E.B.; Parikh, N.D.; Sengupta, N.; Mellinger, J.; Ratz, D.; Lok, A.S.F.; Su, G.L. A risk score to predict the development of hepatic encephalopathy in a population-based cohort of patients with cirrhosis. Hepatology 2018, 68, 1498–1507. [Google Scholar] [CrossRef]
- Nardelli, S.; Gioia, S.; Ridola, L.; Farcomeni, A.; Merli, M.; Riggio, O. Proton Pump Inhibitors Are Associated with Minimal and Overt Hepatic Encephalopathy and Increased Mortality in Patients with Cirrhosis. Hepatology 2019, 70, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Ampuero, J.; Montoliú, C.; Simón-Talero, M.; Aguilera, V.; Millán, R.; Márquez, C.; Jover, R.; Rico, M.C.; Sendra, C.; Serra, M.Á.; et al. Minimal hepatic encephalopathy identifies patients at risk of faster cirrhosis progression. J. Gastroenterol. Hepatol. 2018, 33, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Bannister, C.A.; Orr, J.G.; Reynolds, A.V.; Hudson, M.; Conway, P.; Radwan, A.; Morgan, C.L.; Currie, C.J. Natural History of Patients Taking Rifaximin-α for Recurrent Hepatic Encephalopathy and Risk of Future Overt Episodes and Mortality: A Post-hoc Analysis of Clinical Trials Data. Clin. Ther. 2016, 38, 1081.e4–1089.e4. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zuo, L.; An, G.; Yue, Z.; Zhao, H.; Wang, L.; Liu, F. Risk Factors for Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt in Patients with Hepatocellular Carcinoma and Portal Hypertension. J. Gastrointest. Liver Dis. 2015, 24, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Gioia, S.; Pasquale, C.; Pentassuglio, I.; Farcomeni, A.; Merli, M.; Salvatori, F.M.; Nikolli, L.; Torrisi, S.; Greco, F.; et al. Cognitive impairment predicts the occurrence of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt. Am. J. Gastroenterol. 2016, 111, 523–528. [Google Scholar] [CrossRef]
- Lewis, D.S.; Lee, T.-H.; Konanur, M.; Ziegler, C.; Hall, M.D.; Pabon-Ramos, W.M.; Suhocki, P.V.; Smith, T.P.; Kim, C.Y.; Choi, S.S.; et al. Proton Pump Inhibitor Use Is Associated with an Increased Frequency of New or Worsening Hepatic Encephalopathy after Transjugular Intrahepatic Portosystemic Shunt Creation. J. Vasc. Interv. Radiol. 2019, 30, 163–169. [Google Scholar] [CrossRef]
- Yin, X.; Zhang, F.; Guo, H.; Peng, C.; Zhang, W.; Xiao, J.; Wang, Y.; Zou, X.; Zhang, M.; Zhuge, Y. A nomogram to predict the risk of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt in Cirrhotic Patients. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Trieu, H.; Lee, E.W. A new and improved transjugular intrahepatic portosystemic shunt (TIPS) stent graft: Controlled expansion. Gastrointest. Interv. 2018, 7, 18–20. [Google Scholar] [CrossRef]
- Pieper, C.C.; Jansen, C.; Meyer, C.; Nadal, J.; Lehmann, J.; Schild, H.H.; Trebicka, J.; Thomas, D. Prospective Evaluation of Passive Expansion of Partially Dilated Transjugular Intrahepatic Portosystemic Shunt Stent Grafts—A Three-Dimensional Sonography Study. J. Vasc. Interv. Radiol. 2017, 28, 117–125. [Google Scholar] [CrossRef]
- Pieper, C.C.; Sprinkart, A.M.; Nadal, J.; Hippe, V.; Meyer, C.; Schild, H.H.; Thomas, D. Postinterventional Passive Expansion of Partially Dilated Transjugular Intrahepatic Portosystemic Shunt Stents. J. Vasc. Interv. Radiol. 2015, 26, 388–394. [Google Scholar] [CrossRef]
- Mollaiyan, A.; Bettinger, D.; Rössle, M. The underdilation of nitinol stents at TIPS implantation: Solution or illusion? Eur. J. Radiol. 2017, 89, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Srinivasa, R.N.; Srinivasa, R.N.; Chick, J.F.B.; Hage, A.; Saad, W.A. Transjugular Intrahepatic Portosystemic Shunt Reduction Using the GORE VIATORR Controlled Expansion Endoprosthesis: Hemodynamics of Reducing an Established 10-mm TIPS to 8-mm in Diameter. Cardiovasc. Interv. Radiol. 2018, 41, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, R.; Maruzzelli, L.; Di Piazza, A.; Mamone, G.; Caruso, S.; Gentile, G.; Tuzzolino, F.; Floridia, G.; Petridis, I.; Volpes, R.; et al. Transjugular Intrahepatic Portosystemic Shunt Using the New Gore Viatorr Controlled Expansion Endoprosthesis: Prospective, Single-Center, Preliminary Experience. Cardiovasc. Interv. Radiol. 2019, 42, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Riggio, O.; Gioia, S.; Puzzono, M.; Pelle, G.; Ridola, L. Spontaneous porto-systemic shunts in liver cirrhosis: Clinical and therapeutical aspects. World J. Gastroenterol. 2020, 26, 1726–1732. [Google Scholar] [CrossRef] [PubMed]
- Simón-Talero, M.; Roccarina, D.; Martínez, J.; Lampichler, K.; Baiges, A.; Low, G.; Llop, E.; Praktiknjo, M.; Maurer, M.H.; Zipprich, A.; et al. Association Between Portosystemic Shunts and Increased Complications and Mortality in Patients With Cirrhosis. Gastroenterology 2018, 154, 1694.e4–1705.e4. [Google Scholar] [CrossRef]
- Praktiknjo, M.; Simón-Talero, M.; Römer, J.; Roccarina, D.; Martínez, J.; Lampichler, K.; Baiges, A.; Low, G.; Llop, E.; Maurer, M.H.; et al. Total area of spontaneous portosystemic shunts independently predicts hepatic encephalopathy and mortality in liver cirrhosis. J. Hepatol. 2020, 72, 1140–1150. [Google Scholar] [CrossRef]
- Wang, Q.; Lv, Y.; Bai, M.; Wang, Z.; Liu, H.; He, C.; Niu, J.; Guo, W.; Luo, B.; Yin, Z.; et al. Eight millimetre covered TIPS does not compromise shunt function but reduces hepatic encephalopathy in preventing variceal rebleeding. J. Hepatol. 2017, 67, 508–516. [Google Scholar] [CrossRef]
- Cao, Q.; Yu, C.B.; Yang, S.G.; Cao, H.C.; Chen, P.; Deng, M.; Li, L.J. Effect of probiotic treatment on cirrhotic patients with minimal hepatic encephalopathy: A meta-analysis. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 9–16. [Google Scholar] [CrossRef]
- Hörner, D.V.; Avery, A.; Stow, R. The Effects of Probiotics and Symbiotics on Risk Factors for Hepatic Encephalopathy. J. Clin. Gastroenterol. 2017, 51, 312–323. [Google Scholar] [CrossRef]
- Saab, S.; Suraweera, D.; Au, J.; Saab, E.G.; Alper, T.S.; Tong, M.J. Probiotics are helpful in hepatic encephalopathy: A meta-analysis of randomized trials. Liver Int. 2016, 36, 986–993. [Google Scholar] [CrossRef]
- Cammarota, G.; Ianiro, G.; Tilg, H.; Rajilić-Stojanović, M.; Kump, P.; Satokari, R.; Sokol, H.; Arkkila, P.; Pintus, C.; Hart, A.; et al. European consensus conference on faecal microbiota transplantation in clinical practice. Gut 2017, 66, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Salzman, N.H.; Acharya, C.; Sterling, R.K.; White, M.B.; Gavis, E.A.; Fagan, A.; Hayward, M.; Holtz, M.L.; Matherly, S.; et al. Fecal Microbial Transplant Capsules Are Safe in Hepatic Encephalopathy: A Phase 1, Randomized, Placebo-Controlled Trial. Hepatology 2019, 70, 1690–1703. [Google Scholar] [CrossRef] [PubMed]
- Maharshi, S.; Sharma, B.C.; Sachdeva, S.; Srivastava, S.; Sharma, P. Efficacy of Nutritional Therapy for Patients with Cirrhosis and Minimal Hepatic Encephalopathy in a Randomized Trial. Clin. Gastroenterol. Hepatol. 2016, 14, 454.e3–460.e3. [Google Scholar] [CrossRef] [PubMed]
- Philips, C.A.; Rajesh, S.; Augustine, P.; Padsalgi, G.; Ahamed, R. Portosystemic shunts and refractory hepatic encephalopathy: Patient selection and current options. Hepatic Med. Evid. Res. 2019, 11, 23–34. [Google Scholar] [CrossRef]
- Kochar, N.; Tripathi, D.; Ireland, H.; Redhead, D.N.; Hayes, P.C. Transjugular intrahepatic portosystemic stent shunt (TIPSS) modification in the management of post-TIPSS refractory hepatic encephalopathy. Gut 2006, 55, 1617–1623. [Google Scholar] [CrossRef]
- Nardelli, S.; Gioia, S.; Ridola, L.; Riggio, O. Radiological Intervention for Shunt Related Encephalopathy. J. Clin. Exp. Hepatol. 2018, 8, 452–459. [Google Scholar] [CrossRef]
- De Santis, A.; Nardelli, S.; Bassanelli, C.; Lupo, M.; Iegri, C.; Di Ciesco, C.A.; Forlino, M.; Farcomeni, A.; Riggio, O. Modification of splenic stiffness on acoustic radiation force impulse parallels the variation of portal pressure induced by transjugular intrahepatic portosystemic shunt. J. Gastroenterol. Hepatol. 2018, 33, 704–709. [Google Scholar] [CrossRef]
- Schindler, P.; Seifert, L.; Masthoff, M.; Riegel, A.; Köhler, M.; Wilms, C.; Schmidt, H.H.; Heinzow, H.; Wildgruber, M. TIPS Modification in the Management of Shunt-Induced Hepatic Encephalopathy: Analysis of Predictive Factors and Outcome with Shunt Modification. J. Clin. Med. 2020, 9, 567. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type | Grade | Time Course | Spontaneous/Precipitated | |
|---|---|---|---|---|
| A | Minimal | Covert | Episodic | Spontaneous |
| I | ||||
| B | II | Recurrent | ||
| III | Overt | Precipitated factors | ||
| C | IV | Persistent | ||
| Reference | Study Design | Number of Patients | Risk Factor | Adjusted Hazard Ratio (95% CI) |
|---|---|---|---|---|
| Jepsen et al., 2015 [58] | Secondary analysis * | 862 | Diabetes | 1.86 (1.20–2.87) |
| Child–Pugh class B | 2.57 (0.61–10.8) | |||
| Child–Pugh class C | 4.32 (0.96–19.3) | |||
| Bilirubin, per 10 µmol/l increase | 1.06 (1.03–1.08) | |||
| Albumin, per 5 g/L increase | 0.68 (0.56–0.83) | |||
| Sodium, per 5 mmol/L increase | 0.63 (0.53–0.74) | |||
| Creatinine, per 10 μmol/L increase | 1.09 (1.05–1.13) | |||
| Riggio et al., 2015 [59] | Retrospective cohort | 216 | Previous overt HE | 2.01 (1.24–3.26) |
| Minimal HE | 2.02 (1.23–3.33) | |||
| Albumin level < 3.5 g/dL | 2.32 (1.37–3.93) | |||
| Ruiz-Margáin et al., 2016 [60] | Prospective cohort | 220 | Cachexia | 1.81 (1.08–3.03) |
| Creatinine, per 1 mg/dL increase | 4.12 (1.57–10.77) | |||
| Tapper et al., 2018 [61] | Retrospective cohort | 1979 | Bilirubin, per 1 mg/dL increase | 1.07 (1.05–1.09) |
| Albumin, per 1 mg/dL increase | 0.54 (0.49–0.60) | |||
| Non-selective beta-blocker use | 1.34 (1.09–1.64) | |||
| Statin use | 0.80 (0.65–0.98) | |||
| Nardelli et al., 2019 [62] | Prospective cohort | 310 | Albumin, per 1 g/L increase | 0.47 (0.33–0.69) |
| Previous overt HE | 2.45 (1.66–3.58) | |||
| Minimal HE | 1.79 (1.21–2.65) | |||
| Proton pump inhibitors use | 1.83 (1.22–2.74) |
| Reference | Study Design | Number of Patients | Risk Factor | Adjusted Hazard Ratio (95% CI) |
|---|---|---|---|---|
| Yao et al., 2015 [65] | Retrospective cohort | 279 | Pre-TIPS MELD | 1.69 (1.39–2.06) + |
| PPG post-TIPS | 1.20 (1.07–1.34) + | |||
| Nardelli et al., 2016 [66] | Prospective cohort | 82 | Age | 1.05 (1.02–1.08) |
| Child–Pugh score | 1.29 (1.06–1.56) | |||
| Covert HE before TIPS | 3.16 (1.43–6.99) | |||
| Nardelli et al., 2017 [26] | Prospective cohort | 46 | Sarcopenia | 31.3 (4.5–218.07) |
| Pre-TIPS MELD | 1.16 (1.01–1.34) | |||
| Lewis et al., 2019 [67] | Retrospective cohort | 284 | Age | 1.05 (1.03–1.07) * |
| Pre-TIPS MELD | 1.06 (1.01–1.11) * | |||
| HE before TIPS | 1.51 (1.04–2.20) * | |||
| Proton pump inhibitors use | 3.19 (2.19–4.66) * | |||
| Yin et al., 2020 [68] | Retrospective cohort | 264 | Age | 1.03 (1.00–3.21) |
| Diabetes | 1.84 (1.06–3.21) | |||
| Child-Turcotte-Pugh class C | 6.68 (1.68–8.89) | |||
| Sodium | 0.94 (0.88–0.99) | |||
| Creatinine | 1.01 (1.00–1.03) |
| Reference | No. with Refractory HE/Treated with TIPS | Child–Pugh Class | No. of Patients Improved | Recurrence of Primary TIPS Indication after Shunt Modification | PPG Pre (mmHg) | PPG Post (mmHg) |
|---|---|---|---|---|---|---|
| Nardelli et al., 2016 [66] | 3/82 | B: 1 C: 2 | 3 | - | 5.6 ± 3.2 | 12.1 ± 2.7 |
| De Santis et al., 2018 [88] | 2/38 | B: 1 C: 1 | 2 | Ascites 1 Bleeding 1 | 6.5 ± 2.6 | 12.7 ± 3.8 |
| Bureau et al., 2017 [4] | 1/29 | C: 1 | 1 | - | - | - |
| Rowley et al., 2018 [19] | 10/174 | - | 8 | - | 8.6 ± 4.1 | 13.0 ± 4.0 |
| Schindler et al., 2020 [89] | 20/344 | A: 7 B: 9 C: 4 | 11 | Ascites 2 Bleeding 1 | 7.7 ± 3.9 | 12.1 ± 4.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schindler, P.; Heinzow, H.; Trebicka, J.; Wildgruber, M. Shunt-Induced Hepatic Encephalopathy in TIPS: Current Approaches and Clinical Challenges. J. Clin. Med. 2020, 9, 3784. https://doi.org/10.3390/jcm9113784
Schindler P, Heinzow H, Trebicka J, Wildgruber M. Shunt-Induced Hepatic Encephalopathy in TIPS: Current Approaches and Clinical Challenges. Journal of Clinical Medicine. 2020; 9(11):3784. https://doi.org/10.3390/jcm9113784
Chicago/Turabian StyleSchindler, Philipp, Hauke Heinzow, Jonel Trebicka, and Moritz Wildgruber. 2020. "Shunt-Induced Hepatic Encephalopathy in TIPS: Current Approaches and Clinical Challenges" Journal of Clinical Medicine 9, no. 11: 3784. https://doi.org/10.3390/jcm9113784
APA StyleSchindler, P., Heinzow, H., Trebicka, J., & Wildgruber, M. (2020). Shunt-Induced Hepatic Encephalopathy in TIPS: Current Approaches and Clinical Challenges. Journal of Clinical Medicine, 9(11), 3784. https://doi.org/10.3390/jcm9113784