World Health Organization’s Growth Reference Overestimates the Prevalence of Severe Malnutrition in Children with Sickle Cell Anemia in Africa

 ,
,
Abstract
1. Introduction
2. Materials and Methods
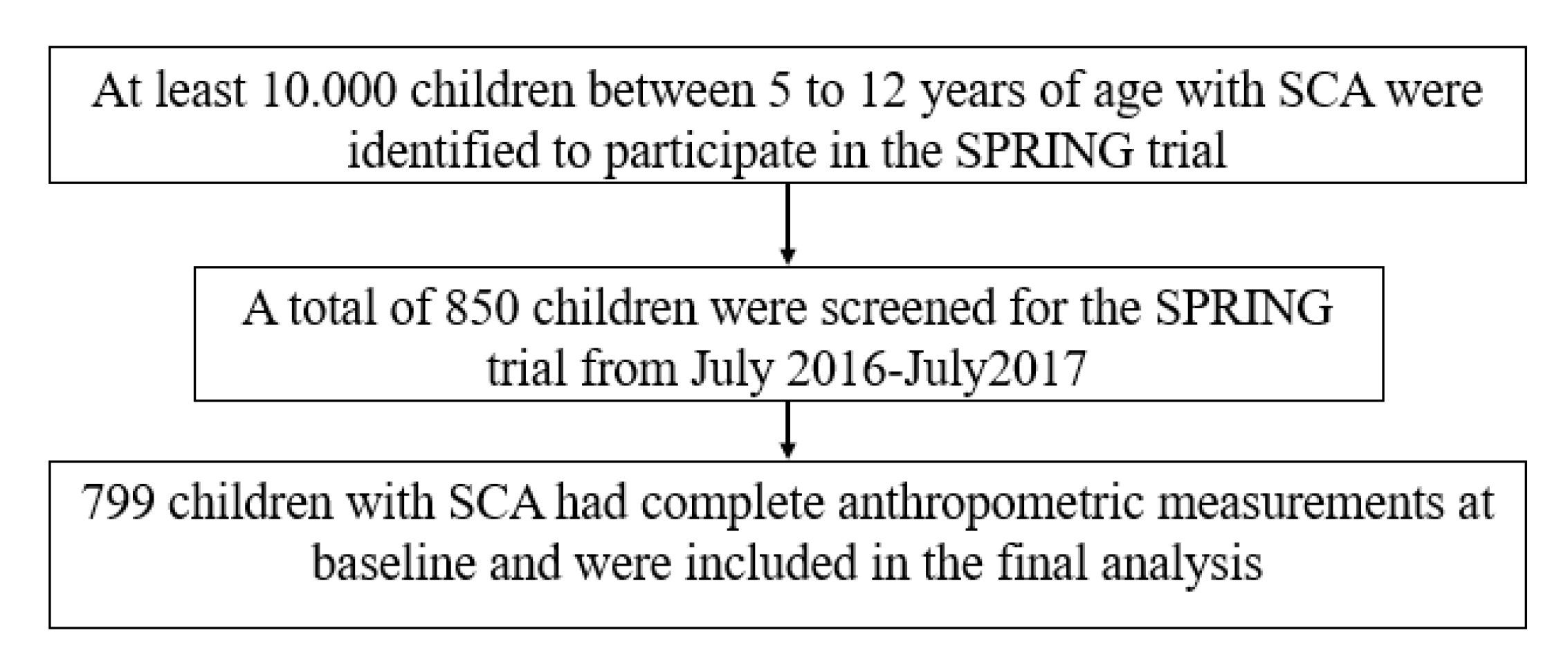
2.1. Study Design and Population
- ○
- Aminu Kano Teaching Hospital (AKTH) is a 500-bed tertiary level facility. The pediatric SCD clinic at AKTH has a total patient pool of about 2010, with approximately 80 children with SCA seen weekly, staffed by a pediatrician and a nurse;
- ○
- Murtala Muhammad Specialist Hospital (MMSH) is an AKTH-affiliated high-volume clinic located less than three miles from AKTH. The pediatric clinic runs daily (Monday through Friday) and has a total patient pool of over 17,810 children with SCA, with at least 400 children seen each week;
- ○
- Hasiya Bayero Pediatric Hospital (HBPH) is a 90-bed pediatric hospital located approximately 2.5 miles from AKTH and is the only hospital in the area dedicated to the care of children. HBPH runs a full pediatric SCD clinic once a week with a total patient pool of over 11,129 children with SCA. Nurses and community health workers evaluate over 100 children with SCA daily and pediatricians once a week;
- ○
- Muhammad Abdullahi Wase Specialist Hospital (MAWSH) is a 320-bed multispecialty hospital and the third busiest hospital in Kano, after MMSH and AKTH. MAWSH is located five miles from AKTH with a total pool of 470 children with SCA. Approximately 42 children with SCA are seen once a week by a pediatrician and a nurse;
- ○
- Barau Dikko Teaching Hospital (BDTH) serves as the teaching hospital for Kaduna State University. The SCD Clinic is open once a week, with an estimated total 1200 children with SCD registered and an average of 40 children seen weekly.
2.2. SCA-Specific Growth Reference
2.3. 2007 WHO Growth Reference
2.4. Data Collection and Definitions
2.5. Statistical Analysis
3. Results
3.1. Demographics
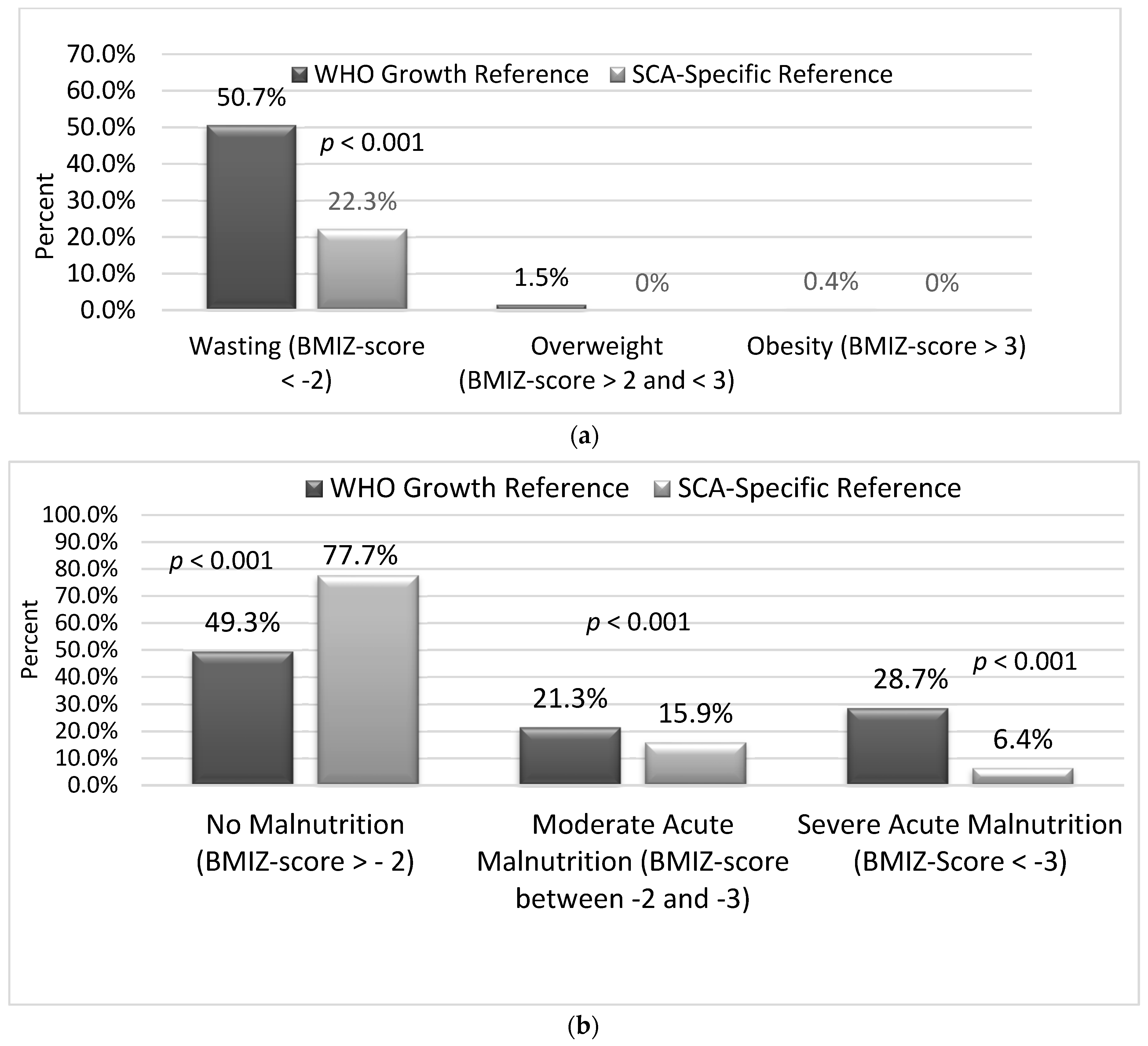
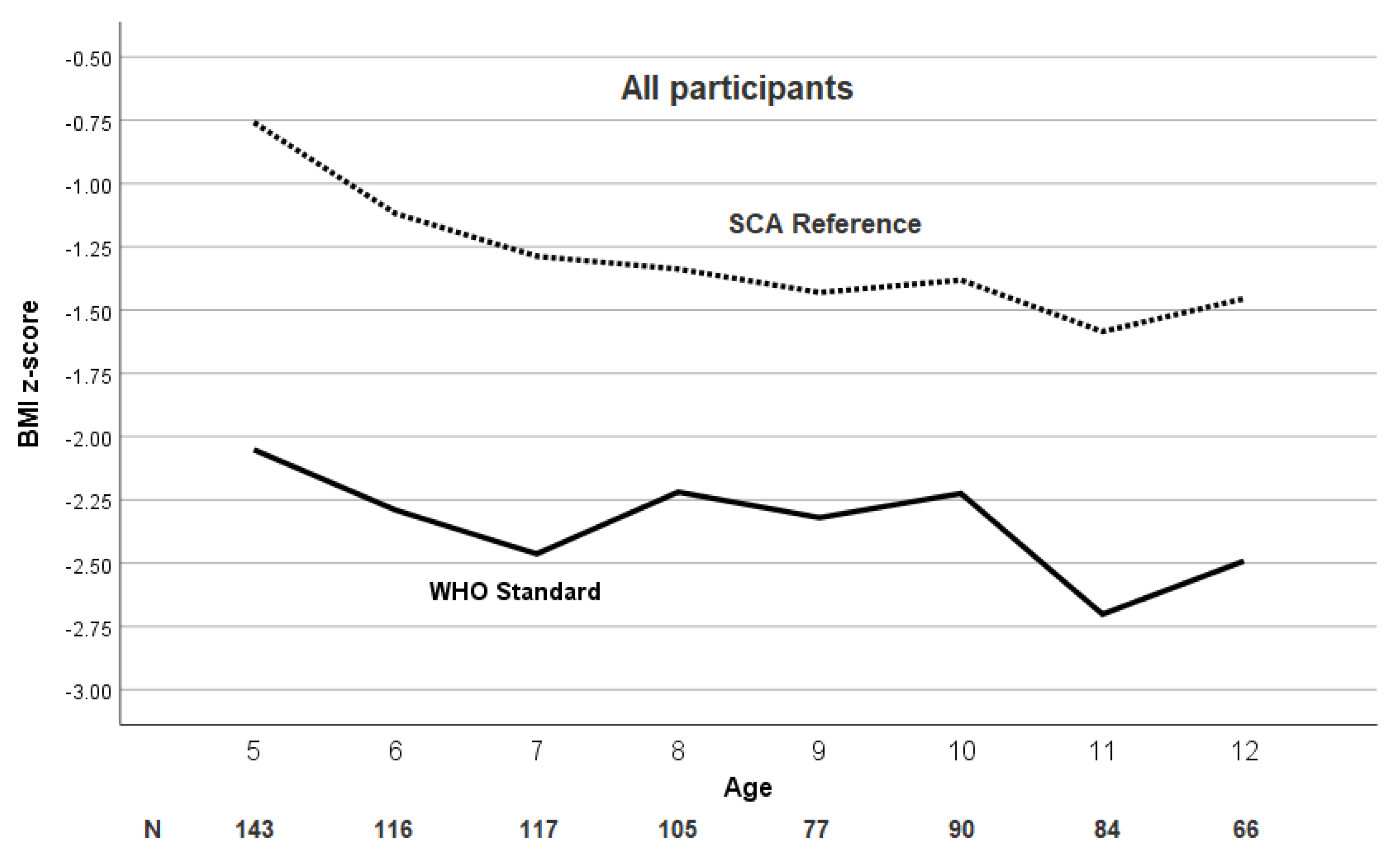
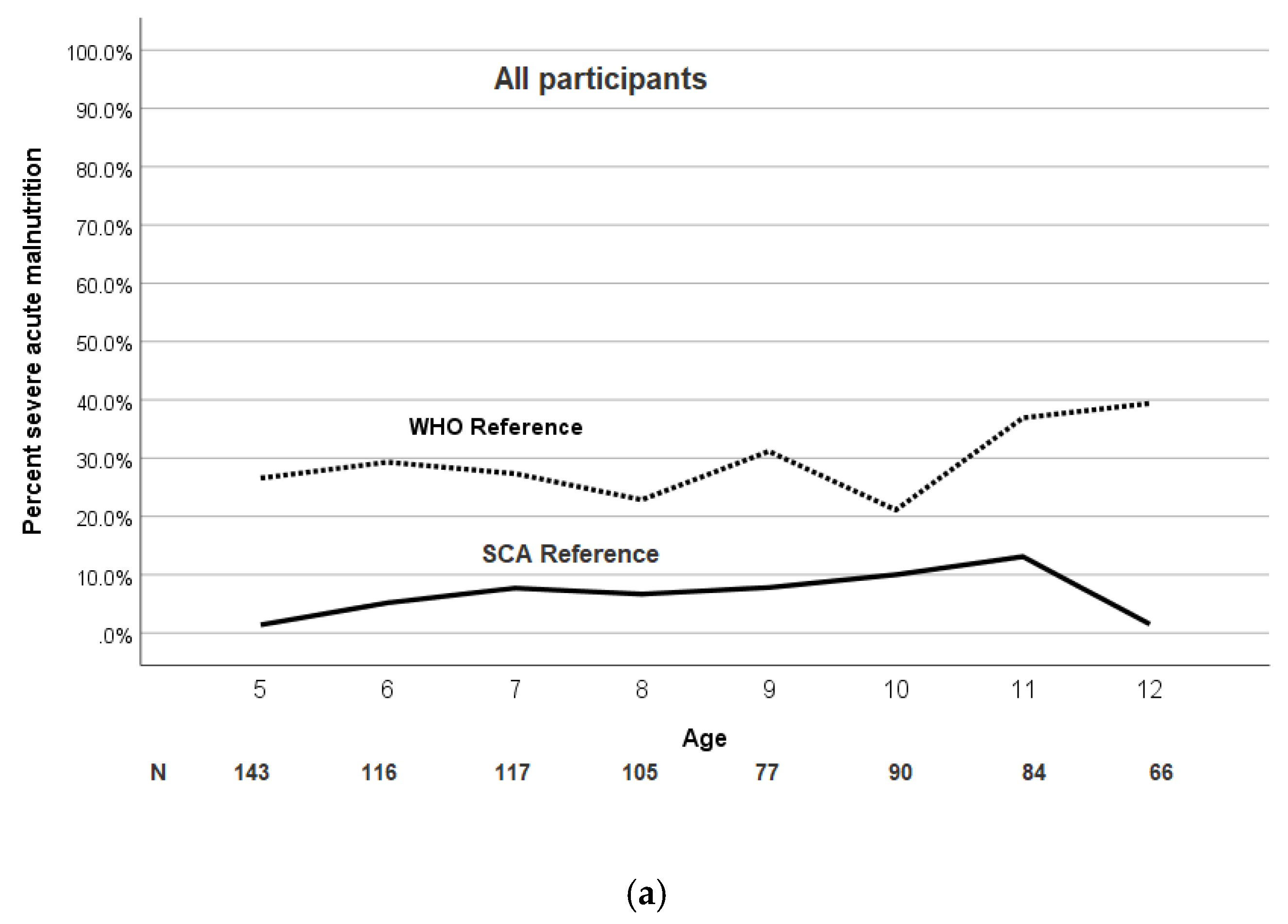
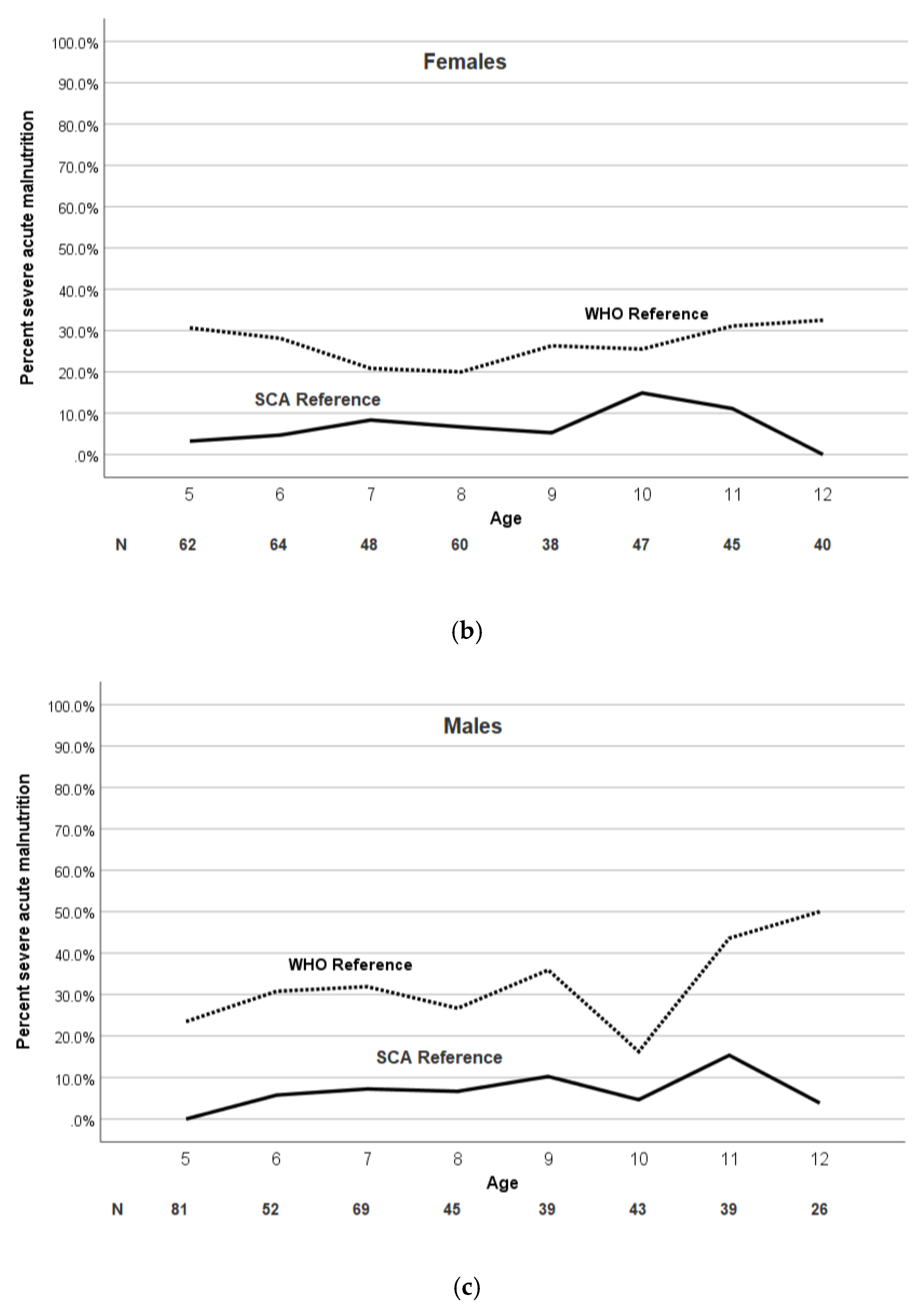
3.2. The Prevalence of Malnutrition Is Higher Based on the WHO Growth Reference Compared to SCD-Specific Growth Reference
3.3. Children with Severe Malnutrition Have Lower Mean TCD Measurements Compared to Those without Malnutrition Based on the WHO and SCA-Specific Growth Reference
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Coefficient * | 95% CI | p-Value |
|---|---|---|---|
| Age | −3.44 | −4.80, −2.09 | <0.001 |
| Sex (male) | −3.27 | −9.24, 2.69 | 0.282 |
| Hemoglobin | −6.96 | −10.04, −3.88 | <0.001 |
| White blood cell count | 0.61 | −0.06, 1.28 | 0.076 |
| SCA-specific moderate malnutrition # | −8.57 | −16.81, −0.34 | 0.041 |
| SCA-specific severe malnutrition # | −10.44 | −22.82, 1.94 | 0.098 |
References
- Piel, F.B.; Hay, S.I.; Gupta, S.; Weatherall, D.J.; Williams, T.N. Global burden of sickle cell anaemia in children under five, 2010–2050: Modelling based on demographics, excess mortality, and interventions. PLoS Med. 2013, 10, e1001484. [Google Scholar] [CrossRef] [PubMed]
- Piel, F.B.; Patil, A.P.; Howes, R.E.; Nyangiri, O.A.; Gething, P.W.; Dewi, M.; Temperley, W.H.; Williams, T.N.; Weatherall, D.J.; Hay, S.I. Global epidemiology of sickle haemoglobin in neonates: A contemporary geostatistical model-based map and population estimates. Lancet 2013, 381, 142–151. [Google Scholar] [CrossRef]
- World Health Organization. Sickle-Cell Anemia: Report by the Secretariat; World Health Assembly: Geneva, Switzerland, 2006. [Google Scholar]
- Therrell, B.L., Jr.; Lloyd-Puryear, M.A.; Eckman, J.R.; Mann, M.Y. Newborn screening for sickle cell diseases in the United States: A review of data spanning 2 decades. In Seminars in Perinatology; Elsevier: Amsterdam, The Netherlands, 2015; Volume 39, pp. 238–251. [Google Scholar]
- Scott, R.B.; Ferguson, A.D.; Jenkins, M.E.; Clark, H.M. Studies in sickle-cell anemia. VIII. Further observations on the clinical manifestations of sickle-cell anemia in children. AMA Am. J. Dis. Child. 1955, 90, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, C.T.; Scott, R.B.; Henry, W.; Sampson, C.C.; Ferguson, A.D. Studies in sickle cell anemia: Xxvi. the effects of homozygous sickle cell disease on the onset of menarche, pregnancy, fertility, pubescent changes, and body growth in negro subjects. Am. J. Dis. Child. 1966, 111, 497–504. [Google Scholar] [CrossRef]
- Platt, O.S.; Rosenstock, W.; Espeland, M.A. Influence of sickle hemoglobinopathies on growth and development. N. Engl. J. Med. 1984, 311, 7–12. [Google Scholar] [CrossRef]
- Rhodes, M.; Akohoue, S.A.; Shankar, S.M.; Fleming, I.; Qi An, A.; Yu, C.; Acra, S.; Buchowski, M.S. Growth patterns in children with sickle cell anemia during puberty. Pediatr. Blood Cancer 2009, 53, 635–641. [Google Scholar] [CrossRef]
- Al-Saqladi, A.W.; Cipolotti, R.; Fijnvandraat, K.; Brabin, B.J. Growth and nutritional status of children with homozygous sickle cell disease. Ann. Trop. Paediatr. 2008, 28, 165–189. [Google Scholar] [CrossRef]
- Lyon, A.J.; Preece, M.A.; Grant, D.B. Growth curve for girls with Turner syndrome. Arch. Dis. Child. 1985, 60, 932–935. [Google Scholar] [CrossRef]
- Morison, S.; Dodge, J.A.; Cole, T.J.; Lewis, P.A.; Coles, E.C.; Geddes, D.; Russell, G.; Littlewood, J.M.; Scott, M.T. Height and weight in cystic fibrosis: A cross sectional study. UK Cystic Fibrosis Survey Management Committee. Arch. Dis. Child. 1997, 77, 497–500. [Google Scholar] [CrossRef]
- Myrelid, A.; Gustafsson, J.; Ollars, B.; Anneren, G. Growth charts for Down’s syndrome from birth to 18 years of age. Arch. Dis. Child. 2002, 87, 97–103. [Google Scholar] [CrossRef]
- Patel, L.; Dixon, M.; David, T.J. Growth and growth charts in cystic fibrosis. J. R. Soc. Med. 2003, 96, 35–41. [Google Scholar] [PubMed]
- Rongen-Westerlaken, C.; Corel, L.; van den Broeck, J.; Massa, G.; Karlberg, J.; Albertsson-Wikland, K.; Naeraa, R.W.; Wit, J.M. Reference values for height, height velocity and weight in Turner’s syndrome. Swedish Study Group for GH treatment. Acta Paediatr. 1997, 86, 937–942. [Google Scholar] [CrossRef] [PubMed]
- Styles, M.E.; Cole, T.J.; Dennis, J.; Preece, M.A. New cross sectional stature, weight, and head circumference references for Down’s syndrome in the UK and Republic of Ireland. Arch. Dis. Child. 2002, 87, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Van Gameren-Oosterom, H.B.; Van Dommelen, P.; Oudesluys-Murphy, A.M.; Buitendijk, S.E.; Van Buuren, S.; Van Wouwe, J.P. Healthy growth in children with Down syndrome. PLoS ONE 2012, 7, e31079. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.B.; Saville, B.R.; Roberts, D.O.; Fissell, R.B.; Kassim, A.A.; Airewele, G.; DeBaun, M.R. Factors associated with growth and blood pressure patterns in children with sickle cell anemia: Silent Cerebral Infarct Multi-Center Clinical Trial cohort. Am. J. Hematol. 2015, 90, 2–7. [Google Scholar] [CrossRef] [PubMed]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Galadanci, A.A.; Galadanci, N.A.; Jibir, B.W.; Abdullahi, S.U.; Idris, N.; Gambo, S.; Ali, S.A.; Kabo, N.A.; Bello-Manga, H.; Haliru, L.; et al. Approximately 40,000 children with sickle cell anemia require screening with TCD and treating with hydroxyurea for stroke prevention in three states in northern Nigeria. Am. J. Hematol. 2019, 94, E305. [Google Scholar] [CrossRef]
- DeBaun, M.R.; Gordon, M.; McKinstry, R.C.; Noetzel, M.J.; White, D.A.; Sarnaik, S.A.; Meier, E.R.; Howard, T.H.; Majumdar, S.; Inusa, B.P.; et al. Controlled trial of transfusions for silent cerebral infarcts in sickle cell anemia. N. Engl. J. Med. 2014, 371, 699–710. [Google Scholar] [CrossRef]
- Thakur, N.; Chandra, J.; Pemde, H.; Singh, V. Anemia in severe acute malnutrition. Nutrition 2014, 30, 440–442. [Google Scholar] [CrossRef]
- Rankine-Mullings, A.E.; Morrison-Levy, N.; Soares, D.; Aldred, K.; King, L.; Ali, S.; Knight-Madden, J.M.; Wisdom-Phipps, M.; Adams, R.J.; Ware, R.E.; et al. Transcranial Doppler velocity among Jamaican children with sickle cell anaemia: Determining the significance of haematological values and nutrition. Br. J. Haematol. 2018, 181, 242–251. [Google Scholar] [CrossRef]
- Zemel, B.S.; Kawchak, D.A.; Ohene-Frempong, K.; Schall, J.I.; Stallings, V.A. Effects of delayed pubertal development, nutritional status, and disease severity on longitudinal patterns of growth failure in children with sickle cell disease. Pediatr Res. 2007, 61, 607–613. [Google Scholar] [CrossRef] [PubMed]





| Variable | SPRING Cohort (n = 799) | SIT Cohort (n = 1127) | p-Value # |
|---|---|---|---|
| Age, median (IQR) (years) | 8.2 (6.4–10.4) | 8.5 (6.7–10.7) | 0.001 § |
| Sex, male, n (%) | 395 (49.4) | 579 (51.4) | 0.402 |
| Weight, median (IQR)(kg) | 19.0 (16.0–22.0) | 25.9 (22.0–31.9) | <0.001 § |
| Height, median (IQR)(cm) | 120.0 (111.0–128.0) | 126.8 (117.9–137.7) | <0.001 § |
| BMI, mean (SD) | 13.7 (1.9) | 16.4 (2.7) | <0.001 |
| Hemoglobin, mean (SD) (n = 1909) | 7.6 (1.1) | 8.2 (2.6) | <0.001 |
| White Blood Count, mean (SD) (n = 1905) | 14.7 (5.1) | 12.6 (5.2) | <0.001 |
| Malnutrition | Abnormal TCD, % | p-Value # |
|---|---|---|
| SCA-Specific Growth Reference n = 799 | ||
| No malnutrition | 14.0 | 0.034 |
| Moderate malnutrition | 7.1 | |
| Severe malnutrition | 4.4 | |
| 2007 WHO Growth Reference n = 799 | ||
| No malnutrition | 14.8 | 0.059 |
| Moderate malnutrition | 12.3 | |
| Severe malnutrition | 7.9 | |
| Malnutrition | Hemoglobin (g/dL), Mean (SD) | p-Value # |
|---|---|---|
| SCA-Specific Growth Reference | ||
| No malnutrition | 7.5 (1.1) | 0.124 |
| Moderate malnutrition | 7.6 (1.1) | |
| Severe malnutrition | 7.9 (1.5) | |
| 2007 WHO Growth Reference | ||
| No malnutrition | 7.5 (1.2) | 0.981 |
| Moderate malnutrition | 7.6 (1.1) | |
| Severe malnutrition | 7.6 (1.2) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghafuri, D.L.; Abdullahi, S.U.; Jibir, B.W.; Gambo, S.; Bello-Manga, H.; Haliru, L.; Bulama, K.; Usman, F.M.; Gambo, A.; Aliyu, M.H.; et al. World Health Organization’s Growth Reference Overestimates the Prevalence of Severe Malnutrition in Children with Sickle Cell Anemia in Africa. J. Clin. Med. 2020, 9, 119. https://doi.org/10.3390/jcm9010119
Ghafuri DL, Abdullahi SU, Jibir BW, Gambo S, Bello-Manga H, Haliru L, Bulama K, Usman FM, Gambo A, Aliyu MH, et al. World Health Organization’s Growth Reference Overestimates the Prevalence of Severe Malnutrition in Children with Sickle Cell Anemia in Africa. Journal of Clinical Medicine. 2020; 9(1):119. https://doi.org/10.3390/jcm9010119
Chicago/Turabian StyleGhafuri, Djamila L., Shehu U. Abdullahi, Binta W. Jibir, Safiya Gambo, Halima Bello-Manga, Lawal Haliru, Khadija Bulama, Fahd M. Usman, Awwal Gambo, Muktar H. Aliyu, and et al. 2020. "World Health Organization’s Growth Reference Overestimates the Prevalence of Severe Malnutrition in Children with Sickle Cell Anemia in Africa" Journal of Clinical Medicine 9, no. 1: 119. https://doi.org/10.3390/jcm9010119
APA StyleGhafuri, D. L., Abdullahi, S. U., Jibir, B. W., Gambo, S., Bello-Manga, H., Haliru, L., Bulama, K., Usman, F. M., Gambo, A., Aliyu, M. H., Greene, B. C., Kassim, A. A., Slaughter, C., Rodeghier, M., & DeBaun, M. R. (2020). World Health Organization’s Growth Reference Overestimates the Prevalence of Severe Malnutrition in Children with Sickle Cell Anemia in Africa. Journal of Clinical Medicine, 9(1), 119. https://doi.org/10.3390/jcm9010119